Article Text

Statistics from Altmetric.com
CLINICAL PRESENTATION
A 50-year-old man presented to our hospital with left chest discomfort. There was no cough, dyspnoea or constitutional symptoms. The family history and past medical history were unremarkable except for vertical hepatitis B infection at birth, with a current status of positive hepatitis B surface antibody and negative hepatitis B surface antigen.
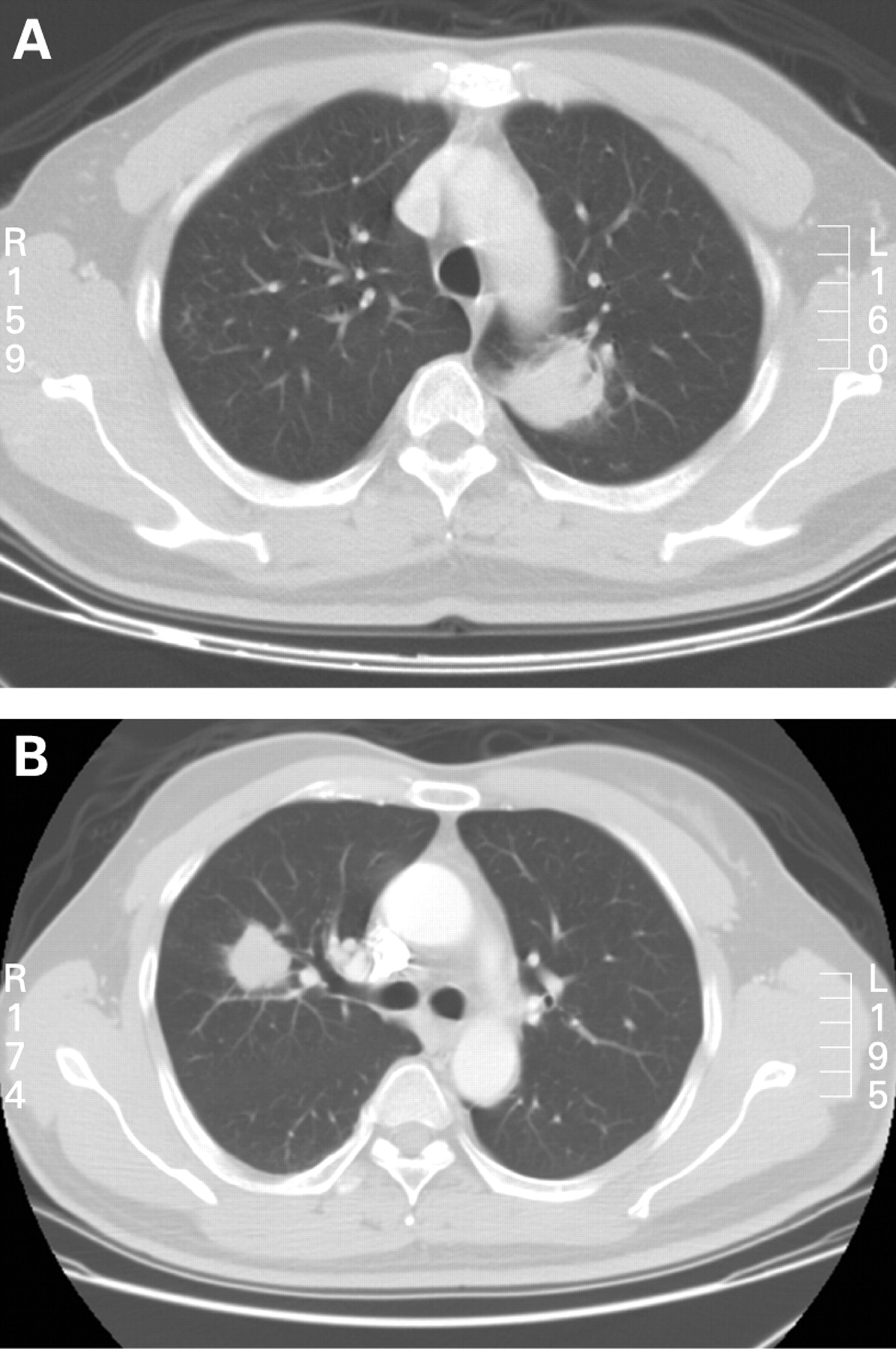
On admission the physical examinations were unremarkable. Chest radiography showed two distinct patches over the bilateral upper lung fields. A chest CT scan disclosed a 4×3 cm lobulated mass at the left upper lobe (fig 1A) and a 1.5×1.5 cm peribronchial nodule at the right upper lobe without mediastinal or hilar lymphadenopathy. The haemogram and blood biochemistry results were within normal limits except for an elevated lactate dehydrogenase level of 568 U/l (normal range 230–460 U/l).

A CT-guided biopsy of the left lung mass was performed which revealed a low-grade B cell mucosa-associated lymphoid tissue lymphoma (MALToma; fig 2A, B). Staging investigation disclosed primary pulmonary MALToma with only lung involvement. Chemotherapy with cyclophosphamide, doxorubicin, vincristine, prednisolone and anti-CD20 monoclonal antibody (rituximab) (R-CHOP) was given for six cycles. The follow-up chest CT scan after the fourth and sixth cycles of chemotherapy revealed a reduced left lung tumour and an increased right lung tumour to 1.8×1.5 cm. A whole body positron emission tomography (PET) scan was performed at the end of the sixth cycle of chemotherapy which showed increased early and delayed standard uptake values (SUV) of 3.5 and 5.0, respectively, in the right lung tumour and no uptake in the left lung lesion. Accordingly, another six cycles of rituximab were administered during the following 6 months. The subsequent chest CT scan showed complete remission of the left lung tumour and an enlarged 2.8×3.3 cm right lung mass (fig 1B).

{kind=link}
{kind=link}
QUESTION
What may have caused the differing treatment responses of the bilateral pulmonary tumours?
See page 239 for answer.
This case was submitted by:
Footnotes
-
Competing interests: None.
Linked Articles
- Pulmonary puzzle