Article Text

Statistics from Altmetric.com
P1 VARIATION IN THE PREVALENCE OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE IN ENGLAND BY OCCUPATIONAL GROUP: AN ANALYSIS OF THE HEALTH SURVEY FOR ENGLAND
A Darnton, J Osman, S Wilkinson. Health and Safety Executive, Bootle, UK
Introduction and Objectives: While smoking is the dominant cause of chronic obstructive pulmonary disease (COPD), surveys of various populations suggest the attributable fraction due to occupational exposure to dusts, gases and fumes is of the order of 15%. Although studies have implicated exposures to specific agents in certain industries in its causation, information about the overall distribution of occupational COPD in the UK is limited. The aim of this study was to compare the prevalence of spirometry-defined COPD among occupational groups after accounting for smoking and age using data from cross-sectional surveys of the English population.
Methods: The Health Survey for England is an annual population survey of approximately 20 000 individuals. Data on lung function, age, sex, smoking habit and occupation were available from four recent surveys carried out in 1995, 1996, 1997 and 2001. We classed subjects as having COPD if FEV1/FVC was less than the predicted lower limit of normal values corresponding to the bottom 5% of the population. We then calculated age and smoking-adjusted COPD prevalence ratios for occupational groups relative to managers after pooling the survey data and by fitting log linear models with a binomial error distribution.
Results: Three major groups within the Standard Occupational Classification 1990 (SOC90) had statistically significantly elevated COPD prevalences relative to managers: personal and protective service occupations (PR 1.23, 95% CI 1.02 to 1.48), plant and machine operatives (PR 1.21, 95% CI 1.06 to 1.39) and craft and related occupations (PR 1.15, 95% CI 1.02 to 1.31). Power to detect differences in prevalence at a more detailed level was limited. Nevertheless, five SOC90 minor groups had significantly elevated COPD prevalences in relation to managers (construction trades, printing and related trades, road transport operatives, other transport and machinery operatives, and other occupations in sales and services). Several others groups had elevated prevalences of borderline statistical significance.
Conclusions: These results provide evidence for variations in COPD prevalence between occupational groups, after accounting for age and smoking differences, which are consistent with increased risks of COPD due to occupational exposures in a number of craft, construction and transport-related occupations. They should help direct future research and intervention activities.
P2 THE SEVERITY AND IMPACT OF SYMPTOMS IN THE MORNING IN THOSE WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE, AS ASSESSED BY QUESTIONNAIRE
1MR Partridge, 2N Karlsson, 3I Small. 1Imperial College London, NHLI Division, Charing Cross Hospital, London, UK, 2Health Economics and Outcomes Research, AstraZeneca R&D, Mölndal, Sweden, 3Peterhead Health Centre, Peterhead, UK
Introduction and Objectives: Chronic obstructive pulmonary disease (COPD) is subject to circadian changes although little is known about symptoms due to COPD in the morning. Qualitative research suggests that COPD patients report being very breathless in the morning and struggle with essential morning activities, such as rising, washing and dressing. This study aimed to quantify the extent of morning symptoms and their impact upon morning routines and quality of life.
Methods: Quantitative internet interviews were conducted with 803 COPD patients from the EU and the USA (⩾40 years, not diagnosed with asthma before 40 years), of whom 289 had severe COPD (⩾1 exacerbation in the last 12 months, regular use of a prescribed COPD medication and assessment of breathlessness >3 using the modified MRC breathlessness questionnaire). Patients completed an on-line questionnaire examining the nature, extent and impact of morning symptoms due to COPD. Results were age-adjusted to the general population.1
Results: Night time and morning were reported as being the worst times of the day for COPD symptoms in severe and non-severe COPD patients (see table); in both time periods, this was more pronounced in the severe subgroup (p<0.05). Their most commonly reported morning symptoms were shortness of breath (78%), coughing up phlegm (63%) and persistent/recurring coughing (60%). Approximately 50% of severe patients experienced these symptoms immediately after waking on all/most days. Nearly three-quarters (73%) of severe COPD patients regarded problems associated with morning routines as bothersome, with 96% indicating that morning routines took longer than they used to. As a result, 84% adapted the way they did some/all of their routines. Morning activities most affected by severe COPD were walking up/down stairs, putting on shoes/socks, making the bed, dressing, showering/bathing and drying (86%, 66%, 63%, 60%, 57%, 56%, respectively).
Discussion: Most COPD patients indicate morning as the time when symptoms are particularly severe. In those with severe COPD shortness of breath is the most frequently reported symptom and this impacts greatly on morning routine and quality of life.
P3 A NEW QUESTIONNAIRE TO ASSESS ACTIVITIES OF DAILY LIVING IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE?
PS Albert, L Davies, J Currie, P Parry, PMA Calverley. University Hospital Aintree, Liverpool, UK
Reduced self-reported physical activity in chronic obstructive pulmonary disease (COPD) is related to the risk of hospitalisation (Garcia-Aymerich et al. Thorax 2003) and mortality (Yohannes et al. Age Ageing 2002). Activities of daily living (ADL) in these patients are usually assessed by subjective questionnaire, the London chest ADL (LCADL) and Nottingham extended ADL (NEADL) questionnaires being validated in COPD. However, we noted that many COPD patients found it difficult to self-complete these questions. Moreover, the total scores do not allow for particular activities that the patient would not have undertaken, regardless of the chest condition. To address this we devised an 18-item questionnaire relating to ADL in COPD patients—the Aintree COPD ADL (ACADL) questionnaire, based on patient interviews, feedback on existing questionnaires and literature review. The score is calculated once activities that the patient would not do (even with healthy lungs) have been excluded. A higher score indicates worse ADL limitation. Another novel feature is the inclusion of a photograph of a street, where the patient is asked to judge their walking distance.
62 stable COPD patients (not previously involved in developing the ACADL), mean (SD) age 67.6 years (9.0), mean FEV1 1.01 litres (0.38), 43.4% predicted (16.6) were asked to complete the ACADL, LCADL, NEADL, St George’s respiratory questionnaire (SGRQ). Six-minute walk (6MW) distance was assessed using a standardised protocol. 20 patients repeated the questionnaires 3 months after their first attendance, without significant change in treatment or participation in a rehabilitation programme.
The ACADL score correlated with the other questionnaires and with 6MW. The intraclass correlation at test–retest was ACADL 0.90 (95% CI 0.73 to 0.96), LCADL 0.72 (0.42 to 0.87), NEADL 0.89 (0.78 to 0.95), SGRQ 0.91 (0.82 to 0.96).
We have described a new questionnaire for measuring ADL in COPD, which patients can complete independently, correlates well with exercise capacity and other validated questionnaires, and shows good day-to-day repeatability. This questionnaire should be easier to apply in routine clinical practice.
P4 DEPRIVATION, RURALITY AND THE USE OF HOME OXYGEN IN ENGLAND AND WALES
1GC Donaldson, 2G Esmond, 3I Balfour-Lynn, 4PMA Calverley, 5R Garrod, 6M Morgan, 1JA Wedzicha. 1University College London, London, UK, 2Barnet PCT, London, UK, 3Royal Brompton Hospital, London, UK, 4University of Liverpool, Liverpool, UK, 5St George’s Hospital, London, UK, 6University Hospitals of Leicester NHS Trust, Leicester, UK
A new service for the supply of domiciliary oxygen started on 1 February 2006 with delivery and maintainence undertaken by four companies (Air Products, Allied Respiratory, BOC and Linde). Subsequently, the BTS established for the first time a database of home oxygen users in England and Wales. We examined the database to see whether living in the countryside in contrast to urban areas affected the use of home oxygen and whether patients from deprived socioeconomic areas were more or less likely to be prescribed oxygen.
Patients were linked by postcode to lower super output area estimates of rurality and deprivation using the Office of National Statistics list of postcodes in February 2007. Urban areas were defined as settlements with a population of 10 000 or more. The index of deprivation was a weighted score using income, employment, health deprivation and disability, education, skills and training, barriers to housing and service, crime and living environment in 2004 (http://www.communities.gov.uk/archived/general-content/communities/indicesofdeprivation/216309/).
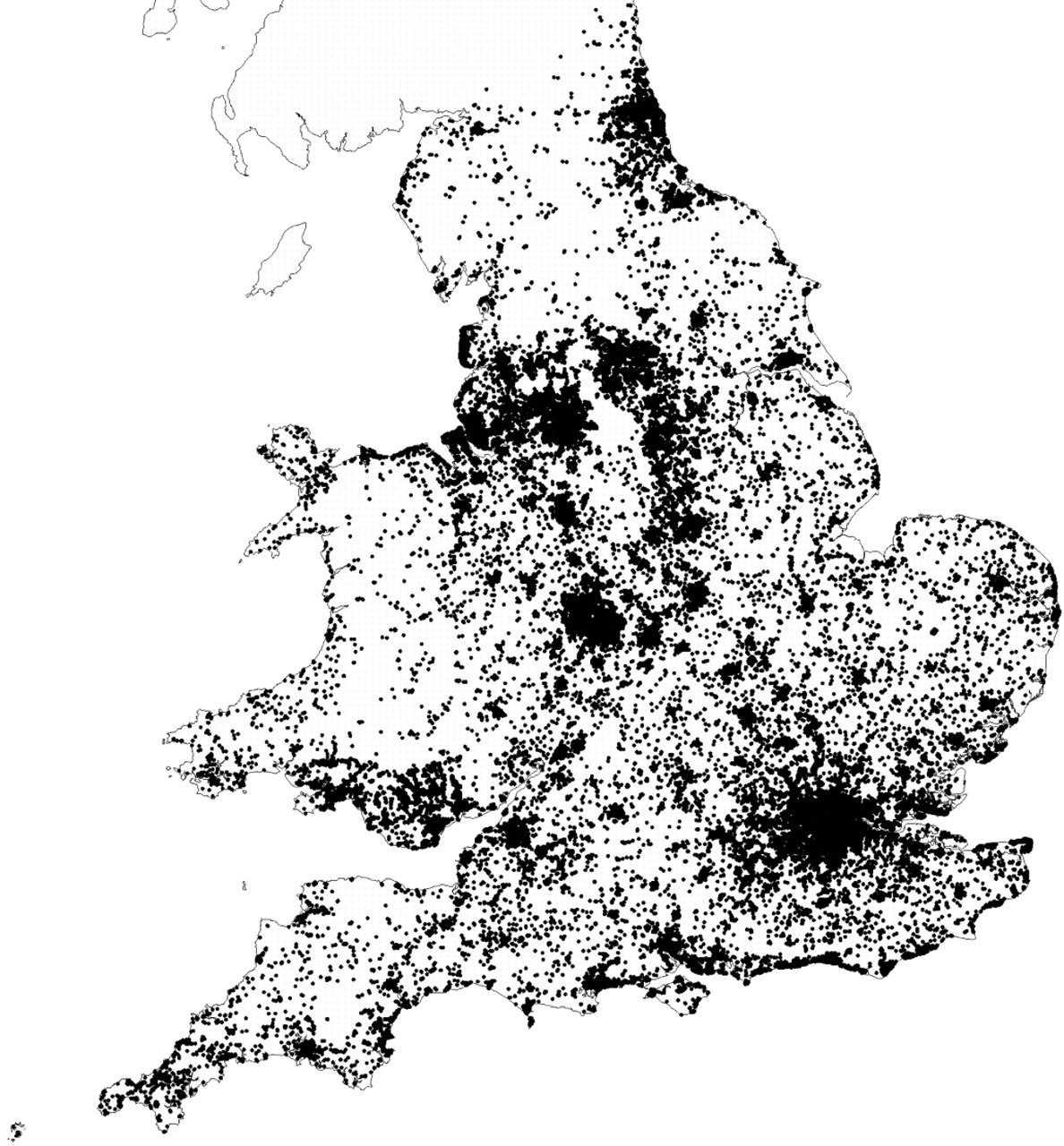
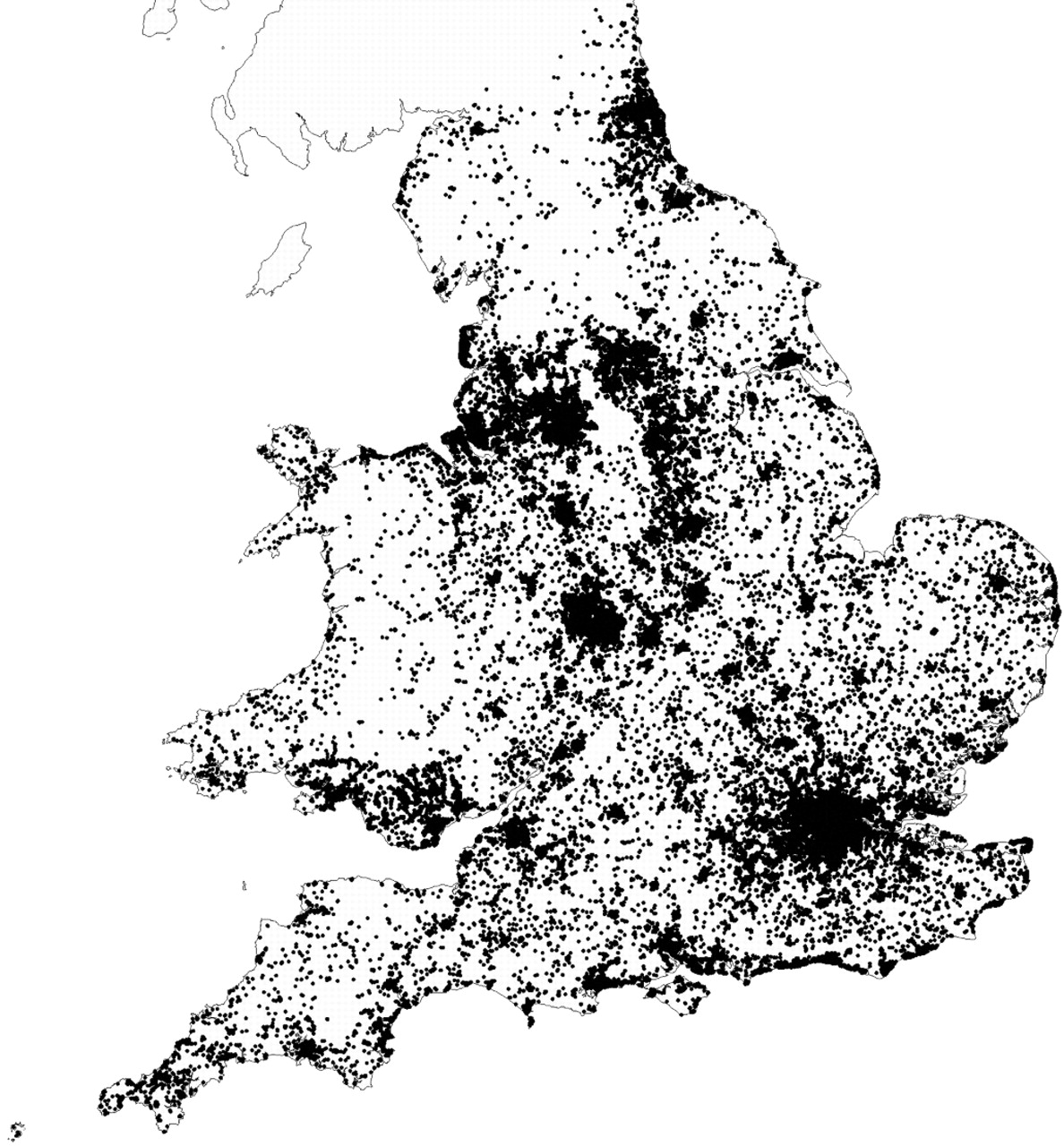
In total, 86 630 patients were on domiciliary oxygen in England and Wales during June 2007. Dates of birth were missing for 1728 patients (1.99%). Of the remainder, there were 3734 (4.4%) paediatric patients and 81 168 (93.7%) adult patients over 17 years of age. All patients had a postcode recorded, but 873 could not be matched due mainly to uncertainty over coding.
The figure shows that most patients were located in the major conurbations. We found no difference in the prevalence of home oxygen use between rural (mean 1.85 adult users/1000 people—all ages) and urban areas (1.86 users per 1000; p = 0.60). The number of adult home oxygen users per 1000 population was highest in the most deprived areas (rho 0.91, p<0.001). This finding possibly reflects the higher incidence of smoking in the more socioeconomically deprived areas. Chronic obstructive pulmonary disease was the most common clinical condition recorded on the home oxygen order form, involving 62.0% of adults on the three oxygen modalities.
Living in the countryside or in socioeconomic deprivation does not reduce a patient’s chances of receiving home oxygen.
Funding: Funded by the Department of Health.
P5 PATIENTS’ PERSPECTIVES ON AMBULATORY OXYGEN: ADVANTAGES AND DRAWBACKS
UG Hill, T Cotter. James Paget University Hospital, Great Yarmouth, Norfolk, UK
Introduction: Ambulatory oxygen is prescribed for patients with chronic respiratory disease who experience exertional dyspnoea and desaturation. In our experience, a substantial proportion of patients who may be suitable for portable oxygen decline its use, a finding that has been substantiated by other researchers.1
Aim: The objective of this survey was to assess patients’ perspectives on ambulatory oxygen, in particular with regard to practical aspects such as weight and transportation of cylinders, desired improvement in exercise tolerance and perceived disadvantages of portable oxygen.
Methods: Over a period of 4 months (April–July 2008), we asked patients with chronic obstructive pulmonary disease (COPD) who reported significant exertional dyspnoea but were not currently using portable oxygen to complete a questionnaire on the perceived advantages and drawbacks of ambulatory oxygen when they attended the respiratory clinic. The questionnaire also included a 10-point functional respiratory score, validated for the assessment of disabilities in patients with COPD. We excluded patients who met criteria for long-term oxygen treatment. Overall, 30 patients completed the questionnaire and results were analysed in a blinded fashion as to the identity of the patient (summarised in the table).
Results: With regard to the practical aspects of portable oxygen, 87% (26/30) of patients would prefer the lightweight to the standard cylinder. 67% (20/30) of patients wanted an alternative to the shoulder bag, such as a trolley (9/20) or a rucksack (11/20). 60% (18/30) of patients expected an improvement in exertional dyspnoea through the use of ambulatory oxygen and desired a mean increase in walking distance of 240 m. The latter expectation is likely to be unrealistic, as other researchers have only shown an increase in walking distance of ∼50 m.1 Interestingly, only 37% (11/30) of patients thought that the use of portable oxygen would enable them to be more active, with 53% (16/30) not being sure and 10% (3/30) of patients not expecting a change in activity levels. Perceived disadvantages of ambulatory oxygen related to the transportation of cylinders (23%, 7/30) and the fear of being embarrassed and stigmatised (17%, 5/30).
Conclusion: This survey has highlighted patients’ concerns about ambulatory oxygen. Addressing these matters may enable more patients to benefit from the use of portable oxygen.
References
P6 SOCIOECONOMIC STATUS IS AN INDEPENDENT FACTOR FOR SMOKING CESSATION IN PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE: A POPULATION-BASED OBSERVATIONAL STUDY
1C Lomas, 2M Al-Khairalla, 2J Winter. 1University of Dundee, Dundee, UK, 2NHS Tayside, Dundee, UK
Introduction: In 2006 the British Thoracic Society highlighted the relationship between social inequality and lung disease. Smoking cessation is the single most important factor in the management of chronic obstructive pulmonary disease (COPD) but there have been few studies investigating factors affecting smoking cessation in COPD patients. Our aim was to investigate factors that may be related to smoking status. We hypothesised that patients with a lower socioeconomic status would be more likely to continue smoking.
Methods: This large population-based observational study used a pre-existing database of COPD patients. We investigated if there was any relationship between smoking status and deprivation category (DEPCAT). We also examined other variables contained in the database. A postal questionnaire was randomly sent out to 300 COPD patients to assess smoking behaviour.
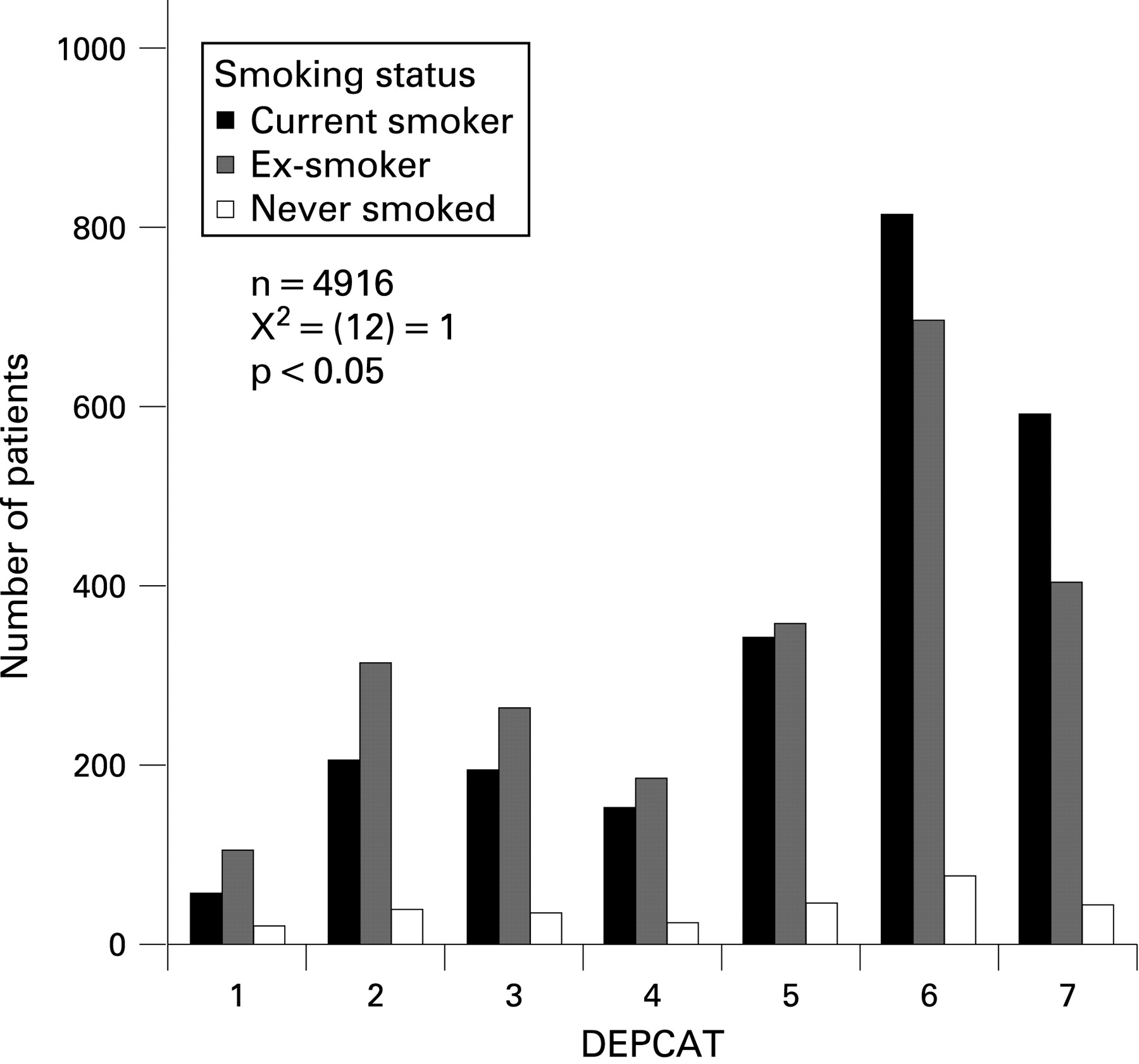
Results: The results of this study clearly demonstrate that socioeconomic status has a significant impact on the smoking status of COPD patients. Deprived groups had a higher prevalence of COPD and a higher proportion of current smokers compared with patients from more affluent groups (N = 4916, χ2 = (12) = 114.73, p<0.05). Female gender and increased hospital anxiety and depression scores were also associated with being a current smoker. Women, current smokers and those from a lower social class had significantly higher anxiety and depression scores. Factors associated with being an ex-smoker were affluent DEPCAT group, male gender, increasing age and hospitalisation. Ex-smokers had less airway obstruction. The postal questionnaire showed that 78% of ex-smokers used willpower alone to stop smoking. Knowledge of having COPD had no effect on smoking status.
Conclusions: The study confirms the social inequalities that contribute to the health inequalities seen in COPD. Deprived groups had a higher prevalence of COPD and a higher proportion of current smokers. Anxiety and depression may be risk factors linking socioeconomic status and smoking status, especially in women. This paper gives an insight into why some patients with COPD continue to smoke. Health providers should note these factors when running smoking cessation services.

P7 DOES INTENSE EDUCATION OF NURSING STAFF MAKE AN IMPACT ON SMOKING CESSATION ADVICE GIVEN TO INPATIENTS?
HS Hill, S Direkze, S Hussein, N Barmania, JT Samuel, DK Mukherjee, B Yung. Basildon and Thurrock University Hospitals NHS Foundation Trust, Basildon, Essex, UK
Background: Smoking cessation advice is often neglected in secondary level care. Inpatient smoking cessation counsellors are often unavailable. We wanted to establish whether intensive smoking cessation training for nurses in targeted acute medical wards affected the quality of smoking cessation advice given.
Method: In May 2007 a snapshot survey of inpatients and staff was performed before England became smoke free. This addressed smoking status of patients and staff, awareness of smoking cessation services and delivery of smoking cessation advice. In June 2008 the nursing staff on three targeted medical wards (respiratory, cardiology, endocrine) were given 3 weeks of intense training on smoking cessation practice and these wards were surveyed a month later to assess the impact.
Results: 537 patients and staff were surveyed in 2007, of which 93 (17%) were smokers. In 2008, 99 patients and staff were surveyed on the three wards, of which 26 (27%) were smokers. All the patients were adults. In both surveys female smokers were the majority, 56% and 65%, respectively, for both years. In 2007 only 31% of patients received smoking cessation advice during admission, in 2008 this was 88%. Moreover in 2008, 47% of the smoking cessation advice given was by nurses compared with none in 2007. There was no significant difference in the number of smokers wanting to quit in 2007 and 2008 (67% and 69%, respectively). Paradoxically, when questioned about referral to smoking cessation services only 23% requested referral in 2008 compared with 52% in 2007.
Conclusion: This survey demonstrates that intense education of nursing staff can have an impact on smoking cessation advice given on medical wards. Whether this effect will continue is being studied. The availability of an inpatient smoking cessation counsellor to educate staff in hospital and patients may be of benefit.
P8 RESULTS OF THE THIRD BTS NATIONAL SURVEY OF SMOKING CESSATION SERVICES
1L McAlpine, 2KE Lewis, 3R Sharrock, 3RJ Allcock, 4BTS Tobacco Committee. 1Monklands Hospital, Airedale, UK, 2Prince Philip Hospital, Llanelli, UK, 3Queen Elizabeth Hospital, Gateshead, UK, 4British Thoracic Society, London, UK
Background: In 2001 and 2003 the BTS surveyed the provision of smoking cessation services in UK hospitals. We carried out a third survey in January 2008.
Methods: A short paper questionnaire was posted to a nominated chest physician at all 261 hospitals in the UK at the end of December 2007 together with a stamped return envelope. Physicians were asked to indicate whether their hospital has a smoking cessation specialist or had access to community-based smoking cessation services. Supplementary questions explored whether the specialist was full or part-time, what follow-up was offered and what outcomes were recorded. Surveys were returned to the authors in early 2008.
Results: The overall response rate (68.6%) was lower than in the previous surveys (83%, 2001; 90.8%, January 2003). Those responding reported an overall increase in the number of smoking cessation services in UK hospitals, although marked regional differences persist (ranging from 100% of hospitals providing a service to only 20% provision) and some had lost their service. The figure shows the proportion of respondents in each health region who answered “yes” to the question: “Is there a smoking cessation counsellor/officer/nurse in your hospital?”
Conclusions: Provision of hospital-based smoking cessation services has improved in the UK but there are still areas where provision is suboptimal.

{kind=link}
{kind=link}
{kind=link}