Article Text

Abstract
The treatment of benign broncho-oesophageal fistula is usually surgical but sometimes other methods of treatment are preferred. The case history is described of an adult in poor general condition in which an endoscopic approach combined with the use of fibrin glue on the bronchial side and metallic clips on the oesophageal side was used to close the fistula.
Statistics from Altmetric.com
Broncho-oesophageal fistulas (BEFs) are rare and their aetiology may be congenital or acquired. In adults BEFs are usually acquired as it is rare for a congenital BEF to go undetected until adulthood, and they can be the result of malignant or benign processes. The latter can be of traumatic, inflammatory, infective or iatrogenic origin.1 The non-specific nature of the presenting symptoms may delay a correct diagnosis, and patients are often first seen for pulmonary infections.1 Surgery is usually the preferred treatment but in some cases—for example, in patients in a poor clinical condition—other approaches have been described.
We present a case in which a double endoscopic approach with the combined use of glue and endoclips was used to close a BEF in an elderly woman in poor clinical condition.
CASE REPORT
An 89-year-old woman was admitted to our unit complaining of dysphagia, cough on liquid ingestion and anorexia. Five weeks earlier she had accidentally ingested a fishbone and during the following weeks she had lost 10 kg. She also suffered from ischaemic cardiomyopathy with an ejection fraction of 25%.
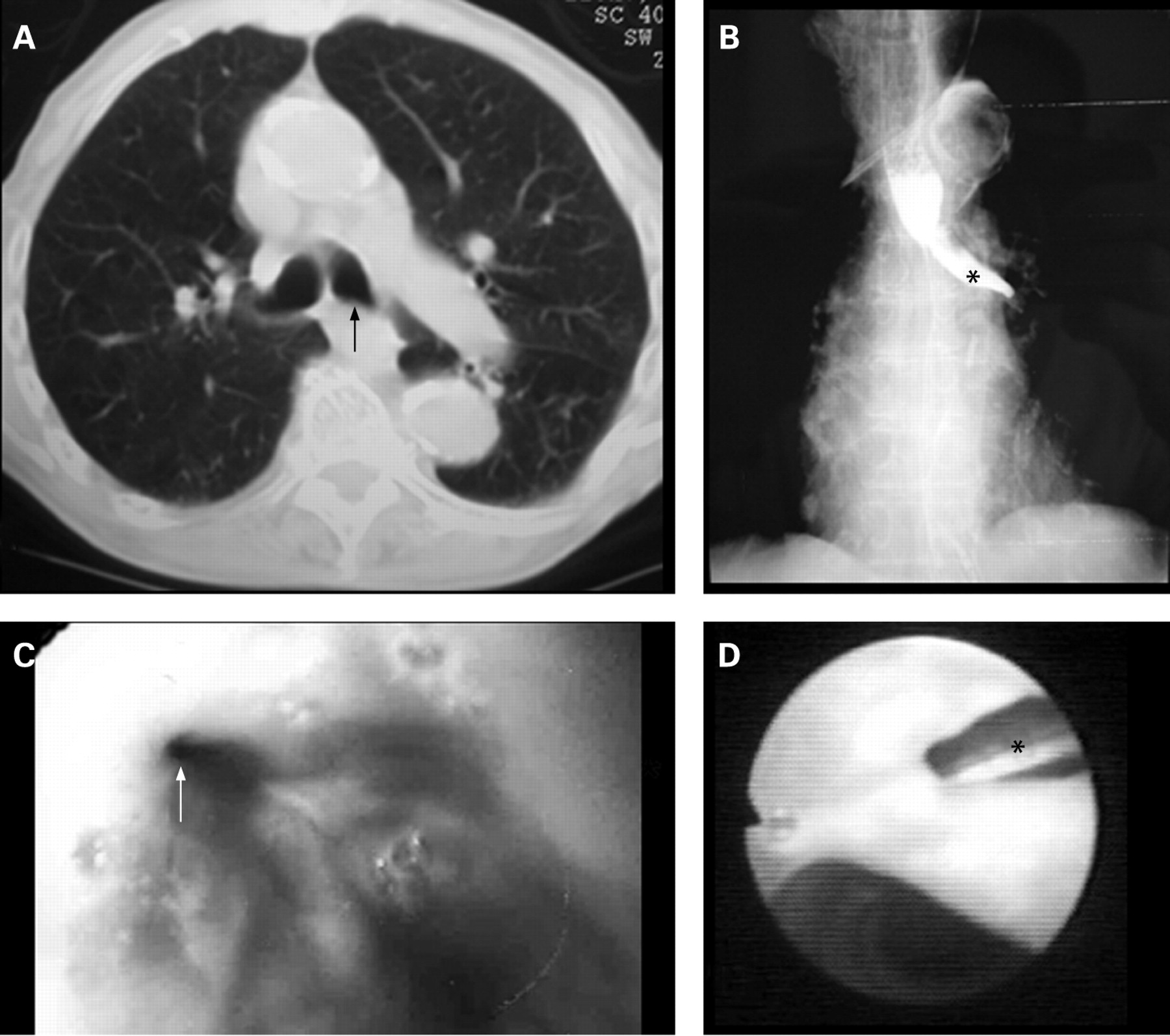
Her chest radiograph was unremarkable. A CT scan with contrast medium was suspicious of a BEF (fig 1A) which was confirmed by oesophagography with contrast medium (fig 1B). Endoscopic examination through the oesophagus and the bronchi further confirmed the diagnosis of BEF (fig 1C and D).

Because of the patient’s advanced age and poor cardiac and general condition, surgery was not deemed safe. With mild sedation, a flexible bronchoscope was introduced and positioned close to the fistula. A catheter was then advanced through the bronchoscope and positioned exactly on the fistula, the tip of the catheter exiting a few centimetres from the tip of the bronchoscope. Fibrin glue (Tissuecol, Baxter, Vienna, Austria) was applied through the catheter and the bronchoscope was slowly withdrawn without retreating the catheter in order not to occlude the instrument. An hourglass-shaped plug was formed, closing the fistula on the airway side. After 20 min, an oesophagoscope was introduced and the fibrin glue plug was clearly visible (fig 2A). Two nitinol metal clips (Boston Scientific, Natick, Massachusetts, USA) were applied on the oesophageal side of the fistula, tightly closing it. The patient was discharged home 10 days after the procedure. Bronchoscopic examination 1 month after treatment showed complete healing of the fistula (fig 2B), but the patient died 6 months later from congestive heart failure.

{kind=link}
{kind=link}
DISCUSSION
Benign BEFs are rare and, owing to the combination of their rarity and the non-specific nature of the symptoms, they can remain undiagnosed for a long time. The diagnosis may be made by endoscopic examination of the bronchi and oesophagus which may show a papilla or a dimple, or by oesophagography with dilute barium showing the contrast entering the bronchi.1 Sometimes, despite extensive investigation, the correct diagnosis is made only at surgery.
Although spontaneous healing of acquired BEF has been reported,2 the treatment of BEF is usually surgical and must be immediate in order to avoid complications and even fatal haemoptysis.1 Thoracotomy is the preferred surgical approach, with direct suturing or excision of the BEF, interposition of a pedicled flap and removal of damaged lung segments. In addition to surgery, other important steps include control of sepsis, establishment of a good nutritional status, pulmonary support and rehabilitation.1
In some patients and in particular circumstances, treatment other than by surgery has been described. The use of sodium hydroxide and acetic acid solution via the bronchoscope and the oesophagoscope has been reported.3 Application of fibrin glue, alone or with the combined use of a Vicryl mesh, has been shown to be very useful in closing BEF in particular patients. It has the advantage of solidifying slowly, thus allowing a more homogeneous spread over the lesion.4 5 The use of stents has been described in malignant lesions associated with stricture, and double stent insertion (ie, in the airway and in the oesophagus) has been reported as a superior option in closing such fistulas.6 The use of endoclips has been found useful either to anchor a stent or to directly close a fistula.7
Our fistula was quite large and we thought that the application of only fibrin glue could result in closure failure. We therefore adopted a double endoscopic approach with the application of fibrin glue on the airway side, which is our normal practice in closing respiratory fistulas, and endoclips on the digestive side. To our knowledge, there are no other reports describing the contemporaneous use of fibrin glue and metal clips in closing BEFs.
Footnotes
Competing interests: None.
Linked Articles
- Airwaves