Article Text

Abstract
Background: Influenza-like illness (ILI) among elderly people living in residential care homes (RCHEs) is a common cause for hospitalisation. A study was undertaken to examine the incidence, underlying aetiology, natural history and associated healthcare resource utilisation related to ILI in the RCHE population.
Methods: A prospective study of ILI in four RCHEs in Shatin, Hong Kong was conducted from April 2006 to March 2007. Each RCHE was monitored daily for the occurrence of ILI and followed up until resolution of illness or death. Clinical features were recorded and sputum, nasopharyngeal aspirate, blood and urine specimens were examined for underlying aetiology.
Results: 259 episodes of ILI occurred in 194 subjects, with mild peaks in winter and summer, over a sustained level throughout the year. The infectious agent was identified in 61.4% of all episodes, comprising bacterial infection in 53.3% and viral in 46.7%. Multiple infections occurred in 16.2% of subjects. The most frequent organism was Streptococcus pneumoniae, followed by respiratory syncytial virus, Pseudomonas aeruginosa, metapneumovirus and parainfluenza virus types 1 and 3. Clinical features did not vary according to the underlying aetiology, the common presenting features being a decrease in general condition, cognitive and functional deterioration, and withholding of food in addition to fever and respiratory symptoms. Overall, mortality at 1 month/discharge was 9.7%. Infection with methicillin-resistant Staphylococcus aureus, low body mass index and poor function predisposed to mortality. No association was observed between influenza vaccination status and underlying aetiology, clinical features or outcome.
Conclusions: The clinical presentation of ILI is non-specific and is mainly due to bacterial and viral infections other than influenza in the RCHE population.
Statistics from Altmetric.com
Influenza-like illness (ILI) among elderly people living in residential care homes (RCHEs) is a public health concern as it may potentially give rise to outbreaks resulting in admission to hospital. It is difficult to identify clinically whether ILI is due to outbreaks of emerging viral infections with serious consequences such as H5N1, or other more “benign” infections such as seasonal influenza or respiratory syncytial virus (RSV). Currently, ILI in RCHEs is monitored by the Centre for Health Protection (CHP) in Hong Kong by passive surveillance, relying on a staff member of each RCHE acting as an infection control officer. Other preventive strategies include free annual seasonal influenza vaccination and oseltamivir chemoprophylaxis for residents in RCHEs in which an influenza outbreak has occurred.
Influenza vaccination has been shown to be effective in reducing hospital admissions during an influenza epidemic, particularly in institutional settings, and may reduce half of the deaths due to influenza.1 2 However, this strategy will only be effective if the ILI episode is caused by influenza. Furthermore, a recent study has queried the efficacy of influenza vaccination for residents of old peoples’ homes in Hong Kong.3 There is a suggestion that, in old peoples’ homes, respiratory infections are caused mostly by pathogens other than influenza virus,4 whereas RSV could represent a disease burden similar to that of seasonal influenza A in a population in which the prevalence of vaccination against influenza is high (eg, in elderly or high-risk adults.5 Oseltamivir chemoprophylaxis is also recommended but it is offered only to those aged <80 years without chronic diseases and normal renal function documented in recent months.6 Assuming that influenza is the cause of most cases of ILI, this local policy appears to be empirical and not evidence-based but, at the same time, consumes significant healthcare resources.
In reality, ILI is merely a description of a clinical presentation consisting of fever ⩾37.8°C or an acute deterioration in physical or mental ability, plus either new onset of one or more respiratory symptoms or an acute worsening of a chronic condition involving respiratory symptoms.7 It may be caused by bacterial or any viral infections of which influenza is only one of many. Furthermore, the underlying cause may not be infective but a consequence of aspiration, a common occurrence in the frail elderly population.8 Figures based on passive surveillance may underestimate the true incidence.9 This study aimed to document the incidence of ILI, the underlying infective aetiology, the natural history and associated healthcare resource utilisation over a 1-year period.
METHODS
Residential care homes for the elderly (RCHEs)
RCHEs supported by the Hong Kong Hospital Authority’s Community Geriatric Outreach Teams (CGAT) in the Shatin district were studied. Two were subsidised (Sage and Caritas) with 204 and 256 residents, respectively, and two were private (Shui On and Cambridge) with 221 and 91 residents, respectively. Infection control policies recommended by the CHP were implemented in all RCHEs and were complied with by reports.
Research staff liaised with the nurse of the CGAT or the Visiting Medical Officer (VMO) responsible for the homes to identify residents with ILI on a daily basis. An ILI episode was defined as fever ⩾37.8°C measured using a digital aural thermometer or an acute deterioration in physical or mental ability, plus either new onset of one or more respiratory symptoms or an acute worsening of a chronic condition involving respiratory symptoms.7 Specimens were collected within the first 2 days of illness and paired serology 2 weeks later, whether the patients were still in hospital or had returned to the RCHE. A follow-up visit was carried out after recovery of illness.
Investigations
All subjects with clinical features fulfilling the inclusion criteria for ILI underwent the following investigations:
Sputum sample
Rapid multiplex nested PCR
Paired serum samples
Urine sample
Sputum sample
Sputum samples were used for:
Routine bacterial culture which covers Streptoccocus pneumoniae, Pseudomonas sp, Haemophilus influenzae, Moraxella catarrhalis and other likely pathogens.
Mycobacterial culture for tuberculosis (restricted to those with prolonged respiratory symptoms such as cough for ⩾2 weeks, systemic symptoms of weight loss or hospital admission).
Rapid multiplex nested PCR
A rapid multiplex nested PCR was undertaken to detect respiratory pathogens. Five groups of multiplex nested-PCR assays targeting 21 respiratory viruses and bacteria were developed. Each detected four viruses and/or bacteria: group 1 comprised influenza A and B group-specific and subtypes H1N1, H3N2, H5N1-specific primers; group 2 comprised parainfluenza 1, 2, 3, 4a and 4b; group 3 comprised RSV A and B, human rhinovirus and enterovirus; group 4 comprised human coronavirus (CoV)-OC43, -229E, -SARS-CoV and human metapneumovirus (hMPV); and group 5 comprised Mycoplasma pneumoniae, Chlamydophila pneumoniae, Legionella pneumophila and adenovirus.10
Nasopharyngeal aspirates were collected and subjected to RNA and DNA extraction. Both viral RNA and DNA were extracted by spin columns (QIAamp MinElute Virus Spin Kit, Qiagen, USA) according to the manufacturer’s recommendations. RNA extracted was converted to cDNA by reverse transcriptase (Superscript III Reverse Transcriptase, Invitrogen, Carlsbad, California, USA). All the DNA and cDNA were used immediately for the five groups of nested PCR as described previously.
Paired serum samples
A paired serum sample was used for atypical pneumonia serological examination including influenza A, influenza B, parainfluenza 1, 2, 3, RSV, adenovirus, mycoplasma, L pneumophila, Coxiella burnetii, Chlamydia spp. The methodology used was the complement fixation test.
Urine sample
A urine sample (for hospitalised cases) was taken to detect L pneumophila serogroup 1 and S pneumoniae antigens (BinaxNOW, Maine, USA).
A chest radiograph was performed in subjects with a cough lasting ⩾2 weeks and as part of the clinical management as indicated for other cases.
In determining the aetiology of ILI, the following criteria were used: positive culture from sputum, blood or nasopharyngeal aspirate; positive urinary antigen for S pneumoniae or L pneumophila serogroup 1; positive PCR identification; serology of fourfold rise or a single titre of 80 or above, and a positive IgM.
Subjects with ILI were managed by the VMO or a doctor from the CGAT in the RCHE. Treatment included antipyretics, antibiotics, antiviral drugs depending on the clinical presentation, attention to hydration and nutrition. Any need for admission to hospital was the decision of the attending doctor and also RCHE staff who might have difficulty in providing additional care or monitoring of the patient.
Documentation of natural history of illness
The following data were documented for each patient: age, sex, past medical history, past vaccination history, co-existing diseases, pre-morbid functional status, presenting symptoms and signs of the illness, investigation results, treatment, allied health services, duration of illness, duration of hospital stay if relevant, mortality as a result of the ILI episode, any functional or cognitive consequences as measured by the Barthel index (BI) and Mini Mental State Examination (MMSE). The activities of daily living (ADL) score was assessed using the BI which covers various dimensions of activities of daily living, with a total score of 20.11 In general a score of 20 is considered to represent independence, 15–19 represents mild to moderate functional limitation and a score of <15 represents severe limitation.12 The ADL score before illness was obtained from the records of the RCHE and the staff.
Sample size calculation
Currently, about 10% of residents of RCHEs have an ILI episode over a 1-year period. Assuming a SD of 4%, a total of 217 subjects or ILI episodes would need to be studied. ILI episodes in Hong Kong generally occur in two major peaks in late summer and winter, in addition to low level background occurrences. Assuming a 10% incidence, the number of episodes covering the two peaks over a 1-year period would be 2×0.1×1000 = 200. Additional episodes of 80 during the other periods would be expected. Assuming 10% were missed, the remaining episodes that could be studied would be 0.9×280 = 252.
Statistical analysis
The variations in the number of ILI episodes according to season and the prevalence of different aetiologies of ILI in RCHE are shown. The number of episodes each month was divided by the total number of residents in each RCHE to calculate the incidence, and the differences between the four seasons (December–February, March–May, June–August, September–November) and between the four homes were examined by the χ2 test. The clinical presentation, natural history and outcome according to the different causes of ILI were examined and tested for statistically significant differences using a χ2 test for categorical variables and ANOVA for continuous variables. Factors associated with mortality were examined using univariate analysis and the results presented as unadjusted odds ratios (ORs) per unit OR for continuous variables (body mass index, MMSE and ADL score) and per year for age, assigning an OR of 1 to the factor level used for comparison. The average cost of an ILI episode to the hospital authority was estimated in terms of bed-days occupied and drug costs using figures supplied by the hospital authority applicable to Shatin. The presence and titres of anti-influenza antibodies were correlated with influenza vaccination status using a χ2 test and an ordinal trend measure.
RESULTS
Incidence of ILI by RCHEs over a 1-year period
A total of 259 episodes of ILI occurred in 194 subjects; 77.8% of these subjects had one episode, 4.4% had two, 4.6% had three, 2.6% had four and one subject had five episodes. The number of ILI episodes and the incidence of ILI for each RCHE (calculated as the number of ILI episodes divided by the total number of residents) are shown in table 1. Overall, the incidence was slightly higher during January–March and April–June, although overall the incidence in different seasons did not reach statistical significance. However, the variation in incidence differed among the RCHEs, with all documenting the highest incidence in April–June with the exception of Caritas.
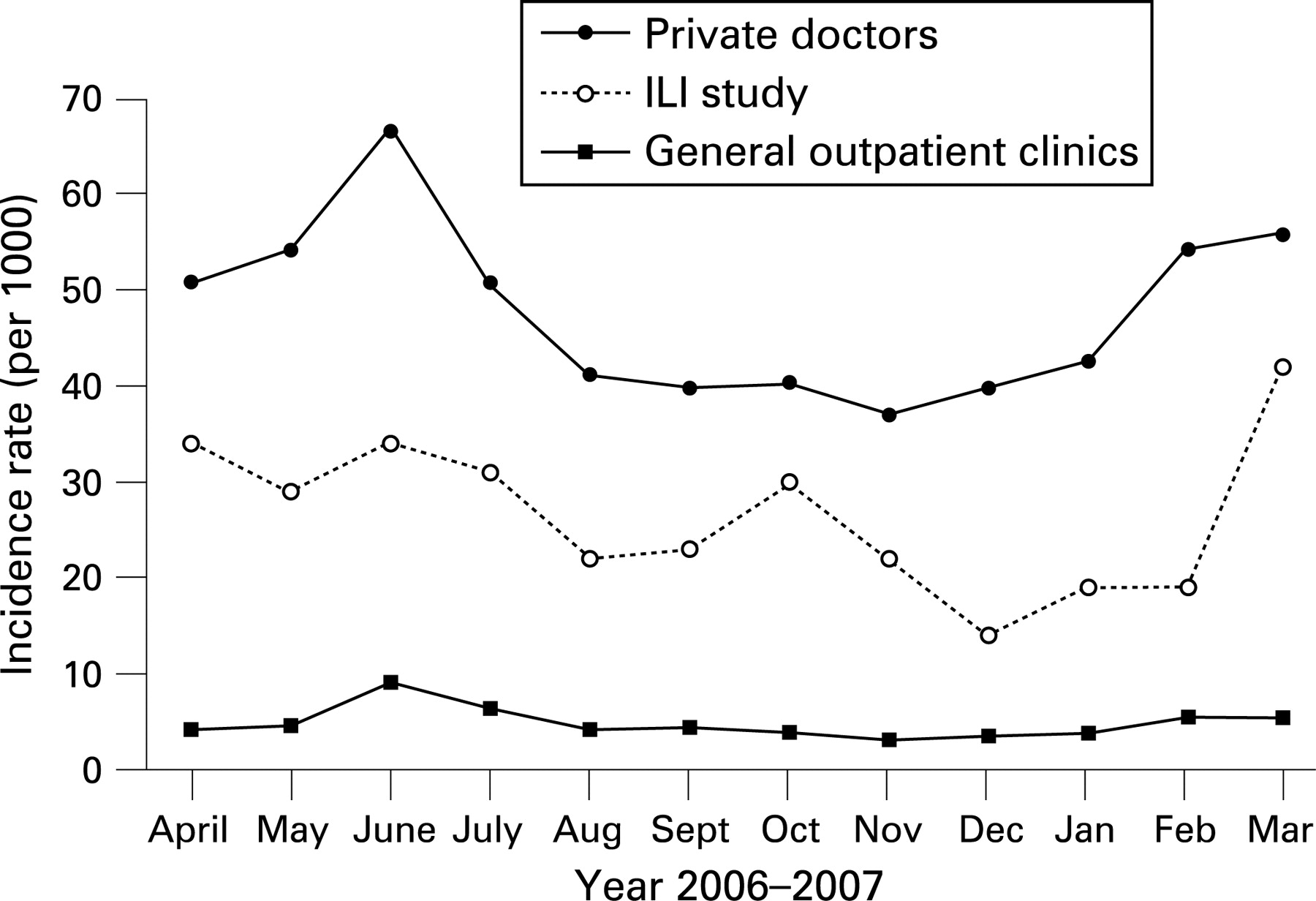
To examine whether the pattern of ILI was similar to the figures provided by the CHP for sentinel RCHEs, the incidence figure was converted to number/1000 (see fig. 1 in online data supplement). In comparison with the CHP data for the community (see fig 2 in online data supplement), the month-to-month variation showed some similarity with the rates from private doctors and general outpatient clinics in the rise in June and February–March, although the magnitude was less. The incidence for RCHEs was also lower than for the general community. These findings are compatible with the spread of infectious agents from the community to RCHEs via staff and visitors during episodes when infections are prevalent in the community, accounting for some of the variations in ILI in RCHEs.

{kind=link}
{kind=link}
Underlying aetiology of ILI in RCHEs
In this study, nasopharyngeal aspirates were processed in 256 of 259 episodes of ILI. Sputum for bacterial cultures was obtained in only 134 episodes. An infectious agent was identified in 61.4% of ILI episodes (table 2). Bacterial infections accounted for 53.3% and viruses were identified in 46.7%. In 42 ILI episodes (16.2%) two or more organisms were identified, and 27 episodes (10.4%) had positive viral-bacterial combinations. The top five causes in order of frequency were S pneumoniae, RSV, P aeruginosa, parainfluenza virus type 1 and hMPV. Seasonal variations in the organisms prevalent for ILI was observed: hMPV and parainfluenza virus type 3 from April to June, RSV and P aeruginosa from July to September, Chlamydophila sp, parainfluenza virus type l and S pneumoniae from October to December and S pneumoniae, RSV, influenza virus type A and human coronaviruses from January to March. For the latter period, RSV and coronavirus infections were equally prevalent as influenza A. In general, viral infections showed more seasonal variations than bacterial infections.
Among the bacterial infections, S pneumoniae was the commonest during the autumn and winter months. P aeruginosa was significant in the summer months, whereas Staphylococcus aureus (including methicillin-resistant S aureus (MRSA)) was among the top five bacteria. With the use of rapid molecular methods for detection,10 atypical organisms with C pneumoniae and M pneumoniae also contributed frequently among bacterial aetiologies. There were no marked differences in the frequency of organisms between the four institutions.
Clinical features and natural history
The results for all RCHEs are combined as there were no significant differences between them (table 3). The mean age of the patients was 85 years, with slightly more women than men. Presentation with “decrease in general condition” in terms of cognition, ADL and/or mobility was observed in 71%. Decline in physical function occurred in about 66% of patients as a result of the illness, while cognitive decline was also observed. 87% of the ILI episodes resulted in hospital admission despite the availability of healthcare consultation, investigations and drug treatment on site.
No particular clinical features were identified for any particular organism. Mortality was 9.7%. Factors associated with mortality were withholding of food (OR 3.37; 95% CI 1.22 to 9.27); lower BMI, lower ADL score during illness and the presence of MRSA and Klebsiella spp as underlying aetiological agents (table 4). The presence or absence of the pre-morbid diseases was not associated with mortality, but we did not collect data on disease severity.
Management included intravenous antibiotic in 87% of cases, oxygen and intravenous fluids in over 60% of patients, and extensive involvement of allied health staff. Food was withheld in 57% of patients as a result of concern over possible aspiration or aspiration that might have precipitated the ILI episode.
Costs to the hospital
The costs per ILI episode are shown in table 5. In calculating overall hospital costs, the figures supplied by the hospital authority for general medical beds for the Prince of Wales (acute) and Shatin (convalescent) hospitals were used, since these were the hospitals admitting cases from the four RCHEs.
Influenza vaccination status
Approximately 90% had received influenza vaccination, half within 6 months and half at 6–12 months. The lowest percentage of unvaccinated subjects was 4% in one subsidised home, but in the other three the percentages ranged from 26% to 37%. Among those vaccinated, 48% had received the vaccine within 6 months and 42% at 6–12 months. There was no significant difference in the occurrence of influenza A infection among those who did not receive vaccination, those receiving the vaccine within 6 months or those vaccinated at 6–12 months. There were no significant differences in age, sex, clinical features, duration of hospital stay or mortality between the three vaccination status groups.
Table 6 shows the influenza A antibody titre of the day 14 serum specimen in the three vaccine status groups. The results were significantly different between the three groups, with a trend for the group receiving vaccination to have higher titres and the unvaccinated group the lowest. The more recently vaccinated group was 3.0–27.5% more likely than the less recently vaccinated group to have a higher titre. However, the size of the Somers D value indicates a high degree of overlap in titre between the three vaccine status categories. Antibody was also detected in those who did not receive vaccination.
DISCUSSION
This study has shown that ILI represents a considerable burden of disease in RCHEs, with 87% of episodes resulting in hospital admissions. The clinical presentation of ILI in the elderly people was non-specific, accompanied by a decrease in general condition, and did not correspond to underlying aetiological agents. However, it led to functional and cognitive impairment, with a mortality of 9.7%. A diagnostic yield of identified organisms of 61.4% was achieved, facilitated by the use of rapid molecular methods.10 Bacterial infection accounted for a higher percentage of ILI than viral infection (53.3% vs 46.7%), and S pneumoniae remained the most common bacterial cause. The incidence of bacterial infections as the cause of ILI was comparable with the weekly incidence of 15–30 cases/1000 residents reported by Harling et al.7 The incidence partly reflected the trend of ILI in the community, but there was an underlying background level of ILI episodes that did not fluctuate with the season. From the 1980s onwards, the percentage of subjects with an identified underlying aetiology rose from 21%13 to about 40% in the 1990s,14 15 and up to 64% in the 2000s.8
In addition to S pneumoniae, P aeruginosa, other Gram-negative bacteria and S aureus (including MRSA) accounted for 19.8% of all aetiological agents identified. This is not surprising since many subjects have co-morbidities such as chronic airway diseases, whereas some might have aspiration pneumonia where Gram-negative organisms would be more commonly isolated. The data reaffirmed the importance of these multidrug-resistant bacteria in the aetiology of pneumonia in this setting.16 Pneumonia in non-ambulatory residents of nursing homes and other long-term care facilities epidemiologically mirrors hospital-acquired pneumonia17 and should be treated according to healthcare-associated pneumonia (HCAP) guidelines.18 19 Interestingly, atypical organisms including Chlamydophila and Mycoplasma, which are detected only by molecular methods, occurred with comparable frequency to H influenzae. Since 27 ILI episodes (10.4%) had positive viral-bacterial combinations, a proportion of bacterial infection could be superimposed on an initial viral infection with or without aspiration.
Viral aetiology was identified in this study in 46.7% of cases with positive aetiology, higher than the finding of 43% in a prospective community cohort surveillance of 533 subjects aged 60–90 years.20 The most common viruses in our study were RSV, parainfluenza 1 and 3 and hMPV, with influenza A ranked fifth. The use of the term “ILI” in Hong Kong tends to be equated with influenza A infection, with subsequent infection control implications; perhaps a broader term such as HCAP18 or—more precisely—nursing home acquired pneumonia (NHAP)8 would be more appropriate. Previous studies in community dwelling elderly individuals aged ⩾65 years have shown that RSV and hMPV were each responsible for as many hospital admissions for respiratory infection as influenza,21 and that hMPV is a common and ubiquitous human pathogen in children and elderly people, with outbreaks having been described in elderly patients in Japan.22
Seasonal variations in ILI episodes were mainly caused by variation in viral infections. Contrary to general assumptions, influenza A infections were more common only in January–March, and during this same winter period S pneumoniae caused more ILI episodes while CoV and RSV were equally prevalent. The current policy of influenza A vaccination in late autumn seems appropriate, and the introduction of pneumococcal vaccination in elderly subjects aged ⩾65 years may reduce further the rates and hospital admissions of these ILI infections.23
The clinical features of ILI were non-specific and no particular pattern could be attributed to any particular organism. The presentation is typical of acute illnesses occurring among the frail elderly population, accompanied by functional and cognitive decline and the occurrence of delirium. The impact of infective episodes on function have also been emphasised in other surveys,20 24 25 and reinforces the need to carry out comprehensive multidimensional assessment and rehabilitation in these patients to avoid a rapid spiral towards increasing dependence.
Only MRSA and Klebsiella were significantly associated with mortality; no association was observed for other organisms or the presence of premorbid conditions. The higher frequency of food being withheld among those who died could be a consequence of the severity of illness, or it might represent those who had aspirated as they were at the end of life stage while in the RCHE. The other factors were general features of frailty.
Antibiotics were prescribed in 87% of cases in this study. The introduction of rapid molecular methods for detecting a wider range of respiratory viruses will enable early de-escalation of antibiotics in patients with clinical improvement and with viral aetiology.10 We have recently shown that a combination of two or all three biomarkers (serum procalcitonin, neopterin and C-reactive protein) may improve the discriminatory power to delineate bacterial versus viral aetiology in patients presenting with lower respiratory tract infection.26 Interestingly, a large proportion of infections caused by P aeruginosa occurred in the summer months of July–September. Further risk factors may be examined to elicit subgroups that may be at risk for such infections. It has been shown that early initiation of appropriate antibiotic therapy improves outcome and reduces mortality.27 Thus, adequate cover for these drug-resistant organisms will need to be reviewed for these RCHE cases.
Similar to our observation in patients admitted to hospital for acute exacerbations of chronic obstructive pulmonary disease,28 there was no difference in the occurrence of influenza A between those who were vaccinated and those who were unvaccinated in this study, although neither study was designed to address the question of vaccine efficacy. Similarly, there was no marked difference in influenza A antibody titres between those who had received vaccination within 6 months and those who had received vaccination at 6–12 months, perhaps suggesting a longer lasting effect beyond 6 months.
This study was limited by the fact that only four RCHEs near the Prince of Wales Hospital were chosen so that specimens could be sent to the hospital quickly. There might be regional variations in the prevalence of infective organisms, although the pattern in this study is comparable to the CHP sentinel survey of ILI in RCHEs and the general community. Although the sputum pathogens included in the study were those that gave only heavy predominant or pure growth of the organism on cultures, it is recognised that a proportion might still represent colonisation in the background of chronic lung disease or prior use of antibiotics. The analysis of factors associated with mortality was based on univariate analysis and did not take into account the severity of illness and other possible confounding factors since the study was not primarily designed to address this question. In addition, we were not able to carry out direct observation of compliance with infection control policy, relying on reports only. Nevertheless, this represented a detailed clinical and microbiological study of ILI in RCHEs over a 1-year period, where the latest laboratory techniques yielded a very high rate of organism identification and information collected will be useful to guide future clinical management.
In summary, ILI represents a considerable burden of disease in RCHE, with 87% giving rise to hospital admissions. Clinical presentation of ILI in older people is non-specific and does not correspond to underlying aetiological agents. A large percentage of ILI is due to bacterial and viral infections other than influenza in the RCHE population.
REFERENCES
Supplementary materials
web only figures 63/8/690
Files in this Data Supplement:
Footnotes
Figs 1 and 2 are published online only at http://thorax.bmj.com/content/vol63/issue8
Funding: This project was funded by the Research Fund for the Control of Infectious Diseases (Health and Food Bureau, HKSAR) #04050452.
Competing interests: None.
Ethics approval: The study was approved by the ethics committee of the Chinese University of Hong Kong and appropriate informed written consent was obtained from the subjects or their immediate relatives.
Linked Articles
- Airwaves