Article Text

Abstract
Background: Statins have anti-inflammatory properties that may be beneficial in the treatment of asthma. A study was undertaken to test the hypothesis that atorvastatin added to inhaled corticosteroids improves lung function and airway inflammation in atopic adults with asthma.
Methods: 54 adults with atopic asthma were recruited to a double-blind randomised controlled crossover trial comparing the effect of oral atorvastatin 40 mg daily with that of a matched placebo on asthma control and airway inflammation. Each treatment was administered for 8 weeks separated by a 6-week washout period. The primary outcome was morning peak expiratory flow (PEF). Secondary outcomes included forced expiratory volume in 1 s, asthma control questionnaire score, airway hyper-responsiveness to methacholine, induced sputum cytology and inflammatory biomarkers.
Results: At 8 weeks the change in mean morning PEF compared with baseline did not differ substantially between the atorvastatin and placebo treatment periods (mean difference −0.5 l/min, 95% CI −10.6 to 9.6, p = 0.921). Values for other clinical outcomes were similar between the atorvastatin and placebo treatment periods. The absolute sputum macrophage count was reduced after atorvastatin compared with placebo (mean difference −45.0×104 cells, 95% CI −80.1 to −9.7, p = 0.029), as was the sputum fluid leucotriene B4 (mean difference −88.1 pg/ml, 95% CI −156.4 to −19.9, p = 0.014).
Conclusion: The addition of atorvastatin to inhaled corticosteroids results in no short-term improvement in asthma control but reduces sputum macrophage counts in mild to moderate atopic asthma. The change in sputum macrophage count suggests potential areas for investigation of statins in other chronic lung diseases.
Statistics from Altmetric.com
Statins are inhibitors of 3-hydroxymethyl-3-glutaryl coenzyme A reductase (HMG CoA reductase), a rate-limiting step in cholesterol synthesis. In addition to clinically important cholesterol-lowering properties,1 statins also have diverse anti-inflammatory effects.2–5 They prevent the isoprenylation of signalling molecules such as Ras and Rho, which are involved in driving many inflammatory processes including lymphocyte activation. Statin treatment therefore has the potential to modify immune-driven diseases, and this has been tested in experimental models of autoimmune diseases.6 A recent trial of atorvastatin in rheumatoid arthritis showed improvement in clinical outcome measures7 associated with reduction in blood inflammatory biomarkers such as erythrocyte sedimentation rate, C-reactive protein (CRP) and interleukin 6 (IL6).
Atopic asthma is an immune-mediated airway disease associated with eosinophilic airway inflammation and Th2 cytokine functional profile.8 Recent studies have shown that simvastatin and pravastatin can effectively reduce these acute changes in murine models of allergic lung inflammation.3 9 10 It has been postulated that the anti-inflammatory effects of statins may have relevance for the treatment of asthma and other respiratory disease.5
The aim of this study was to test the hypothesis that atorvastatin added to inhaled corticosteroid treatment improves lung function and sputum cell counts in atopic adults with asthma. We designed a randomised double-blind crossover placebo controlled trial to investigate the effect of oral atorvastatin 40 mg daily for 8 weeks on measures of asthma control and airway inflammation in adults with allergic asthma receiving inhaled corticosteroids alone. The dose and duration of statin therapy with atorvastatin was greater than that used in a previous placebo controlled crossover trial of short-term low-dose simvastatin in 16 subjects with steroid-naïve asthma which showed no clinical beneficial effects on asthma control.11 Atorvastatin was chosen because of its favourable in vitro and in vivo anti-inflammatory properties7 12 13 and evidence of clinical benefit at a dose of 40 mg daily in rheumatoid arthritis.7
METHODS
Subjects
Subjects with chronic symptomatic atopic asthma aged 18–70 years were recruited from general practices and hospital clinics. They were taking ⩽1000 μg beclometasone equivalent daily, no other medication for asthma other than a short-acting β2 agonist and had been on stable medication for at least 4 weeks before randomisation. Atopy to common allergens was established by skin prick test or specific serum IgE antibody measurement. Subjects were excluded if they were pregnant or lactating, current smokers, ex-smokers with a smoking history of >5 pack-years, receiving statins or had a known allergy to them, had a respiratory tract infection or needed oral corticosteroids in the 6 weeks preceding inclusion. All participants gave written informed consent. The study was approved by the West Glasgow ethics committee.
Study design and assignment
The study was a 24-week randomised double blind crossover study comparing the effect of oral atorvastatin therapy (40 mg daily) with that of a matched placebo on asthma control and airway inflammation. After a 2-week run-in period, each treatment was administered to randomised patients for 8 weeks, separated by a 6-week washout period. Randomisation was performed by a centralised telephone service in sequential blocks of four. Researchers and participants were blinded to allocation and had no access to the randomisation code held by the data centre until completion of the study.
During the 2-week run-in period, subjects continued their usual asthma medication and recorded peak expiratory flow (PEF) and symptoms twice daily in their diary. Further visits were undertaken at randomisation and after 2, 4 and 8 weeks (phase 1). After a washout period of 6 weeks, phase 2 of the crossover was started with visits after 2, 4 and 8 weeks. At each visit, spirometry was performed. Patients recorded morning and evening PEF measurements and symptoms throughout the study. Before and after each treatment period, airway responsiveness to methacholine, a validated asthma control questionnaire (ACQ) score, asthma quality of life questionnaire (AQLQ) score, induced sputum and exhaled nitric oxide (FeNO) were recorded and blood samples were taken for immunological tests, lipids and liver functions. Tablets were counted at the end of each treatment period as a measure of compliance.
Measurements
Patients maintained a validated diary card14 recording morning and night PEF (Mini-Wright; Clement Clarke, Harlow, UK), daytime symptoms, night awakenings, use of inhaled rescue medication and study tablet consumption. Spirometric parameters were measured with a dry spirometer (Vitalograph, Buckingham, UK).15 ACQ was recorded.16 Methacholine airway responsiveness was measured in subjects with a baseline forced expiratory volume in 1 s (FEV1) of >60% predicted using Cockcroft’s technique17 with concentrations of methacholine from 0.03 to 16 mg/ml.18 Skin prick tests for allergy to cat dander, house dust mite (Dermatophagoides farinae) and mixed grass pollen were performed (Soluprick, ALK, Horsholm, Denmark). Total IgE and specific IgE to house dust mite, grass pollen and cat dander were assayed by the Unicap 100 System (Pharmacia, Milton Keynes, UK). Total IgE levels >120 IU/ml and specific IgE levels >0.35 AU/ml were considered raised. Atopy was defined when a patient had a positive skin prick test or elevated specific IgE level. Sputum was induced as previously described.19 Differential cell counts were performed and the sputum supernatant fluid analysed for leucotriene (LT) B4 and myeloperoxidase (MPO) using an enzyme immunoassay (R&D Systems, Abingdon, UK). Interleukin-8 (IL-8), tumour necrosis factor α (TNFα) and interferon γ (IFNγ) were measured using a Luminex microbead fluorescence kit (Biosource, Invitrogen, Paisley, UK). FeNO was measured using a chemiluminescence analyser (Logan Research, Rochester, UK) at a flow rate of 50 ml/s according to consensus guidelines.20 Serum was analysed for IL5, high sensitivity (hs) IL6, IL8, hsTNF-α, soluble intercellular adhesion molecule-1 (sICAM-1) and high sensitivity C-reactive protein (hsCRP) by an enzyme immunoassay (R&D Systems). Peripheral blood concentrations of urea, electrolytes, lipids, liver function and full blood count were measured in the hospital accredited laboratories at the beginning and end of each treatment period.
Statistical analysis
Baseline characteristics were described by number and percentage of patients for categorical variables and mean (SD) for continuous variables. Response to atorvastatin on lung function, diary data, induced sputum, mediator levels and exhaled nitric oxide versus placebo was assessed by normal linear models that included parameters for patient, period and treatment. When variables were unsuitable for this, the within-patient treatment differences were calculated and then analysed by either t test or Wilcoxon test, as appropriate. Significance at a level of 5% was accepted for the primary end point, the mean of the morning PEF measurements taken from the 7 days of diary recording before each study visit. The mean was calculated if there were at least 3 days of completed data within that period.
A sample size of 44 was calculated to have 90% power to detect a difference in means of 20 l/min in PEF (primary end point),21 assuming a standard deviation of differences of 40 l/min using a paired t test with a 5% two-sided significance level. A total of 54 patients were recruited to ensure that 44 patients completed the study. All data were analysed using SAS Version 9 (SAS Institute, Cary, North Carolina, USA).
RESULTS
Recruitment and baseline characteristics
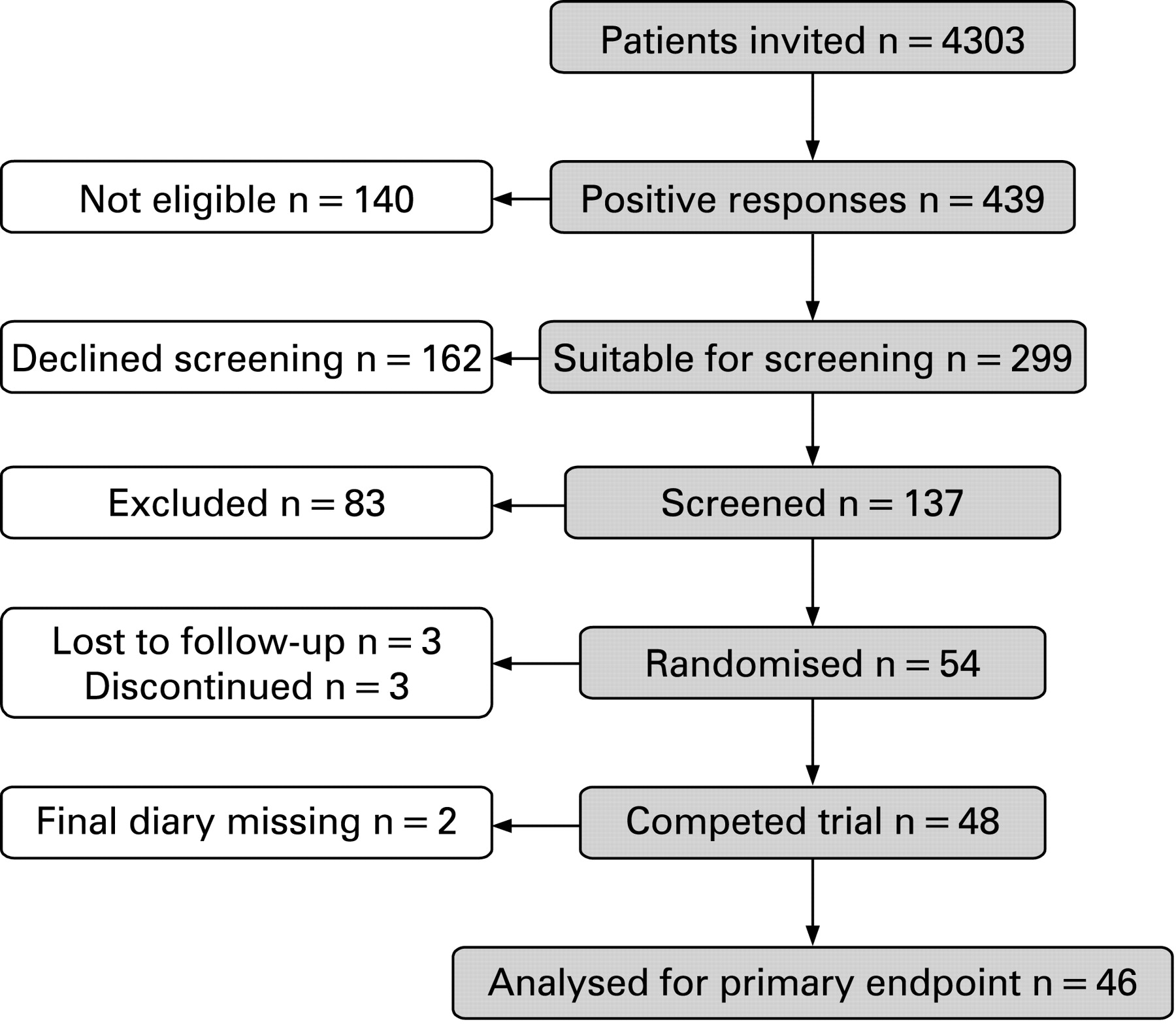
A total of 4303 patients with asthma from 39 practices and hospital clinics were invited to participate in the study (fig 1). Of the 439 replies received, screening visits were arranged for 137 volunteers and 54 were randomised. Baseline demographic and clinical characteristics of the patients are shown in table 1 and baseline inflammatory biomarkers in table 2. Distributions of baseline characteristics were similar for patients starting with placebo and those starting with atorvastatin. All subjects were atopic.

Changes in clinical outcomes
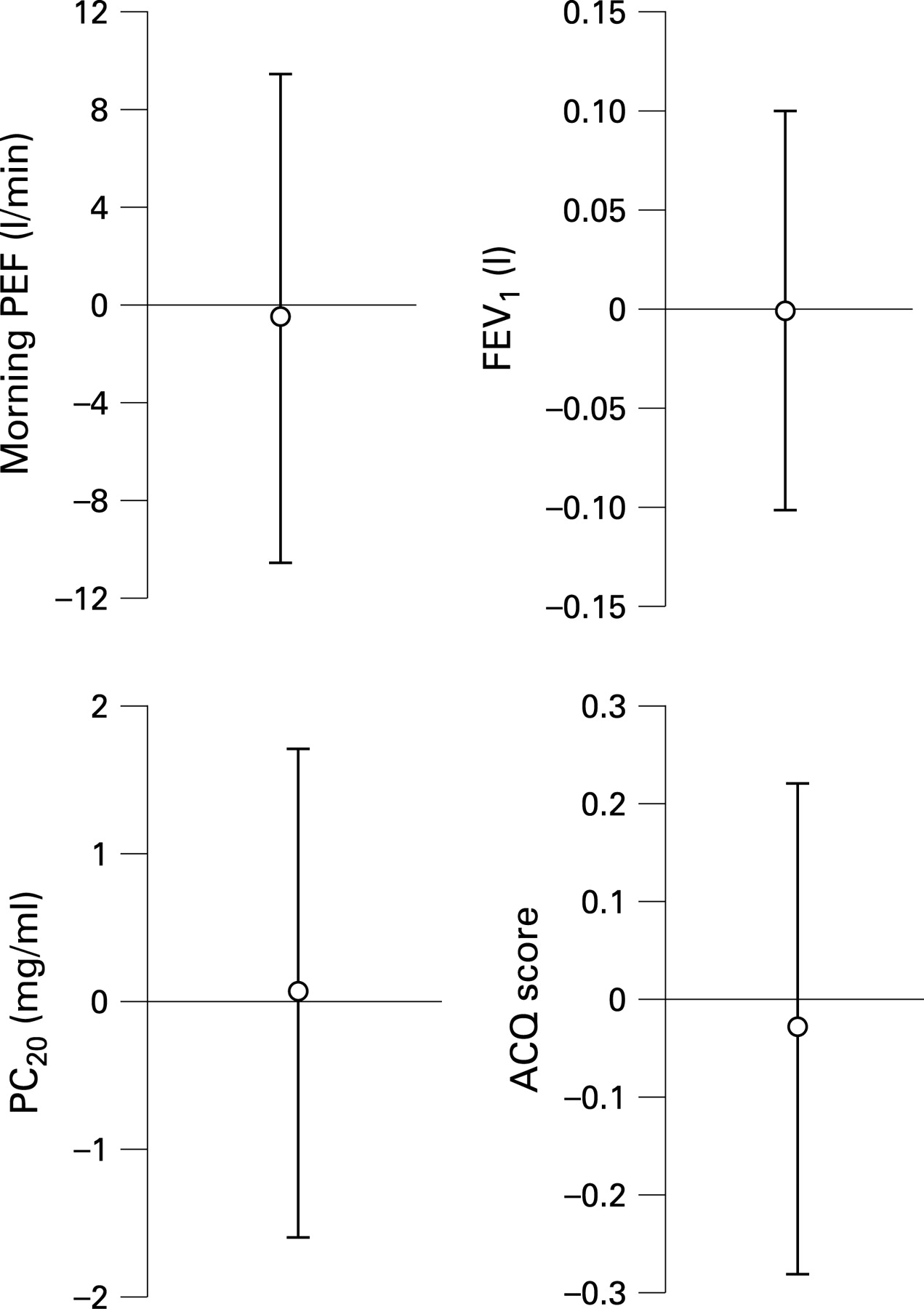
Changes in clinical outcomes after atorvastatin treatment are listed in table 3 and shown in fig 2. At 8 weeks the change in mean morning PEF compared with baseline did not differ between the atorvastatin and placebo treatment periods (mean difference −0.5 l/min, 95% confidence interval (CI) −10.6 to 9.6, p = 0.921).

The estimated mean difference for the primary outcomes (20 l/min) was much larger than that obtained in the study. No statistically significant effect of atorvastatin was seen in evening PEF, pre- and post-salbutamol FEV1 or methacholine responsiveness (PC20). Similarly, there was no significant difference in ACQ score or AQLQ score between atorvastatin and placebo treatment periods.
Changes in inflammatory biomarkers
Induced sputum cytology
The total cell counts recovered from sputum were similar after atorvastatin and after placebo treatment (table 3). After 8 weeks the mean absolute and relative sputum macrophage count was significantly reduced after atorvastatin compared with placebo (mean absolute difference −44.9×104 cells, 95% CI −80.1 to −9.7, p = 0.029; table 3, fig 3). There was a reciprocal increase in the relative proportion of sputum neutrophils (mean proportion difference 13.1% (95% CI 1.8 to 24.4), p = 0.025; table 3, fig 3), but there were no significant changes in the absolute count of these cells or the counts and proportions of the other sputum cell phenotypes under atorvastatin treatment.

{kind=link}
{kind=link}
{kind=link}
Inflammatory biomarkers in sputum
The sputum concentrations of inflammatory cytokines and mediators were similar after atorvastatin and after placebo treatment (table 3) other than LTB4 which was significantly reduced (mean difference −88.1 pg/ml (95% CI −156.4 to −19.9), p = 0.014).
Exhaled nitric oxide
There was no significant change in FeNO after atorvastatin compared with placebo (mean difference −1.6 ppb (95% CI −7.1 to 3.9), p = 0.559; table 3).
Inflammatory biomarkers in serum
No significant difference was seen in the concentration of any serum marker of inflammation between atorvastatin and placebo treatment periods (table 3). The change in hsCRP was of borderline significance (mean difference −0.65 mg/l (95% CI −1.38 to 0.09), p = 0.082) but there were no changes in sICAM-1, TNFα, IL-5, IL-6 and IL-8.
Change in biochemical markers
The biochemical effects of atorvastatin therapy were reflected in a significant reduction in concentration of serum lipids: cholesterol (mean difference −1.71 mmol/l, 95% CI −1.94 to −1.48, p<0.0001), HDL-cholesterol (mean difference −0.14 mmol/l, 95% CI −0.26 to −0.02, p = 0.026), but not triglycerides (table 3). There were significant, albeit modest, increases in mean bilirubin, aspartate aminotransferase (AST) and alanine aminotransferase (ALT).
Adverse events
Adverse event rates were similar in patients taking atorvastatin and in those on placebo. One patient receiving atorvastatin required oral steroid compared with none in the placebo group. Two patients from each group made unscheduled visits to their general practitioner and two patients from the atorvastatin group compared with one from the placebo group attended the emergency department in relation to their asthma during the study. Equal numbers of patients were lost to follow-up in both arms of the study. One patient died of unrelated causes while taking the placebo medication.
Compliance
There was no difference in compliance, assessed by number of tablets returned and by biochemical results.
DISCUSSION
This randomised controlled study tested the hypothesis that atorvastatin added to inhaled corticosteroids could improve lung function and airway inflammation in adults with allergic asthma. We found that that there were no clinically important improvements in a range of clinical indices of asthma control after 8 weeks of treatment with atorvastatin despite expected changes in serum lipids. There were, however, changes in airway inflammation and, in particular, a reduction in the absolute sputum macrophage count after atorvastatin compared with placebo and an associated reduction in sputum LTB4.
The lack of any evidence of clinical benefit of atorvastatin in allergic asthma confirms and extends the findings of Menzies et al11 who performed a randomised placebo controlled crossover trial of simvastatin in 16 steroid-naïve subjects with asthma. Simvastatin was administered for 2 weeks at 20 mg daily and 2 weeks at 40 mg daily, with no washout between active and placebo treatment periods.11 In our study the statin chosen, atorvastatin, was administered at a higher dose and for a longer duration and to a larger group of participants (n = 54), but we found no evidence of improvement in lung function or airway hyper-responsiveness. We estimated that 8 weeks duration of therapy was long enough to show a clinical effect, on the basis that serum cholesterol levels fall within 6 weeks of statin treatment22 and our own findings show a highly significant drop in cholesterol after 8 weeks’ treatment. Plasma CRP concentration has been shown to fall within 4 weeks, and possibly even in the first 2 days of treatment.23 However, CRP reduction was only of borderline significance in the present study, possibly because the CRP levels were not high at baseline or due to lack of statistical power. Changes in CRP may be more apparent in lung diseases with raised CRP levels such as chronic obstructive pulmonary disease (COPD), or in exacerbations, because previous studies have suggested that statins decrease episodes of pneumonia.24 Statins have an inhibitory effect on human airway smooth muscle cell proliferation,25 so it is possible that the administration of atorvastatin for a longer duration of time might have improved different clinical outcome measures of asthma such as indices of airway remodelling.
It is unlikely that using a different statin would have shown any greater effects. A trial in rheumatoid arthritis7 used atorvastatin with evidence of clinical benefit. Although the initial experimental work in inflammatory lung disease used simvastatin3 10 and pravastatin,9 Joukhadar and colleagues showed no difference in effect on inflammatory parameters when comparing atorvastatin, simvastatin or pravastatin.12 Furthermore, no therapeutic effect was found with simvastatin in asthma.11 The 6-week washout period in the present study was considered acceptable because evidence suggests that the anti-inflammatory effects of statins do not last this long. Circulating levels of soluble vascular cell adhesion molecule-1 revert to normal in 2 days,26 and CRP27 and IL6 concentrations have returned to baseline after 7 days withdrawal.23 28 No evidence of a carryover effect on clinical outcome measures was seen in the present study.
One possible explanation for the apparent lack of clinical efficacy in this study is that all patients were taking regular inhaled corticosteroid therapy and had a low basal sputum eosinophil count. In the study by Menzies et al, all patients were withdrawn from inhaled corticosteroids before treatment began, with patients receiving a long-acting β2 agonist instead.11 The lack of efficacy with atorvastatin is unlikely to be due to insufficient room for improvement in clinical outcome measures since the patient group had evidence of reversibility in FEV1 of approximately 15% and a raised mean ACQ score of 1.5. Compliance with medication was supported by tablet counting and by the significant changes in serum lipids and liver function tests observed in the patients receiving atorvastatin.
Statin therapy had no effect on any of the inflammatory biomarkers other than decreases in sputum macrophage count and LTB4 concentration.
Several mechanisms, either alone or in combination, might explain these observations. First, statins reduce growth of both animal and human macrophages29 30 and it is possible that atorvastatin had a similar effect on sputum alveolar macrophage numbers. Second, LTB4 is raised in induced sputum supernatant in asthma31 and mediates the recruitment of alveolar macrophages through the B leucotriene receptor-1.32 The decrease in sputum LTB4 concentrations observed in patients treated with atorvastatin could contribute to the reduced sputum macrophage count. Third, statins interfere with cell binding by reducing monocyte to endothelial cell adhesion and the recruitment of macrophages to the lung.33 34 Finally, statins reduce the in vitro release of cytokines and mediators including TNFα from monocytes35 and endothelial cells.36 37 Similar effects on the release of these cytokines and mediators, including from cells within the airways, could reduce the recruitment of alveolar macrophages to the airways. Against this latter mechanism, we found no reduction in sputum TNFα or circulating IL6, TNFα and ICAM-1 concentrations following atorvastatin therapy. Future studies should examine these potential pathways.
The reduction in alveolar macrophage count found in patients with allergic asthma may have relevance to the treatment of chronic lung diseases such as COPD in which alveolar macrophage function has been implicated in the pathogenesis.38 Lovastatin has effects on human and mouse macrophage function by enhancing the clearance of apoptotic cells, a statin-specific effect reversible with mevalonate, through modulation of Rho-GTPases.39 Production of matrix metalloproteinase-9 is also reduced by statins,29 which could also have an impact on COPD. Recent evidence suggests that statins may inhibit lung parenchymal destruction and peribronchial and perivascular infiltration of inflammatory cells in a rat model of smoking-induced emphysema.40
In a mouse model, the neutrophilia associated with acute lung injury is markedly reduced with lovastatin treatment.41 Paradoxically, we found a significant increase in the proportion of neutrophils in induced sputum with atorvastatin therapy. The absolute neutrophil counts were not significantly different between groups, suggesting that the increased proportion of neutrophils occurred because of the low macrophage proportion and the expression of the results as a percentage. In support of this explanation, the sputum LTB4 concentration was reduced after atorvastatin therapy, which would be more likely to be associated with a reduced neutrophil count.
In conclusion, we have shown that short-term treatment with statins does not improve lung function or other indices of asthma control in patients with mild to moderate atopic asthma who are already receiving treatment with inhaled corticosteroids. The reduction in the sputum macrophage count suggests potential areas for investigation of atorvastatin in chronic lung disease in which activated alveolar macrophages have been implicated in the pathogenesis, such as COPD.
Acknowledgments
The authors thank the Research and Development Directorate of the Greater Glasgow Primary Care NHS Trust (provided funding support) and, in particular, acknowledge the advice and guidance of Brian Rae of that department, Kay Pollock of the Pharmacy Production Unit, Western Infirmary Glasgow; also the Pharmacy Department of Gartnavel General, Glasgow; Biochemistry and Immunology laboratories at the Western Infirmary, Glasgow; and all the general practitioners and their staff who assisted with recruitment.
REFERENCES
Footnotes
Funding: Funded by Asthma UK.
Competing interests: None.
Ethics approval: All participants gave written informed consent and the study was approved by the West Glasgow ethics committee.
This paper is dedicated to the memory of Dr Stuart Wood, Senior Lecturer in General Practice at the University of Glasgow, who died in March 2006.
Linked Articles
- Airwaves