Article Text

Abstract
Background: Circulating levels of Clara cell secretory protein-16 (CC-16) have been linked to Clara cell toxicity. It has therefore been suggested that this protein may be a useful marker of chronic obstructive pulmonary disease (COPD).
Methods: Serum CC-16 levels were measured in 2083 individuals aged 40–75 years with COPD and a smoking history of ⩾10 pack-years, 332 controls with a smoking history of ⩾10 pack-years and normal lung function and 237 non-smoking controls.
Results: Serum CC-16 had a coefficient of repeatability of 2.90 over 3 months in a pilot study of 267 individuals. The median serum CC-16 level was significantly reduced in a replication group of 1888 current and former smokers with COPD compared with 296 current and former smokers without airflow obstruction (4.9 and 5.6 ng/ml, respectively; p<0.001) and 201 non-smokers (6.4 ng/ml; p<0.001). Serum levels of CC-16 were lower in current than in former smokers with GOLD stage II and III COPD but were not different in individuals with stage IV disease. Former, but not current smokers, with COPD had lower serum CC-16 levels with increasing severity of COPD (GOLD II vs GOLD IV COPD: 5.5 and 5.0 ng/ml, p = 0.006; r = 0.11 with forced expiratory volume in 1 s, p<0.001) and had significantly higher levels if they also had reversible airflow obstruction (p = 0.034). Serum CC-16 was affected by gender and age (r = 0.35; p<0.001) in subjects with COPD but not by body mass index or the presence of either chronic bronchitis or emphysema.
Conclusions: Serum CC-16 levels are reduced in individuals with COPD and there is a weak correlation with disease severity in former smokers.
Trial registration number: SCO104960, NCT00292552.
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) was responsible for 3 million deaths in 20051 and is predicted to become the third leading cause of death by 2020.2 It is a major cause of morbidity that is estimated to affect 210 million people worldwide.3 The development of disease is intimately associated with the inhalation of noxious agents, particularly cigarette smoke.2 This causes airways disease and emphysema that result in progressive irreversible airflow obstruction. Despite its prevalence, there are no biomarkers that can distinguish current and former smokers with and without airflow obstruction and which can be used to monitor the response to therapeutic interventions.4 5 An ideal biomarker should be lung-specific, reproducible, easy to assess in large numbers of patients and validated in a large well-characterised cohort of patients and controls.6
Clara cell secretory protein-16 (CC-16, CC-10 or uteroglobulin) is a member of the secretoglobin family of small secreted disulphide-bridged dimeric proteins.7 It is secreted by the non-ciliated Clara cells8 which are found predominantly in the respiratory bronchioles, and by non-ciliated columnar cells of the large and small airways.9 CC-16 is also expressed in the epithelial cells of the nose10 and the male and female urogenital tract.11 Despite being produced by other tissues, serum levels of CC-16 largely reflect protein produced by the lower respiratory tract with little contribution from protein released by the urogenital organs.12 Circulating levels of CC-16 have therefore been suggested as a marker of respiratory disease.
CC-16 acts as an immunosuppressant and provides protection against oxidative stress and carcinogenesis.13 Serum levels rise following acute exposure to smoke, chlorine and lipopolysaccharide.11 They also rise in response to ozone but can be suppressed by inhaled fluticasone propionate.14 The serum level of CC-16 is low in subjects with obliterative bronchiolitis,15 asthma16 and in smokers.12 It is reduced in the lungs of smokers and individuals with COPD.17 18 There are conflicting data on the serum level of CC-16 in COPD,17 19 20 but this has yet to be assessed in a large cohort of well-characterised individuals. We have used the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) cohort to evaluate serum CC-16 as a potential biomarker for COPD (see Appendix 1).
METHODS
The aims and operational aspects of the ECLIPSE cohort have been described elsewhere.21 Briefly, ECLIPSE is a 3-year multicentre longitudinal prospective study to identify novel endpoints in COPD. Individuals aged 40–75 years were recruited to the study if they had a smoking history of ⩾10 pack-years, a post-bronchodilator ratio between forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC) ⩽0.7 and GOLD stage II (FEV1 50–80% predicted), III (FEV1 30–50% predicted) or IV (FEV1 <30% predicted) COPD.2 Smoking (⩾10 pack-years) and non-smoking (<1 pack-year) control subjects were enrolled if they were aged 40–75 years and had normal lung function (post-bronchodilator FEV1 >85% predicted and FEV1/FVC >0.7). Individuals recruited to the study were genotyped for α1-antitrypsin deficiency. Six PiZZ and 11 PiSZ individuals were identified and excluded from the analysis. All subjects underwent standardised spirometry following 180 μg (2 puffs) salbutamol22 with reversible airflow obstruction being defined as an increase in FEV1 of 15% and at least 200 ml.
All subjects were offered a low-dose CT scan of the chest to exclude non-COPD-related disease and to evaluate the severity and distribution of emphysema. The CT scans were evaluated at the central imaging unit at the University of British Columbia, Vancouver. The extent of emphysema was assessed in two ways. First, it was independently scored by two radiologists who were blind to the individual’s lung function. Emphysema was reported as trivial, mild, moderate, severe and very severe if it affected <5%, 5–25%, 25–50%, 50–75% and >75% of the lungs, respectively. A consensus reading was obtained when there was a difference of more than one emphysema category between the two observers. Otherwise, the average of the two readings was used in the analysis. Second, emphysema was assessed by the percentage of the lung with attenuation below −950 HU using the Pulmonary Workstation 2.0 software (VIDA Diagnostics, Iowa City, IA, USA).
Measurement of serum CC-16
Whole blood was collected into Vacutainer tubes at the beginning of the study. Serum was prepared by centrifugation at 1500 g for 10–15 min. The serum was collected and stored at −80°C until analysed. Serum CC-16 was measured by operators who were blind to an individual’s lung disease using a colorimetric sandwich immunoassay method (BioVendor GmbH, Heidelberg, Germany) according to the manufacturer’s instructions. Serum samples were diluted 5–20-fold with the dilution buffer supplied by the manufacturer. The concentration of CC-16 was determined by comparison with a standard curve prepared with known concentrations of CC-16. The assay had a validated range of 80–4000 pg/ml with an intra-assay coefficient of variation and relative error of 1.67% to 4.10% and −9.15% to −2.01%, respectively, and an inter-assay coefficient of variation and relative error of 3.75% to 4.85% and −11.96% to −1.08%, respectively.
Statistical analysis
Reproducibility of CC-16 in the ECLIPSE cohort was assessed using Bland-Altman plots. Owing to the non-normality of CC-16 values identified by Shapiro-Wilk and Kolmogorov-Smirnov tests, all CC-16 values in the ECLIPSE cohort were log-transformed prior to analysis. All comparisons between subject groups were then conducted by analysis of variance (ANOVA) based on the log-transformed values. Spearman correlation coefficients (based on ranks) were calculated for correlations between CC-16 and clinical parameters. All analyses were performed with SAS Version 8.2 (SAS Institute, Cary, NC, USA).
RESULTS
Pilot study to test the reproducibility of serum CC-16
It is important to assess whether a putative biomarker is reproducible over time. Serum CC-16 was measured in an age-matched subgroup of 195 former smokers with COPD, 36 former smoking controls and 36 non-smoking controls selected from the ECLIPSE cohort (table 1). It gave reproducible values in non-smokers, smokers without airflow obstruction and across all severities of COPD when measured over a period of 3 months (coefficient of repeatability 2.90, variability 15.8%, fig 1 and table 1). The results for serum CC-16 were within the 95% limits of agreement for most of the subjects tested. However, several subjects showed a high degree of variability between the values at baseline and at 3 months. The reason for this was unclear. There was no reproducible difference between median levels of CC-16 in former smokers with and without COPD in these pilot samples. The median level of CC-16 was significantly lower in subjects with COPD than in non-smoking controls (p = 0.005).

Assessment of serum CC-16 in individuals with COPD
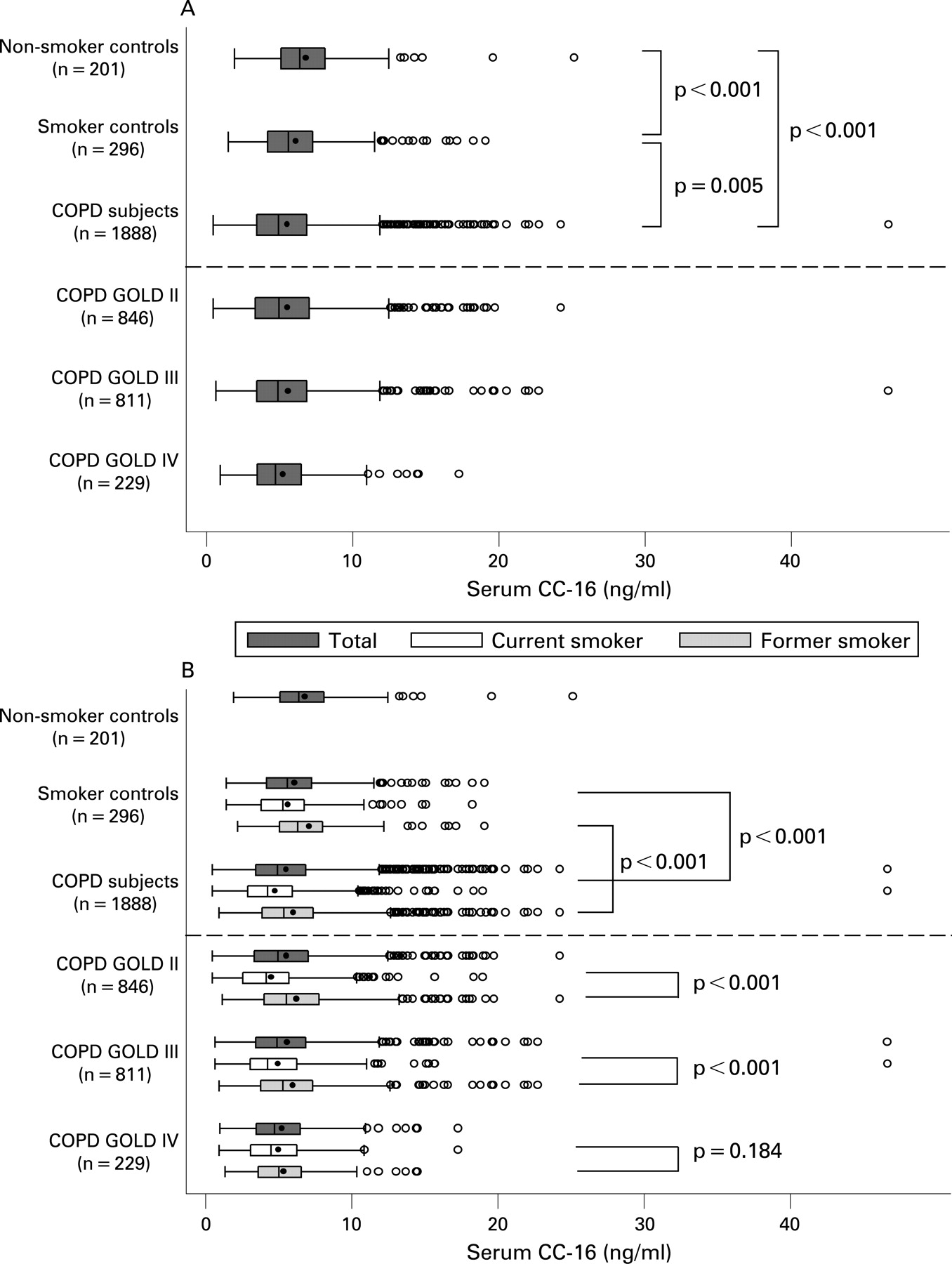
Serum CC-16 was then measured in a larger replication set of 1888 individuals with COPD, 296 smoking controls with no airflow obstruction and 201 non-smoking controls (table 2 and fig 2A). The median serum CC-16 level was significantly lower for current and former smokers with COPD than for current and former smokers with no airflow obstruction (4.9 and 5.6 ng/ml, respectively; p<0.001). Median CC-16 levels were significantly lower in current and former smokers with no airflow obstruction than in non-smoking controls (5.6 and 6.4 ng/ml, respectively; p = 0.005). However, there was no significant difference in serum CC-16 levels with increasing severity (GOLD stage) COPD when analysed in this mixed group of current and former smokers.

{kind=link}
{kind=link}
Serum CC-16 levels were higher in men than women with COPD (5.21 and 4.30 ng/ml; n = 1222 and 666, respectively; p<0.001) and in smoker controls (6.09 and 4.66 ng/ml; n = 161 and 135, respectively; p<0.001) but they were similar in men and women who were non-smokers (6.88 and 6.25 ng/ml; n = 74 and n = 127, respectively; p = 0.385). There was a significant correlation between CC-16 levels and age (r = 0.35; p<0.001), but serum CC-16 was not affected by body mass index or the presence of either chronic bronchitis or emphysema (whether scored by the radiologist or analysis of lung density). There was a small but significant difference in serum CC-16 levels in those who did take long-acting β2 agonists compared with those who did not (4.81 and 5.07 ng/ml; n = 1280 and 608, respectively; p = 0.047), but there was no difference in serum CC-16 levels between individuals who were taking inhaled corticosteroids and those who did not (4.81 and 5.08 ng/ml; n = 1346 and 542, respectively; p = 0.135). Median serum CC-16 levels were lower in current smokers than in former smokers, both with (4.2 and 5.4 ng/ml; n = 746 and 1142, respectively; p<0.001) and without COPD (5.3 and 6.3 ng/ml; n = 201 and 95, respectively; p<0.001). The pack-years smoked were 48.7 and 49.9 for former and current smokers with COPD and 31.2 and 32.4 for former and current smokers with no airflow obstruction.
Our data show a clear effect of current smoking on serum levels of CC-16. This biomarker was therefore analysed in groups divided into current and former smokers (fig 2B). Median serum levels of CC-16 were lower in current than in former smokers in individuals with stage II and III COPD but not in those with stage IV disease. The serum levels of CC-16 were reduced in individuals with stage IV COPD irrespective of whether they were current or former smokers. There was a weak correlation between serum CC-16 with severity of COPD in former smokers (GOLD II vs GOLD IV: 5.5 vs 5.0 ng/ml, p = 0.006; r = 0.11 with FEV1, p<0.001) but not in current smokers (GOLD II vs GOLD IV: 4.1 vs 4.5 ng/ml, p = 0.046; r = −0.07 with FEV1, p = 0.069).
It is clear that age, gender, smoking status and lung function can all affect serum levels of CC-16. However, when adjusted for these factors, there was still a significant difference in median levels of serum CC-16 between individuals with COPD and the smoker controls (adjusted means 4.5 and 6.1 ng/ml, respectively, p<0.001).
Assessment of serum CC-16 as a biomarker for reversible airflow obstruction
There was no correlation between serum CC-16 and the presence of reversible airflow obstruction (increase in FEV1 of 15% and at least 200 ml following 180 μg salbutamol) in current and former smokers with COPD (5.2 ng/ml in individuals with reversible airflow obstruction (n = 393) and 4.8 ng/ml in those with no reversible airflow obstruction (n = 1495)). However, former smokers with COPD had significantly higher serum levels of CC-16 if they also had reversible airflow obstruction (6.0 ng/ml for former smokers with reversible airflow obstruction (n = 222) and 5.2 ng/ml for those without reversible airflow obstruction (n = 920) (p = 0.034). Age had no effect, but there was an effect of gender with men having higher levels of serum CC-16 if they also met the criteria for reversible airflow obstruction (5.6 ng/ml for men with reversible airflow obstruction (n = 297) and 5.1 ng/ml for those without reversible airflow obstruction (n = 925) (p = 0.046). There was no correlation between serum CC-16 levels and the magnitude of increase in FEV1 following the administration of 180 μg salbutamol in individuals with COPD (r = 0.04, p = 0.062).
DISCUSSION
Serum CC-16 is a lung-derived protein that has been proposed as a biomarker for epithelial cell dysfunction. COPD is characterised by both airways disease and emphysema, so CC-16 is an obvious candidate for assessment as a marker for this condition. It is important that any putative biomarker is stable when assessed over a short period of time. This was evaluated in a subset of 267 individuals who were either non-smokers or former smokers. Serum levels of CC-16 had a coefficient of repeatability of 2.90 when assessed over a period of 3 months. This reflects 15.8% variability in CC-16 from baseline measurements. Thus, serum CC-16 is relatively stable and therefore worthy of further assessment as a biomarker for COPD.
Serum CC-16 was evaluated in the rest of the ECLIPSE cohort to determine whether it could distinguish individuals with COPD from current and former smokers with normal lung function. Serum CC-16 levels were significantly lower in individuals with COPD than in smokers with normal lung function, and CC-16 levels were also lower in smoking controls than in non-smokers. However, these results should be tempered by the differences in the demographic characteristics of the three groups. Individuals with COPD were significantly older and were more likely to be male than the smoker and non-smoker controls, and they had a greater pack-year smoking history. As a result of the recruitment criteria, they had worse lung function, more emphysema on their CT scans and were more likely to be taking inhaled medication for airways disease. It is therefore important to evaluate the effect of each of these parameters on serum CC-16 levels.
The large number of individuals with COPD recruited to the study made it possible to assess the effect of confounding factors on serum CC-16 levels. Serum levels of CC-16 increased with age in individuals with COPD. This was in keeping with the findings of others,23 and has been attributed to a combination of an age-related decline in glomerular filtration rate (and hence reduced clearance of CC-16) and increased alveolar capillary leak.23 24 These pathologies are likely to be enhanced in individuals with COPD. Serum CC-16 levels were higher in men than in women who were current and former smokers, both with and without COPD. There was no gender effect on serum CC-16 levels in individuals who were non-smokers. The absence of a gender effect is in keeping with previous reports,12 but there has been no assessment of the relationship between gender and levels of CC-16 in individuals with COPD. There are conflicting data on the relationship between serum CC-16 and body mass index,13 25 but no correlation was identified in individuals with COPD in the ECLIPSE cohort.
Smoking status has previously been shown to have a significant effect on serum CC-16 levels.12 Indeed, the serum level of CC-16 was lower in current smokers than in former smokers irrespective of whether or not they had COPD. This is likely to reflect increased epithelial dysfunction as a result of toxins within cigarette smoke. However, it was striking that individuals with GOLD stage IV COPD had similar serum levels of CC-16 irrespective of smoking status. This implies that epithelial damage cannot be reversed by smoking cessation in individuals with the most severe airflow obstruction. Moreover, serum CC-16 may be a useful biomarker of therapeutic strategies to repair epithelial damage in this group of individuals.
It seems likely that a biomarker for COPD will show a trend with increasing disease. This was most apparent in former smokers in whom there were significantly lower serum levels of CC-16 in individuals with GOLD stage IV disease than in those with GOLD stage II COPD. Moreover, there was a weak correlation between serum CC-16 and FEV1 in this group of individuals. The relationship between serum CC-16 and disease was less clear in current smokers in whom serum CC-16 levels were higher in those with more severe disease (as defined by GOLD severity), but there was no correlation between serum CC-16 and FEV1. The opposing effects of levels of serum CC-16 and FEV1 in current and former smokers explains the lack of correlation between serum CC-16 and GOLD stage of COPD in the combined group of former and current smokers with COPD. It is clear that age, gender, smoking status and lung function can all affect serum levels of CC-16. Indeed, this would explain the higher serum level of CC-16 in subjects with COPD in the pilot study of reproducibility than in COPD subjects in the replication cohort. However, if we adjust for all of these factors, serum CC-16 is still significantly lower in individuals with COPD than in the group of smoker controls.
It is important to determine whether the association of serum CC-16 with COPD is driven by the airways or emphysema components of the disease. There was no correlation between the presence or severity of emphysema and serum CC-16 levels in individuals with COPD. This was irrespective of whether emphysema was scored by a radiologist or by density mask imaging. Serum CC-16 has been proposed as a marker of airway epithelial dysfunction, so it may correlate with reversible airways disease. However, there was no correlation between serum CC-16 and symptoms of chronic bronchitis and no difference in serum CC-16 levels between individuals taking inhaled corticosteroids and those taking other medications. However, the serum CC-16 level was reduced in individuals with COPD receiving long-acting β2 agonists and was higher in men than in women and in former than in current smokers with reversible airflow obstruction. Although the effects are modest, the level of CC-16 in the serum may in part reflect reversible airflow obstruction.
Our data indicate that the serum level of CC-16 is reduced in individuals with COPD and that there is a weak correlation with disease severity in former smokers. There is also a signal from CC-16 in former smokers with reversible airflow obstruction. Serum CC-16 did not correlate with lung function or reversible airflow obstruction in current smokers. It is important to consider the usefulness of CC-16 as a biomarker for COPD. The difference between the median levels of serum CC-16 in individuals with COPD, while statistically significant, is small. Moreover, the variation between samples is 15.8%. Thus, CC-16 cannot be used to screen populations of individuals for COPD and cannot be used as a surrogate for lung function testing to evaluate the presence of reversible airflow obstruction. However, there is clearly a signal from CC-16 in individuals with COPD over and above that caused by smoking. Moreover, the levels remain low in former smokers with GOLD stage IV COPD. Serum CC-16 may therefore be useful in longitudinal studies to assess epithelial repair or may be combined with other biomarkers to diagnose or monitor the progression of COPD. Any assay based on serum CC-16 will need to correct for age, gender, smoking status and lung function.
The association between serum CC-16 and COPD reported here is from a cross-sectional study of individuals with COPD. It is clearly important to assess whether CC-16 tracks the decline in lung function and progression of emphysema, airways disease, systemic features (such as body mass index, fatigue, muscle wasting, systemic inflammation) and exacerbations in individuals with COPD during the 3 years of follow-up of the ECLIPSE cohort. These investigations are required to determine whether serum CC-16 levels can report disease progression. Finally, it is important to recognise that changes in serum CC-16 levels are not specific to one agent, disease state or specific exposure.11 Thus, serum CC-16 is likely to be affected by other forms of lung disease.
Acknowledgments
The authors thank all the subjects who took part in these studies and are grateful to E Kurali, GlaxoSmithKline for exploratory statistics. The CT scans were qualitatively assessed by Drs N Müller and P Nasute Fauerbach, Vancouver.
Appendix 1 Principal investigators and centres participating in ECLIPSE (NCT00292552, SCO104960)
Bulgaria: Y Ivanov, Pleven; K Kostov, Sofia. Canada: J Bourbeau, Montreal; M Fitzgerald, Vancouver; P Hernandez, Halifax; K Killian, Hamilton; R Levy, Vancouver; F Maltais, Montreal; D O’Donnell, Kingston. Czech Republic: J Krepelka, Praha. Denmark: J Vestbo, Hvidovre. The Netherlands: E Wouters, Horn. New Zealand: D Quinn, Wellington. Norway: P Bakke, Bergen. Slovenia: M Kosnik, Golnik. Spain: A Agusti, Palma de Mallorca. Ukraine: Y Feschenko, Kiev; V Gavrisyuk, Kiev; L Yashina, Kiev; N Monogarova, Donetsk. UK: P Calverley, Liverpool; D Lomas, Cambridge; W MacNee, Edinburgh; D Singh, Manchester; J Wedzicha, London. USA: A Anzueto, San Antonio, TX; S Braman, Providence, RI; R Casaburi, Torrance CA; B Celli, Boston, MA; G Giessel, Richmond, VA; M Gotfried, Phoenix, AZ; G Greenwald, Rancho Mirage, CA; N Hanania, Houston, TX; D Mahler, Lebanon, NH; B Make, Denver, CO; S Rennard, Omaha, NE; C Rochester, New Haven, CT; P Scanlon, Rochester, MN; D Schuller, Omaha, NE; F Sciurba, Pittsburgh, PA; A Sharafkhaneh, Houston, TX; T Siler, St Charles, MO; E Silverman, Boston, MA; A Wanner, Miami, FL; R Wise, Baltimore, MD; R ZuWallack, Hartford, CT.
Steering Committee: H Coxson (Canada), L Edwards (GlaxoSmithKline, USA), K Knobil (Co-chair, GlaxoSmithKline, UK), D Lomas (UK), W MacNee (UK), E Silverman (USA), R Tal-Singer (GlaxoSmithKline, USA), J Vestbo (Co-chair, Denmark), J Yates (GlaxoSmithKline, USA).
Scientific Committee: A Agusti (Spain), P Calverley (UK), B Celli (USA), C Crim (GlaxoSmithKline, USA), A Lazaar (GlaxoSmithKline, US), W MacNee (Chair, UK), S Rennard (USA), R Tal-Singer (GlaxoSmithKline, USA), E Wouters (The Netherlands), J Yates (GlaxoSmithKline, USA).
REFERENCES
Footnotes
Funding: This work was funded by GlaxoSmithKline.
Competing interests: None.
Ethics approval: The studies were conducted in accordance with the Declaration of Helsinki and Good Clinical Practice Guidelines and were approved by relevant ethics and institutional review boards at the participating centres.