Article Text

Statistics from Altmetric.com
CLINICAL PRESENTATION
A 75-year-old man was admitted with a non-productive cough and chest discomfort. He had been admitted 2 months previously with left lower lobe (LLL) consolidation for which he received intravenous antibiotics. He had no weight loss or constitutional symptoms. The chest radiograph (fig 1) revealed persistent consolidation and he was urgently referred to the chest clinic for review.

He was an ex-smoker with a 50 pack-year history. 12 years previously he was diagnosed with carcinoma of the piriform fossa which was successfully treated with pharyngolaryngectomy, radical radiotherapy and subsequent tracheostomy. Examination revealed evidence of his previous surgery and a tracheostomy. He had no clubbing or lymphadenopathy and coarse crackles were heard at the left base, as on the previous admission. After treatment with co-trimoxazole for 3 weeks his chest radiograph remained unchanged. A CT scan of the thorax (fig 2) revealed LLL collapse with dense consolidation in the posterior aspect of the right middle and lower lobes. The possibility of aspiration was suggested. Bronchoscopy was performed via his tracheostomy which showed a normal right bronchial tree and only a moderate amount of thick white sputum on the left which was easily cleared by washing. Washings were negative for cytology, culture and acid-fast bacilli.

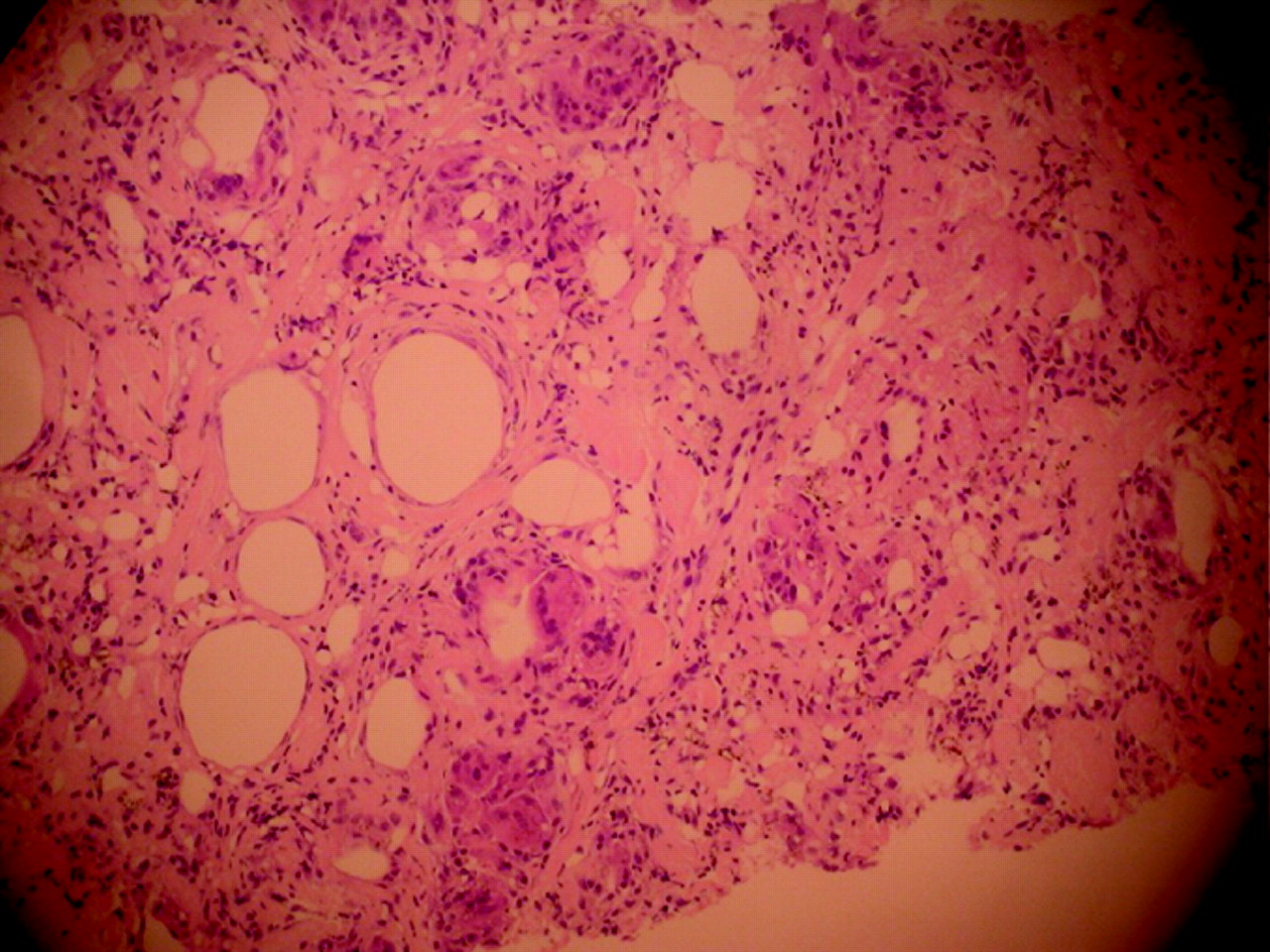
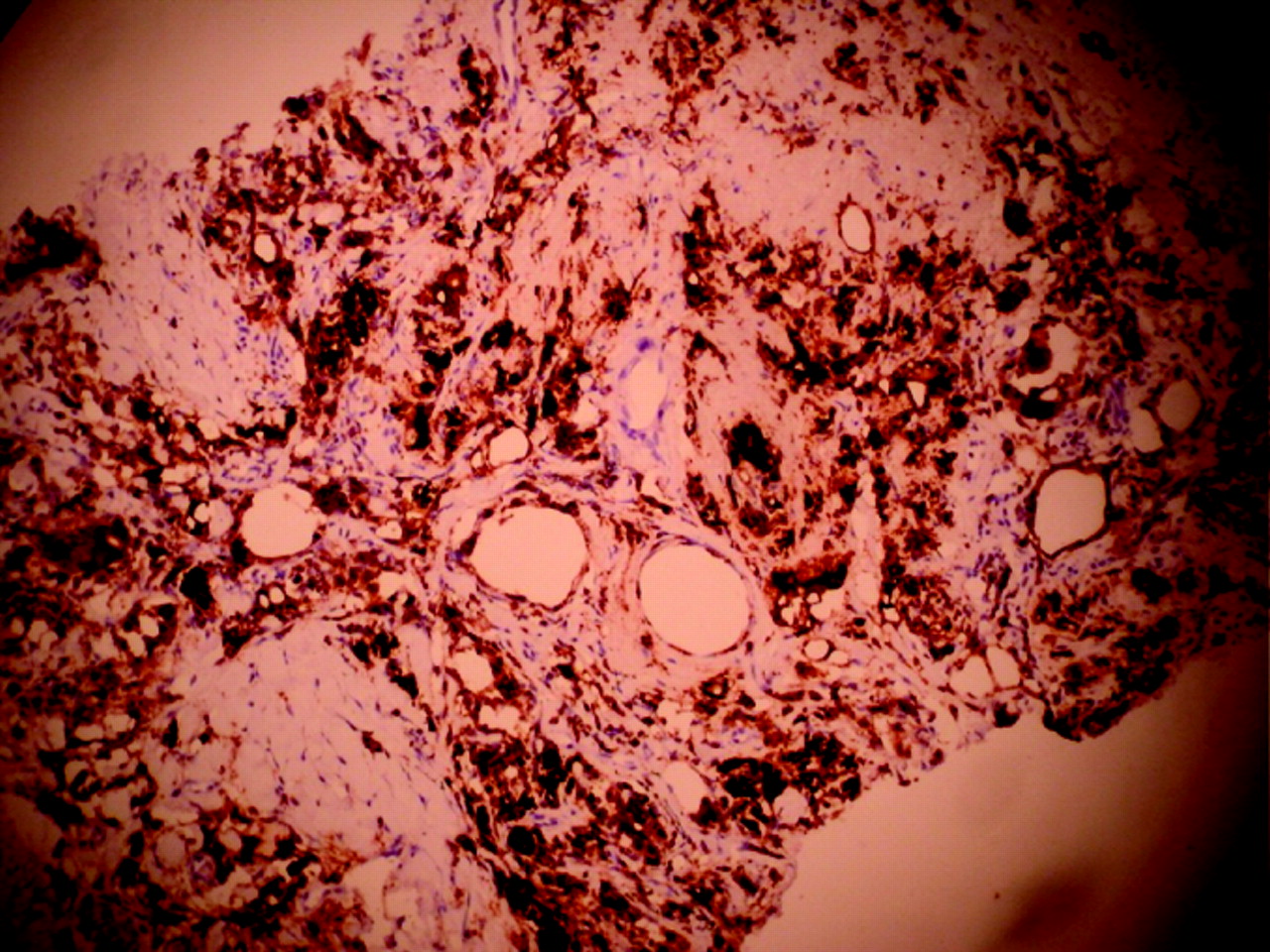
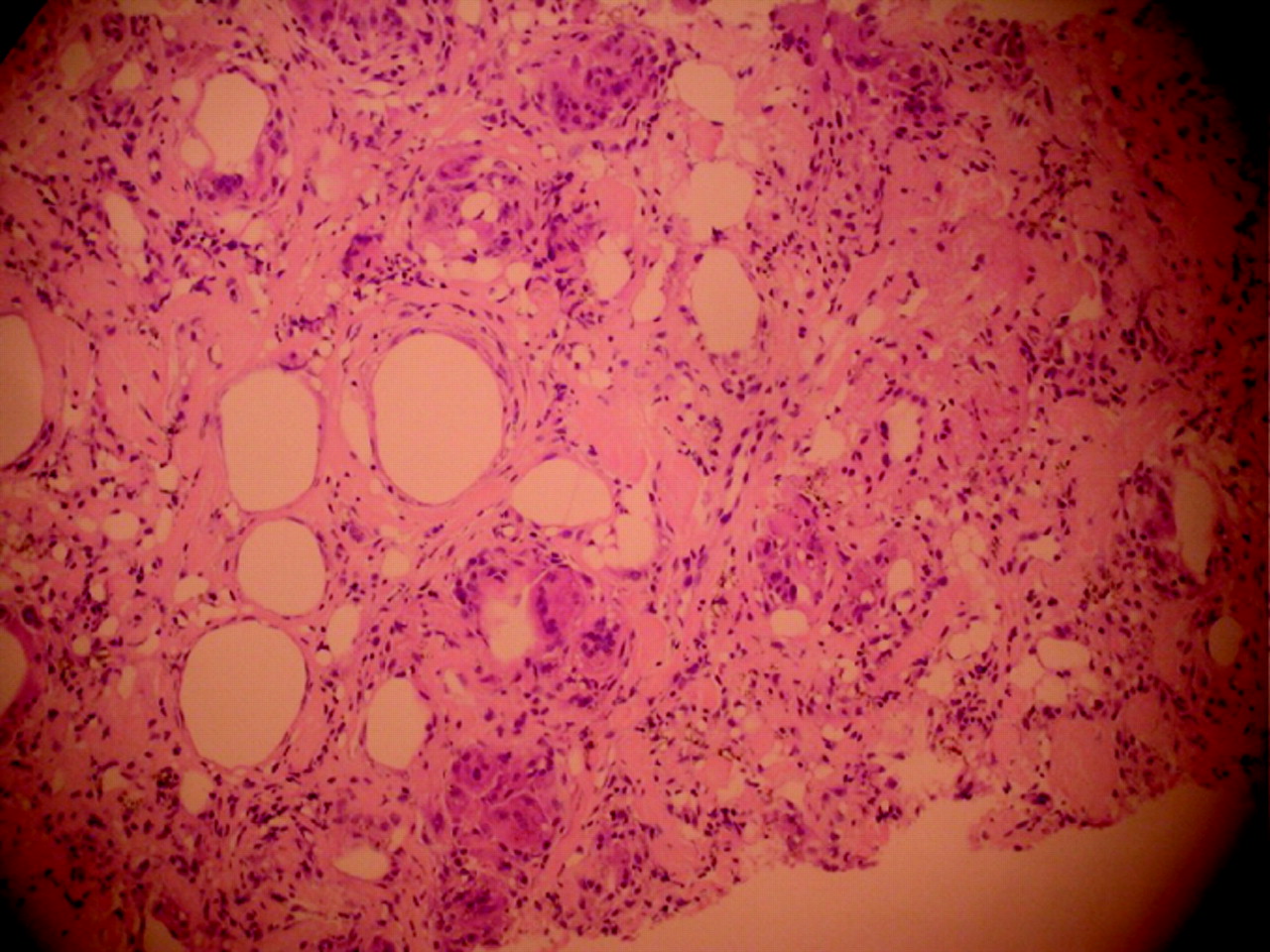
CT-guided biopsy (fig 3) showed fibrosis, elastosis and numerous macrophages (CD68 positive, fig 4) with several multinucleated giant cells surrounding spaces, presumed to contain fat. Black carbon pigment was seen in the interstitium and within macrophages. Occasional associated needle-shaped refractile crystals were present and a chronic inflammatory cell infiltrate of lymphocytes. There was no evidence of malignancy.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
QUESTION
Is there anything further you would like to ask in the history and can you suggest a possible diagnosis?
See page 376 for answer
This case was submitted by:
Footnotes
Competing interests: None.
Linked Articles
- Pulmonary puzzle