Article Text

Statistics from Altmetric.com
P176 THE STATE OF TUBERCULOSIS IN VANUATU
1JN Fullerton, 1LJ Thomas, 2DT McLeod. 1University of Birmingham, Birmingham, UK, 2Sandwell and West Birmingham Hospital, Birmingham, UK
Background: Tuberculosis is one of the top 10 causes of death in Vanuatu; however, reported rates of multiple drug resistance (MDR) and HIV are currently low. To date, no study has systematically examined the diagnosis, management and clinical outcome of tuberculosis in Vanuatu, a practice strongly advocated by the WHO.
Aim: To assess whether the diagnosis and management of tuberculosis in Vanuatu is in line with regional and WHO guidelines and evaluate the quality of routine surveillance data in order to advise future practice and policy.
Method: A retrospective review of clinical and laboratory records for all cases of tuberculosis in Vila Central Hospital, Vanuatu, from 1 April 2006 to 31 March 2007
Results: 51 cases of tuberculosis were identified: 26 female (51%), average age 28.7 years. This extrapolates to a population rate of 63.75/100 000 per year, reflecting a 7% rise since 2005. The majority of cases were pulmonary (28, 54.9%). Sputum smears were performed in 32 (63%) cases. Combination therapy was readily available. Three patients (6%) received the correct dose, regimen and duration of therapy. Inadequate surveillance for HIV and MDR-TB was observed. Only eight (15.6%) cases were tested for HIV, one (12.5%) was positive. No MDR-TB was identified.
Conclusions: National surveillance data may be inaccurate and the rising incidence in tuberculosis is likely to be underestimated. Given the high level of sexually transmitted diseases and the experience of other Melanesian islands, an HIV epidemic is likely. Existing public health systems and tuberculosis services are not meeting WHO standards and are ill-prepared to cope with such an eventuality.
Acknowledgements: Morriston Davies Trust (BTS), Target TB.
P177 HEALTH STATUS OF UK PATIENTS WITH ACTIVE TUBERCULOSIS STARTING THERAPY
1ME Kruijshaar, 2M Lipman, 3ML Essink-Bot, 4S Lozewicz, 5D Creer, 6S Dart, 6H Sadler, 7H Maguire, 1I Abubakar. 1Health Protection Agency, Centre for Infections, London, UK, 2Royal Free Hospital, Respiratory Medicine, London, UK, 3University of Amsterdam, Department of Social Medicine, Amsterdam, The Netherlands, 4North Middlesex University Hospital, Respiratory Medicine, London, UK, 5Barnet and Chase Farm Hospitals NHS Trust, London, UK, 6Royal Free Hospital, North Central London TB Service, London, UK, 7Health Protection Agency, London Regional Epidemiology Unit, London, UK
Introduction: Tuberculosis has re-emerged as a serious public health problem in the UK over the past two decades. Few studies, however, have looked at the impact of tuberculosis and treatment on patients’ quality of life and functioning, and no data are available for the UK context.
Methods: Questionnaires were administered prospectively to patients in three London clinics at diagnosis, and one month into treatment for active tuberculosis. We assessed generic health-related quality of life (SF-36 and EuroQoL), symptoms and emotional impact (state–trait anxiety short-form (STAI-6), Center for Epidemiologic Studies depression scale (CESD) and worry items).
Results: To date, 42 baseline questionnaires have been returned. Most respondents (38 patients, 91%) were non-UK born, 13 (32%) were Indian and 12 (29%) black African, 18 (43%) were aged 30–45 years, and 12 were unemployed. 28 patients (68%) had pulmonary tuberculosis.
Symptoms frequently reported at diagnosis were tiredness (36 patients, 86%) and weight loss (29, 71%). The figure shows the proportion of patients reporting problems on the five EuroQoL domains plus their mean SF-36 and emotional scores. Higher SF-36 scores indicate better health status. Mean scores were below or just around 40 and the physical and mental component summary scores (36 and 40, respectively) were lower than the average observed for people with chronic illness. Higher STAI-6 and CESD scores indicate more symptomatology. The mean scores of 14 and 22, respectively, suggest the presence of anxiety and depression. Worries most frequently reported concerned respondents’ own health (39, 93%), the health of their family (35, 83%) and infecting others (31, 80%).
Conclusion: Tuberculosis patients suffer from significantly diminished health-related quality of life. Full results will be presented including changes in reported problems/levels after one month of treatment.

P178 ADEQUACY OF SAMPLE COLLECTION IN TUBERCULOSIS: IS IT SPECIALTY DEPENDENT?
MB Sikkel, A Abbas, T Langham, A McGown. Royal Berkshire Hospital, Reading, UK
Introduction and Objectives: Tuberculosis diagnosis in England and Wales is imperfect at present with only 62% of patients having culture-confirmed disease. We set out to audit our current practice in terms of adequacy of sample collection for suspected tuberculosis cases as defined by NICE guidelines. We also assess whether adequacy of sampling is dependent on the specialty of the requesting physician.
Methods: We identified 96 sequential patients notified to the tuberculosis register following tuberculosis diagnosis at our hospital trust between March 2006 and August 2007. Using the hospital’s computerised databases, we identified the number and types of diagnostic sample collected, which tests were requested on these samples and the specialty of the requesting physician.
Results: Of 96 patients, 49% (47/96) had pulmonary tuberculosis and 51% (49/96) non-pulmonary tuberculosis. Overall, 68% (65/96) were culture positive, 3% (3/96) smear positive but culture negative, 15% (14/96) culture negative and 15% (14/96) had no microbiological sample testing. Of patients with pulmonary disease and complete information on sampling, 76% (32/42) had adequate sampling (bronchoalveolar lavage or ⩾3 sputum) and 24% (10/42) had inadequate sampling. Pulmonary samples requested by respiratory physicians (87% adequate) were significantly more likely to be adequate than those requested by other physicians (33% adequate), p = 0.003. Of patients with extrapulmonary disease 73% (36/49) had adequate sampling (appropriate samples collected and microbiologically tested), 18% (9/49) had inadequate sampling (usually because the whole sample was placed in formalin for histology) and 8% (4/49) had no samples collected. Medical specialties were significantly more likely to collect adequate samples (96% adequate) than surgical specialties (73% adequate), p = 0.032.
Conclusions: In our study 24% (23/96) of patients had inadequate samples or no samples taken. This topic has been less extensively studied than other aspects of tuberculosis diagnosis such as the use of molecular and immunological techniques. Improving the adequacy of patient sampling could be a cost-effective, pragmatic way of improving the proportion of patients with microbiological confirmation of tuberculosis. We identified a link between specialty and adequacy of sampling, suggesting that early referral to specialist services and targeted education of healthcare workers may improve tuberculosis diagnosis.
P179 PREVALENCE OF SEVERE VITAMIN D DEFICIENCY IN NON-CAUCASIAN TUBERCULOSIS PATIENTS IN LEICESTER
1H Thuraisingam, 2A Nasimudeen, 2H Fernando, 3G Woltmann. 1Leicester City PCT, Leicester, UK, 2University Hospitals Leicester, Leicester, UK, 3Institute for Lung Health, Leicester, UK
Introduction: Vitamin D (25(OH)D3) is a modulator of macrophage function and an important immunomodulatory hormone. It enhances innate antimycobacterial activity in vitro and severe deficiency may be an important risk factor for the development of active disease after infection. We aimed to determine the incidence of vitamin D deficiency in all non-caucasian tuberculosis patients in Leicester in 2007.
Methods: Vitamin D levels were measured in patients of Asian and African ethnicities notified with tuberculosis in a University Hospital tuberculosis clinic in 2007. 104 patients were identified and 95 (91.3%) patients had their vitamin D levels measured mostly before treatment. Epidemiological data including ethnicity, country of origin, age, disease site and smear/culture positivity were recorded. Vitamin D deficiency was graded according to severity as severe (<8 ng/l), mild (8–20 ng/l), insufficiency (20–30 ng/l) and sufficiency (>30 ng/l)
Results: Of 104 patients, 19 (18%) were UK born and 85 (81%) were foreign born. 89 patients were from the Indian subcontinent, three of African origin and 10 others. 95/104 (91%) patients were tested. 77% (63/82) of patients of Indian subcontinent origin tested were found to be severely deficient (89% of UK born and 74% of foreign born). 2/2 (100%) African patients and 6/9 (66.7%) others were severely deficient. 20 (21.1%) patients had mild deficiency of which 17 were from the Indian subcontinent. 2/95 (2.1%) patients had insufficiency and none had sufficient levels. Age distribution: 7 (7.4%) patients were <20 years, 34 (35.8%) between 20 and 29 years, 22 (23.2%) between 30 and 39 years, 9 (9.5%) between 40 and 49 years, 13 (13.7%) between 50 and 59 years and 10 (10.5%) were older than 60 years. All nine patients in the 40–50-year age group were severely deficient followed by six (85.7%) patients in the under 20-year group and 28 (82.4%) in the 20–29-year group. 75% of respiratory and 85% of non-respiratory tuberculosis cases were severely deficient. No significant sex differences were seen. 46 (75.4%) out of 61 culture-positive cases and 16 (80%) of 20 smear-positive cases were severely deficient.
Conclusion: In accordance with previous UK reports severe and mild vitamin D deficiency are very common among British Asian and African tuberculosis patients in Leicester. A prospective intervention study of pharmacological vitamin D replacement is needed in the most commonly affected UK tuberculosis patients and their contacts.
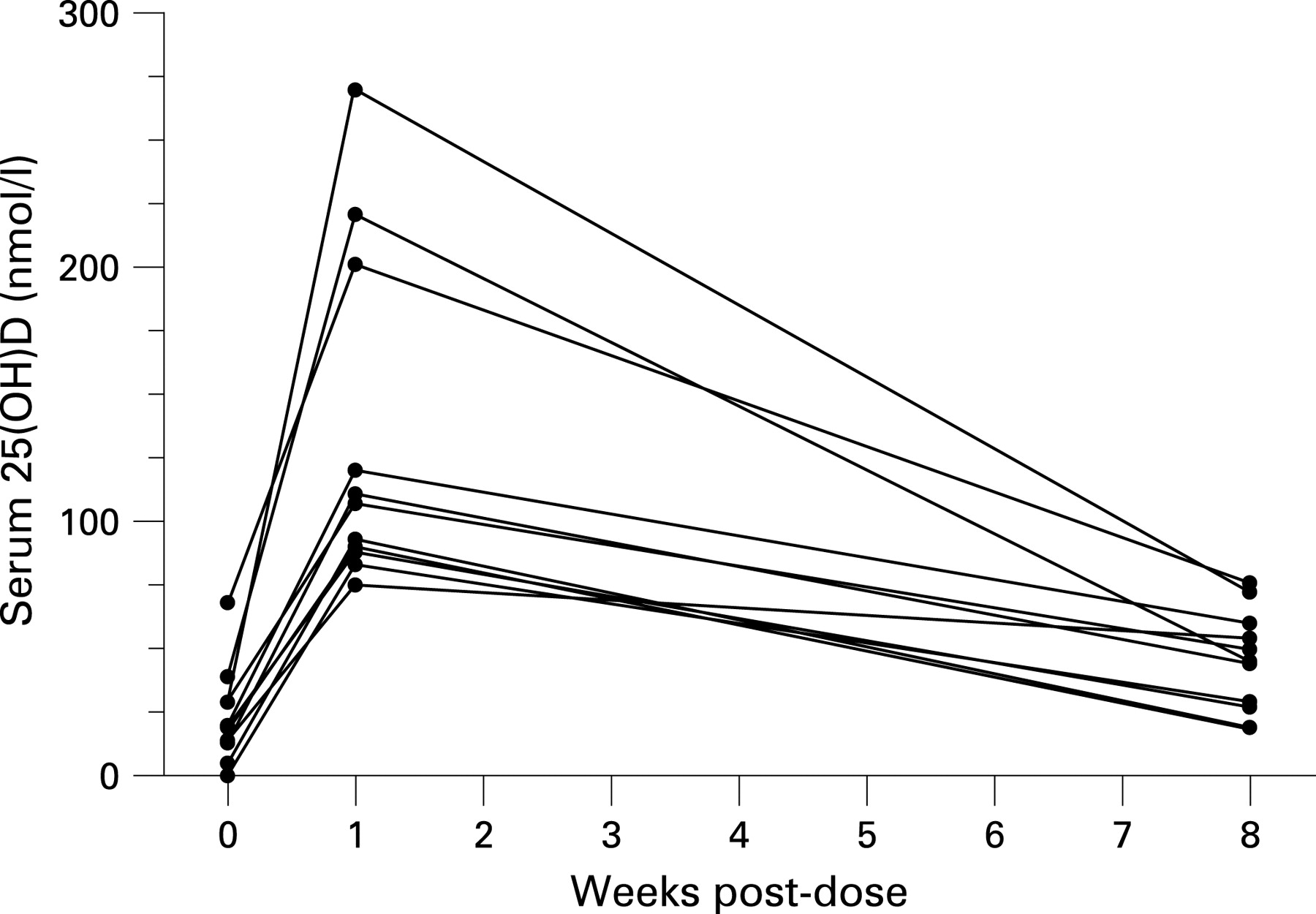
P180 INFLUENCE OF A SINGLE ORAL DOSE OF VITAMIN D2 ON SERUM 25-HYDROXYVITAMIN D CONCENTRATIONS IN TUBERCULOSIS PATIENTS
1AM Nanzer, 2KR Satkunam, 2GE Packe, 3SJ Rainbow, 3ZJ Maunsell, 4PM Timms, 4TR Venton, 1SM Eldridge, 5RN Davidson, 6RJ Wilkinson, 1CJ Griffiths, 1AR Martineau. 1Centre for Health Sciences, Barts and The London School of Medicine and Dentistry, London, UK, 2Newham Chest Clinic, Forest Gate, London, UK, 3Department of Clinical Biochemistry, North West London Hospitals NHS Trust, Northwick Park Hospital, Harrow, UK, 4Department of Chemical Pathology, Homerton University NHS Foundation Trust, London, UK, 5Tuberculosis Clinic, North West London Hospitals NHS Trust, Northwick Park Hospital, Harrow, UK, 6Division of Medicine, Wright Fleming Institute, Imperial College London, London, UK
Introduction and Objectives: Administration of bolus-dose vitamin D has been proposed as a potentially valuable adjunct to standard antituberculous therapy, but the safety and efficacy of this practice in elevating serum 25-hydroxyvitamin D (25(OH)D) concentrations have not been established. Our aim was to determine the effect of a bolus-dose vitamin D on serum 25(OH)D and corrected calcium concentrations in patients with tuberculosis.
Methods: A total of 25 tuberculosis patients was randomly assigned to receive a single oral dose of 2.5 mg vitamin D2 or placebo. Serum 25(OH)D and corrected calcium concentrations were determined at baseline, one week and 8 weeks post-dose and compared with those of a cohort of 56 healthy adults receiving 2.5 mg vitamin D2.
Results: Hypovitaminosis D (serum 25(OH)D <75 nmol/l) was present in all patients at baseline. A single oral dose of 2.5 mg vitamin D2 induced a 109.5 nmol/l mean increase in patients’ serum 25(OH)D concentration and corrected hypovitaminosis D in all patients at one week post-dose. Hypovitaminosis D recurred in 10/11 patients at 8 weeks post-dose. No patient receiving vitamin D2 experienced hypercalcaemia. Patients experienced greater mean increase in serum 25(OH)D at one week than healthy adults.
Conclusions: A single oral dose of 2.5 mg vitamin D2 corrects hypovitaminosis D at one week, but not at 8 weeks post-dose in tuberculosis patients.
P181 ENHANCED DETECTION OF LATENT TUBERCULOSIS INFECTION USING IFN-GAMMA RELEASE ASSAYS PRIOR TO COMMENCEMENT OF ANTI-TUMOUR NECROSIS FACTOR ALPHA THERAPY
T Chapman, LC Evans, S Linstead, M Cootauco, J Groth, YE Ong, A Draper, F Chua. St George’s Healthcare NHS Trust, London, UK
Introduction and Objectives: Optimal screening for latent tuberculosis infection (LTBI) prior to commencing anti-tumour necrosis factor (TNF) alpha therapy for chronic inflammatory disorders is not established. Such individuals are at increased risk of tuberculosis disease reactivation when subjected to systemic TNFα blockade. We hypothesised that a screening protocol integrating chest radiography (CXR), tuberculin skin testing (TST) and IFN-γ release assays (IGRA) would enhance LTBI diagnosis in these patients who may have disease or treatment-related immunosuppression.
Methods: Retrospective tuberculosis database analysis identified 31 patients (20 women, age range 23–85 years, median 46; 11 men, age range 33–64 years, median 45) referred for exclusion of LTBI between March 2006 and June 2008. BCG status, CXR features, underlying disease and pharmacological history were compared. LTBI was defined as immunological evidence (TST or IGRA reactivity) of asymptomatic tuberculosis infection.
Results: Primary diseases included rheumatoid arthritis (23/31; 74%), psoriasis (4/31, 13%), Crohn’s disease (n = 2) and ankylosing spondylitis (n = 1). Three-quarters had previous BCG vaccination (24/31, 77%) and TST responses ranged from 0 to 16 mm. IGRA was performed in 90% (28/31) of cases: QuantiFeron-Gold (QTF) in 11/28 (39%), commercial Elispot in 3/28 (11%) and an in-house Elispot-based T-SPOT.TB assay in 14/28 (50%). Of these, five patients (18%) had a positive result (QTF 2; T-SPOT.TB 2; Elispot 1). Two were TST anergic (0 mm) despite previous BCG, one had a 9 mm TST response (BCG-positive) and two avoided TST due to self-recalled previous tuberculosis disease. All were taking one or more immune-modifying drugs when assessed, most commonly methotrexate, sulfasalazine or prednisolone. CXR scarring or granulomata were present in four. Among 13 individuals exonerated of LTBI (anergic TST plus non-reactive IGRA), four (31%) had radiographic signs of past tuberculosis disease. Two patients with “indeterminate” QTF retested negative to Elispot.
Conclusion: IGRA identified LTBI in almost a fifth of potentially immunosuppressed individuals being considered for anti-TNFα therapy within a tuberculosis-prevalent area in south-west London. Crucially, when TST was non-diagnostic (anergic) in patients on immune-modifying drugs, IGRA revealed LTBI in 2/15 (13%) cases. IGRA also increased confidence in excluding LTBI in those with radiographic changes suggesting previous pulmonary tuberculosis. Furthermore, the use of an in-house T-SPOT.TB assay circumvented uncertainty associated with an indeterminate QTF result.
P182 IMPROVING TUBERCULOSIS SERVICES IN A LOW INCIDENCE AREA: A CASE STUDY OF TEES PRIMARY CARE ORGANISATION CLUSTER
E Kunonga, J Taylor, T Sangowawa. North Tees PCT, Stockton-on-Tees, UK
In Teesside, tuberculosis has been increasing rapidly, almost doubling between 2006 and 2007. Middlesbrough has the highest incidence (24.71 per 100 000 population) not only in the Tees primary care organisation (PCO) cluster, but also across the north east region as a whole. We carried out a review of tuberculosis services in the Tees PCO cluster to help commissioners and service providers secure the best tuberculosis services to meet local need.
Tuberculosis epidemiology was reviewed by analysing notification data. The Department of Health “TB commissioning toolkit” (2007), National Institute for Health and Clinical Excellence tuberculosis guidelines (2006) and Stopping tuberculosis in England, Chief Medical Officer action plan (2004) were used as a benchmark for local services. Key informant interviews were conducted with clinicians, PCO commissioners and the Health Protection Agency.
Although local tuberculosis incidence and workload have almost doubled within the past 2 years, there has been no increase in the tuberculosis workforce. All three tuberculosis services revealed inadequacies in specialist tuberculosis nursing capacity. One service, in particular, did not have adequate arrangements for contact tracing and treatment supervision and monitoring. Commissioning of the three tuberculosis services was carried out through block contracts without specific service level agreements.
The review led to the development of MDT tuberculosis meetings, a tuberculosis network and strategy and a redesign of the tuberculosis nursing service. It also brought together clinicians, commissioners and public health to discuss ways of ensuring that local tuberculosis services are in line with national policy and guidance.
In conclusion, the three national policy documents on the prevention and management of tuberculosis can be used to compile standards of best practice from which local services can be evaluated against. As tuberculosis incidence continues to rise in England, there is a strong need for all organisations, including those in low tuberculosis incidence areas, to be assured that their tuberculosis services are sustainable and capable of delivering efficient and effective tuberculosis prevention and control.
P183 ARE WE DELIVERING PATIENT-CENTRED CARE TO THOSE WITH TUBERCULOSIS?
1C Philips, 2C McCrudden, 1NJ Roberts, 1MR Partridge. 1NHLI Division at Charing Cross Hospital, Imperial College London, London, UK, 2Imperial College NHS Healthcare Trust, London, UK
Background: Tuberculosis is increasing worldwide, often co-existing with HIV, and there is understandable concern about the emergence of multidrug-resistant disease. Guidelines exist on correct management but there has been limited research on patients’ fears and concerns about tuberculosis and on their information needs. Addressing such issues is likely to be fundamental in ensuring adherence to therapy.
Methods: A qualitative study of patients diagnosed with tuberculosis was undertaken to elicit patients’ fears and concerns about their condition and their opinions about the care and information they receive. 22 patients were interviewed (mean length 21 minutes (SD 10)) over a 2-month period (semistructured recorded interview format). All transcripts were themed by three independent researchers using standard methodologies.
Results: Of the 22 patients studied, 15 were male (mean age 48 years (SD 19.01)). 60% had not reached secondary school education levels. 86% completed the interview without an interpreter although English was not their first language. The patients represented 13 different nationalities, the largest being Somalian (23%). From the patient transcripts seven major themes were identified: stigma; emotional experiences; understanding of disease; infectivity; healthcare satisfaction; information and past experiences of tuberculosis. Stigma remained a dominant emotion and the range of emotional responses recorded included denial, fear, shock and relief at the diagnosis. There were substantial inconsistencies in the understanding of the disease, with very little understanding of extrapulmonary disease and many misconceptions regarding infectivity. The views about healthcare satisfaction were mostly positive, although there were negative comments about waiting times in clinics. Discrepancies were shown to exist between expressed patient wants and those perceived to be necessary by healthcare professionals. No one uniform form for information given was identified and information needs were diverse.
Conclusions: In a patient-centred service for tuberculosis, we need to address the fears and concerns that patients have about their condition and we need to see their disease within the wider psychosocial context. Public misconceptions about the disease still need to be tackled and we need to enhance patients’ understanding especially about non-pulmonary disease.
P184 THE NATIONAL MULTIDRUG-RESISTANT TUBERCULOSIS SERVICE: THE FIRST 6 MONTHS
DM Cullen, PDO Davies. Liverpool Heart and Chest Hospital, Liverpool, UK
Introduction: The management of multidrug-resistant tuberculosis (MDRTB) is an emerging problem in the UK. Although still relatively uncommon (approximately 1% of all tuberculosis cases in the UK), global comparisons suggest it is likely to increase. The low incidence in the UK means that few specialists treating tuberculosis have much experience of managing patients with MDRTB and no mechanism for collecting data on the progress and outcomes of such patients exists. To attempt to overcome this gap, with the acknowledgement of the relevant professional bodies, and a grant from Genus Pharma, the MDRTB Service was established at the Liverpool Heart and Chest Hospital in January 2008.
Method: The service offers ready access to expert advice on the management of patients with MDRTB via an electronic virtual committee of tuberculosis experts. Members include chest physicians, ID physicians, paediatricians, public health physicians, a specialist nurse and the directors of the HPA laboratories where drug sensitivity for tuberculosis is undertaken. The advice given offers the likely best treatment for patients and by doing so prevents the emergence of extremely drug-resistant tuberculosis (XDRTB). The second function of the service is to collect data on all MDRTB cases identified in the UK, to record outcomes and develop a consensus on the most effective methods of treatment of MDRTB.
Results: From 1 January to 30 June, the MDRTB service provided advice on 21 cases of MDRTB and one XDRTB case in the UK. Information on the initial resistance patterns of 16 MDRTB cases showed that in addition to resistance to isoniazid and rifampicin, 63% of the cases were resistant to streptomycin, 50% to rifabutin, 44% to ethambutol and 38% to pryazinamide. The majority of the cases were of a non-white ethnic background, the highest number being Asian (five) and African (four.) To date, one of the 22 patients is known to have died and the rest are continuing on treatment. Eleven patients were known to be sputum smear positive and therefore infectious.
Conclusion: The MDRTB service is an important means of providing expert advice on the management of these cases. Streptomycin resistance was present in the majority.
P185 ADHERENCE TO CHEMOPROPHYLAXIS OF LATENT TUBERCULOSIS: AN AUDIT OF CARDIFF AND VALE CASES IN 2007
C Martin, J Duckers, E Weeks, O Seddon, I Campbell. Department of Respiratory Medicine, Cardiff University, Cardiff, UK
Introduction and Objectives: The rationale for treating latent tuberculosis is to prevent later reactivation.1 The incidence of tuberculosis was 6.5 per 100 000 population in Wales in 2006 and was lower than the UK average.2 However, some areas in Cardiff have seen a surge in the number of tuberculosis patients and of those requiring chemoprophylaxis especially following the identification of Cardiff as a port of entry. We suspected low adherence rates in patients receiving chemoprophylaxis.
Methods: We performed a retrospective audit of patients identified with latent tuberculosis between 1 January 2007 and 1 January 2008 in the Cardiff and Vale area. Local policy is to issue 3 months of isoniazid therapy along with education and a contact number. After 3 months patients are reviewed and a further 3 months of isoniazid prescribed. Non-attenders receive a letter and telephone call. If they fail to attend or are uncontactable they are deemed to have not adhered to treatment. Patients are contacted following the 6-month course to ensure completion.
Results: 41 patients were identified as requiring chemoprophylaxis (33 adults, eight children). Of the 41, 19 were tuberculosis contacts, 18 new entrants (11 immigrants, seven asylum seekers) and four needed chemoprophylaxis pre-disease-modifying therapy for rheumatoid arthritis. Overall, 25/41 (61%) adhered to the therapy. The remaining 16 (39%) defaulted at the 3-month appointment and were uncontactable. There was no significant difference (p>0.05) in the adherence rates between subsets of patients (children/adults, male/female, contacts/new entrants). 30 of the 41 patients would not have been identified as requiring chemoprophylaxis before the change in screening that followed NICE guidance of 2006.
Conclusions: The local adherence rate of 61% is substantially lower than that set by NICE guidelines but is similar to a recent study.3 NICE guidance1 on new entrant and contact screening has led to the identification of an extra 30 cases in the year 2007. This 140% increase in workload may further impact on the ability to achieve adherence targets in an already disparate population.
P186 HEPATOTOXICITY DUE TO ANTITUBERCULOSIS THERAPY: GUIDANCE AND PRACTICE
NF Walker, D Turner, M Kliner, S Bhagani, I Cropley, S Hopkins, M Lipman. Department of HIV, Infectious Diseases and Respiratory Medicine, The Royal Free Hospital, London, UK
Introduction: Hepatotoxicity due to antituberculosis therapy is a significant clinical problem in both HIV-negative and co-infected populations. Guidelines recommend screening for chronic liver disease and baseline liver function tests (LFT) before treatment. Further monitoring is indicated for those with risk factors (viral hepatitis, other chronic liver disease, LFT above the upper limit of the normal range at baseline).
Methods: A retrospective review was undertaken of patients diagnosed with tuberculosis between 1 June 2006 and 1 June 2007. HIV, hepatitis B (HBV), hepatitis C (HCV) and LFT were extracted from the hospital pathology system. Hepatotoxicity was defined as elevation of serum transaminases (AST/ALT) more than three times the upper limit of normal (>3ULN).
Results: 103 patients were diagnosed and started antituberculosis treatment. 53 were male with a median age of 43 years (range 0–82). The population was ethnically diverse: 24 Asian, 46 black African, 22 European Union countries, 11 other. 19 patients were known to be HIV positive at diagnosis. 81/103 (79%) patients were tested for HBV, seven (9%) were HBV surface antigen positive. 76/103 (74%) patients were tested for HCV, six (8%) were HCV antibody positive. 60/84 (71%) had HIV tests at baseline, 5/84 (6%) were positive. 87 (84%) patients had baseline LFT. The figure outlines the LFT results during the course of antituberculosis treatment in relation to HIV, HBV and HCV status. Similar proportions of subjects with and without abnormal baseline LFT had biochemical hepatotoxicity (11% and 16%, respectively). The incidence of HIV was notable in patients with hepatotoxicity, particularly in those with normal baseline LFT. The median number of LFT performed over the following 6-month period was nine (range 0–90) for those with HBV or HCV co-infection or abnormal baseline LFT and five (0–60) without.

{kind=link}
{kind=link}
{kind=link}
Conclusion: Only 84% patients had baseline LFT. HIV, HBV and HBC are prevalent. Improved screening is required. LFT were monitored during treatment more frequently than recommended, particularly in those with normal baseline LFT without viral hepatitis. However, there was a high incidence of hepatotoxicity in this group, especially in HIV-positive individuals. The current recommendations may require modification in an urban tuberculosis population.
P187 TREATMENT-RELATED TUBERCULOSIS PARADOXICAL REACTIONS ARE ASSOCIATED WITH INCREASES IN ANTIGEN-SPECIFIC MYCOBACTERIAL RESPONSES IN THE LUNG
1A Dunleavy, 2RAM Breen, 2HJ Stauss, 1MCI Lipman. 1Department of Thoracic Medicine, The Royal Free Hospital, London, UK, 2Department of Immunology, University College London, The Royal Free Hospital, University College London, London, UK
Introduction: Paradoxical reactions (PR) occur in up to 15% of HIV-negative and 30% of HIV-positive subjects receiving treatment for active tuberculosis. The diagnosis is based on clinical features; and its pathogenesis is not defined, though is likely to involve antigen-specific T-cell responses. We hypothesised that people who develop PR would have an amplification of their CD4 IFN-γ purified protein derivative of Mycoplasma tuberculosis (PPD)-specific response at the time of PR. The amplification would be more evident in the lung (measured by induced sputum) compared with blood, irrespective of the site of disease.
Methods: We undertook a prospective study of patients with active tuberculosis commencing treatment. Clinical evaluation was performed throughout therapy and used to establish evidence of PR. Serial blood and induced sputum samples were obtained at baseline and during therapy. The percentage of IFN-γ synthetic CD4 lymphocytes following 16-h stimulation with PPD was assessed. CD4 T-cell differentiation was measured in blood and induced sputum by staining with CCR7 and CD45RA. Samples were analysed using four-colour flow cytometry.
Results: To date, 10 subjects have been investigated (nine pulmonary and one renal). Three have had clinical PR. No difference was noted in baseline PPD response between those who did and did not develop PR (p = 1). In those with PR, lung but not blood PPD-specific CD4 IFN-γ and IL-2 responses increased (see table). The PPD-specific response switched from <5% of CD4 cells to >5% in all cases. None of the patients without PR had a rise in their antigen-specific responses above 5%. One patient without PR had an initial huge response (36% of all cells) that decreased with treatment. There appeared to be no consistent pattern to changes in memory T-cell populations between those with and without PR.
Conclusion: Our data support the hypothesis that tuberculosis-related PR is associated with increases in lung antigen-specific CD4 responses. However, this is not present in paired blood samples, suggesting activation of a compartmentalised, specific immune response.