Article Text

Abstract
Background: The combination of cisplatin and etoposide (PE) has been a standard treatment for patients with poor-prognosis small cell lung cancer (SCLC). This non-inferiority design trial aimed to determine whether the combination of gemcitabine and carboplatin (GC) results in similar survival but is less toxic with better quality of life.
Methods: Previously untreated patients with SCLC with extensive disease or limited stage with poor prognostic factors were randomly assigned to six 3-weekly cycles of GC or PE.
Results: 241 patients (121 GC, 120 PE) were recruited, of which 216 (90%) had died. There was no difference in overall survival (HR 1.01, 95% CI 0.77 to 1.32). Median survival with GC and PE was 8.0 and 8.1 months, respectively. Median progression-free survival was 5.9 months with GC and 6.3 months with PE. Grade 3 or 4 myelosuppressions were more frequent with GC (anaemia: 14% GC vs 2% PE; leucopenia: 32% GC vs 13% PE; thrombocytopenia: 22% GC vs 4% PE), but these were not associated with increased hospital admissions, infections or fatalities. Grade 2–3 alopecia (68% PE vs 17% GC) and nausea (43% PE vs 26% GC) were more frequent with PE. Patients given GC received more chemotherapy as outpatients (89% GC vs 66% PE of treatment cycles). In QoL questionnaires, more patients receiving PE reported being upset by hair loss (p = 0.004) and impaired cognitive functioning (p = 0.04).
Conclusions: GC is as effective as PE in terms of overall survival and progression-free survival and has a toxicity profile more acceptable to patients.
Trial registration number: ISRCTN 39679215
Statistics from Altmetric.com
The prognosis of extensive disease and poor-prognosis limited stage small cell lung cancer (SCLC) remains disappointing. Less than 10% of these patients survive 2 years despite treatment with combination chemotherapy.1 With no clear survival advantage for any particular regimen, reduction in treatment-related toxicity and improved quality of life (QoL) become important clinical goals.
Over the last decade several new cytotoxic drugs have been identified with good activity against SCLC. Gemcitabine (Gemzar, Lilly) has been shown to have clinical activity in untreated and previously treated patients and preclinical studies showed synergy between gemcitabine and cisplatin.2–4 The favourable toxicity warrants further investigation in combination regimens.
Current standard therapy for poor-prognosis SCLC is most commonly cisplatin plus etoposide (PE) which produces a response rate of approximately 60–70% and a median survival of 6–12 months.1 However, major problems with cisplatin treatment are administration time and significant symptomatic non-haematological toxicity. Because our goals were symptom and disease control, we chose carboplatin because it is less toxic than cisplatin in terms of emesis, neurotoxicity, renal damage and electrolyte disturbance and it can be given as outpatient treatment without special hydration.5 Carboplatin monotherapy has also been shown to be active in SCLC7 and, when combined with etoposide, achieved similar survival benefit with less toxicity than PE.6 7
The present non-inferiority trial aimed to determine whether the newer regimen of gemcitabine plus carboplatin (GC) is less toxic and associated with better QoL than PE chemotherapy.
METHODS
Patients
This open-label study was conducted in 26 cancer centres/units in the UK and was approved by all relevant ethics committee and undertaken according to the Declaration of Helsinki. Eligibility included chemotherapy naive patients with a histological or cytological diagnosis of SCLC, measurable or evaluable disease, and those with either extensive disease or limited disease with poor prognostic factors (ECOG performance status ⩾2 and/or alkaline phosphatase >1.5 times the upper limit of normal range according to Souhami et al8). Patients were required to have adequate bone marrow reserve (white blood cell count ⩾3.0×109/l, platelet count ⩾100×109/l and haemoglobin ⩾10 g/dl) and renal function adequate for chemotherapy (>60 ml/min when measured by 51Cr-EDTA or 24 h urine collection or >50 ml/min when calculated by the Cockcroft and Gault formula9). Patients were ineligible if they had a history of prior malignancies (unless there was no evidence of disease for at least 3 years or the tumour was a non-melanoma skin tumour), symptomatic brain metastases or life expectancy of <8 weeks.
In this study “limited disease” was defined as confined to one hemithorax but including mediastinal extension with contralateral hilar lymphadenopathy, ipsilateral supraclavicular lymphadenopathy and ipsilateral pleural effusions (not cytologically proven).10
Randomisation and treatment
This was a multicentre randomised trial comparing a 3-weekly schedule of six cycles of GC or PE to assess survival, response rate, toxicity and quality of life. Patients were registered and centrally randomised at the Cancer Research UK and UCL Cancer Trials Centre (London) by minimisation to receive GC or PE. Stratification was by participating centre, disease stage (extensive or limited poor prognosis), ECOG performance status (0/1 or 2/3), age (<70 or ⩾70 years) and sex.
Intravenous gemcitabine 1200 mg/m2 was given on days 1 and 8, and carboplatin was given intravenously at a dose of area under the curve (AUC) 5 calculated according to the Calvert formula on day 1 after the gemcitabine. Where possible the glomerular filtration rate was calculated using 51Cr-EDTA or by a 24 h urine collection. Where neither of these methods was possible, the Cockcroft and Gault method was used.9 As this method underestimates by approximately 10%, the dose of carboplatin was calculated using AUC 6. Patients in the PE arm received intravenous cisplatin 60 mg/m2 on day 1 with hydration and intravenous etoposide 120 mg mg/m2 on day 1 with 100 mg twice daily given orally on days 2 and 3, which was the standard London Lung Cancer Group (LLCG) regimen.11
It was recommended that all patients received intravenous granisetron 3 mg and intravenous dexamethasone 8 mg before administration of each chemotherapy and intravenous metoclopromide 20 mg before administration of gemcitabine on day 8. All patients were to receive prophylactic antibiotics on days 8–21 of each cycle to minimise the risk of infection.12
Recommended dose modifications were based on the time of retreatment full blood counts. If the white blood count was between 1.5 and 2.99×109/l or the platelets were between 50 and 99.9×109/l, all drugs were reduced to 75%. If the white blood count was <1.5×109/l or the platelets were <50×109/l, the cycle was delayed for 1 week. Nadir counts were not collected except for GC patients returning on day 8 for gemcitabine administration. Administration of gemcitabine on day 8 was omitted if the white blood count was <2×109/l or the platelets <50×109/l. Cisplatin and gemcitabine doses were reduced for renal function by 50% if the glomerular filtration rate was 40–60 ml/min and omitted if it was <40 ml/min.
Patients with limited stage disease who achieved a partial/complete response received thoracic radiotherapy, and those with a complete response also received prophylactic cranial irradiation (PCI).
Assessments
Patients were assessed at baseline, before each visit for chemotherapy, every 4 weeks for the first year and 8-weekly thereafter. At each visit, assessments included history, physical examination, ECOG performance status, chest radiography, full blood count, liver function tests and measurements of urea, creatinine, electrolyte levels and radiology assessments. Minimum baseline imaging consisted of chest radiography, chest and abdominal CT scans, and a CT scan of the brain and isotope bone scan if clinically indicated.
The response was assessed according to the WHO criteria13 and was evaluated prior to each cycle of chemotherapy by chest radiography. Examination of CT scans was repeated after cycles 3 and 6 and when clinically indicated. Metastatic sites were reassessed after the last cycle of chemotherapy by the most appropriate method.
QoL was assessed using the EORTC QLQ-C30 questionnaire14 with the lung cancer module LC-17 as well as the LLCG daily diary card (DDC).15 Patients completed the questionnaire prior to randomisation, before each chemotherapy and at the first two follow-up visits. DDCs were completed by the patient at baseline and then daily until 3 weeks after the last cycle of chemotherapy.
Toxicity was assessed using the National Cancer Institute Common Toxicity Criteria Version 2.0 (revised 1994).
Statistical analysis
The primary outcome measure was overall survival; secondary outcome measures were progression-free survival, tumour response, toxicity and QoL. The aim of the trial was to demonstrate whether GC would not be inferior to PE in terms of survival (non-inferiority trial), but would be less toxic with better QoL. With an estimated 1-year overall survival rate of 20% in the PE group calculated from an earlier study,11 the trial was designed to reliably exclude (80% power, 95% CI) the possibility that GC was more than 10% worse at 1 year, which required 193 events and planned accrual of 241 patients.
The planned design incorporated a review by an Independent Data Monitoring Committee analysing response and toxicity data from the first 40 patients treated with GC. The trial was only to continue to completion if predefined criteria were met. These were: (1) at least 15 responses among the first 40 patients (ie, if the true response rate was at least 50% there would be less than a 5% chance of <15 responses); and (2) not more than 30% (95% CI 20% to 40%) of cycles 2–4 should be delayed because of toxicity.
Duration of overall survival was calculated from the date of randomisation to the date of death from any cause. Progression-free survival was calculated from the date of randomisation to date of the first progression or date of death, whichever occurred first. The log-rank test was applied to compare the Kaplan-Meier curves for overall survival and progression-free survival. The Cox proportional hazard regression model adjusted by the stratification factors (ECOG performance status, age, sex and stage) also applied. The χ2 test for interaction was implemented to assess the relative differences in treatment in different subgroups of patients. Tumour response and toxicities during treatment were compared using the standard χ2 test or Mann-Whitney test.
EORTC QoL questionnaires were analysed using recommended scoring scales and items. Forms with <80% of questions completed and scales with <50% of items completed were excluded. Raw scores for the scales and items of the questionnaires were compared between baseline and specified time points using the Mann-Whitney test. Scores were also compared by calculation of the area under the score-time curve over the treatment period. Symptom scores recorded on DDCs were plotted to display the changes over time. The mixed model for repeated measurements using PROC NLMIXED in SAS (SAS Institute, Cary, North Carolina, USA) was applied in an exploratory manner for the two treatment comparisons.
All analyses were done on an intention-to-treat basis except for the analyses of response, toxicity and DDCs. The latter analyses were restricted to patients who received at least one cycle of allocated treatment. All p values are two-sided.
RESULTS
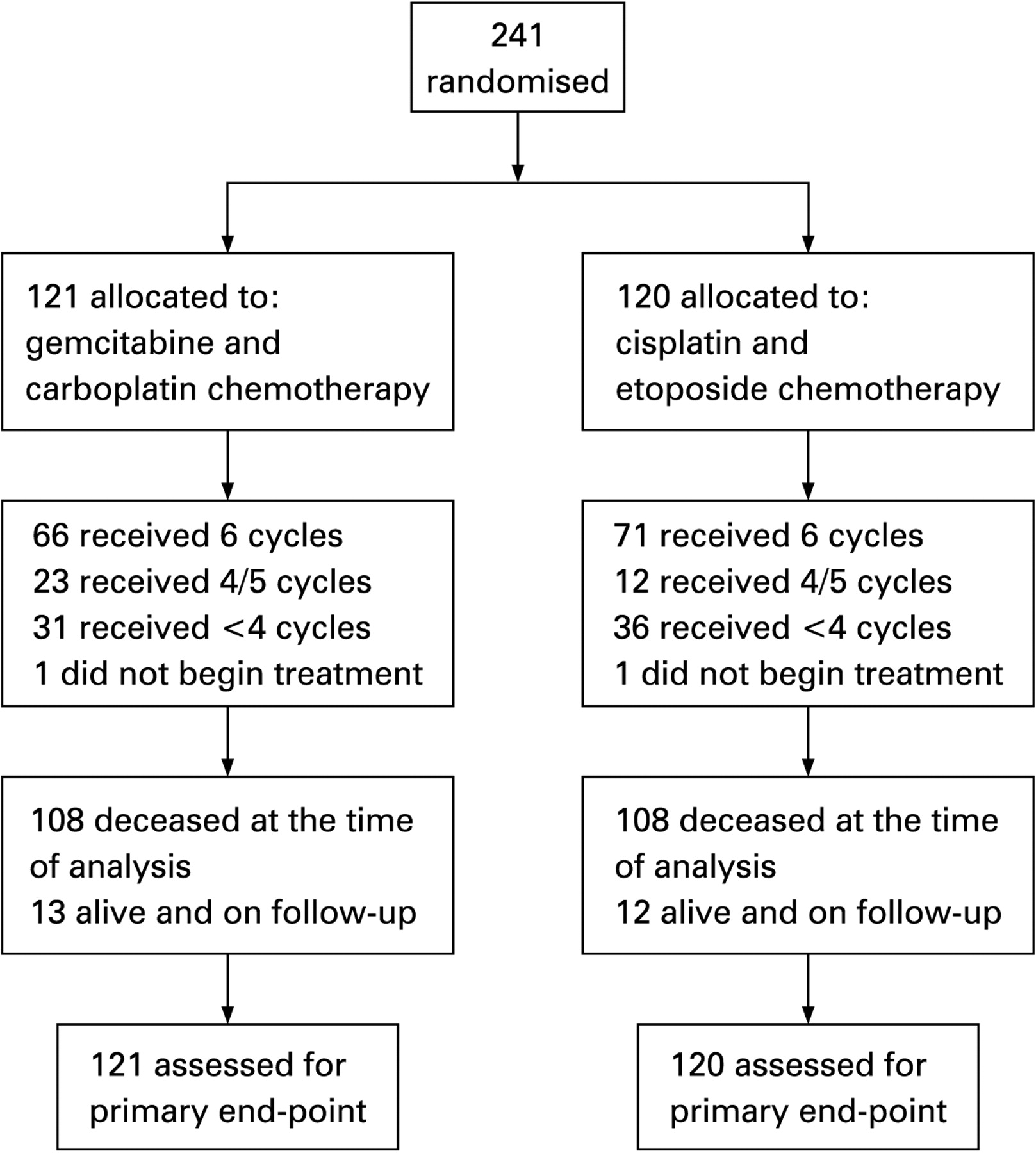
From January 1999 to September 2001, 241 patients from the UK were entered into the study (fig 1); 121 patients were randomised to the GC arm and 120 patients to the PE arm. The two arms were well balanced for age, sex, performance status and stage (table 1).

Treatment
Most of the patients completed the intended six cycles of chemotherapy (66 (55%) GC; 71 (59%) PE); 74% of patients on the GC regimen completed at least four cycles compared with of 69% of patients treated with PE, but this difference was not statistically significant. The main reasons for not completing all six cycles (55 GC, 49 PE) were progressive disease (25 GC, 21 PE), toxicity (16 GC, 9 PE) and clinical decision/patient refusal (8 GC, 10 PE). Two patients did not receive any protocol treatment, one patient on GC due to inadequate renal function and one on PE due to progressive disease.
Treatment delays were seen in 24% of cycles in patients treated with GC compared with 14% of cycles in those receiving PE, the major reason being haematological toxicity. Dosage modifications were seen in 33% of cycles in patients treated with GC and 25% of cycles in those treated with PE. These differences occurred mainly because the day 8 chemotherapy on the GC schedule doubled the opportunities for dose modification. Excluding day 8 omissions, only 22% of cycles in GC were modified. The main reason for dose modification was haematological toxicity (50%) and renal toxicity (15%) for patients receiving GC, and renal toxicity (53%) and haematological toxicity (19%) for those treated with PE. Renal toxicity resulting in platinum dose modification occurred in 13% of patients receiving PE and 5% of those receiving GC (difference 7%, 95% CI 10% to 3%).
Consolidation thoracic radiotherapy to the chest was given to 30 patients receiving GC (18 PCI) and 37 patients treated with PE (23 PCI).
Toxicity
There were 561 evaluable chemotherapy cycles in the GC arm and 542 cycles in the PE arm.
Haematological toxicity
There was a significantly higher incidence of grade 3 and 4 haematological toxicity in patients on GC than in those on PE (table 2): anaemia (14% vs 2%); leucopenia (32% vs 13%) and thrombocytopenia (22% vs 4%). These were not associated with increased hospitalisation, neutropenic sepsis, bleeding or deaths.
Non-haematological toxicity
Non-haematological toxicities were in general similar in each arm with the exception of nausea, alopecia and rash (see table S1 in online supplement). Patients receiving PE experienced significantly more grade 2–3 nausea (43% vs 26%, p = 0.04) and 50% more grade 2–3 alopecia (68% vs 17%, p<0.0001) than those on GC. There was a higher incidence of rash in patients treated with GC (28% vs 14%) which was generally mild with grade 2–3 seen in 10% of patients on GC and 2% on PE. There was no difference between other recorded toxicities including infection.
Hospital admissions for chemotherapy
Forty-nine patients (41%) on GC were admitted overnight for their first cycle of chemotherapy compared with 70 patients (59%) treated with PE. The total number of cycles given on an outpatient basis was 496 (89%) for GC and 356 (66%) for PE (difference 23%, 95% CI 18% to 28%). The number of patients admitted at least once to hospital for chemotherapy was 52 (44%) for GC and 73 (62%) for PE (difference 22%, 95% CI 9% to 35%) with median (range) nights of 2 (1–22) for GC vs 3 (1–39) for PE (p = 0.019, Mann-Whitney test).
Survival
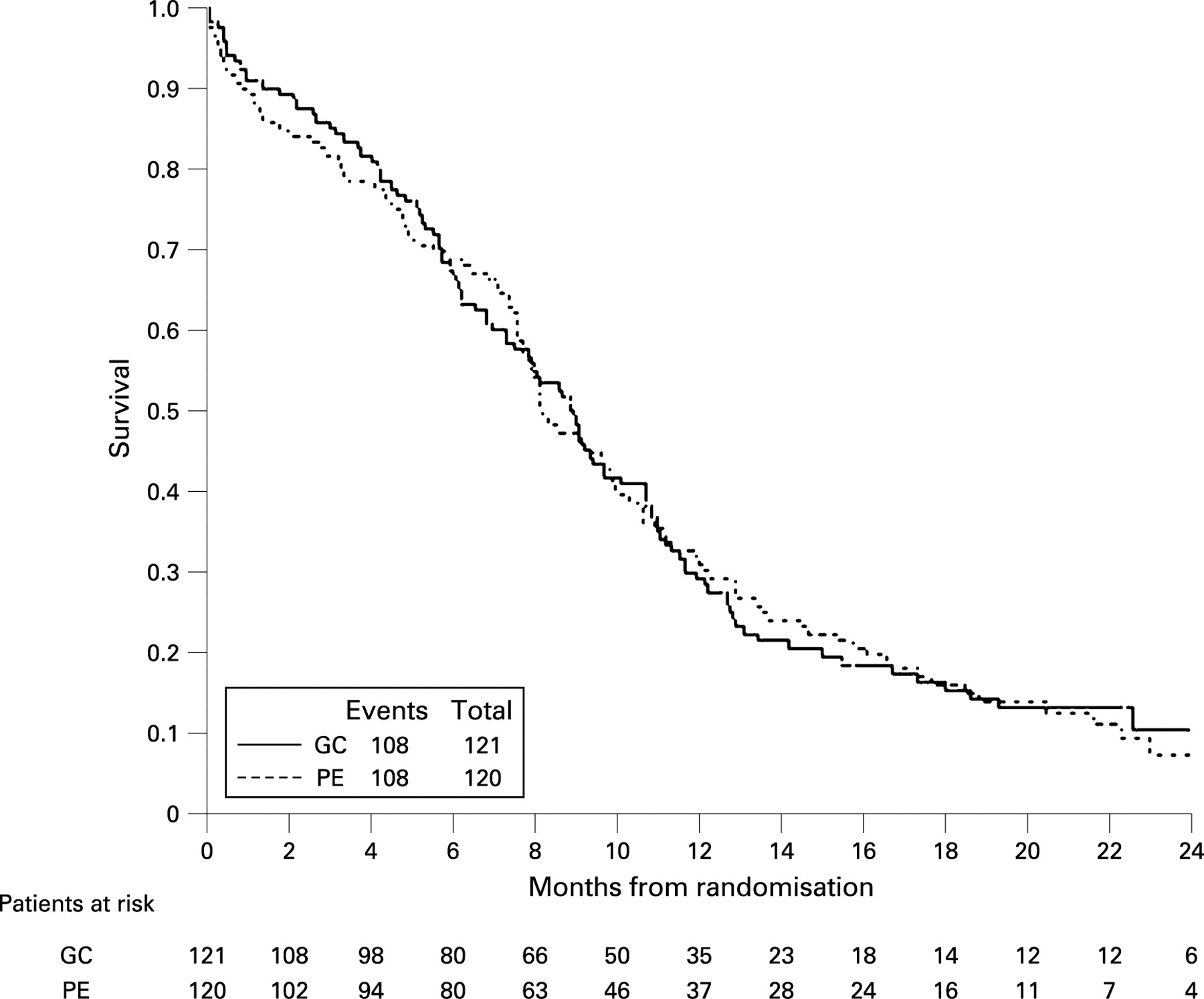
At the time of analysis a total of 216 patients (90%) had died. There was no difference in overall survival (hazard ratio (HR) 1.01, 95% CI 0.77 to 1.32, p = 0.96, log rank test; fig 2). Median overall survival was 8.0 months with GC and 8.1 months with PE (absolute difference 0.1 month, 95% CI −1.84 to 2.56). The 1-year overall survival rates were 30.6% and 31.0% for those receiving GC and PE, respectively (absolute difference 0.4%, 95% CI −9.6% to 9.7%). The result was unaffected by adjusting for age, sex, ECOG performance status and stage (HR = 0.997, 95% CI 0.76 to 1.31, p = 0.98, Cox model). There was no difference in progression-free survival (HR = 1.07, 95% CI 0.82 to 1.41, p = 0.61, log rank test; fig 3). Median progression-free survival was 5.9 months in the GC arm and 6.3 months in the PE arm, which was unaffected by adjustment forage, sex, ECOG performance status and stage (HR = 1.08, 95% CI 0.82 to 1.42, p = 0.58, Cox model).

{kind=link}
{kind=link}
{kind=link}
Exploratory subgroup analyses indicate that there was no difference in treatment effect on overall survival or progression-free survival in subgroups defined by age, sex, performance status and stage. The subgroup analysis for stage and Kaplan-Meier plots by stage and treatment are shown in fig 1 in the online supplement. Median overall survival was 12 months in patients with limited disease and 7.6 months in those with extensive disease. Median progression-free survival was 7.7 months in patients with limited disease and 5 months in those with extensive disease.
Response
Patients who received at least one cycle of chemotherapy were eligible for response assessment (see table 2 in online supplement). The best overall response rates (complete (CR) and partial (PR)) were similar for both regimens (63.3% (12.5% CR + 50.8% PR) in patients treated with GC and 62.7% (11.0% CR + 51.7% PR) in those treated with PE (p = 0.92).
Causes of death
The main cause of death was SCLC and the proportion was similar for both treatment regimens (91% GC, 92% PE). There were two treatment-related deaths in the GC arm and one in the PE arm; this difference was not statistically significant.
Quality of life (QoL)
Compliance with QoL questionnaires at baseline and throughout the active treatment was >60% but subsequently declined, so the analysis is restricted to the treatment period. There was no significant difference in compliance at the different assessment points between the two treatment arms. All scales/items measured by the EORTC QLQ-C30 and LC17 questionnaires were well balanced across the two treatment groups at baseline. The most common symptoms reported as “quite a bit” or “very much” at baseline were fatigue in 58% of patients, dyspnoea in 51%, insomnia in 48%, coughing in 45%, appetite loss in 43% and pain in 41%. Comparison of changes in scores between baseline and 6 weeks showed significant advantages for GC over PE with respect to hair loss (p<0.0001) and being upset by hair loss (p = 0.004). There was also some indication of improved cognitive functioning (p = 0.047) in patients treated with GC. Sixty-six per cent of patients on PE reported experiencing “quite a bit” or “very much” hair loss at week 6 compared with only 12% patients in the GC arm, and this persisted at week 18 (p<0.001). This difference was also seen in the AUC analysis (p<0.001).
DDCs were completed for up to 18 weeks. Compliance was high initially but decreased over time. Over 50% of patients completed more than 70% of planned diary card days. There was no evidence of any difference between the two treatment arms.
DISCUSSION
This is the first randomised study comparing GC with PE chemotherapy for patients with poor-prognosis SCLC. This study found that GC chemotherapy achieved a survival rate, response rate and time to progression equivalent to PE, which has been the standard since the mid 1980s.16–18 Our study was designed to exclude a 10% difference in overall survival. This is a large difference to be considered for a non-inferiority trial. However, based on the observed HR of 1.01 and 95% confidence interval of 0.77 to 1.32 for overall survival, our conclusion is unlikely to change even with a much larger sample size.
The GC regimen has a different toxicity profile from PE. Grade 2–3 nausea occurred in 43% of PE-treated patients but in only 26% of GC-treated patients. More significantly, 68% of PE-treated patients developed grade 2–3 alopecia compared with only 17% of GC-treated patients. This is an important finding as chemotherapy-induced alopecia is ranked as one of the most troubling side effects, especially in women, and can have profound psychosocial and QoL consequences resulting in anxiety, depression, a negative body image, lowered self-esteem and a reduced sense of well-being.19 Indeed, our QoL results found that more patients in the PE arm were upset by hair loss and cognitive functioning. In contrast, more frequent grade 3 and 4 haematological toxicity was seen with the GC schedule, but this was largely asymptomatic and was not associated with increased grade 3 or 4 infection, bleeding or death. This increased frequency is likely to be the results of haematological assessment collected on all patients on GC returning for day 8 gemcitabine whereas nadir counts were not collected for PE-treated patients. The overall mortality rate associated with chemotherapy-related toxicity (neutropenic sepsis in all patients) was low (1.24%) with three treatment-related deaths.
GC is a much easier regimen to administer without the need for pretreatment and post-treatment hydration associated with PE, thereby avoiding a hospital stay for several hours or even overnight (62% of patients treated with PE were admitted for overnight chemotherapy compared with 44% of patients treated with GC). PE can be a problematic regimen to administer in elderly poor-performance patients with extensive SCLC in whom the aim of treatment is symptom and disease control and the use of cisplatin may be poorly tolerated, such as those with substantial baseline renal impairment, hearing loss, peripheral neuropathy or other serious medical comorbidities. Although 44% of patients given GC were treated as inpatients, this largely occurred for cycle 1 of the treatment when patients were often already in hospital for investigations and symptom control.
The efficacy of GC is supported by a phase II trial involving 69 patients with extensive SCLC using a similar 3-week GC regimen with a slightly reduced dose of gemcitabine (1100 mg/m2). The median survival rate, estimated 1-year survival rate and response rate reported were 9.2 months, 33% and 43%, respectively.20 Another phase II trial in 88 patients with extensive SCLC which evaluated a regimen of cisplatin (75 mg/m2) instead of carboplatin and gemcitabine 1250 mg/m2 on days 1 and 8 obtained a median survival of 9 months, 1-year survival rate of 28% and a response rate of 56%.21 A third study of 70 patients using cisplatin 70 mg/m2 and gemcitabine 1000 mg/m2 on days 1 and 8 achieved a comparable rate of 10 months for median survival and a 63% response rate.22 These data support our randomised findings that GC is an effective regimen. An initial Japanese-based phase III trial reported a survival advantage in favour of irinotecan plus cisplatin compared with cisplatin plus etoposide in extensive SCLC,23 but recent results from two other studies found no survival advantage and excessive toxicity was noted in patients with performance status 2.24 25
Our findings that GC is as effective as PE in terms of survival and progression-free survival but is associated with a toxicity profile more acceptable to patients are noteworthy. We suggest that GC is a worthwhile regimen to consider for the treatment of poor-prognosis SCLC, particularly in patients with extensive disease and/or those who wish to avoid hair loss, nausea and other cisplatin-related toxicity. The greater cost of GC will soon be less relevant as gemcitabine comes off patent in early 2009 and as carboplatin is already off patent.
Acknowledgments
The authors thank all the participating centres and investigators who helped recruit patients to the trial: RHT/St Bartholomew’s, London: R Rudd, J Steele, P Wells, M Evans; Birmingham Heartlands NHS Trust Birmingham: D Ferry, D Richardson; Addenbrookes NHS Trust, Cambridge: D Gilligan, S E Old, L Magee; Guy’s & St Thomas’ NHS Trust, London: P G Harper, P Ellis, J Prendiville, A Poole; Walsgrave Hospital NHS Trust: M Hocking, D Halliman, S Williams, L Wimbush; Ninewells Hospital/Perth Royal Infirmary: E M Rankin, B Massie, D Forbes; Oldchurch (Havering) Hospital: J Shamash, C Dunphy; North Middlesex Hospital: T Eisen, H Bridle; St George’s Hospital, London: J Mansi, R Woodhill, J Diffley, F Thompson, R Schurstein; Weston Park Hospital: P C Lorigan, M Q Hatton; Stobhill Hospital: R Milroy, R Jones, J McPhelim, J Graham; North Devon Hospital: M Napier, B Holbrook; Leicester Royal Infirmary: K O’Byrne, F Shields; Royal Free Hospital: A Jones; Gloucestershire Oncology Centre, 3 Counties Cancer Networks: D Farrugia, A Ashton, M Walker; Chelsea & Westminster Hospitals: M Bower, P Shah, S Cox; Southend Hospital: A Lamont, C W Trask, M Philips; Norfolk & Norwich University Hospital/James Paget Hospital, Norfolk: C Martin, J Beety; Sunderland Royal Hospital: H W Clague, J Anderson; University College London Hospitals Trust: S M Lee, S G Spiro, A Leary; North Devon and Royal Devon & Exeter Hospitals: M Napier; Torbay Hospital: J Goldman, A Goodman, F Roberts; Essex County Hospital: P Murray, B Sizer, S Heatley; Mount Vernon Hospital: E Lyn; Royal Berkshire Hospital: P Rogers, C Lewis. Trial centre staff include the following: Lindsay James, Paul Smith, Nicole Gower, Susan Wan, Katy O’Donnell.
REFERENCES
Supplementary materials
web only appendix 64/1/75
Files in this Data Supplement:
Footnotes
▸ Additional tables and a figure are published online only at http://thorax.bmj.com/content/vol64/issue1
Funding: The trial was funded by The London Lung Cancer Group (registered charity no. 1074994) which received an educational grant from Lilly Oncology to support this trial. The trial was supported by the National Cancer Research Institute (NCRI).
Competing interests: None.
Ethics approval: The trial was approved by all relevant ethics committees and was undertaken according to the Declaration of Helsinki. All patients provided written informed consent.