Article Text

Statistics from Altmetric.com
CLINICAL PRESENTATION
Two homozygotic twins were delivered at 31 weeks of gestational age by caesarean section, with birth weight 1490 and 1710 g, respectively. The family history was unremarkable. Their mother received steroid prophylaxis for hyaline membrane disease. They showed no perinatal problems. By the age of 8 months both had recurrent spells of respiratory distress, possibly triggered by viral infections, characterised by cough, fever, wheezing, tachypnoea, dyspnoea, desaturation, bilateral crackles and chest radiographs suggestive of an acute interstitial involvement. One twin had four admissions (two of these required orotracheal intubation) and the other had three (one with intubation). Each time they were empirically treated with oxygen, antibiotics, steroids and nebulised bronchodilators. Endotracheal tube suction cultures and tests for cytomegalovirus, Pneumocystis and Mycoplasma were negative.
By 11 months of age both showed progressive growth impairment (from 25° to 3° centile) and, in the following months, reduced levels of physical activity. Physical examination progressively showed digital clubbing, chest deformities with flattening of the anteroposterior diameter, tachypnoea at rest (respiratory rate 60/min and 50/min) with oxygen saturation of 97% in both and no requirement for domiciliary oxygen.
Sweat tests, immunoglobulin levels, fecal elastase levels and lymphocyte subsets were normal. Genetic tests for cystic fibrosis, Schwachmann disease and mannose binding lectin deficiency were negative. The cardioechogram was normal with no evidence of pulmonary hypertension.
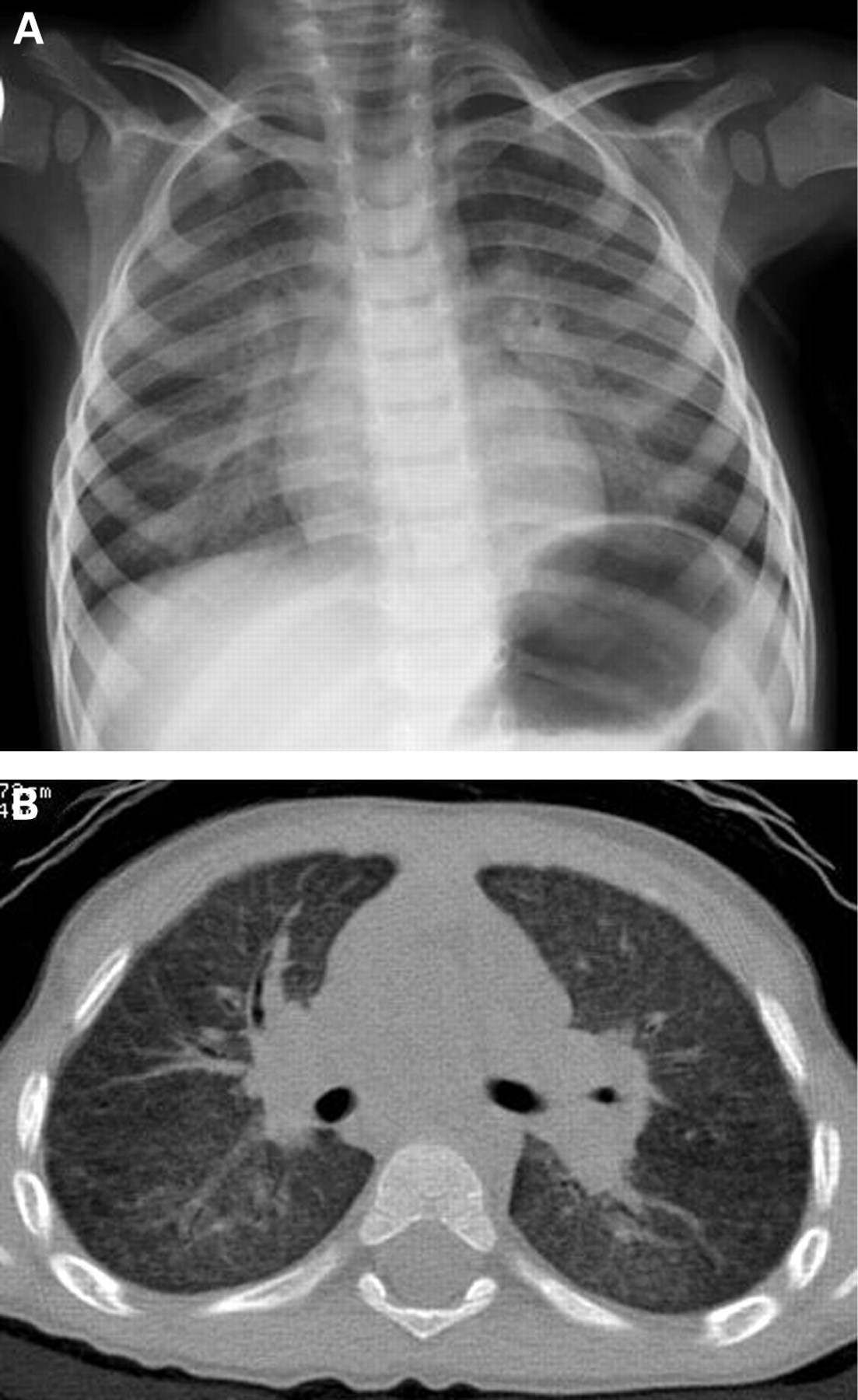
At the age of 30 months a chest radiograph performed in the twin with the most severe clinical history during a period of well being showed persistent findings of interstitial alveolar involvement (fig 1A). At that age his respiratory rate at rest was 60/min, heart rate 120/min, oxygen saturation 97% with digital clubbing. In the same twin a high-resolution CT scan of the chest revealed ground glass attenuation with interstitial pattern and fine nodules throughout the lungs (fig 1B).

{kind=link}
Footnotes
Competing interests: None.
Patient consent: Parental/guardian consent obtained.