Article Text

Abstract
Chronic infection with Pseudomonas aeruginosa is common in cystic fibrosis (CF) and certain strains are more transmissible and virulent than others. Of these, the Liverpool Epidemic Strain (LES) is highly transmissible and cross infection has been reported between patients with CF and healthy non-CF relatives. However, the risk of transmission from humans to animals is unknown. The first report of interspecies transmission of the LES strain of P aeruginosa from an adult patient with CF to a pet cat is described. This development further complicates the issue of infection control policies required to prevent the spread of this organism.
Statistics from Altmetric.com
A previously well 5-year-old neutered male Egyptian Mau cat presented with a 6 week history of intermittent serous nasal discharge and recurrent episodes of sneezing. Physical examination and a sinus x ray were unremarkable. He was empirically treated with a 2 week course of oxytetracycline 100 mg twice daily without improvement. Culture of retrograde deep nasal flushings performed under general anaesthesia yielded a profuse growth of Pseudomonas aeruginosa. Tests for feline herpes virus-1, feline calicivirus and cultures for fungal pathogens were negative. PCR diagnostic tests1 and tube array genomic fingerprinting2 both identified multiple P aeruginosa isolates as the Liverpool Epidemic Strain (LES) (fig 1), a strain that had chronically infected the cat’s owner, a patient with cystic fibrosis (CF), for over 10 years. Each of 18 LES isolates tested was sensitive to marbofloxacin, ceftazidime, piperacillin–tazobactam, colistin, meropenem and tobramycin. Although ceftazidime resistance has been reported as a feature of the LES, LES isolates have been shown to be intermittently sensitive to ceftazidime.3 Following treatment with marbofloxacin 10 mg once daily for 3 weeks, the symptoms recurred. Repeat nasal washings confirmed the presence of the LES. A further 6 week course of marbofloxacin transiently improved the symptoms, but the cat continues to experience recurrent paroxysmal sneezing episodes and intermittent mucopurulent nasal discharge. At 4 months, a repeat throat swab confirmed the continuing presence of the LES.
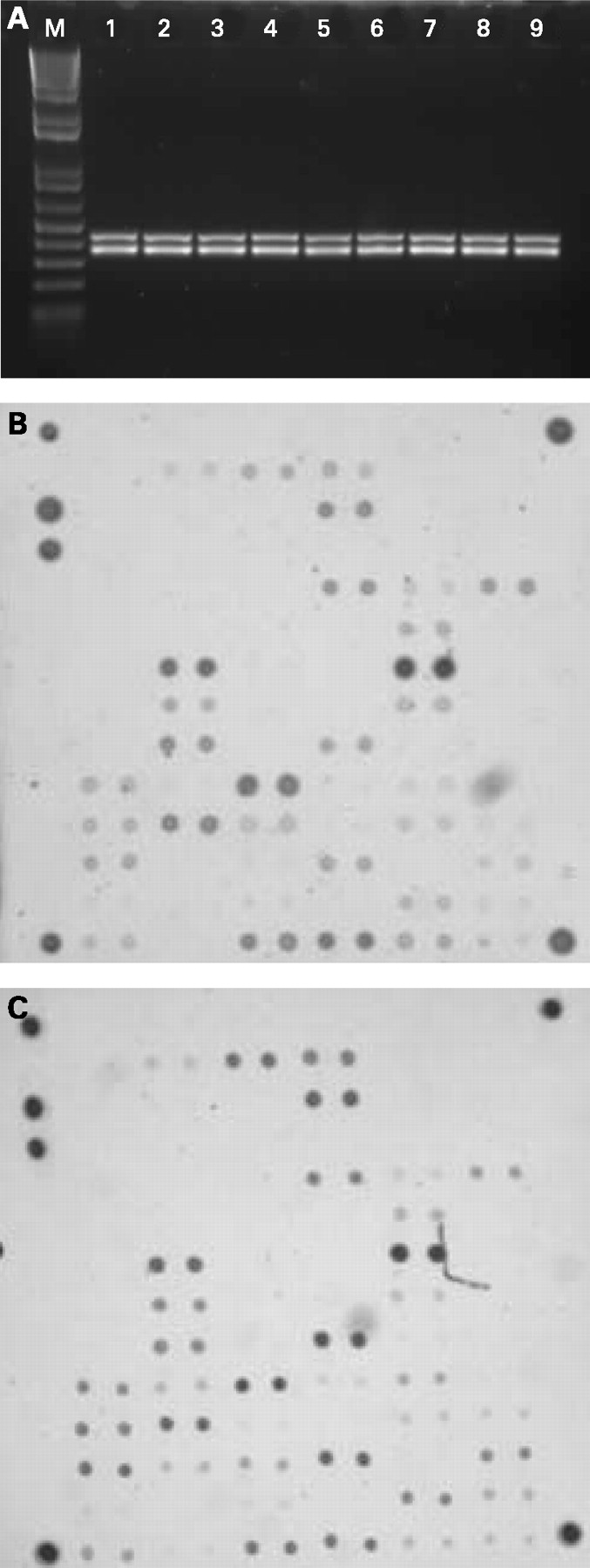
{kind=link}
The owner was a 54-year-old male with CF (DF508/DF508) who had been chronically infected with LES (identified by genomic fingerprinting) which was intermittently sensitive to ceftazidime. Since 2000 his lung function has been stable (forced expiratory volume in 1 s 60% predicted) and he only requires an average of one course of oral antibiotics per year for pulmonary exacerbations. In between these, he is well with little daily sputum production and rarely carries out chest physiotherapy. The owner lives in a small flat: the cat is an indoor pet and had been living in close contact with his owner since he was 13 weeks old, having free rein of the dwelling space.
DISCUSSION
Chronic infection with P aeruginosa is common in CF, occurring in up to 80% of adults. While most patients are infected with unique strains, some strains can be passed between CF patients. Of these, the LES is highly transmissible and is common throughout UK CF clinics.4 We have shown that it can “superinfect” patients with CF who already possess previously well established strains of P aeruginosa5; it can infect the relatives of patients with CF, with subsequent chronic morbidity,6 and is associated with a poorer prognosis.7 Although cross infection of bacteria (methicillin resistant Staphylococcus aureus), fungi and viruses (H5N1) can occur between humans and pets,8 this is the first report of interspecies cross infection of a highly transmissible P aeruginosa strain.
Respiratory tract infections are a common cause of morbidity and mortality in cats. Although a number of bacteria have been isolated from the airways in healthy cats,9 P aeruginosa is an uncommon cause of respiratory tract infection.10 In experimental cat models, repeated P aeruginosa infection causes chronic bronchiolitis and pneumonia, with similar histological features to chronic P aeruginosa infection in human CF.11 In this case, we excluded the two most common causes of feline chronic rhinitis (herpesvirus-1 and calicivirus), and it is likely that the chronic respiratory tract infection in the cat by P aeruginosa was due to transmission from the owner, via infected sputum or aerosol spread. Although this individual was not a copious sputum producer nor did he have productive rhinitis, the cat cohabited in a small living space as an indoor pet with ample opportunity for cross infection to occur.
Cross infection with virulent organisms is an increasing problem in the CF community, necessitating the adoption of stringent patient segregation. This report suggests that the LES may have a greater potential for transmission than previously contemplated, further complicating infection control measures for this patient group.
Footnotes
Competing interests: None.
Patient consent: Obtained.