Article Text

Abstract
Background: The combination of salmeterol and fluticasone propionate (SFC) and tiotropium bromide (TIO) are commonly used treatments in chronic obstructive pulmonary disease (COPD) but there are few data on their effectiveness when used together. We compared the effects of SFC 50/500 μg twice daily in addition to TIO 18 μg once daily with the individual treatments alone.
Methods: 41 patients with COPD participated in a randomised, double blind, double dummy, three way crossover study with 2 week washout periods between treatments. Lung function assessment included plethysmography and spirometry. The primary end point was post-dose specific airways conductance (sGaw) area under the curve (AUC0–4 h) on day 14.
Results: AUC0–4 h sGaw was significantly higher on day 14 after SFC+TIO compared with TIO (22%) or SFC alone (27%) (both p<0.001). SFC+TIO significantly improved trough forced expiratory volume in 1 s compared with TIO alone (212 ml, p<0.001) and SFC alone (110 ml, p = 0.017) on day 14. Inspiratory capacity measurements also showed significant benefits for triple therapy over individual components on day 14. Subjects receiving SFC+TIO had clinically relevant improvements in Transition Dyspnoea Index (TDI) total score of 2.2 compared with TIO alone (p<0.001) (but not SFC alone, 0.7; NS) and used significantly less rescue medication (1.0 occasion less daily than TIO (p<0.001) and 0.6 less than SFC (p = 0.01)).
Conclusion: SFC+TIO triple therapy led to greater improvements in bronchodilation compared with TIO and SFC alone. The advantages of triple therapy are observed across a range of physiologically important parameters, including airway conductance and lung volumes. Triple therapy also led to patient related benefits by improving TDI and use of rescue medication.
Trial registration number: NCT00325169.
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is a multi-component disease with inflammation playing a key role, even in the early stages.1 It is characterised by airflow obstruction that is both progressive and poorly reversible.2 Drug treatments for COPD aim to control symptoms, maximise pulmonary function and reduce exacerbation rates.2 The inhaled anticholinergic tiotropium (TIO) provides effective bronchodilation over 24 h and reduces symptoms.3 ,4 These effects are associated with a reduction in exacerbation rates.5 The long acting beta agonist (LABA) salmeterol is an alternative inhaled bronchodilator therapy and is often prescribed in a combination inhaler with the anti-inflammatory corticosteroid fluticasone propionate (FP).6–9 This combination of salmeterol and FP (SFC) has demonstrated a broad range of anti-inflammatory effects10 that are greater than those seen with inhaled corticosteroid (ICS) monotherapy11 and the likely explanation for this is a molecular interaction (synergy) between the LABA and ICS.12 The anti-inflammatory and bronchodilator effects of SFC provides greater symptom control, pulmonary function improvement and exacerbation reduction compared with either of the individual component treatments.9
Current COPD guidelines recommend that long acting bronchodilators should be used in patients who are symptomatic despite therapy with short acting bronchodilators. ICS therapy is reserved for patients with a forced expiratory volume in 1 s (FEV1) of ⩽50% predicted, who are having two or more exacerbations requiring treatment with antibiotics or oral corticosteroids in a 12 month period.2 ,13 “Triple therapy” with long acting anticholinergics, LABA and ICS is widely used in clinical practice. The components of triple therapy have different molecular mechanisms of action, so there is a good rationale for the use of these drugs together to maximise clinical benefits.14–16 However, there is limited evidence to support the superiority of triple therapy over other combinations. In a 1 year study in patients with COPD, “triple therapy” with TIO plus SFC was compared with TIO plus salmeterol or TIO alone, and found to be the most effective therapy in terms of improvement in pulmonary function and symptom control.16 Additionally, a pilot study in patients with severe COPD showed a benefit for triple therapy over SFC alone and TIO alone for pre-dose morning FEV1 at 3 months.17 A formal power calculation for this pilot study does not appear to have been performed, and the authors state that false negative results for lung function changes at earlier time points may be attributed to insufficient statistical power. Properly statistically powered studies are needed to fully define the pulmonary function advantages of triple therapy when compared with SFC alone and TIO alone. Information regarding the effects of triple therapy on measurements of both airflow obstruction and hyperinflation are needed.
Here we report a double blind, placebo controlled, crossover study in patients with COPD evaluating the effects of triple therapy for 2 weeks with SFC and TIO compared with treatment with SFC alone and TIO alone. We assessed whether triple therapy had pulmonary function benefits after the first dose, or whether this effect occurred only after 14 days of therapy. We used the sensitive pulmonary function measurement of specific airway conductance as the primary end point to compare the different treatment regimens.18–21 Pulmonary function measurements of spirometry and lung volumes were also performed, and symptom scores were evaluated.
METHODS
Patient population
Patients were recruited between December 2005 and August 2006 in five centres from the UK and Belgium. We recruited patients with COPD diagnosed according to current guidelines. Patients were required to meet the following inclusion criteria: aged 40–80 years, smoking history of ⩾10 pack years, post-bronchodilator FEV1 >30% to ⩽75% predicted normal, post-bronchodilator FEV1/forced vital capacity (FVC) ratio ⩽70% and a minimum score of ⩾2 on the modified Medical Research Council Dyspnoea Scale. Exclusion criteria were a diagnosis of asthma, any respiratory disorder other than COPD, previous lung surgery, current pulmonary rehabilitation, regular long term oxygen use ⩾12 h per day, exacerbation or use of parenteral or oral steroids or change in COPD medication in the 4 weeks before randomisation, a course of antibiotics in the 8 weeks before randomisation and hospitalisation within the past year for an exacerbation. All patients gave written informed consent and the study protocol was approved by the appropriate institutional review boards and conducted in accordance with good clinical practice guidelines and the 1996 version of the Declaration of Helsinki.
Study design
This was a randomised, double blind, double dummy, three way crossover study. Patients entered a 2 week washout period at the start of which they discontinued all existing COPD medications. Eligible patients were then randomised to one of six treatment sequences. Each patient received all three treatment options of SFC 50/500 μg twice daily, TIO 18 μg once daily or SFC 50/500 μg twice daily plus TIO 18 μg once daily for 2 weeks in a randomised double blinded fashion. There were 2 week washout periods between treatment periods. After randomisation, the only medication allowed in addition to the study medication was salbutamol for relief therapy. Patients could also take smoking cessation therapy if required. Pulmonary function measurements were performed on the first day of each treatment period (day 1) and on day 14. Patients were asked to withhold rescue salbutamol for 6 h prior to the visit on days 1 and 14.
The total study duration was 13 weeks. Post-randomisation, patients were reviewed for safety purposes every 2 weeks for 10 weeks and patients attended a final visit 1 week after the end of treatment or study withdrawal. Double blind study medication was provided as matched Diskus/Accuhaler inhalers (GlaxoSmithKline, UK) and Handihalers (Boehringer Ingelheim, Germany). Treatment compliance was assessed at each post-treatment study visit by recording the number of doses remaining in each returned Diskus/Accuhaler inhaler and the number of capsules returned.
Pulmonary function
During each treatment period, body plethysmography measurements of specific airway conductance (sGaw) were performed before the first administration of study drug on day 1, and then at 30, 75, 120 and 240 min post-dose. This was repeated on day 14. Spirometric measurements of FEV1 and FVC were performed pre-dose (trough value) on days 1 and 14, and also at 2 h and 4 h post-dose. Inspiratory capacity (IC), residual volume (RV) and total lung capacity (TLC) measurements were also obtained at these time points. sGaw, functional residual capacity, vital capacity and IC were measured in a constant volume plethysmograph (Sensormedics Vmax 6200). TLC and RV were then calculated from these parameters. Body plethysmograph measurements were performed in triplicate and the mean used for analysis.
Diary cards and symptoms
Patients were given daily record cards to measure morning peak expiratory flow (PEF) and the number of occasions they used rescue medication over a 24 h period. The Baseline Dyspnoea Index was recorded at the end of the run-in, and the Transition Dyspnoea Index (TDI) score was assessed by study staff on day 14 of each treatment period.
Safety
Safety was assessed at each clinic visit by documenting all adverse events and measuring vital signs.
Statistical methods
The treatment comparisons, which were considered of equal importance, were SFC+TIO versus TIO and SFC+TIO versus SFC. Based on previous data,18 a treatment decrease of 15% in sGaw on the individual treatments compared with the combination was defined as clinically relevant. To detect a decrease of 15% in AUC(0–4 h) sGaw between one of the individual treatments and SFC+TIO with 90% power, a two sided 0.025 significance level and a within subject SD of 0.1652 (log transformed sGaw), it was estimated that 30 subjects would be required to complete at least two active treatment periods. The primary population for the analysis of efficacy was the modified intention-to-treat (MITT) population and this was used for the analysis of all efficacy end points. The MITT population comprised all subjects who were randomised and who, during each of at least two treatment periods, received at least one dose of study treatment and completed the baseline and at least one post-treatment efficacy assessment.
The primary efficacy end point was specific airway conductance AUC(0–4 h) sGaw on day 14. sGaw AUC(0–4 h) was log transformed and then analysed using a mixed model with treatment, period, baseline and mean baseline included as fixed effects, and subject fitted as a random effect. Analyses were adjusted for baseline (the pre-dose value on day 1) and mean baseline (the mean of the three baselines for each subject) to account for the subject’s status at the beginning of each treatment. The Kenward and Roger method22 for approximating the denominator degrees of freedom and correcting for bias in the estimated variance–covariance matrix of the fixed effects was used.
Treatment ratios for the comparison of SFC+TIO with each individual treatment (TIO and SFC) were calculated by taking the anti-log of the difference between least square means, and 97.5% confidence interval (CI) was calculated using pooled estimates of variance for the difference and then anti-logged for reporting. Adjusted means and differences in logged data were thus converted to geometric mean ratios. An adjusted geometric mean ratio would be exactly equal to 1 if there was no difference between the treatments or time points compared. A value higher than 1 indicates a positive difference and a value less than 1 a negative difference.
The 97.5% CI was used to draw conclusions regarding the relative efficacy of the treatments in order to account for the two equally important treatment comparisons, with a p value of ⩽0.025 being significant. The 2 week washout period between treatment periods was considered sufficient to ensure subjects were in a similar condition at the start of each treatment period. Treatment by period interaction and carryover effects were not formally investigated. Secondary end points included FEV1, FVC, IC, RV and TLC, and were analysed in a similar way to the primary efficacy parameter, although FEV1 and FVC were not log transformed prior to analysis.
The TDI total score, mean morning PEF and the mean number of occasions salbutamol was used as rescue medication in a 24 h period were analysed using a mixed model with treatment and period as fixed effects and subject as a random effect.
RESULTS
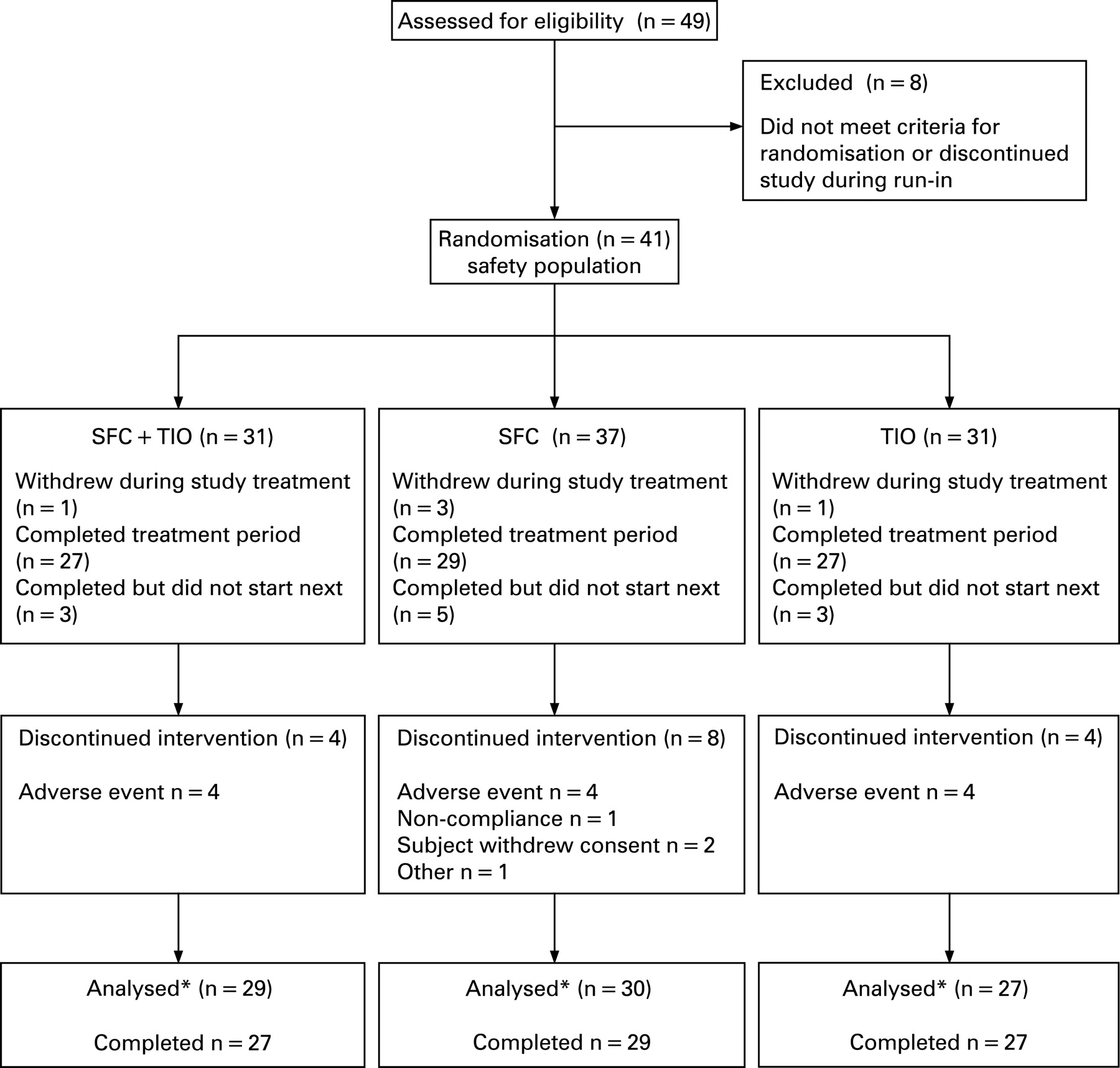
Of 49 patients screened, 41 were randomised to treatment and received at least one dose of medication. Of those randomised, 30 subjects comprised the MITT population for efficacy analysis, with a total of 25 (61%) patients completing all treatment periods. Details of patient baseline characteristics are shown in table 1 and the flow of patients through the study with reasons for discontinuation are shown in fig 1. During each treatment period, compliance with study medication was ⩾93% and similar in all treatment periods.

Day 14 pulmonary function
sGaw
Analysis of AUC(0–4 h) for sGaw after the morning dose of study medication showed that the SFC+TIO combination was significantly more effective than both TIO and SFC alone in improving sGaw (fig 2A). The ratios of SFC+TIO to the individual treatments showed that the combination produced a 22% improvement in AUC(0–4 h) sGaw over TIO alone (ratio 1.22, 97.5% CI 1.10 to 1.35; p<0.001) and a 27% improvement over SFC alone (ratio 1.27, 97.5% CI 1.14 to 1.42; p<0.001).

SFC+TIO was significantly more effective than TIO or SFC alone at improving post-dose sGaw at all time points from 30 min to 4 h. At 2 h, the ratio for SFC+TIO compared with TIO and SFC was 1.22 (97.5% CI 1.09 to 1.37; p<0.001) and 1.28 (97.5% CI 1.13 to 1.44; p<0.001), respectively. At 4 h, the ratio was 1.24 (97.5% CI 1.09 to 1.42; p<0.001) and 1.27 (97.5% CI 1.11 to 1.46; p<0.001) compared with TIO and SFC, respectively. Similarly, SFC+TIO was significantly more effective than both TIO and SFC alone in improving the trough sGaw with a ratio compared with TIO of 1.17 (97.5% CI 1.04 to 1.30; p = 0.002) and 1.18 (97.5% CI 1.05 to 1.32; p = 0.002) compared with SFC.
Spirometry
A significant improvement in FEV1 was seen during treatment with SFC+TIO compared with TIO alone at both 2 and 4 h post-dose (198 ml at 2 h, p<0.001; 251 ml at 4 h, p<0.001), and SFC alone, reaching statistical significance at 4 h (97 ml; p = 0.023) but not at 2 h (93 ml; p = 0.029) (fig 2B). There were also significant improvements in post-dose FVC for SFC+TIO compared with TIO and SFC alone (table 2). There was a statistically significant improvement in pre-dose (trough) FEV1 for SFC+TIO compared with TIO alone (212 ml; p<0.001) and SFC alone (110 ml; p = 0.017) (fig 3). There was also a significant improvement in pre-dose FVC for SFC+TIO compared with TIO but not compared with SFC alone (table 3).

{kind=link}
{kind=link}
{kind=link}
Lung volumes
There were significant improvements in post-dose IC and RV on day 14 for SFC+TIO compared with TIO and SFC alone, as shown in table 2, but not for TLC. The post-dose IC data are shown in fig 2C. There were also statistically significant improvements for SFC+TIO compared with TIO alone for pre-dose IC and RV (table 3). There was no difference in these parameters between SFC+TIO and SFC alone.
Day 1 pulmonary function
sGaw
There were improvements in sGaw on day 1 after all three treatments (fig 2A). There was no statistically significant difference between SFC+TIO and the individual components.
Spirometry and lung volumes
The improvements after SFC+TIO were not significantly different to those observed with the individual components for FEV1 (fig 2B), IC (fig 2C) and TLC (table 2). Only FVC and RV showed some evidence of a benefit in favour of SFC+TIO compared with the individual components (table 2).
Diary cards and TDI score
The daily record cards and TDI results are shown in table 4. There was a significant difference in the total TDI score between SFC+TIO and TIO at day 14 (2.2 units; p<0.001) but no difference between SFC+TIO and SFC alone (0.7 units, p = 0.24). For morning PEF, there was no statistically significant difference between SFC+TIO and either TIO alone or SFC alone. For rescue medication, the SFC+TIO group used salbutamol on 1.0 occasion less than TIO alone in a 24 h period (p<0.001) and on 0.6 of an occasion less than the SFC group (p = 0.013).
Safety
The overall incidence of adverse events was comparable between the treatment groups. Four patients on each treatment were withdrawn after randomisation due to an adverse event, two of which were due to an exacerbation of COPD, one during treatment with TIO alone and one during treatment with SFC alone. The mean blood pressure and pulse rate were comparable between the treatment groups at baseline and at the end of the study (data not shown).
DISCUSSION
Triple therapy with SFC plus TIO for 14 days improved sGaw to a significantly greater degree compared with treatment with SFC alone or TIO alone. This improvement was observed for the sGaw primary end point of AUC(0–4 h), and also for the sGaw secondary end points at pre-dose (trough) and 2 and 4 h post-dose on day 14. Pulmonary function measurements of FEV1 confirmed the superiority of triple therapy both pre- and post-dose on day 14. There was also evidence that triple therapy caused a greater reduction in hyperinflation on day 14 compared with treatment with SFC or TIO alone. The superiority of triple therapy demonstrated by this range of pulmonary function measurements translated into clinically important benefits in terms of symptom scores and rescue medication use, particularly compared with TIO used alone.
There are some published data regarding triple therapy in COPD.16 ,17 ,23 The novel findings of the current study are that triple therapy improves a range of pulmonary function measurements, including sGaw, FEV1 and IC, after 14 days therapy, but not after the first dose. These differences were observed both pre- and post-dose on day 14. This is the first properly statistically powered study to evaluate triple therapy with SFC and TIO compared with TIO alone and SFC alone, and we have unequivocally shown that triple therapy causes greater improvements in pulmonary function measurements that are clinically relevant.
The measurement of sGaw by body plethsymography is a sensitive way of measuring the effects of drugs in patients with asthma and COPD.18–21 FEV1 is the most commonly used pulmonary function measurement in COPD clinical trials, as it is required by regulatory authorities and is a simple and reproducible technique to perform. However, even when taking the increased variability of sGaw into account, sGaw is still a more sensitive method of detecting changes in lung function than FEV1 in patients with COPD.18 ,20 ,21 Increased airway conductance, assessed by sGaw, is associated with improved expiratory airflow, assessed by FEV1, in patients with COPD.18 ,20 However, FEV1 can be relatively insensitive to treatment effects in patients with COPD, so large sample sizes are often needed to compare treatments based on FEV1. In contrast, sGaw measurements more readily change with improvements in airway function, so studies can be designed using smaller sample sizes based on this measurement.18 ,20 Body plethysmography also has a practical advantage as it uses tidal breathing, thus avoiding the possibility of bronchoconstriction during forced expiration in patients with airflow obstruction.24
sGaw is not routinely used in clinical trials as it requires a greater degree of operator training, and is more expensive and time consuming. We chose to use this sensitive method as the primary end point in order to maximise the power of the study to detect a difference between treatments with lower patient numbers. sGaw has not been widely used in COPD trials, and therefore it is also important to evaluate more traditional pulmonary function parameters, so we also performed measurements of FEV1 and lung volumes. Our study design therefore allowed a comprehensive assessment of airway conductance, airflow and lung volumes.
On day 14, both sGaw and FEV1 data showed that triple therapy was superior to SFC alone or TIO alone. This superiority was observed both pre-dose and in the 4 h post-dose. These pre-dose measurements are indicative of the cumulative effects of 13 days of treatment, rather than the acute effects of treatment. We can infer that the superiority of triple therapy over the other treatments after multiple dosing was present throughout the 24 h period post-dose, and not just immediately post-dose. The day 14 pre-dose FEV1 data allow the magnitude of this effect to be fully appreciated; triple therapy had a superiority of 212 ml over TIO and 110 ml over SFC. The accompanying changes in TDI scores and rescue medication use demonstrate that these differences are also clinically relevant.
IC is a widely used measurement of pulmonary hyperinflation that can be related to the degree of breathlessness that patients suffer.25 Our findings on day 14 post-dose demonstrate a greater increase in IC with triple therapy compared with the other treatments. SFC therapy alone26 and TIO alone27 are known to increase IC, and hence reduce hyperinflation, leading to improvements in exercise capacity. We have shown that greater increases in IC can be achieved when both of these inhalers are used together, compared with the individual treatments, and accordingly would expect this to translate into further improvements in exercise capacity. This warrants further study.
At pre-dose on day 14, the effects of triple therapy on IC and RV were significantly greater than TIO, but not compared with SFC. Interestingly, data also showed that triple therapy was superior to treatment with TIO alone for TDI score, but not compared with SFC. The current study was not statistically powered to evaluate TDI scores, but our findings are suggestive that changes in TDI scores were determined by the degree of hyperinflation throughout the 24 h period, rather than just in the 4 h after dosing. In this respect, triple therapy may not have any advantage over treatment with SFC alone.
Our study was focused on day 14 to compare the effects of the different treatments after multiple dosing. We also measured pulmonary function after the first dose, and found no advantage of triple therapy compared with the other treatments for the key measurements of sGaw, FEV1 and IC. There was some evidence of triple therapy superiority for FVC, but overall the pulmonary function data indicated no difference. The major advantages of triple therapy compared with TIO alone or SFC alone appears therefore to be a cumulative effect resulting from repeat dosing and can already be observed after 2 weeks of therapy.
We did not recruit patients based on specific reversibility criteria. Accordingly, our results are probably applicable to patients with COPD generally, and not confined to a subgroup with specific characteristics. Our study should encourage further research to evaluate the potential of triple therapy on clinically relevant end points. Aaron et al showed that SFC (50/500 μg twice daily) plus TIO (18 μg once daily) was superior to TIO alone in terms of pulmonary function and symptoms over 1 year, and results for TIO plus salmeterol (50 μg twice daily) were similar to TIO alone.16 The primary end point of this study was exacerbations, but the number of subjects was too small to provide adequate statistical power for the observed treatment difference. The pulmonary function findings of the superiority of triple therapy compared with TIO alone agree with the findings of the current study. Cazzola et al evaluated the same three treatment arms as the current study, but in a parallel group design based on the primary end point of FEV1, and reported data that agrees with the current study at 3 months, but not at earlier time points.17 Villar and Pombo reported a crossover study in patients on continual treatment with inhaled FP (500 μg/12 h), comparing 1 week of therapy with FP plus salmeterol (50 μg/12 h) versus FP plus TIO (18 μg/24 h) versus FP plus TIO plus salmeterol.23 There was a triple therapy arm (concurrent therapy with free combination FP plus TIO plus salmeterol), but it is important to note that the combination inhaler SFC was not used. Triple therapy was found to have the greatest effect on FEV1. Comparison of triple therapy with FP plus salmeterol agrees with the current study findings. However, we used the SFC combination inhaler which has been shown to have superior effects on pulmonary function compared with the individual inhalers in asthma.28 Nevertheless, these previous publications in conjunction with the current study provide a strong case that triple therapy is the best way of optimising pulmonary function in patients with COPD of an appropriate severity.
Triple therapy is widely used in clinical practice for patients with COPD to optimise lung function, improve symptoms and reduce exacerbations. However, the evidence base for this approach is limited. The current study provides an important addition to our knowledge, proving that triple therapy with SFC plus TIO is more effective than SFC alone or TIO alone in terms of pulmonary function. Adequately powered, long term studies of the benefits of triple therapy on exacerbation rates and other clinical end points are now needed to fully justify this approach in clinical practice.
Acknowledgments
This study was funded by GlaxoSmithKline. The authors would like to thank the investigators, S D Singh (Manchester), B O'Connor (London), R Djukanovic (Southampton), W Wedzicha (London), G Joos (Gent, Belgium), who participated in the study and Diana Jones, a medical writer, who provided medical writing support sponsored by GSK.
REFERENCES
Footnotes
Funding: The study was funded by an unrestricted research grant from GlaxoSmithKline.
Competing interests: None.
Ethics approval: The study protocol was approved by the appropriate institutional review boards and conducted in accordance with good clinical practice guidelines and the 1996 version of the Declaration of Helsinki (study No SCO104962).
Note from Editor-in-Chief: J A Wedzicha recruited patients to this study but was not involved in data analysis or preparation of the manuscript and was not the handling editor of this paper.