Article Text

Statistics from Altmetric.com
A 26-year-old female presented with progressive cough and breathlessness for 4 months. At her initial visit she was 6 weeks’ pregnant and reported that she could only climb 10 steps before becoming short of breath. Her past medical history was significant for a miscarriage the previous year, and her only medication was a prenatal vitamin. She was a registered nurse and had no history of smoking or drug use.
Physical examination was unremarkable. A chest x ray revealed a right perihilar mass and the CT scan (fig 1) demonstrated a well defined, slightly ovoid and homogenous cystic mass in the mediastinum measuring a maximum of 5.7×8.1 cm, with up to 75% luminal narrowing of the right pulmonary artery.

In view of her pregnancy and previous miscarriage, she was considered high risk for an open operative procedure, and the decision was made to attempt diagnosis and drainage using a minimally invasive technique.
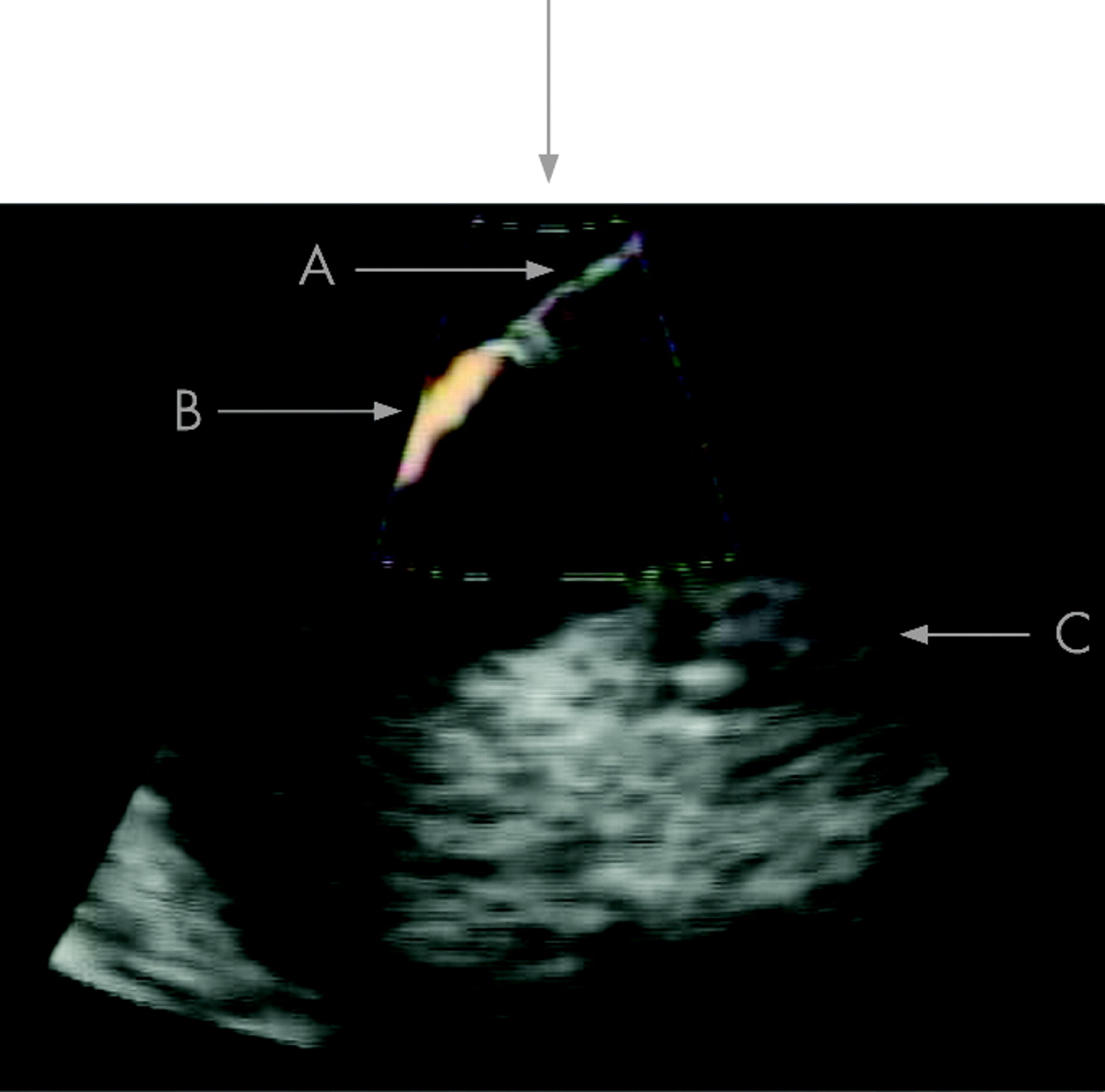
She continued to be monitored until she was 12 weeks’ pregnant and then underwent bronchoscopy with endobronchial ultrasound guided needle aspiration and drainage of the mass. Layering was noted on ultrasound of the structure, suggesting a debris filled cyst. Aspiration was accomplished at the level of the carina at the take off of the left main stem bronchus (fig 2). A total of 20 ml of mucoid fluid were aspirated. The airways were then suctioned to remove additional debris, and bronchoplasty was used to increase luminal airway diameter. Additional secretions were removed by further suctioning.

{kind=link}
{kind=link}
Cultures and cytology from the aspirated fluid were negative for any bacterial growth or malignancy, showing only bronchial epithelial cells. Six weeks later the patient was followed-up in clinic and was feeling well with complete resolution of the shortness of breath and cough.
Bronchogenic cysts are the most common benign mediastinal cyst in adults, and frequently present incidentally on chest x ray.1 Transbronchial needle aspiration is a sensitive and highly specific technique that has a major role in the diagnosis of mediastinal lesions.2 The technique can also be extended to provide treatment for patients unsuitable to undergo an open surgical procedure.
Learning points
Pulmonary artery compression by a bronchogenic cyst can cause severe symptomatic dyspnoea
Endobronchial ultrasound guided fine needle aspiration can be used to treat large bronchogenic cysts
The technique is especially useful in patients in whom an open surgical procedure is undesirable
Footnotes
Competing interests: None.