Article Text

Abstract
Background: Most patients with cystic fibrosis (CF) die of respiratory failure due to chronic infection and destructive neutrophilic inflammation.
Objective: To identify potential therapeutic targets by characterising the neutrophil stimulating mediators in the CF airway.
Methods: Spontaneously expectorated CF sputum was extracted in phosphate buffered saline for assays of neutrophil chemotaxis, intracellular calcium mobilisation and cell shape change. Mediators were purified by ion exchange, C18 reversed phase and size exclusion chromatography.
Results: A pool of CF sputum contained considerable neutrophil stimulating activity but neutralisation of interleukin (IL)8/CXCL8 had little inhibitory effect on neutrophil chemotactic (10149 (2023) migrating cells vs 8661 (2597) at 62 mg sputum/ml; NS) or shape change (% forward scatter increase 46 (8) vs 38 (5) at 19 mg sputum/ml; p<0.05) responses. Furthermore, the CF sputum pool induced an elevation in intracellular calcium ions even after desensitisation of the neutrophils to IL8. Chromatography identified contributions to the neutrophil shape change inducing activity from IL8, other CXC chemokines, leukotriene (LT) B4 and two formyl peptides. There was also suggestive evidence for contributions from platelet activating factor (PAF) and C5a. Using non-chromatographed individual sputum samples, anti-IL8 alone did have an inhibitory effect on neutrophil chemotaxis (median inhibition 41%; p = 0.0002). However, even in this experiment, there were clearly significantly important, non-IL8 mediated, effects of CF sputum on neutrophils, and an inhibitor cocktail of anti-IL8 plus CXCR2, LTB4, formyl peptide, PAF and C5a receptor antagonists inhibited chemotaxis by a median of 97% (p = 0.0002).
Conclusion: Many chemoattractants contribute to the neutrophil stimulating activity in CF sputum although the relative contribution of these mediators differs in different patients. Selective blockade of single mediators may not be sufficient to control neutrophil recruitment and activation in the CF airway.
Statistics from Altmetric.com
Cystic fibrosis (CF) is characterised by cycles of infection and predominantly neutrophilic inflammation. There is debate as to whether infection causes inflammation, or the CF airway is itself proinflammatory, even in the absence of infection.1–4 Late on, both are consistently present, and it is generally believed that the major cause of the airway damage that ultimately leads to respiratory failure is the excessive host response. Modulation of this response by prednisone is beneficial, but with unacceptable side effects,5 ,6 and inhaled corticosteroids are largely ineffective.7 There is a need for more specific immunomodulators and, in this context, understanding the neutrophil recruiting mediators is important.
The potent neutrophil chemoattractant interleukin (IL)8/CXCL8 is increased in CF samples,8–10 but there are many other potential candidate molecules apart from IL8. Several other CXC chemokines, containing the ELR motif immediately before the first of the conserved cysteines, are capable of stimulating neutrophils, including growth related oncogene α (GRO-α/CXCL1), GRO-β/CXCL2, GRO-γ/CXCL3, epithelial derived neutrophil activating protein 78 (ENA-78/CXCL5), granulocyte chemotactic protein 2 (GCP-2/CXCL6) and neutrophil activating protein-2 (NAP-2/CXCL7).11–15 IL8 and GCP-2 can act via CXCR1 or CXCR2, both receptors being present on neutrophils, whereas the other ELR+ CXC chemokines only signal through CXCR2.16 ,17
CXC chemokines are cationic and may bind to the anionic DNA that is released from necrotic cells in the CF lung, thus preventing the chemokines from binding to neutrophil receptors.18 For this reason, non-chemokine mediators may be of considerable importance in the excessive neutrophil recruitment in the CF lung. Potential non-chemokine neutrophil stimulating mediators include bacterial derived peptides (such as N-formyl-L-methionyl-L-leucyl-L-phenyalanine), host derived peptides (such as N-acetyl-Pro-Gly-Pro, a degradation product of the extracellular matrix), complement activation products (such as C5a) and lipid mediators (such as leukotriene (LT) B4 and platelet activating factor, PAF).19–22 To our knowledge, only two of these mediators, LTB4 and C5a, have so far been identified in CF airway samples.23–27
The relative importance of these mediators to CF pathology is not known. As neutrophil stimulating mediators play such a vital role in the detrimental inflammatory response seen in patients with CF, their characterisation may improve understanding of the pathogenesis of CF and enable potential therapeutic targets to be identified. We hypothesised that multiple neutrophil chemoattractants are present in CF sputum, many of which have been poorly studied. The aim of this study was therefore to characterise the range of mediators present in CF sputum, using a variety of neutrophil stimulating assays.
METHODS
Patients
We collected spontaneously expectorated sputum from 22 patients with CF, diagnosed on conventional criteria28 and described in table 1, at the Royal Brompton Hospital (London, UK). Spirometry was performed to ATS standards.29
Sputum supernatant
Sputum from patients with CF was pooled (pool 1, see online supplement table 1), homogenised in phosphate buffered saline (PBS, 300 mg sputum/ml), centrifuged and the supernatant recovered was stored as aliquots at −20°C. Individual sputum samples were homogenised at 100 mg/ml.
Cell preparation
Mixed granulocytes were isolated from the peripheral venous blood of healthy human volunteers and resuspended in assay buffer (AB; PBS without Ca2+ Mg2+ containing 0.1% bovine serum albumin, 10 mM glucose, 10 mM HEPES (Invitrogen, Paisley, UK), pH 7.2–7.4). For chemotaxis and CD11b assays, the cells were supplemented with Ca2+ and Mg2+ (0.9 mM and 0.5 mM, respectively).
Chemotaxis
Chemotactic responses were examined using 96 well chemotaxis plates (ChemoTx, Gaithersburg, Maryland, USA) with 3 μm pore size polycarbonate filters, as described previously.30 Results are expressed as the mean number of migrated cells, as counted by flow cytometry.
Leucocyte shape change
Shape change responses of mixed granulocytes were analysed as previously described.31 Briefly, mixed granulocytes were stimulated at 37°C for 4 min, after which their cell shape was maintained by fixation and analysed by flow cytometry. A minimum of 1000 neutrophil events were acquired using the FL-2 fluorescence channel, allowing neutrophils to be distinguished from eosinophils by their lower autofluorescence. Results are expressed as percentage increase in forward scatter compared with buffer treated cells.
CD11b upregulation
Upregulation of this integrin was measured by use of FITC labelled anti-CD11b and flow cytometry, as described previously.32
Intracellular calcium ion mobilisation
Intracellular calcium mobilisation responses were examined using the fluorescent indicator FURA-2, as previously described.33 Changes in fluorescence emitted at 510 nm were measured after stimulation at 340 and 380 nm. Results are expressed as the relative increase in fluorescence compared with baseline.
ELISA
Inflammatory mediators were measured by specific sandwich ELISAs.
Chromatography
To estimate the range of neutrophil stimulating mediators, sputum was pooled (n = 4–6 patients with CF), homogenised in appropriate buffer, centrifuged and the supernatant applied to combinations of ion exchange, C18 reversed phase and size exclusion chromatography protocols (see online supplement table 1). Fractions collected were analysed by the cell shape change bioassay which provides a rapid and sensitive indicator of potential chemoattractant mediators.
Statistical analysis
Experimental data are presented as mean (SEM), unless otherwise stated. Effects of inhibitors on concentration response curves were analysed using the repeated measures ANOVA with Bonferroni’s post test. Effects of inhibitors on single concentrations of mediators or chromatography fractions were analysed with the Student’s paired t test. The effects of inhibitors on sputum from 13 individual patients with CF were analysed by non-parametric methods (Wilcoxon test). Statistical analyses were performed on raw data, using GraphPad Prism V.3.02. There were insufficient data in the literature to inform a prior power calculation.
RESULTS
We recruited 22 patients with CF and their details are summarised in table 1.
Sputum from six patients with CF was pooled (pool 1, online supplement table 1), homogenised in PBS, centrifuged and the supernatant used in a variety of neutrophil stimulation assays. There was considerable neutrophil stimulating activity (eg, significant responses were detected at concentrations as low as 7.8 mg sputum per ml extract in chemotaxis assays and 1.2 mg/ml when cell shape change was measured). In the chemotaxis assay, cell migration was observed when the CF sputum supernatant was added to the lower chamber but not when added to the cells in the upper chamber, indicating that migration was a truly directional chemotactic response, rather than a more random chemokinetic response (data not shown). Chemotaxis to the CF sputum supernatant was much greater than could be explained by the IL8 concentration and was not significantly inhibited by an excess of neutralising anti-IL8 antibody (fig 1A). Indeed, CF sputum supernatant was more efficacious than IL8, inducing a higher maximum neutrophil response. Similar discrepancies between CF sputum and IL8 were found in assays of neutrophil cell shape change (fig 1B) and CD11b upregulation (online supplement fig 1). These results indicate that IL8 is not the sole, and probably not the major, neutrophil stimulating mediator in the CF airway.

To verify the presence of mediators other than IL8, we used Fura-2 loaded neutrophils to measure kinetic changes in intracellular calcium ion concentrations in response to the successive administration of different test samples. Repeated administration of IL8 induced desensitisation of the calcium elevation response to this mediator but the cells still responded to the subsequent addition of CF sputum supernatant (fig 2A). In contrast, when the neutrophils were first desensitised to the CF sample, they were unresponsive to subsequent IL8 (fig 2B). To establish that the cells were still responsive to another stimulus, despite being desensitised to sputum components, we used PAF as the final addition. PAF always induced a calcium ion elevation response showing that the cells were still capable of responding to appropriate stimuli (fig 2). However, this response (relative increase in fluorescence 0.32 (0.12)) was less than that seen when PAF was added as the first stimulus (data not shown, relative increase in fluorescence 1.59, mean of two cell preparations). This may indicate an overall decline in responses with successive additions to the cells but it also raises the possibility of a partial desensitisation to PAF by the CF sputum. The results again suggest the presence of substantial neutrophil stimulating activity other than IL8, possibly including PAF, in the CF sputum.

To examine the range of neutrophil stimulating mediators in CF sputum, we performed different chromatography protocols, each using a different pool of sputum (see online supplement table 1). The fractions collected were analysed for their ability to induce neutrophil shape change in the absence and presence of a CXC chemokine blockade consisting of anti-IL8 plus a CXCR2 antagonist to inhibit responses to other ELR+ CXC chemokines. Firstly, we verified that the bioactivity was unaffected by exposure of the sputum supernatant to trifluoroacetic acid (TFA) and acetonitrile (data not shown) which permitted the use of these reagents in the versatile and potentially highly resolving C18 reversed phase high pressure liquid chromatography (HPLC).
Sputum (pool 2) was extracted in TFA containing 1.0 M NaCl and the soluble fraction applied to C18 HPLC (fig 3A). The salt insoluble pellet was then re-extracted in TFA at a low salt concentration and applied to C18 HPLC (fig 3B). Both extracts contained neutrophil stimulating activity which separated into many fractions, indicating the range of mediators present. While the bioactivity in some fractions was inhibited by the chemokine blockade, indicating the presence of CXC chemokines, there were clear suggestions of the presence of non-chemokine mediators. Furthermore, while the low salt re-extract of the pellet contained less bioactivity than the high salt extract, the low salt sample contained a higher proportion of more hydrophobic mediators which were unaffected by the chemokine blockade (fig 3), again indicating the range of different neutrophil stimulating mediators in CF sputum.

These high and low salt fractions contained a total of 8.7 pmol IL8, 2.4 pmol GRO, 1.1 pmol ENA-78 and 0.2 pmol GCP-2 per gram of sputum but no detectable NAP-2. GRO (the ELISA does not distinguish between GRO α, β or γ) eluted before IL8 and probably accounts for some of the activity in high salt fraction 4 (the proportion that was partially inhibited by the CXC chemokine blockade, fig 3A). GCP-2 can stimulate neutrophil CXCR1 and is the only ELR+ CXC chemokine that is not inhibited by the combination of anti-IL8 and the CXCR2 antagonist. However, there was insufficient GCP-2 to have accounted for the neutrophil stimulating activity in the fractions at the dilutions used. We also measured a total of 7.6 pmol C5a, a complement derived chemoattractant protein of similar molecular size to the chemokines, per gram sputum.
High salt fraction 4 and a pool of high salt fractions 13+14, which were largely resistant to inhibition by the chemokine blockade, were selected for further analysis using size exclusion chromatography. We detected neutrophil stimulating activities of approximately 25 kDa (unidentified), 8–12 kDa (likely to be the CXC chemokines previously detected) and two low molecular weight activities, differing in both hydrophobicity and molecular size, that were inhibited by a formyl peptide FPR receptor antagonist (see online supplement fig 2).
The second chromatography protocol used a combination of chemistries. The sputum extract (pool 3) was separated into three ion exchange fractions (cationic, anionic and the breakthrough from both cationic and anionic columns) which were then applied separately to C18 reversed phase HPLC for subsequent bioassay. The cationic fraction contained neutrophil stimulating activity that eluted as a single peak from C18 HPLC and was completely inhibited by the CXC chemokine blockade (see online supplement fig 3A). The anionic fraction contained little detectable bioactivity (see online supplement fig 3B). The breakthrough fraction separated into two clear C18 peaks, the first of which may have contained a mixture of formyl peptide(s) plus some chemokine(s) (we found that approximately 28% of the sputum IL8 unexpectedly broke through the cation exchange column, perhaps because of binding to DNA). More interestingly, the second peak was substantially inhibited by an LTB4 BLT1 receptor antagonist (see online supplement fig 3C).
We have thus identified a contribution of IL8, other CXC chemokines such as GRO, formyl peptides and LTB4, and a possible contribution from C5a and PAF, to the neutrophil stimulating activity in CF sputum. Next, we used a CF sputum extract in PBS (pool 1) and various inhibitor combinations to determine the relative contributions of these mediators to the overall bioactivity. The CXC chemokine blockade and the LTB4 receptor antagonist each significantly inhibited the neutrophil shape change response, but only to a small extent (see online supplement fig 4A, B), but there was no detectable inhibition by the formyl peptide receptor antagonist (see online supplement fig 4C). However, a combination of anti-IL8 plus antagonists to CXCR2, BLT1 and FPR inhibited neutrophil responses to a much larger degree (64 (10)%, p<0.001; see online supplement fig 4D). This substantiates the HPLC data of a mixture of neutrophil stimulating mediators that contribute to the overall activity in CF sputum. To investigate the potential contribution of C5a or PAF, we used antagonists to their receptors and found no significant inhibitory activity when the antagonists were tested individually (see online supplement fig 4E, F). In contrast, addition of C5a and PAF receptor antagonists to the inhibitor combination described above produced a greater inhibitory effect (96 (4)%, p<0.001; see online supplement fig 4g). These data underline the complexity of the neutrophil stimulating mediators in CF sputum.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
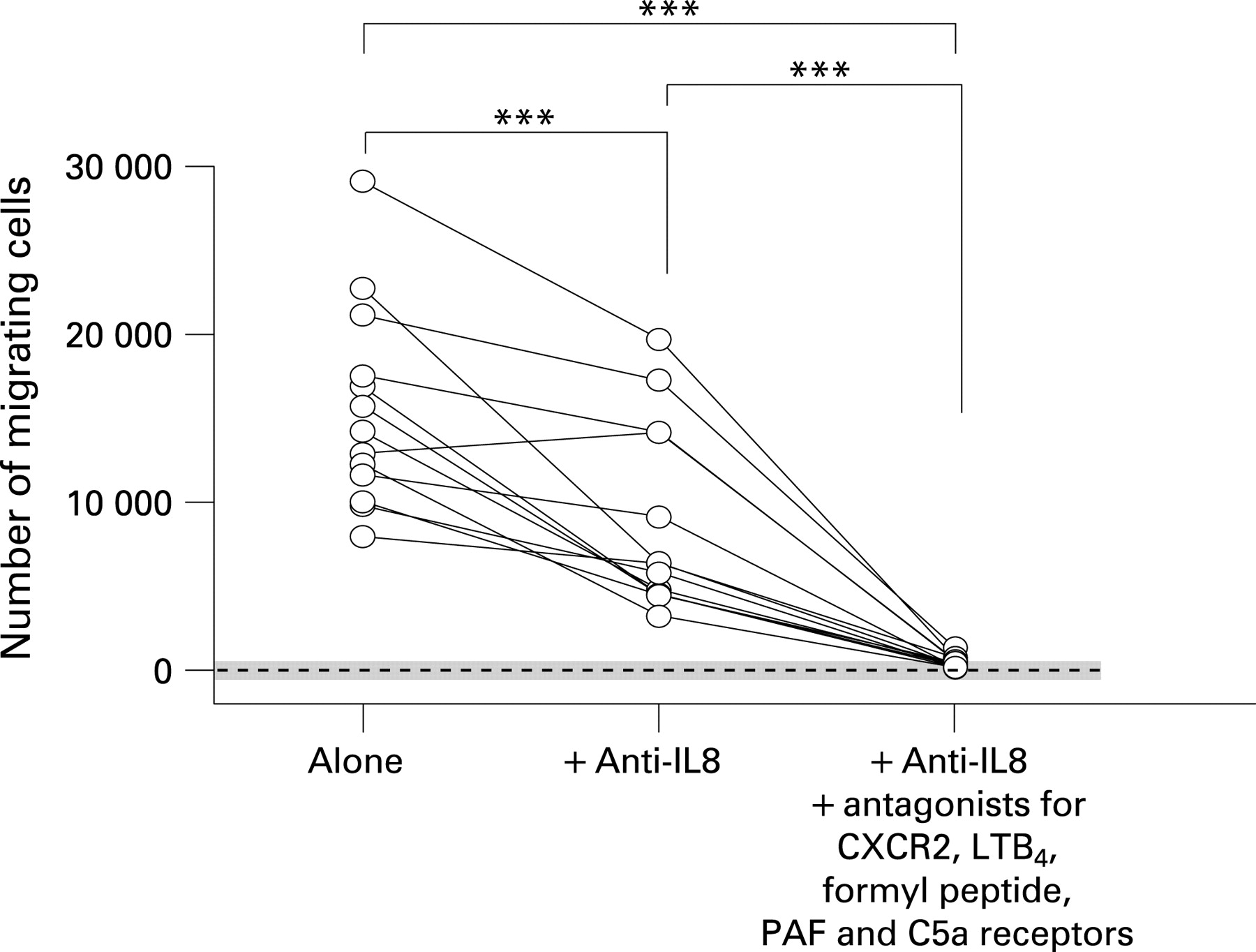
All experiments so far have been performed on pools of sputum to investigate the range of neutrophil stimulating mediators that are likely to be present in at least some patients with CF. To test our findings in a cross section of patients, sputum samples were homogenised individually and the supernatants assayed for neutrophil chemotaxis at a single concentration of 50 mg sputum/ml (fig 4). There was a wide range in responses, indicating different overall activity in samples from different patients, and a partial inhibition in the presence of anti-IL8 (median inhibition 41% (range −10 to +73%); p = 0.0002). However, inhibition of the wider range of mediators that we have found to contribute to activity in CF sputum resulted in a much more effective inhibition (median inhibition 97% (range 90–99%); p = 0.0002). These results confirm the presence of multiple neutrophil stimulating mediators in the sputum of the majority of patients with CF.
DISCUSSION
Neutrophils are important cells in the inflammatory pathogenesis of CF and knowledge of the mediators that recruit neutrophils to the CF airway has been sought by many investigators.8–10 ,23–27 However, many of these studies have focused on specific, often single, candidate mediators without regard to the complex nature of the inflammatory response. This study has characterised the range of neutrophil stimulating mediators in CF sputum by use of specific inhibitors and a variety of chromatographic methods. We have found evidence for a contribution of IL8, the related CXC chemokine GRO, LTB4 and two distinct formyl peptides to the neutrophil stimulating activity of CF sputum. In addition, there was suggestive evidence that C5a and PAF might also play a role.
IL8 has been the most widely implicated neutrophil chemoattractant in CF disease. However, we found that inhibition of IL8 with a monoclonal antibody had only a partial effect on the neutrophil stimulating activity of CF sputum in a variety of assays when pooled sputum was used. When looking at individual sputum samples there was a significant effect of anti-IL8, suggesting that IL8 may play a more important role in some patients with CF than others; further studies in patients with CF lung disease of different severities are needed to explore this further. Furthermore, blockade of responses to other CXC chemokines also had little effect. As IL8, and possibly other CXC chemokines, may be inhibited by the large amount of DNA in the CF lung,18 the non-chemokine mediators described in this article may be more important in CF airway disease.
We have corroborated results from other studies that LTB4 is indeed present and active in CF samples.25 ,26 However, blockade of the BLT1 receptor had little effect on neutrophil shape change induced by CF sputum. The presence of formyl peptides in CF sputum is not surprising based on the high degree of bacterial infection seen in these patients and the report of a size exclusion fraction that acted on the formyl peptide receptor.34 Indeed, we found evidence for at least two formyl peptides of different size and hydrophobicity that appear to act on the same neutrophil receptor. Blockade of this receptor had no detectable effect on the activity in CF sputum. In contrast, the combined blockade of responses to IL8, other CXC chemokines, LTB4 and formyl peptides produced a 64 (10)% inhibition of the neutrophil response to CF sputum.
The above mentioned mediators were clearly defined by use of specific inhibitors of the bioactivity in chromatography fractions. There was also suggestive evidence that C5a and PAF might contribute to the neutrophil stimulating activity in CF sputum. C5a has been suggested to contribute to CF disease24 and the levels of immunoreactive C5a that we found in reversed phase chromatography fractions of CF sputum would be expected to contribute to the neutrophil stimulating activity detected. Despite this fact, none of the activities that we isolated from CF sputum could be ascribed to this mediator. PAF is a phospholipid mediator that is usually rapidly metabolised to the inactive lyso-PAF metabolite although airway epithelium has the potential to reverse this process, at least transiently.35 Thus it is often difficult to detect bioactive PAF and we are not aware of any studies demonstrating PAF in CF sputum. However, the PAF receptor has a rather broad specificity and recognises a number of bacterial lipids.36 Thus the suggestion of an activity in CF sputum that partially desensitised Fura-2 loaded neutrophils to PAF was sufficient to warrant the use of a PAF antagonist in later studies. C5a and PAF receptor antagonists, used separately, did not inhibit neutrophil shape change responses to CF sputum. However, the addition of these antagonists to the combined blockade of CXC chemokines, LTB4 and formyl peptides mentioned above resulted in a 96 (4)% inhibition of the neutrophil response to CF sputum. Similarly, in cross sectional studies, this complex mixture inhibited neutrophil chemotaxis by a median of 97% (range 90–99%), whereas the inhibitory effect of anti-IL8 alone was a more variable median 43% (range −10% to 73%).
Thus CXC chemokines, LTB4, formyl peptides and one or both of C5a and PAF account for a substantial proportion of the neutrophil stimulating activity in CF sputum. We also found evidence for two mediators that were only partially characterised owing to their minor contribution. One of these has an apparent molecular weight of 25 000 but was detected in only one pooled sputum sample. The second unidentified mediator (data not shown) had molecular weight and hydrophobicity characteristics of a lipid mediator. Lipids such as hepoxilin A3 have been shown to promote the migration of neutrophils through epithelial cell monolayers37 but a role for this lipid in CF has not been defined.
While we have identified a complex mixture of neutrophil chemoattractants in sputum, it is difficult to predict their relative importance in the lung of patients with CF. In vitro studies have demonstrated an intracellular signalling hierarchy that may determine the chemoattractant to which the neutrophil will respond.38 For example, there is a predominant attraction by even low concentrations of end stage chemoattractants, such as formyl peptides and C5a, over intermediary chemoattractants such as IL8 and LTB4.
We used pools of sputum, for the most part from patients in whom an infective exacerbation had been diagnosed by an independent physician, because we wanted to maximise our chances of capturing as many mediators as possible. While we have shown that IL8 has a partial contribution to neutrophil stimulating activity in CF, we have not demonstrated the full range of mediators in individual patients. Pooling sputum, and the cross sectional design, means that we cannot assess the pathophysiological significance of the individual mediators we found. We also cannot say whether these mediators are important in very early stage disease, since all of our patients were spontaneously expectorating sputum, and thus by definition had disease of at least moderate severity. Further cross sectional studies looking at patients with a range of disease severities, and longitudinal studies, observing the changes in individual mediators over time and with treatment, are needed to see which have significance at particular stages of the disease. It is probable that the CF airway contains a mixture of neutrophil stimulating mediators from different sources in response to variations in disease severity in the patient.
It is also possible that treatment for CF with, for example, macrolide antibiotics may mean that some mediators are not detected.39 ,40 We accept that ideally we would have studied patients who were not taking azithromycin, but the benefits of this antibiotic are well known,41–43 and so its use is so widespread that it is difficult to find many patients with moderate lung disease who are not currently taking macrolides.
In conclusion, this study has demonstrated the presence of several neutrophil stimulating mediators in CF sputum. The inhibition of neutrophil responses achieved by a combination of inhibitors of CXC chemokines, LTB4 and formyl peptides suggests that these mediators, probably in combination with lipids acting on the PAF receptor and/or C5a, are the key players in neutrophil recruitment in the CF airway. Selective blockade of single mediators was usually insufficient to markedly reduce the neutrophil stimulating activity. These findings suggest a broader targeting of neutrophil stimulating mediators may be required to reduce the accumulation of neutrophils in the CF airway and result in beneficial treatment for patients.
Acknowledgments
The authors thank the children and families who took part in this study and the physiotherapists at the Royal Brompton Hospital for their help in collecting samples. They also thank Pfizer for the use of their UK-74,505 PAF receptor and CP-105,696 LTB4 receptor antagonists.
REFERENCES
Supplementary materials
web only appendices 63/7/614
Files in this Data Supplement:
Footnotes
Details of methods and data supplements are published online only at http://thorax.bmj.com/content/vol63/issue7
Funding: Cystic Fibrosis Trust PhD studentship RS21 (KJM) and Asthma UK (PJJ).
Competing interests: None.