Article Text

Statistics from Altmetric.com
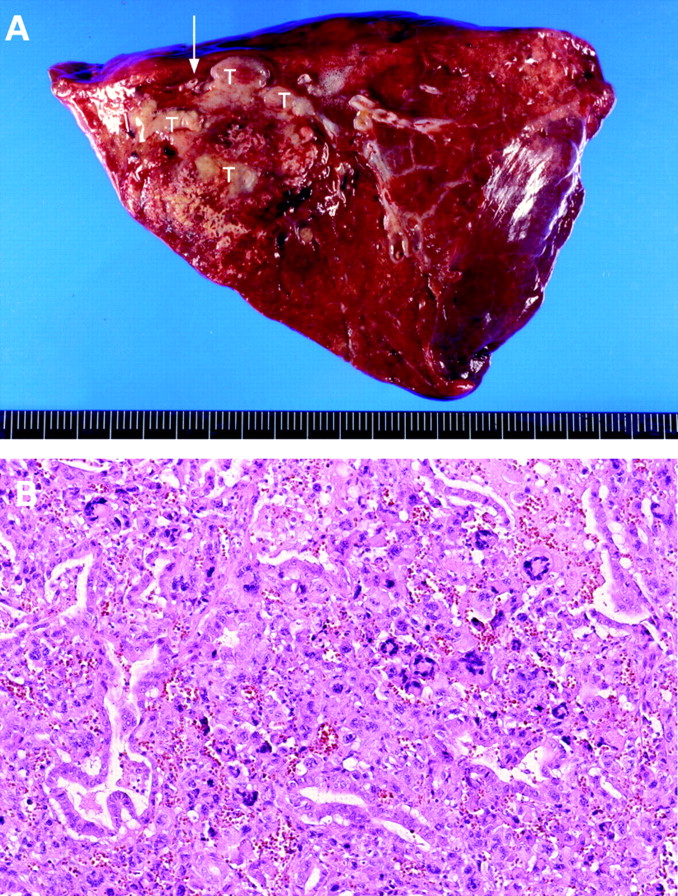
From the question on page 620.
Lobectomy was performed. The cut surface revealed a poorly circumscribed yellow to white firm area 9.0×6.5×6.0 cm which included a white necrotic tumorous lesion measuring 6.0×5.5×5.0 cm (fig 1A). A feeding artery, 0.3 cm in diameter, from the descending thoracic aorta was seen nearby. Pathological examination of the consolidated mass was consistent with an intralobar sequestration accompanied by obstructive pneumonia with dense infiltrations of lymphoplasma cells, foamy histiocytes and fibroblasts. The tumour demonstrated an adenocarcinoma admixed with spindle cells and pleomorphic cells (fig 1B) which showed cytokeratin and vimentin coexpression. The diagnosis of a pleomorphic carcinoma arising in an intralobar sequestration with frequent tumour emboli and regional lymph node metastases was made.

{kind=link}
Adjuvant chemotherapy with two cycles of navelbine was administered but was withdrawn owing to neutropenia. Hoarseness, exertional dyspnoea, productive cough and choking developed progressively. The patient was readmitted 3 months after surgery because of total occlusion of the left main bronchus, left upper lobe collapse, vocal cord palsy and right fourth rib metastasis with pathological fracture. Although a stent was inserted in the left main bronchus as palliative treatment, the patient died of right lung pneumonia with septic shock.
Pulmonary sequestration is rarely associated with lung cancer.1 ,2 In the previously reported four cases, three cases of squamous cell carcinoma and one case of adenocarcinoma developed within the sequestered lung. The relationship between pulmonary sequestration and lung cancer is uncertain. Complete resection of the malignant lesion with the sequestered lung was performed, and all the patients tolerated the surgery well.
Pleomorphic carcinoma, also known as monophasic sarcomatoid carcinoma, is a rare and aggressive pulmonary malignancy. This type of tumour shows concurrent presence of malignant epithelial and homologous sarcomatoid cell components by co-expressing cytokeratin and vimentin in various degrees. Men are affected far more frequently than women (13:3) and the disease is strongly associated with smoking. All of the patients succumbed to early distant metastases (range 2 weeks to 5 months). The prognosis is poor with a median survival of 3 months even when early-stage disease was diagnosed and resected.3 ,4
To our knowledge, this is the first case of a pleomorphic carcinoma arising in intralobar sequestration. Preoperative diagnosis of such a case is difficult. When pleomorphic carcinoma is encountered, the outlook is poor despite radical resection and adjuvant chemotherapy.5