Article Text

Abstract
Background: Chronic obstructive pulmonary disease (COPD) is an insidiously starting disease. Early detection has high priority because of the possibility of early implementation of smoking cessation interventions. An evidence based model for case finding of COPD is not yet available.
Objective: To describe the early development of COPD, and to assess the predictive value of early signs (respiratory symptoms, lung function below the normal range, reversibility).
Design and methods: In a prospective study, based in general practice, formerly undiagnosed subjects (n = 464) were assessed at baseline and at 5 years for respiratory symptoms and pulmonary function. Odds ratios for early signs were calculated (adjusted for age, gender, pack-years at baseline and smoking behaviour during follow-up), and defined as possible indicators of disease progression.
Results: Over a 5 year period, the percentage of subjects with obstruction increased from 7.5% (n = 35) at baseline to 24.8% (n = 115) at 5 years. The presence of mild early signs and lung function below the normal range at baseline were related to an increased risk of developing mild to moderate COPD (GOLD I: OR 1.87 (95% CI 1.22 to 2.87); GOLD II: OR 2.08 (95% CI 1.29 to 3.37) to 2.54 (95% CI 1.25 to 5.19)) at 5 years.
Conclusion: Lung function below the normal range and early respiratory signs predict the development and progression of COPD.
Statistics from Altmetric.com
In the past decades, an increase in the prevalence of chronic obstructive pulmonary disease (COPD) and asthma has been observed.1 2 As a result of demographic changes, the global burden of COPD is expected to shift from the sixth leading cause of death in 1990 to third position by 2020.3 This evolution is a significant challenge for primary care, as the prevalence of COPD is expected to nearly double over the period 1994–2015.4 5
Although it is generally recognised that patients with COPD should be identified before the disease becomes substantial, early stage COPD often remains undiagnosed6 or misdiagnosed.7 To decrease morbidity and mortality from this chronic lung disorder, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) programme was initiated.8 In a number of cross sectional, population based surveys,9–11 the GOLD guidelines were used to estimate the prevalence of COPD. One of the first surveys, the confronting COPD International Survey,12 confirmed the huge burden to society and, furthermore, identified a significant disparity between subjects’ perception of disease severity and the assessed degree of severity.
The hallmark of COPD is the presence of airway obstruction. Recently, the prevalence of undiagnosed airflow obstruction was estimated by reviewing data from 13 (mainly cross sectionally designed) studies.13 Prevalence ranged from 3% to 12%. Furthermore, the GOLD guidelines define a very early stage of COPD, in which subjects are considered to be “at risk” for COPD.14 This so-called GOLD stage 0 is defined by chronic respiratory symptoms without measurable obstruction. Meanwhile, prospective long term and population based studies, focusing on early stage COPD in relation to respiratory disease years later, are scarce.10 15 In one study,10 the Copenhagen City Heart Study, the authors concluded that GOLD stage 0 was not prognostic for the development of COPD. In the Obstructive Lung Disease in Northern Sweden study,15 subjects with respiratory symptoms at study entry showed an increased risk of developing COPD. As this ambiguity warrants further research, the objective of the current study was to investigate the value of early respiratory symptoms and lung function below the normal range as indicators for progression of COPD.
METHODS
Design
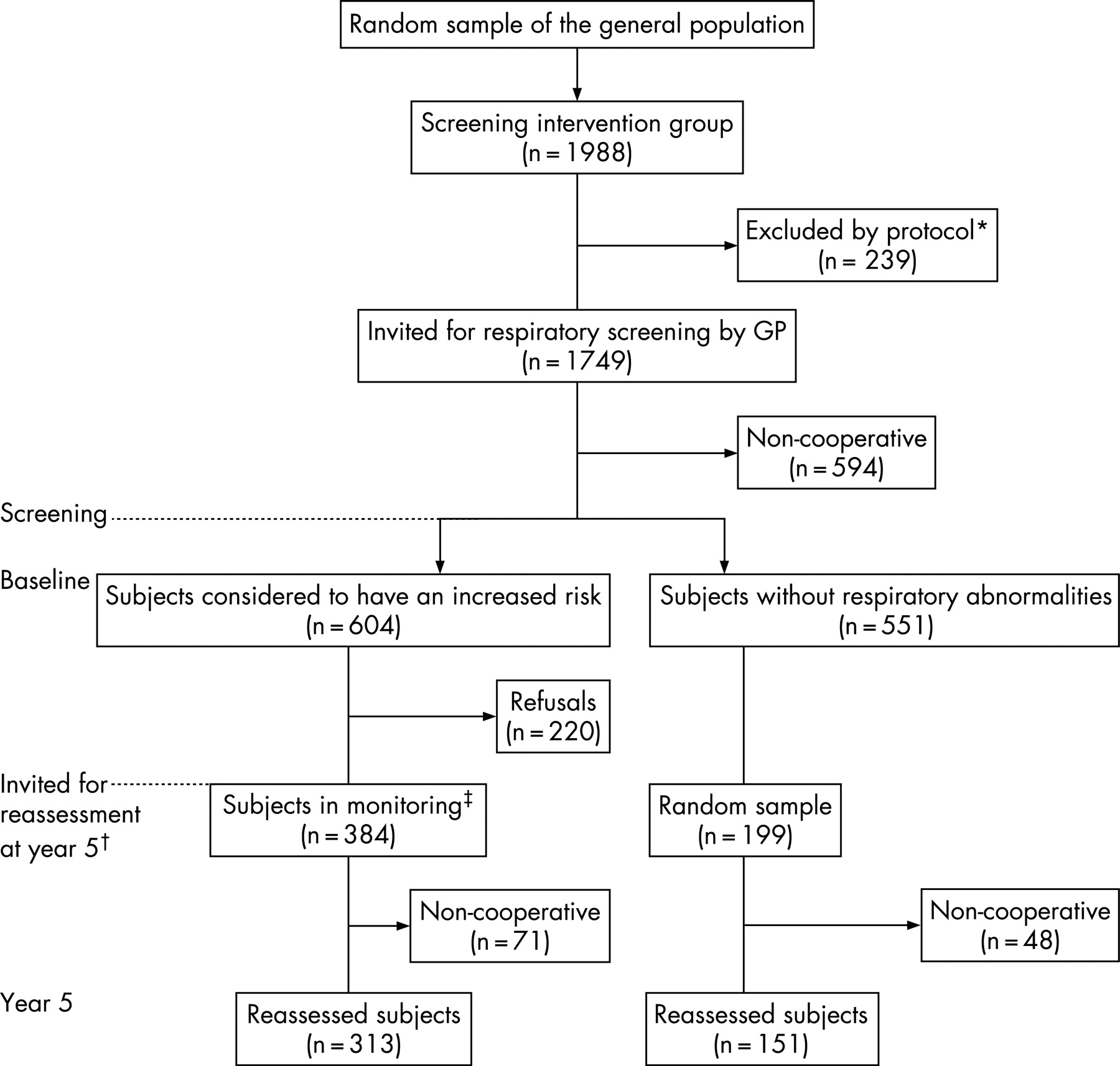
The Detection, Intervention and Monitoring of COPD and Asthma in general practice (DIMCA study) is a prospective cohort study, designed to assess the feasibility of active detection of early stage chronic respiratory disease (COPD, asthma) in the Dutch general population16 (fig 1). The initial cohort can be regarded as a random sample from the Dutch general population. Adult subjects (20–70 years) without a medical history of COPD, asthma or other chronic respiratory disease were included. All subjects took part in a screening programme for COPD or asthma at the earliest possible stage of disease. The assessment consisted of a respiratory symptoms questionnaire and lung function measurement. The criteria in the original screening programme, further referred to as early signs of respiratory morbidity,i were used to define the baseline respiratory status of screened subjects. Subjects with either respiratory symptoms, lung function below the normal range17 or a response on salbutamol (reversibility) at baseline were considered to have an increased risk of developing respiratory morbidity. Otherwise, subjects were labelled as having no abnormalities. Subsequently, at risk subjects were invited to participate in a 2 year monitoring programme. After monitoring, those showing persistent signs and symptoms (of varying severity) were invited for an intervention study with inhaled corticosteroids in a series of three randomised controlled trials. The results of the trials are described elsewhere.18–20
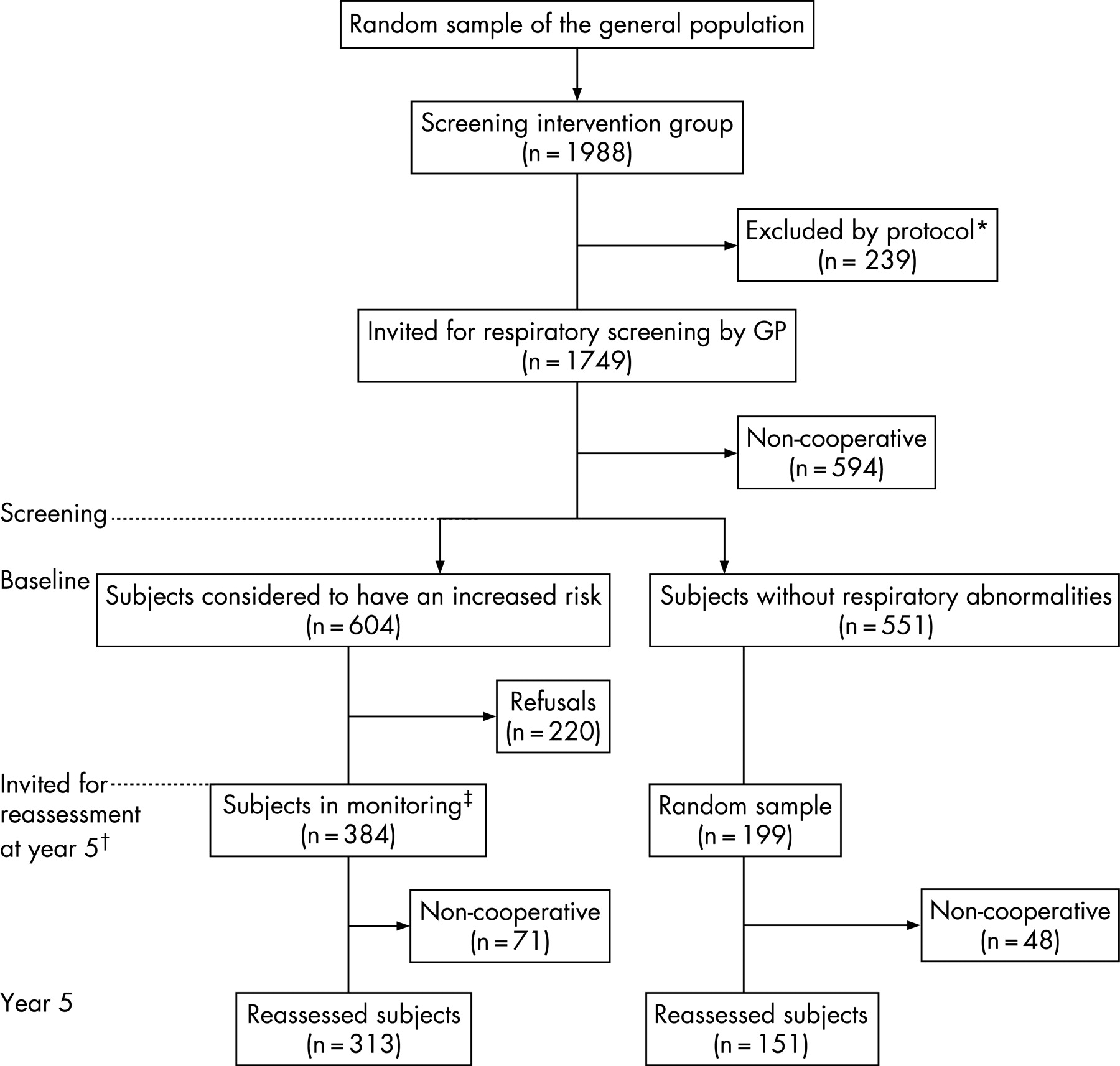
For the present study, subjects were reassessed after 5 years with regard to their respiratory symptoms and lung function. Invited were the following: all subjects with an increased risk of developing respiratory morbidity who participated in monitoring (n = 384) and a random sample of subjects with no baseline abnormalities (n = 199) (fig 1).
The course of respiratory morbidity was operationalised by the change in lung function, reversibility, respiratory symptoms and self-reported smoking behaviour over the 5 year period. Subjects were classified by COPD stages, as the recently developed GOLD guidelines21 facilitate such classification. To study whether early signs and symptoms of respiratory morbidity precede development of actual disease, an algorithm based on the GOLD criteria (table 1) was used to allocate subjects to one of the following categories: asthmatic, at risk for COPD (GOLD 0), mild COPD (GOLD I), moderate COPD (GOLD II), severe COPD (GOLD III) or no COPD or asthma.
The medical ethics review board of the University Medical Centre Nijmegen approved the study. Subjects gave their written informed consent.
Measurements
Lung function and reversibility
Lung function was assessed by two trained lung function technicians at two different points in time (at baseline and at 5 years). Measurements were performed according to the American Thoracic Society standards.22 ECCS reference values were used.23 Variation in spirometer performance was assessed and accounted for. Reversibility24 was assessed 15 min after inhalation of 800 μg of salbutamol by spacer. At the moment of screening, lung function below the normal range17 was defined as bronchodilator forced expiratory volume in 1 s/vital capacity (FEV1/VC) less than or equal to the lower limit of normal (predicted minus 1.64 SD). Reversibility was defined as positive if after bronchodilatation the change in FEV1 (relative to the predicted value) was at least 15%.24 In the GOLD based disease classification,21 definitions were for obstruction, a post-bronchodilator FEV1/VC <70%, and for reversibility, a 12% change in predicted FEV1 after bronchodilatation with a change of at least 200 ml.
Respiratory symptoms and smoking behaviour
The occurrence of respiratory symptoms was measured at baseline and at 5 years with the Dutch modified version of the Medical Research Council questionnaire.25 Chronicity of respiratory symptoms was defined by occurrence of symptoms for more than 3 months per year. Mucus hypersecretion was defined as continuous production of sputum in the winter season. Furthermore, subjects were asked whether they were current smokers, ex-smokers or never smokers.
Statistical analysis
To describe the course of respiratory morbidity, the mean individual change over the 5 year follow-up period in lung function was compared for the group of subjects with no abnormalities versus the group of at risk subjects. The appropriate univariate statistical tests were used.
Progression of COPD was studied using multinomial logistic modelling. The dependent variable was respiratory morbidity at 5 years. This outcome was defined by the three categories of absence of COPD or asthma, mild COPD or moderate to severe COPD. Initially obstructed subjects were excluded from the analysis. Odds ratios (OR) of early signs of respiratory morbidity were calculated and defined as possible indicators of disease progression. Because of gained insight, mucus hypersecretion was added to the signs initially defined at the screening. ORs were based on adjustment for age, gender, number of pack-years at baseline and smoking behaviour during the 5 year follow-up period. Following disease classification at 5 years (table 1), categories were compared on lung function and obstruction over the 5 years using confidence limits. The SAS statistical package (V8.2 for Windows) was used for all analyses. Two sided p values of <0.05 were considered to be statistically significant.
RESULTS
The flow of the DIMCA cohort (fig 1; n = 1749) showed different rates of non-participation. Over the 5 year period, 10 subjects were lost to follow-up because of death (none was COPD related). Between the initial (screened) sample and the (on GOLD stage) classified sample at 5 years there were no signs of selection (dropoutii, trial participants,iii). A total of 583 subjects were invited for reassessment at 5 years. In the group without respiratory abnormalities (n = 199), the response was 76%; in the at risk group (n = 384), the response was 82%.
Symptoms and lung function in screened subjects
The characteristics of the study population, and their evolution over the 5 year period, are given in table 2. At baseline, there was no difference in age, gender, height or smoking history between subjects without respiratory abnormalities and at risk subjects. Both at baseline and at the reassessment after 5 years, at risk subjects had more symptoms (p = 0.001), lower post-bronchodilator FEV1 (p = 0.0001) and lower post-bronchodilator FEV1/VC (p = 0.0003 and p<0.0001, respectively), and were more often current smokers (p = 0.07 and p = 0.04, respectively) than subjects without baseline abnormalities. Over the 5 year period, the overall individual change (n = 464) showed a decrease in post-bronchodilator FEV1 (−241 (SD 303) ml; on average, −48 ml/year) and in post-bronchodilator FEV1/VC (7.1% (SD 9.9%)). At risk subjects demonstrated more reduction in lung function (post-bronchodilator FEV1 −262 ml vs −199 ml; p = 0.02) and a lower average post-bronchodilator FEV1/VC (−8.0 vs −5.2; p = 0.04).
Respiratory morbidity
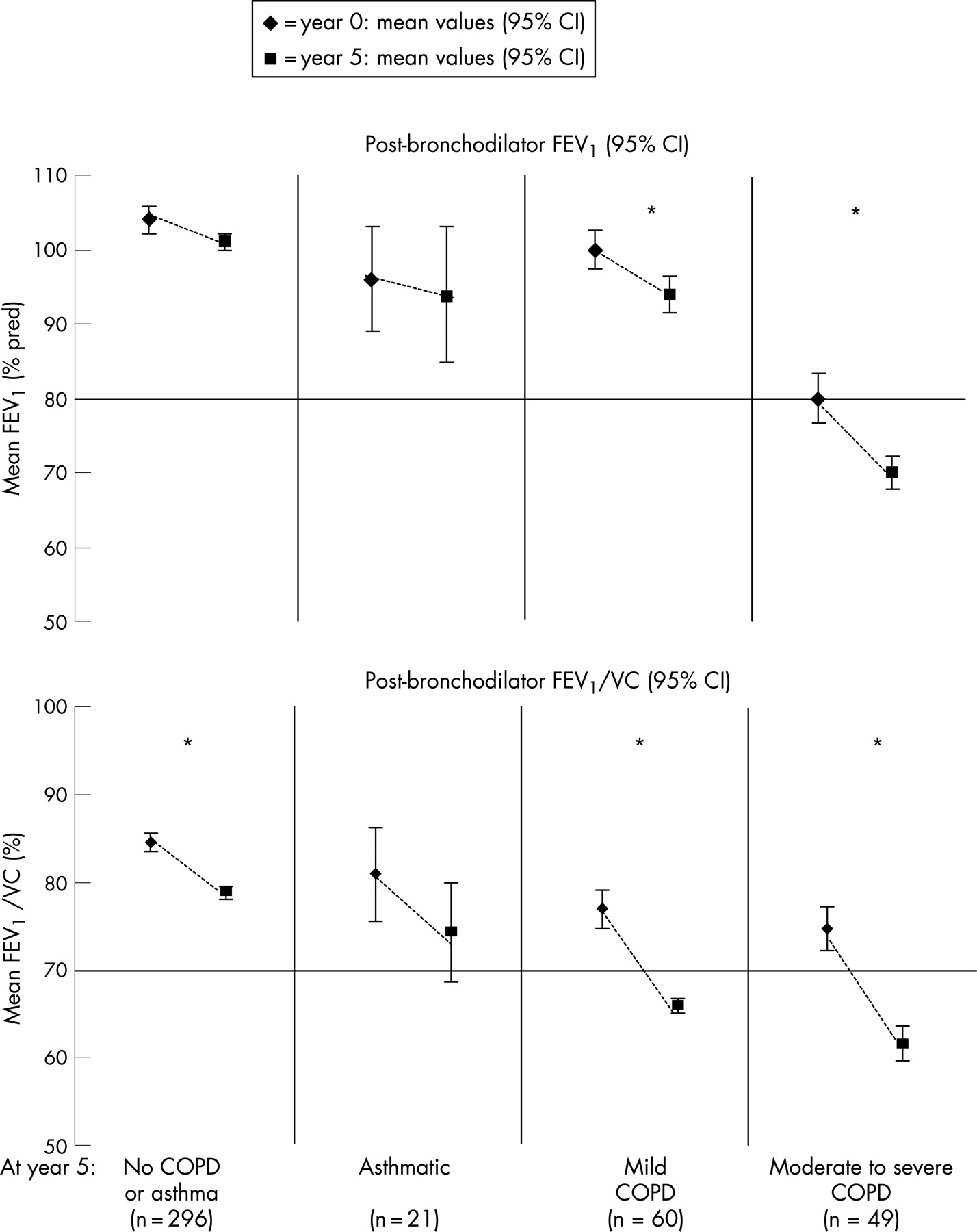
The distribution of respiratory morbidity at 5 years is presented in table 3. Over the 5 year period, the percentage of subjects with obstruction increased from 7.5% (n = 35) at baseline to 24.8% (n = 115) at 5 years. The change in lung function (post-bronchodilator FEV1) and obstruction over the 5 year period is presented in fig 2. The group of subjects labelled at 5 years as not having COPD or asthma (n = 296) did not show a decline in lung function. There was a slight but significant decrease in post-bronchodilator FEV1/VC, but subjects did not become obstructive. Asthmatic subjects at 5 years (n = 21) showed no decrease in lung function or post-bronchodilator FEV1/VC. Over the 5 year period, subjects with mild COPD (n = 60) or moderate to severe COPD (n = 49) had significantly decreased lung function and also became obstructive.
{kind=link}
{kind=link}
Respiratory morbidity odds ratios
Assessment of respiratory morbidity at 5 years included 464 subjects (table 3). The multinomial logistic regression analysis focused on subjects without COPD or asthma (n = 287), mild COPD subjects (n = 48) and moderate to severe COPD subjects (n = 39). Subjects with obstruction at baseline (n = 35) were excluded from the analysis. ORs for early signs of respiratory morbidity were adjusted for age, gender, number of pack-years at baseline and smoking behaviour (table 4). Results showed that subjects with a baseline presence of mild obstruction or reversibility, or a weather dependent cough or shortness of breath, or a recurrent productive coughi had an increased risk of developing mild COPD (OR 1.87) or moderate COPD (OR 2.08). The presence of lung function below the normal range and mucus hypersecretion at baseline appeared to be predictive of the development of moderate COPD (OR 2.54 and OR 1.88, respectively). Female gender was significantly underrepresented in mild COPD (OR 0.54) whereas older age (OR 1.06) and an increased smoking history contributed to the risk of development of moderate COPD (OR 1.06 and OR 1.05, respectively).
DISCUSSION
The main objective of the current study was to investigate the value of early respiratory symptoms and lung function below the normal range as indicators of progression of COPD. During the study period, we observed a substantial increase in morbidity in subjects who at baseline were considered to have an increased risk for development of chronic obstructive airway disease. The most prominent predictors for developing COPD were lung function below the normal range and mild early signs of reversibility, weather dependent cough or shortness of breath or recurrent productive cough.i
COPD appears to be an insidious disease at the start. Because of subjects’ lack of perception of disease severity,12 there is enormous under-presentation of early signs of respiratory morbidity26 causing underdiagnosis of COPD in general practice. As smoking cessation can reduce symptoms and prevent progression of disease,27 early detection is important. Additional reasons to promote early detection is that treatment of COPD can improve lung function and quality of life in many patients, can reduce admissions to hospital and may even improve survival.27 Spirometry is considered the “gold standard” for detecting obstruction, and also provides prognostic information.11 28. As yet, mass screening for obstruction is not considered feasible in general practice13 and until now there has been no long term evidence on its effectiveness. Several studies focused on screening of high risk groups,29 30 but this will only detect part of the population with obstruction.31 For reasons of feasibility and cost effectiveness, it is generally agreed that case finding is the most appropriate tool in reducing underdiagnosis of COPD in general practice. As a first step in the development of an evidence based model for case finding, risk factors for the detection of early COPD need to be identified. Development of COPD was investigated in several studies,32–36 in which a great variety of risk factors (such as middle age, current or past smoking status, a self reported history or a general physician’s diagnosis of chronic obstructive airway disease, laryngeal height, bronchial hyperresponsiveness, respiratory symptoms, body mass index, accelerated decline in lung function, exercise capacity, occupational exposure, air pollution, asthma, genetic variation and functional status) were used.
In the present study, in a population based sample with initially undiagnosed subjects from general practice, we used prospective data to describe early development of COPD, and to identify risk factors. We used an algorithm, based on the recently developed GOLD guidelines, to relate disease severity at 5 years to the baseline presence of early signs. However, there are several points to raise. Firstly, in the study design, the early signs were fixed by the screening criteria defined at baseline. Because of gained insight, mucus hypersecretion (prominent in former GOLD stage 0) was added to this selection of early signs. Secondly, subjects were classified on the basis of a cross sectional measurement at 5 years. Although a well defined algorithm was used, classification was only based on post-bronchodilator FEV1, VC, reversibility and respiratory symptoms. In daily practice, however, often additional clinical assessment will be needed to arrive at an undisputed diagnosis, with a reliable disease staging. On the other hand, in the present study, reversibility data were used to distinguish between COPD and asthma. Development of COPD was further confirmed by progressive lung function decline and development of obstruction (fig 2). In their study of the population impact of different definitions of airway obstruction, Celli and colleagues11 stated that the rates according to the GOLD guidelines were found to produce lower estimates than other spirometry based definitions. This may be explained by the fact that in that study, spirometry was performed only pre-bronchodilator.37 Celli et al did not have disposition of reversibility testing, making it impossible to distinguish reversible from irreversible obstruction.11 In a recent editorial,38 Vestbo indicated that GOLD has not attempted to separate 0 COPD from symptomatic asthma. With the algorithm used, including an effort to minimise mislabelling of asthmatic subjects, we used a prudent estimate of prevailing disease at 5 years. Thirdly, as in regression analysis, adjustment was restricted to a limited set of risk factors (age, gender, pack-years at baseline and smoking behaviour during follow-up) and not all confounding factors may have been excluded. A further finding concerned the steady (or slightly decreased) percentage of subjects with respiratory signs and symptoms in the at risk group. The most obvious explanation might be that after assessment of symptoms, the problem is identified and subjects will deal with it.
Over the 5 year period, the number of subjects with obstruction increased considerably. In other terms, screened subjects, considered to have an increased risk for development of COPD, appeared to have a more than threefold risk of actually developing mild or moderate COPD. The most prominent predictor for development of moderate COPD was a baseline presence of lung function below the normal range (OR 2.54). In this cohort of initially undiagnosed subjects, a baseline presence of mild obstruction or reversibility, or a weather dependent cough or shortness of breath, or a recurrent productive cough were predictive for the development of mild COPD (OR 1.87) or moderate COPD (OR 2.08) 5 years later. Furthermore, baseline mucus hypersecretion (in the absence of airflow obstruction without full reversibility) appeared to be predictive (OR 1.88) for subsequent development of moderate COPD. A prolonged follow-up from early stage COPD onwards, followed by an undisputed clinical diagnosis, may further clarify these relations. In terms of healthcare, identification of risk factors for early detection of COPD may contribute to the development of an evidence based model for case finding. This is specifically of interest for the studied cohort, as these undiagnosed subjects did not present themselves in primary care.
In conclusion, lung function below the normal range and early respiratory signs are possible predictors of progression of COPD. As a result, implementation of GOLD guidelines in general practice may reduce underdiagnosis and under treatment.
Acknowledgments
The authors thank Guido van den Boom. His former support and contribution were critical to the present article. The authors also wish to thank Lea Peters and Joke Grootens for their support in data collection, logistics and generating graphs.
Appendix
Appendix 1
Table A1 shows the screening criteria used to determine respiratory status of subjects and table A2 shows the baseline values of the respective follow-up groups
Appendix 2
A total number of 145 at risk subjects participated in one of the randomised controlled trials (for a period varying between 12 and 30 months), in which inhaled corticosteroids (n = 68) were compared with placebo treatment (n = 77). The mean individual change in post-bronchodilator FEV1 over the 5 year period was −352 ml (SD 287) in the corticosteroid treated group versus −280 ml (SD 307) in the placebo treated group. Based on the individual change over the 5 year period, corticosteroid treatment did not show a different course in respiratory symptoms, post-bronchodilator FEV1 (p = 0.09) or post-bronchodilator FEV1/VC (p = 0.96) from placebo treatment. As a consequence, participants in the intervention study were included in the sample.