Article Text

Statistics from Altmetric.com
S133 BETA CRYPTOXANTHIN LEVELS CORRELATE WITH LUNG FUNCTION IN MIDDLE-AGED MEN
1KM McClean, 2JS Elborn, 2F Kee, 2J Woodside, 2IS Young. 1Royal Victoria Hospital, Belfast, UK, 2Queen’s University, Belfast, UK
Background: Beta cryptoxanthin is one of the pro-vitamin A carotenoids and is found in many yellow/orange fruits and vegetables. It is known to be an antioxidant and is reported to be a good biomarker of fruit and vegetable intake. We hypothesised that levels of serum beta cryptoxanthin would be related to FEV1.
Methods: From 1991 to 1994, 2745 men aged 50–59 years were recruited into the Belfast arm of the Prospective Epidemiological Study of Myocardial Infarction (PRIME). 2010 of these men were rescreened at 10 years. In this study we describe the cross-sectional analysis of the 1208 men who had a valid spirometry trace (ERS/ATS criteria) and plasma sample at follow-up. Beta cryptoxanthin levels were measured using HPLC analysis. FEV1 values at 10 years were modelled using simple linear regression, and adjusted for age, height, body mass index, smoking history, cholesterol level and social status.
Results: The men had a mean age of 64.4 years and 36.9% had never smoked. Serum beta cryptoxanthin levels were positively correlated with FEV1 (r = 0.23, n = 1208, p<0.001). In the crude analysis, for each nanomole per litre increment in serum beta cryptoxanthin levels, FEV1 was 2.22 ml greater (95% CI 1.60 to 2.75). Following adjustment for covariates, for each nanomole per litre increment in serum beta cryptoxanthin levels, FEV1 was 1.26 ml greater (95% CI 0.78 to 1.75, p<0.001).
Conclusion: Serum beta cryptoxanthin levels are positively correlated with FEV1 in this cohort of middle-aged men from Northern Ireland. This suggests that in this population a moderate increase in serum beta cryptoxanthin levels (achievable by a modest increase in dietary intake of fruit and vegetables) may have a protective effect on lung function.
S134 DIETARY PATTERNS AND ADULT ASTHMA: POPULATION-BASED CASE–CONTROL STUDY
1Mr Bakolis, 1Dr Hooper, 2Dr Thompson, 1Dr Shaheen. 1Respiratory Epidemiology and Public Health Group, National Heart and Lung Institute, Imperial College London, London, UK, 2World Cancer Research Fund International, London, UK
Introduction and Objectives: Epidemiological studies of diet and asthma have focused largely on relations with intakes of individual nutrients and foods or food groups and few studies have examined associations with dietary patterns. The main aim of this paper is to determine whether dietary patterns are related to asthma and related outcomes in adults.
Methods: We carried out a population based case–control study of adults aged 16–50 years in Greenwich, south London. Information about usual diet was obtained by food frequency questionnaire and we used principal components analysis to define five dietary patterns. We used logistic and linear regression, adjusting for confounding factors, to relate these patterns to asthma, asthma severity, rhinitis and chronic bronchitis in 601 cases and 856 controls.
Results: There were no statistically significant associations between dietary patterns and asthma or severity of asthma after controlling for confounders. Dietary patterns I (characterised by a high intake of fish, salad vegetables, pasta, couscous and vegetable dishes) and III (associated with high intake of chips, processed meats, crisps, fried snacks, chocolate bars, sponge puddings, ketchup and cola) were positively associated with chronic bronchitis after adjusting for potential confounders. Dietary pattern II (which loaded highly on tomatoes and fruits) was positively associated with rhinitis (adjusted odds ratio per quintile increase of pattern score 1.75 (95% CI 1.08 to 3.27) (see table).
Conclusions: We have not found any relation between dietary patterns and adult asthma. The findings for chronic bronchitis and rhinitis were unexpected and require replication.
S135 TRENDS IN FIRST HOSPITALISATION FOR CHRONIC OBSTRUCTIVE PULMONARY DISEASE IN MEN AND WOMEN IN SCOTLAND, 1991–2006
M Gillies, J Lewsey, H Starkie, A Briggs, M Shepherd, K MacIntyre. University of Glasgow, Glasgow, UK
Background: We describe the changing pattern of first hospitalisation for chronic obstructive pulmonary disease (COPD) in men and women in Scotland over a 15-year period.
Methods: The Scottish Morbidity Record was used to identify all first hospitalisations in adults aged 35 years and over in Scotland where COPD was coded in the principal diagnostic position at discharge from 1991 to 2006. Annual age and sex-specific rates of first hospitalisation were calculated using denominator data from the 1991 and 2001 censuses, with interpolation and extrapolation for the inter-census years. Direct standardisation was carried out using 2001 census data. Rates over time were modelled using Poisson regression.
Results: There were 80 242 first hospitalisations for COPD in Scotland between 1991 and 2006; 41 522 (52%) were in women. The mean age at admission in men was invariant over time at 70.5 years (SD 10.5). In women the mean age at first hospitalisation rose from 69.9 years (10.6) in 1991 to 70.5 years (11.5) in 2006 (p = 0.031). Age standardised rates of first hospitalisation for COPD (per 100 000 population) increased in men from 175 (95% CI 167 to 182) in 1991 to 227 (218 to 235) in 1993, before falling to 176 (169 to 183) in 2006. In women rates increased from 124 (118 to 129) in 1991 to 217 (210 to 224) in 1999 before falling to 185 (178 to 192) in 2006. No significant change in the relative rate (RR) of first hospitalisation for COPD (2006 vs 1991) was found in men, RR 1.00 (0.81 to 1.24). However, a non-significant trend towards a reduction in RR in men aged 75 years and over was observed. In women the RR of first hospitalisation (2006 vs 1991) was 2.85 (2.68 to 3.02) overall, with increases observed across all age groups.
Conclusions: Despite an ageing population rates of first hospitalisation for COPD in men in Scotland appear to have stabilised. Indeed, a trend towards falling rates in elderly men is reported. Rates in women have more than doubled over the study period. However, there is some evidence that these may have peaked.
S136 WHAT SMOKING PREVALENCE CAN TELL US ABOUT HEALTH INEQUALITIES (OR VISA VERSA?)
K Tocque. North West Public Health Observatory, Centre for Public Health, John Moores University, Liverpool, UK
Introduction: Despite smokefree legislation and continuing declines in smoking prevalence, smoking remains the largest single killer in England: with approximately 85 000 deaths from smoking-related diseases each year. Effective targeting of local interventions to reduce smoking prevalence requires identification of communities who smoke the most but this intelligence is often lacking. It is time consuming and often prohibitively expensive to collect robust information on peoples’ behaviours. Population segmentation enables “types” of people and places to be identified that can help the targeting of communities with particular health needs.
Objective: To apply population segmentation methods to identify local communities at greatest risk of smoking-related diseases
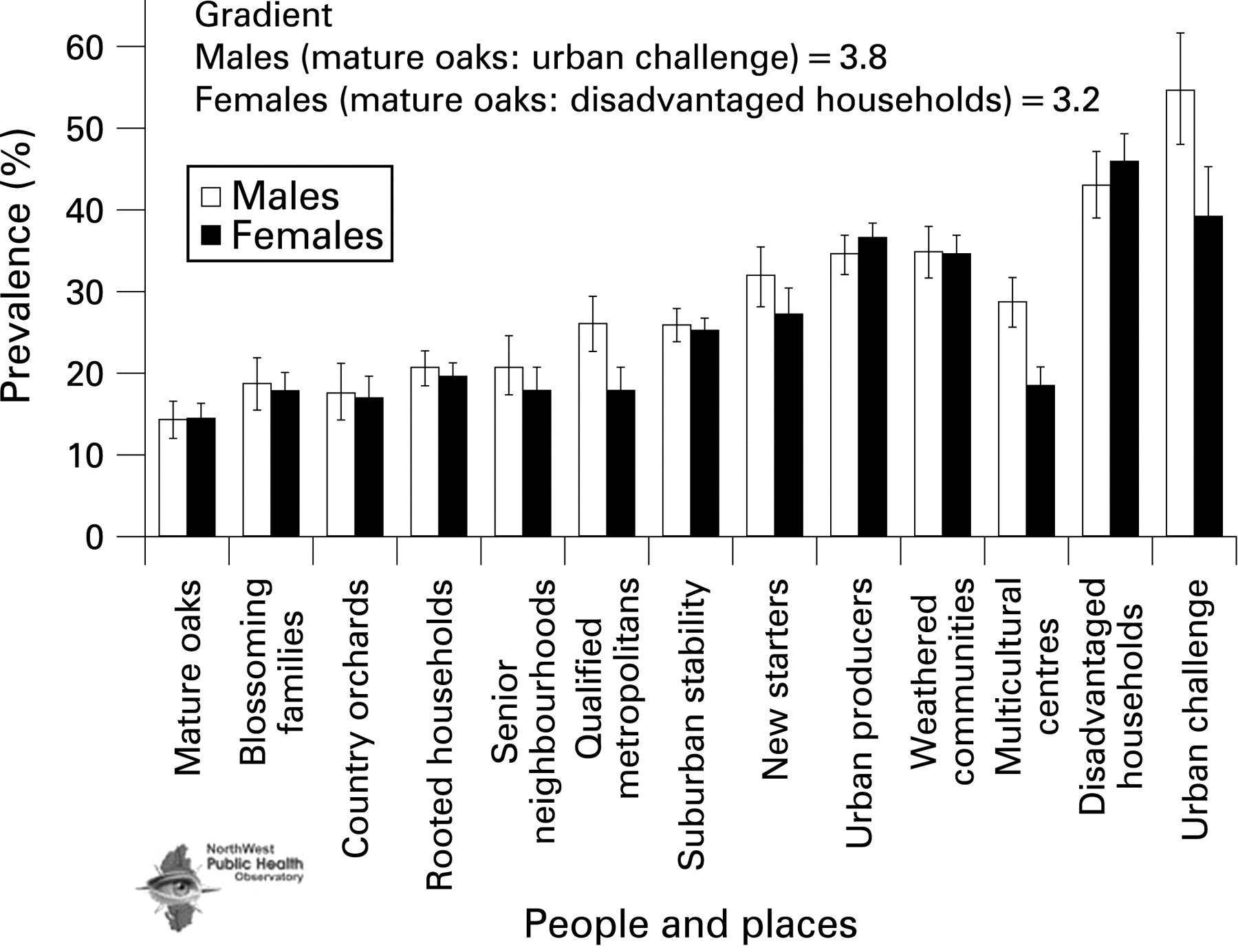
Methods: Using national Health Survey for England (HSE) data, smoking measures were generated for two different small area geographical classifications—the index of multiple deprivation (IMD, 2004) and the geodemographic lifestyle classification, P2 people and places. These classifications are available at postcode or lower super output area (LSOA) and therefore every respondent to the HSE could be assigned to one group within each classification. A smoking prevalence “gradient” was generated for each classification, which was used to estimate the number of smokers in every LSOA and local authority in England. These measures were compared with other modelled estimates and data on smoking-related deaths.
Results: Smoking prevalence showed the expected strong relationship with deprivation (IMD, 2004): higher deprivation resulting in over double the proportion of people who smoked. This almost exactly matched the gradient of smoking prevalence identified using individual socioeconomic status. People and places showed an even stronger gradient with over three times more people smoking in the most deprived communities than in the most affluent (fig). Estimates of smoking prevalence generated by these methods showed very high correlations with the rate of deaths due to smoking (R2 = 0.72). We will illustrate how these geodemographic classifications enable the identification of very localised communities with predicted higher levels of smoking.
Conclusions: Although accurate local measures of smoking status are needed to monitor the effectiveness of interventions, the targeting of campaigns and programmes to reduce smoking prevalence can usefully benefit from population segmentation techniques.
{kind=link}
S137 THE EFFECT OF GENDER ON DECLINE OF LUNG FUNCTION OVER 9 YEARS: A POPULATION-BASED STUDY
S Cooke, S Lewis, T McKeever, J Britton, A Fogarty. Division of Epidemiology and Public Health, University of Nottingham, Nottingham City Hospital, Nottingham, UK
Objectives: To investigate the effect of gender on decline in lung function in a population-based cohort.
Methods: In 1991, 2633 individuals aged 18–70 years were randomly sampled from a local authority area in the UK. In 2000, 1334 of these individuals were re-studied. On both occasions, data were collected on forced expiratory volume in one second (FEV1), forced vital capacity (FVC) and a variety of other exposures including a detailed smoking history. These data were analysed using linear regression to create age, sex and height-adjusted FEV1 residuals for 1991 and 2000 and to estimate the effect of gender on decline in FEV1 after adjustment for smoking status, smoking pack years and body mass index over this time.
Results: The study populations from 1991 and 2000 are described in the table. Over the 9-year period the unadjusted FEV1 fell by 386 ml in men and 297 ml in women. After adjustment for potential confounding factors, this resulted in a difference of −74 ml (95% CI −37 to −111) for men compared with women. This effect was also observed after the analysis was restricted to those who had never reported smoking (excess decline for men −99 ml; 95% CI −169 to −30). However, after adjustment for baseline FEV1, this difference ceased to be significant (excess decline for men −2 ml; 95% CI −46 to −43).
Conclusions: In this population-based cohort, men experienced a larger absolute decline in lung function than women. This effect is probably a consequence of the higher baseline lung function observed in men compared with women. This observation differs from previous reports of the effect of baseline lung function on subsequent decline in lung function.
Funding: British Lung Foundation and Asthma UK.
S138 HETEROGENEOUS CLINICAL EXPRESSION OF EOSINOPHILIC AIRWAY DISEASES IN AN ADULT HOSPITAL CLINIC POPULATION
1D Desai, 1P Haldar, 2G Davenport, 1ID Pavord. 1UHL Glenfield Hospital, Leicester, UK, 2Leicester University Medical School, Leicester, UK
Introduction: Eosinophilic airways inflammation is seen across a spectrum of different airway diseases with distinct pathophysiological and clinical features. Recognising these overlapping patterns is important for appropriate planning of clinical trials of specific anti-eosinophil therapy.
Methods: We performed a retrospective observational study of 100 consecutive patients with airway diseases and a raised induced sputum eosinophil count (>3%) attending a specialist airway clinic. Patients returned a symptom questionnaire and visual analogue symptom score for their most prominent symptom on a 10 cm horizontal scale. They all underwent spirometry with reversibility if pre-bronchodilator FEV1/FVC was less than 0.7 or methacholine provocation (PC20) if it was over 0.7. Sputum induction and processing was performed using standard methods. Asthma was identified in patients with a post-bronchodilator FEV1 greater than 80% and FEV1/FVC greater than 0.7 and either bronchodilator reversibility greater than 15% or a PC20 less than 8 mg/ml. Patients with bronchodilator reversibility greater than 15% but FEV1/FVC less than 0.7 were labelled as having mixed chronic obstructive pulmonary disease (COPD) and asthma and those with airflow obstruction without a significant bronchodilator were labelled COPD. Patients with predominant cough, without evidence of variable airflow obstruction or airway hyperresponsiveness were diagnosed as having eosinophilic bronchitis (EB).
Results: Asthma was diagnosed in 35 (35.3%), mixed COPD and asthma in nine (9.1%), COPD in 15 (15.2%) and EB in 40 (40.4%). The geometric mean sputum eosinophil count across all groups was 13.59% (SD 0.39). There was no significant difference comparing mean sputum eosinophil count across all four groups in this population (p = 0.849).
Conclusion: Eosinophilic airways disease presenting to secondary care is heterogeneous and a significant proportion does not fulfil standard criteria for asthma. The role of corticosteroids and novel anti-eosinophilic agent therapies under development requires consideration in a broader population of patients with airways disease and greater emphasis needs to be placed on identifying eosinophilic airway inflammation in patients presenting with airway symptoms.