Article Text

Abstract
Background: There are limited data comparing interferon-γ release assays (IGRAs) for the detection of Mycobacterium tuberculosis infection in highly endemic settings.
Methods: A cross-sectional household contact study was conducted to measure the agreement of two IGRAs in relation to the tuberculin skin test (TST) to detect M tuberculosis infection and to assess the influence of M tuberculosis exposure and age.
Results: In 82 individuals in household contact, 93% of children and 42% of adults had a high M tuberculosis contact score. The TST was positive in 78% of adults and 54% of children, the T-SPOT.TB was positive in 89% of children and 66% of adults and the QuantiFERON TB Gold (QTF) was positive in a similar proportion of adults and children (38.1% and 39.6%). In children there was poor agreement between the TST and T-SPOT.TB (κ = −0.15) and the T-SPOT.TB and the QTF (κ = −0.03), but good agreement between the TST and the QTF (κ = 0.78) using 10 mm cut-off. In adults there was fair to moderate agreement between the TST and T-SPOT.TB (κ = 0.38), the TST and QTF (κ = 0.34) and T-SPOT.TB and QTF (κ = −0.50). High levels of exposure to M tuberculosis were associated with at least a sevenfold odds of being T-SPOT.TB positive (95% CI 7.67 to 508.69) and a threefold odds of being QTF positive (95% CI 3.02 to 30.54). There was a significant difference in the magnitude of T-SPOT.TB early secretory antigenic target (ESAT)-6 and culture filtrate protein 10 kD (CFP-10) spot counts between adults and children.
Conclusions: The T-SPOT.TB may be more sensitive than the TST or QTF for detecting recent M tuberculosis infection in children. Differences between assays and the predictive utility of these findings for subsequent disease development should be prospectively assessed.
Statistics from Altmetric.com
Every year almost nine million people contract tuberculosis and two million people die from the disease.1 The risk of progressing to active tuberculosis following Mycobacterium tuberculosis infection is high in young children during the first year following infection, with children aged <1 year of age having a 50–60% risk of disease progression.2 3 HIV-infected adults and children are also at high risk of disease progression and reactivation.4 Since up to 60% of young children diagnosed with active tuberculosis have a reported household contact with an infectious index case in high-burden settings,5 contact tracing of children and other individuals exposed to a household index case represents an opportunity for intensified tuberculosis control.6
The diagnosis of M tuberculosis infection is complicated by the lack of a practical gold standard. Long-term follow-up of individuals to establish disease progression is therefore required to assess the predictive utility of diagnostic tools for tuberculosis. Although regarded as relatively robust for the diagnosis of M tuberculosis infection, the tuberculin skin test (TST) has reduced specificity in populations with exposure to non-tuberculous mycobacteria (NTM) and/or M bovis Bacille Calmette-Guérin (BCG) vaccination.7 TST values of ⩾10 mm are often regarded as positive in populations with normal immunity and who are BCG-vaccinated.8 9 TST sensitivity is limited in immune compromised individuals, very young and/or severely malnourished children or individuals with severe tuberculosis.7 The ability of the TST to detect recent M tuberculosis infection may be limited, as demonstrated by a high proportion of individuals who convert their TST 6–12 weeks after documented M tuberculosis exposure.10 Similarly, the proportion of individuals with T cell-based interferon gamma (IFNγ) release assay (IGRA) conversion following initial assessment may be as high as 24.6% at 3 months following negative initial responses.11 The potential benefits of an accurate diagnostic test of M tuberculosis infection include timely institution of preventive or curative treatment, with reduction of both underdiagnosis and overdiagnosis and burdening of healthcare systems.
IGRAs using early secretory antigenic target (ESAT)-6 and culture filtrate protein 10 kD (CFP-10) offer enhanced sensitivity and specificity by measuring IFNγ production in response to antigens more specific to M tuberculosis, and are not influenced by cross-reactivity to M bovis BCG and most NTM.7 However, there are limited data on the utility of IGRAs to diagnose M tuberculosis infection in persons from highly tuberculosis endemic settings. The two commercially available IGRAs include the ELISPOT-based T-SPOT.TB (Oxford Immunotec, UK) and the ELISA-based QuantiFERON TB Gold (Cellestis, Australia), with the in-tube form as the most recently available version, including TB 7.7 as an additional combined antigen. In the absence of a practical gold standard for M tuberculosis infection, exposure to an infectious tuberculosis index case has been used as a surrogate measure of infection and has been shown to correlate well with ELISPOT IFNγ responses in household contact and outbreak investigations.12 13 14 Direct comparisons of discordance between the two commercial IGRAs and the TST are limited, and there are few data on the comparison of both assays in relation to M tuberculosis exposure as a surrogate measure of infection and the influence of age.
We conducted a cross-sectional household contact study to assess the agreement of two commercially available IGRAs in relation to the TST and investigated the impact of M tuberculosis exposure and age on TST and IGRA responses to detect M tuberculosis infection.
Methods
Study setting
Our study was conducted in the Ravensmead/Uitsig (R/U) community in the Tygerberg District, Western Cape Province, South Africa, where the incidence of culture-confirmed tuberculosis in children aged ⩽13 years was 407/100 000 in 2004.15 The total tuberculosis notification rate was 841 per 100 000 in 2002,16 and the prevalence of HIV among patients with tuberculosis was 8% in 2005 (Cape Town City Health). R/U is a well-characterised poor urban community of predominantly mixed ethnicity, with both formal and informal housing structures, often on the same residential property. Multiple families therefore often share the same residential address. There is a high level of ongoing M tuberculosis transmission at the household and community level.17 In 2005 the calculated annual risk of M tuberculosis infection in R/U assessed through community-based school surveys was 3.5% among children aged 6–14 years, with 34.4% of children having a positive TST (⩾10 mm) (unpublished findings). BCG vaccine (Danish strain; 1331, Statens Serum Institute (SSI), Copenhagen, Denmark) is routinely given at birth.
Participants
From September 2005 through March 2006, HIV-uninfected children aged 0–5 years and adults aged ⩾15 years in recent household contact with a tuberculosis index case were recruited. Individuals were eligible if exposed to a pulmonary tuberculosis index case and excluded if they were acutely ill, diagnosed with HIV infection, had active tuberculosis or were receiving isoniazid or antituberculosis treatment. Women were excluded if they were pregnant. All children with a household index case were referred for isoniazid preventive therapy in accordance with South African National Tuberculosis Control Program guidelines; all tuberculosis suspects were referred for further evaluation.
Measures
Data were collected on age, gender, BCG vaccination status (scar or documentation of vaccination record) and M tuberculosis exposure. A household tuberculosis index case was defined as a person aged ⩾15 years with bacteriologically positive tuberculosis (sputum smear and/or culture positive) diagnosed at the R/U clinic during the previous 3 months and currently living in the same or neighbouring physical dwelling located on the same residential property. Caregivers and adult participants were interviewed to determine the participant’s extent of contact with the index case during a typical week. A previously published M tuberculosis contact score18 was modified for use in this study setting. The modified M tuberculosis contact score was based on the assumptions that the gradient of M tuberculosis exposure was a composite function of the infectivity of the index case, the duration of exposure and the proximity of exposure (table 1). The mean contact score was calculated for each participant. After exploration of cut-off values, the score was dichotomised as low (<4) vs high exposure (⩾4) based on the score distribution in the sample.
Mycobacterium tuberculosis contact score
Following phlebotomy (10 ml venous blood), a TST using 2 TU PPD RT 23 (Mantoux PPD, SSI) was placed on the volar aspect of the left forearm and read within 48–72 h using the ball-point pen and ruler method. TST reading by the study nurse was standardised through a large-scale community-based TST survey. A positive TST was defined as an induration of ⩾10 mm, in accordance with national guidelines.
Blood was transported at room temperature and processed within 3 h at the research laboratory. Laboratory analyses were blinded. Phlebotomy resulting in inadequate blood volumes, specimens not transported within the specified window period or clotted blood specimens were documented as “failed phlebotomy”. If blood volumes were inadequate, the T-SPOT.TB was preferentially completed.
The T-SPOT.TB and QuantiFERON TB Gold (QTF) tests were performed according to the manufacturers’ instructions using positive and negative controls. All T-SPOT.TB tests were read by the same laboratory technician using an automated spot counter (Zeiss, Germany). The manufacturers’ standard guidelines were used to define positive cut-off values for interpretation of IGRAs. HIV status was determined using a rapid screening test (AxSym, Abbott Diagnostics, Cape Town, South Africa) and confirmed by ELISA or by PCR in children aged ⩽18 months.
Data analysis
Data are expressed as frequencies and percentages for categorical variables and means for continuous variables. Agreement between tests was estimated using Cohen’s kappa (κ) coefficient, while also describing the pattern of disagreement (discordant results). To aid in the interpretation of agreement and disagreement, estimates of the prevalence of positive results are presented. These estimates were compared between diagnostic tests using the McNemar χ2 test for correlated proportions. The association between each diagnostic test and the M tuberculosis contact score (high vs low score) was estimated using logistic regression models, controlling for the potential confounding effect of age.
In addition to categorical representation of IGRAs based on manufacturers’ guidelines, individual and total antigen responses for T-SPOT.TB (ESAT-6 and CFP-10, spot count per 250 000 peripheral blood mononuclear cells) and IFNγ QTF antigen response (IU/ml) were described as continuous measures.19 Comparisons between children and adults were performed using the Pearson χ2 and Wilcoxon rank sum tests for dichotomous and continuous tests results, respectively. Receiver operating characteristic (ROC) curves were generated to compare individual continuous IGRA antigen responses in relation to the M tuberculosis contact score, which was used as a surrogate gold standard. Correlations were explored between T-SPOT.TB and QTF for the ESAT-6 and CFP-10 assay levels for children and adults using the Spearman rank correlation coefficient. The T-SPOT.TB spot count and QTF IFNγ IU/ml were both transformed to the natural log scale for graphical purposes. Missing data and indeterminate results were excluded from analyses.
Results
Eighty-two individuals were enrolled (29 children and 53 adults); 4 HIV-infected individuals (4.7%) were excluded from the study.20 Two children with symptoms were referred for further investigation and excluded from the analysis based on abnormal chest radiographs. The primary outcome measures and patient characteristics are summarised in table 2. The mean M tuberculosis contact score was significantly higher in children than in adults; 93% of children reported a high M tuberculosis contact score (⩾4) compared with 42% of adults. In 55.2% of children the tuberculosis index case was the parent or primary caregiver.
Clinical characteristics and measures of Mycobacterium tuberculosis infection in adults and children in recent household contact with a tuberculosis index case
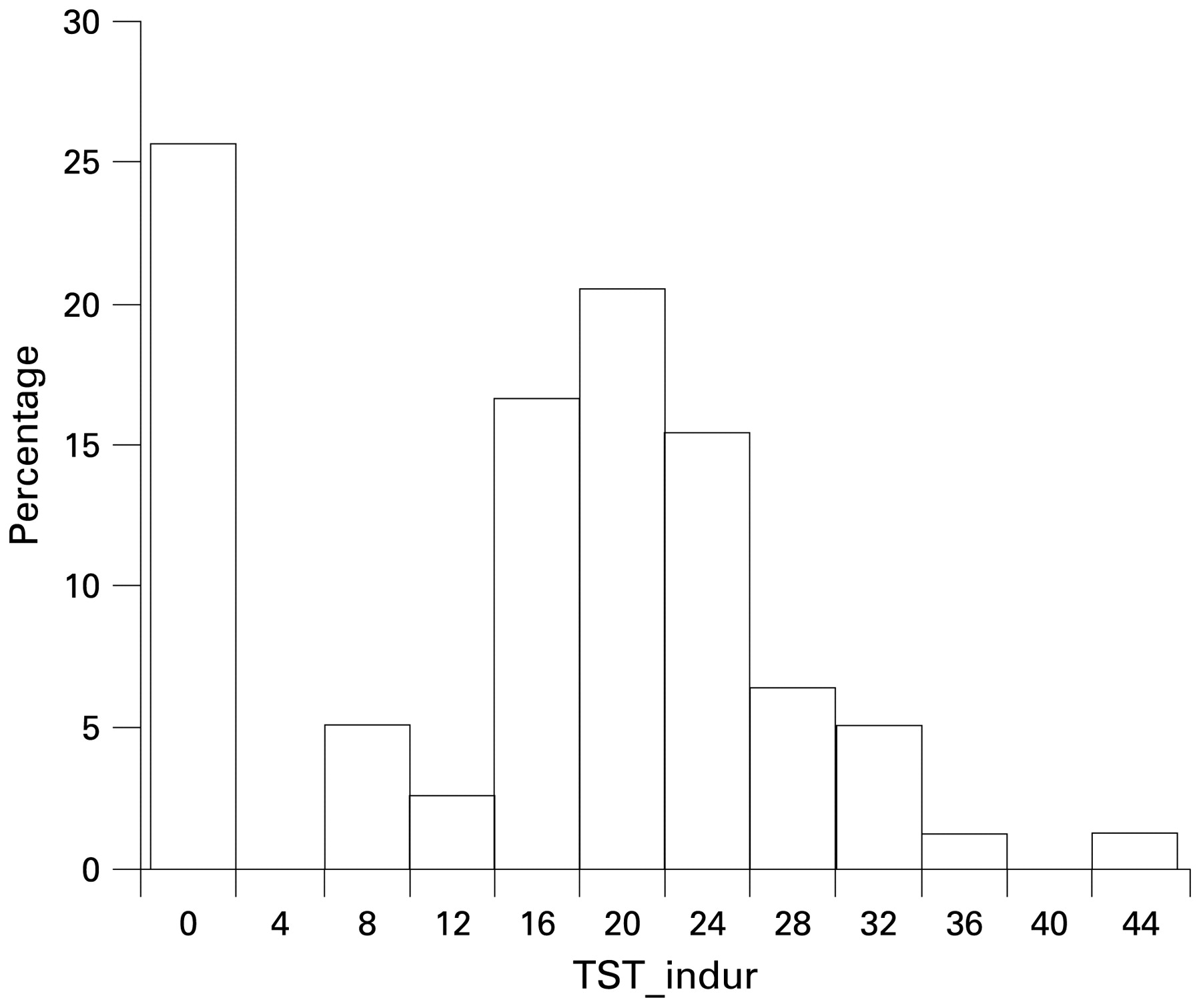
Results were available for the TST and T-SPOT.TB for the entire sample. Owing to inadequate blood volumes, a smaller sample of 74 individuals had QTF responses. The TST distribution in millimetres is shown in fig 1; the TST was positive in 69% of individuals (median values in children vs adults in those with TST >0 mm: 14.5 mm vs 19.0 mm). There was no significant difference between the mean size of induration between BCG-vaccinated and unvaccinated subjects (21.43 mm vs 19.93 mm, p = 0.070). None of the participants had a reported TST in the 6 months preceding enrolment. The TST was positive in significantly more adults than children (78.0% vs 53.6%, χ2 = 5.0, p = 0.02). Conversely, the T-SPOT.TB was positive in more children than adults (92.6% vs 66.0%, χ2 = 6.7, p = 0.01). QTF results were positive in adults and children (39.6% vs 44.4%, χ2 = 0.13, p = 0.72). The T-SPOT.TB produced indeterminate results in 1/28 children (3.6%) and the QTF in 3/21 children (14.3%). No indeterminate results were observed in adults.
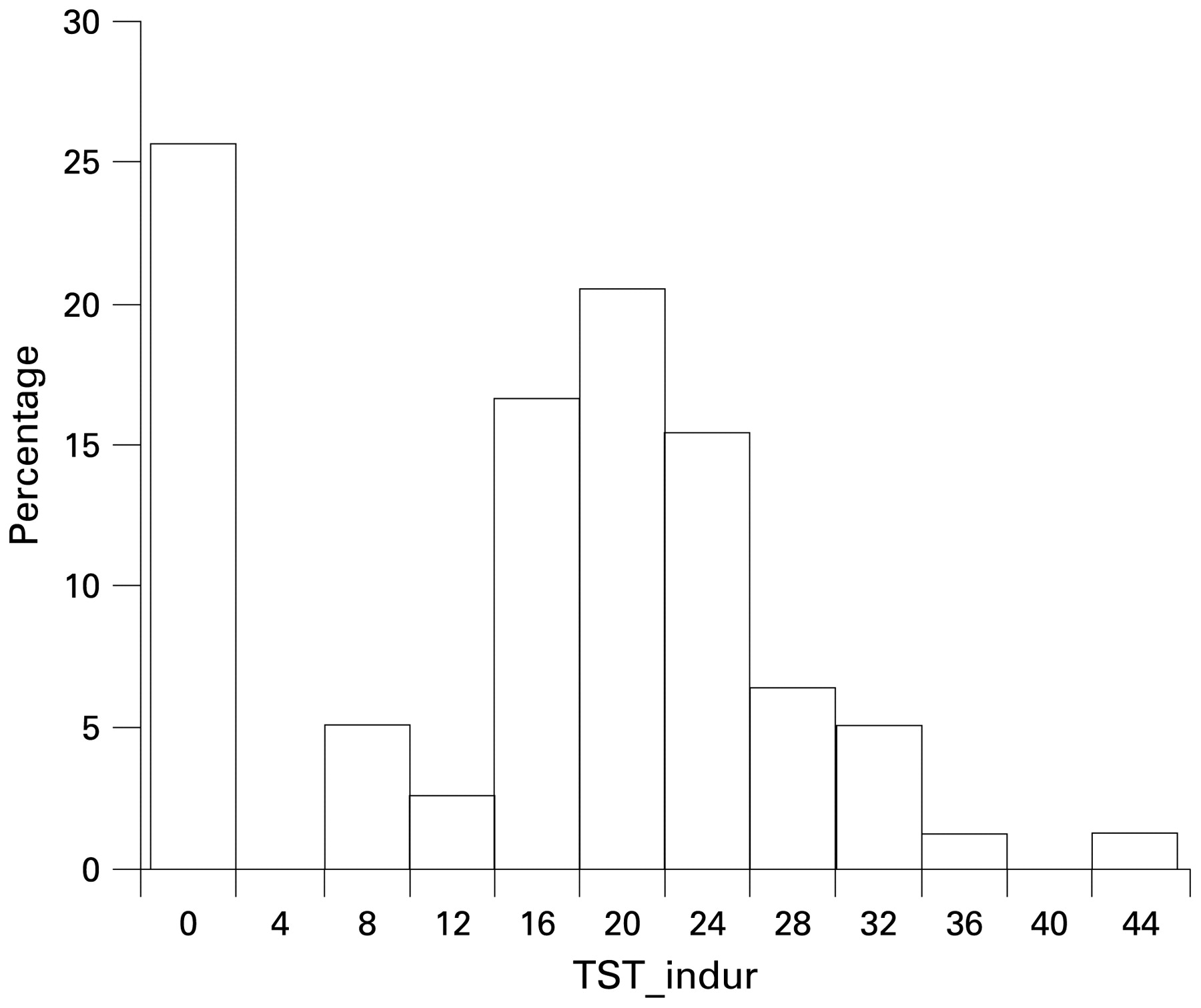
Mantoux tuberculin skin test distribution in HIV-uninfected adults and children in recent household contact with a tuberculosis index case. Mantoux tuberculin skin test (TST) induration in millimetres.
Discordant results between all three tests were common with percentage agreement ranging from 46.1% to 88.9% (table 3). Using different cut-off values for the TST did not improve the yield or test agreement significantly (proportion positive: 73.0%, 69.2% and 65.4% for TST cut-off values of 5, 10 and 15 mm, respectively, in all subjects).
Comparison of TST and IGRA responses in adults and children in recent household contact with a tuberculosis index case
Table 4 shows the relation between exposure to M tuberculosis and IGRA results. Participants with a high M tuberculosis contact score were at least seven times more likely to be T-SPOT.TB positive than those with a low score (odds ratio (OR) 62.42, 95% CI 7.67 to 508.69) regardless of age, and at least three times more likely to be QTF positive (OR 9.60, 95% CI 3.02 to 30.54). This relationship was confounded by age. The TST was not significantly associated with M tuberculosis exposure in unadjusted or adjusted regression models. Using a higher M tuberculosis exposure score cut-off value of 8 decreased the association between M tuberculosis exposure and measures of infection (data not shown). All children were BCG-vaccinated and had a BCG scar; in adults (data not shown), the presence of a BCG scar did not confound the relationship between exposure to M tuberculosis and test results.
Logistic regression of dichotomous measures of Mycobacterium tuberculosis infection in relation to exposure and age in adults and children in recent household contact with a tuberculosis index case
The mean (SD) T-SPOT.TB ESAT-6 response was higher than the CFP-10 response in all participants (111.7 (134.5) vs 26.6 (44.4); Wilcoxon sign test, p⩽0.001). In contrast, the mean (SD) QTF CFP-10 response was higher than the mean ESAT-6 response in all participants (5.1 (10.0) vs 1.5 (3.5); Wilcoxon sign test, p⩽0.001). There was a significant difference in the magnitude of the T-SPOT.TB ESAT-6 and CFP-10 spot counts between adults and children (mean (SD) ESAT-6 response in children 162.7 (144.0) vs 84. 8 (122.2) in adults; Wilcoxon sign test, p = 0.002). In contrast, there was no difference between T-SPOT.TB CFP-10 responses in adults and children (mean (SD) response 29.9 (54.6) vs 24.9 (38.5), respectively). The magnitude of the QTF ESAT-6 response was similar in children and adults (mean (SD) response 4.0 (4.6) vs 1.1 (3.0); p = 0.49); the mean (SD) QTF CFP-10 response in children was 8.4 (14.4) compared with 3.8 (7.6) in adults (p = 0.61). Exploration of correlation coefficients, although not significant, suggested an age-related correlation between QTF and T-SPOT.TB CFP-10 responses (adults r = 0.71; children r = 0.39; p = 0.10 for comparison of coefficients between groups) and a lesser correlation between QTF and T-SPOT.TB ESAT-6 responses (adults r = 0.34; children r = −0.06; p = 0.14 for comparison of coefficients between groups; figs 2 and 3).
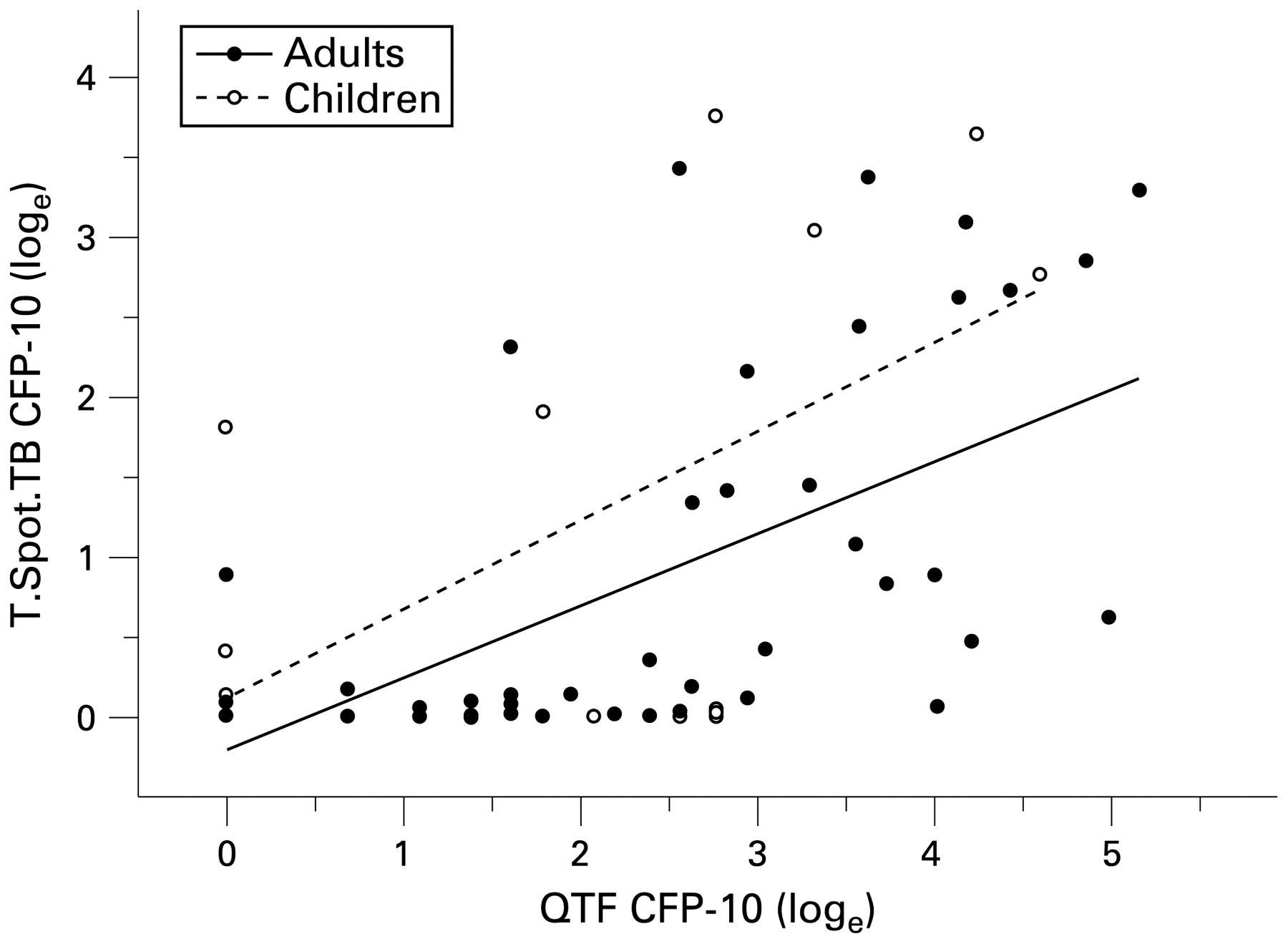
Correlation between interferon γ (IFNγ) culture filtrate protein 10 kD (CFP-10) responses measured by QuantiFERON TB Gold (QTF) and T-SPOT.TB in adults and children. Vertical axis: T-SPOT.TB CFP-10 IFNγ responses (spot count per 250 000 peripheral blood mononuclear cells); horizontal axis: QTF IFNγ CFP-10 response (IU/ml); both measures are reflected on the natural log scale. Spearman rank correlation coefficient for adults r = 0.71 and for children r = 0.39; p = 0.097 for comparison of coefficients between groups.

Correlation between interferon γ (IFNγ) early secretory antigenic target (ESAT)-6 responses measured by QuantiFERON TB Gold (QTF) and T-SPOT.TB in adults and children. Vertical axis: T-SPOT.TB ESAT-6 IFNγ responses (spot count per 250 000 peripheral blood mononuclear cells); horizontal axis: QTF IFNγ ESAT-6 response (IU/ml); both reflected on the natural log scale. Spearman rank correlation coefficient for adults r = 0.34 and for children r = −0.06; p = 0.135 for comparison of coefficients between groups.
ROC curves describe the sensitivity and specificity of ESAT-6 and CFP-10 responses compared with high M tuberculosis exposure (⩾4) (fig 4). T-SPOT.TB ESAT-6 responses appeared to offer the highest sensitivity and specificity of any single antigen (area under the curve (AUC) = 0.933). T-SPOT.TB CFP-10 individual responses were less sensitive and specific (AUC = 0.687). The combined ESAT-6 CFP-10 T-SPOT.TB response appeared to be largely influenced by the ESAT-6 component. The sensitivity and specificity of the QTF ESAT-6 and CFP-10 responses (AUC) were 0.721 and 0.825, respectively.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operating curves (ROC) for individual and mean combined early secretory antigenic target (ESAT)-6 and culture filtrate protein 10 kD (CFP-10) interferon γ (IFNγ) responses for T-SPOT.TB and Quantiferon-Gold (QTF) in adults and children in relation to high M tuberculosis exposure (contact score ⩾4). Individual antigen responses for T-SPOT.TB: panel A; ESAT-6, and panel B; CFP-10 spot count, and IFNγ QTF antigen response (IU/ml) to ESAT-6 and CFP10.
Discussion
There was a high prevalence of M tuberculosis infection in HIV-uninfected children and adults in this study population with documented recent household exposure to tuberculosis. We found significant discordance between TST, T-SPOT.TB and QTF. Participants with a high degree of exposure to M tuberculosis had a high risk of having a positive IGRA result, regardless of age. The high prevalence of infection is consistent with recently published data from adults in a neighbouring high incidence community in Cape Town where discordant results were also detected,21 although that study did not correlate test results with degree of M tuberculosis exposure or age.
Agreement between the three tests in children varied dramatically. Widely discrepant results between QTF and TST in children have been reported in both low and high incidence settings.22 23 24 The T-SPOT.TB was positive in a significantly higher proportion of children than the TST and the QTF. These results suggest that the T-SPOT.TB may be a more sensitive measure of M tuberculosis infection than the TST or QTF in children with recent exposure, and appeared to be largely driven by robust ESAT-6 responses. The most pronounced disagreement between the results in children was between the T-SPOT.TB and the TST or QTF, whereas the TST and the QTF had good agreement. Our data also suggest improved specificity of both IGRAs compared with the TST. This could be explained by the fact that TST responses in older individuals are continually boosted by a variety of recurrent exposures, including NTM25 and M tuberculosis. The clinical importance of these observed discordances is unknown. Studies incorporating serial follow-up measures in different populations will support further exploration of these differences and the predictive utility of IGRAs to identify acute and latent infection and the subsequent risk of progressing to active tuberculosis.
Children had a higher mean M tuberculosis contact score than adults, reflecting the importance of proximity of contact and the duration of exposure to M tuberculosis experienced by young children. In the majority of cases the index case was the child’s parent or primary caregiver, consistent with previous findings.26 A key consideration for the interpretation of our findings is that the majority of children had recent and significant documented household exposure, whereas many adults had less reported household exposure although they may have had previous or remote M tuberculosis exposure. Adults had a higher probability of being TST positive (78%) but a lower probability of being IGRA positive (66% for T-SPOT.TB vs 39.6% for QTF), suggesting higher IGRA specificity but lower sensitivity in the presence of recent exposure.
Based on ROC analysis, T-SPOT.TB ESAT-6 responses were more strongly associated with recent M tuberculosis exposure than CFP-10 responses. An interesting finding is that the mean T-SPOT.TB and QTF responses were different for ESAT-6 and CFP-10, with higher mean values observed for T-SPOT.TB ESAT-6 responses than for CFP-10 responses, but that higher QTF CFP-10 than ESAT-6 responses were observed. The ELISpot-based technique measures the number of IFNγ-producing cells while the ELISA technique (QTF) measures the accumulation of IFNγ over time. Since not every IFNγ-producing cell produces identical amounts of IFNγ, a linear relationship between production and numbers of producing cells cannot be expected. Therefore, despite the association between the ELISA and ELISpot results, there is no absolute correlation, as demonstrated by our results and those of others.27 Leyten et al have proposed that the two tests appear to differ in their sensitivity for detecting cells producing low levels of IFNγ, which may partly explain these observed discrepancies.28 Bennekov et al demonstrated that, in an ELISA-based assay, most of the IFNγ produced came from a subset of cells and that samples with similar ELISpot results could therefore have different ELISA results. In animal models this observation was also associated with different disease outcomes.29 Further studies are therefore needed to assess the clinical relevance of these findings.
Regression analyses showed that individuals with high M tuberculosis exposure were more likely to have a positive IGRA. This is consistent with a recent household contact study in Nigeria; children exposed to a smear-positive index case were more likely to be Quantiferon-in-tube positive than those with a smear-negative index case.30 Our data suggest that the use of an exposure gradient to M tuberculosis in high burden settings such as South Africa is feasible. Exposure gradients need to be further validated and refined in tuberculosis endemic settings to elucidate differences between risk factors for household and other sources of transmission. Our composite contact score allowed for multiple factors including smear status, duration and proximity of exposure. The enhanced performance of the T-SPOT.TB compared with the QTF as assessed through exploratory ROC analysis in relation to M tuberculosis exposure also requires further validation.
The consideration of age-related differences between IGRA test agreement in adults and children is important as test responses may be dependent on both age and recent degree of M tuberculosis exposure. Although our study had limited power to measure the impact of age on the relationship between M tuberculosis exposure and IGRAs, our results suggest that the odds of having a positive IGRA result increased when controlling for age. Chee et al have demonstrated different age-related responses to the T-SPOT.TB for the two antigens used in adults with M tuberculosis infection.31 Our results also indicate a potential age-related correlation between antigen responses. Potential mechanisms for these observations may include age-dependent immune l maturation.
This study is limited by its cross-sectional nature and its small sample size, as reflected in wide confidence intervals around effect estimates despite statistically significant results for main outcomes. Other limitations include the age distribution and lack of serial measures to assess discordant results and test reproducibility. Since this was a household contact study, we did not assess individuals without documented M tuberculosis exposure; future studies should incorporate the use of such control populations and should ideally include serial measurements of both exposure and infection. We do not report on findings in HIV-infected patients. ELISPOT-based IGRAs have been shown to be sensitive measures of M tuberculosis infection in HIV-infected individuals in endemic settings and also in those with decreased CD4+ T cell counts.20 21 32 33 The QTF was not completed in all children owing to inadequate blood volumes. Finally, although the QTF used in this study is still in use, a newer in-tube version which includes TB 7.7 as an additional antigen is currently being marketed and differences between responses measured by different generations of QTF test may be considerable.34 An important potential distinction which we have retained by using the QTF in the present study is the ability to distinguish between different antigen responses; this has been lost using the newer generation in-tube QTF which combines all three antigens.
In summary, we found that the T-SPOT.TB, QTF and TST were highly discordant in adults and children in recent household contacts. The T-SPOT.TB correlated better with high exposure levels in young child contacts. Larger community-based longitudinal studies with serial assessment of discordant results and accurate long-term outcome measures are essential to assess the predictive value of IGRAs for infection and disease in HIV-uninfected and infected children and adults. Further studies should also assess age-related individual IGRA antigen responses and the use of more comprehensive exposure gradients as a surrogate measure of infection.
Acknowledgments
The authors thank the study nurses, the TB clinic staff in Ravensmead and Uitsig, the patients and their families for their kind cooperation, the Cape Town City TB directorate and Dr Ivan Toms for permission to conduct this study, and Professor Mark Doherty, Statens Serum Institute, Denmark for helpful advice regarding technical aspects of the assays used in this study.
REFERENCES
Footnotes
Funding Supported by the South African National Research Foundation NRF Thuthuka TTK2006051500016 (ACH), NIH IK23-HD40982 (AMM) and the Bill and Melinda Gates Foundation through Grand Challenges in Global Health Grant 37772 (NNC, KS, GB, GW) and the Norwegian Centre or Cooperation in Higher Education (ACH, GW).
Competing interests None.
Ethics approval Informed consent was obtained for participation and HIV testing. Institutional approval was obtained from Stellenbosch University.