Article Text

Abstract
Background: Respiratory muscle unloading during exercise could improve locomotor muscle oxygenation by increasing oxygen delivery (higher cardiac output and/or arterial oxygen content) in patients with chronic obstructive pulmonary disease (COPD).
Methods: Sixteen non-hypoxaemic men (forced expiratory volume in 1 s 42.2 (13.9)% predicted) undertook, on different days, two constant work rate (70–80% peak) exercise tests receiving proportional assisted ventilation (PAV) or sham ventilation. Relative changes (Δ%) in deoxyhaemoglobin (HHb), oxyhaemoglobin (O2Hb), tissue oxygenation index (TOI) and total haemoglobin (Hbtot) in the vastus lateralis muscle were measured by near-infrared spectroscopy. In order to estimate oxygen delivery (Do2est, l/min), cardiac output and oxygen saturation (Spo2) were continuously monitored by impedance cardiography and pulse oximetry, respectively.
Results: Exercise tolerance (Tlim) and oxygen uptake were increased with PAV compared with sham ventilation. In contrast, end-exercise blood lactate/Tlim and leg effort/Tlim ratios were lower with PAV (p<0.05). There were no between-treatment differences in cardiac output and Spo2 either at submaximal exercise or at Tlim (ie, Do2est remained unchanged with PAV; p>0.05). Leg muscle oxygenation, however, was significantly enhanced with PAV as the exercise-related decrease in Δ(O2Hb)% was lessened and TOI was improved; moreover, Δ(Hbtot)%, an index of local blood volume, was increased compared with sham ventilation (p<0.01).
Conclusions: Respiratory muscle unloading during high-intensity exercise can improve peripheral muscle oxygenation despite unaltered systemic Do2 in patients with advanced COPD. These findings might indicate that a fraction of the available cardiac output had been redirected from ventilatory to appendicular muscles as a consequence of respiratory muscle unloading.
Statistics from Altmetric.com
Pulmonary ventilatory adjustments, especially dynamic hyperinflation and its sensorial consequences, are centrally related to exercise impairment in patients with chronic obstructive pulmonary disease (COPD).1 More recently, however, much emphasis has also been placed on peripheral muscle abnormalities as adjunct mechanisms to constrain (or even limit) exercise tolerance in this patient population.2
A more fundamental approach to peripheral muscle dysfunction in patient populations, however, should also take into consideration the issue of local energy supply to the locomotor muscles. There are several lines of evidence suggesting that oxygen delivery to the working muscles may be critically impaired during dynamic exercise in patients with COPD.3–6 In this context, it is interesting to note that some interventions known to unload the respiratory muscles—such as pharmacological bronchodilation,7 heliox breathing3 4 and non-invasive positive pressure ventilation8 9—are associated with lower leg effort scores and/or reduced blood lactate levels. These findings might indicate that such interventions have improved the central haemodynamics to exercise and/or arterial oxygen content (Cao2) leading to enhanced oxygen delivery to the peripheral muscles. No previous study, however, has looked at the potential benefit of respiratory muscle unloading on peripheral oxygenation in patients with COPD.
The primary objective of this study was to investigate whether locomotor muscle oxygenation during exercise (as measured by near-infrared spectroscopy, NIRS)10 would be significantly improved by respiratory muscle unloading (via proportional assist ventilation, PAV)11 in patients with moderate to severe COPD. We also investigated whether this potential effect of respiratory muscle unloading would be associated with increased systemic oxygen delivery to the peripheral muscles (ie, higher cardiac output and/or improved Cao2).
METHODS
Subjects
The study population comprised 16 men with a clinical and functional diagnosis of COPD according to the Global Initiative for Obstructive Lung Disease criteria, presenting with a forced expiratory volume in 1 s/forced vital capacity (FEV1/FVC) ratio <0.7 and post-bronchodilator FEV1 <60% predicted.12 The patients were referred from the COPD outpatients clinic of our institution. Before entering the study they were required to be clinically stable for at least 3 months and optimised in terms of medical treatment. No patient had used oral steroids in the preceding 6 months. The patients were also required to present with a resting arterial oxygen tension (Pao2) of >8 kPa (60 mm Hg) at room air and no evidence of severe pulmonary hypertension (estimated systolic pulmonary arterial pressure <40 mm Hg) and/or relevant cardiac dysfunction (including ejection fraction <60%) as assessed by Doppler echocardiography. Patients gave written informed consent and the study protocol was approved by the medical ethics committee of the Federal University of São Paulo/São Paulo Hospital.
Study protocol
After a ramp incremental cardiopulmonary exercise test on a cycle ergometer, the patients performed, on a separate day, a high-intensity constant work rate (WR) trial test at 70–80% peak WR to individually select the flow and volume assist levels of proportional assisted ventilation (PAV). At subsequent experimental visits the patients undertook, on separate days, two post-bronchodilator constant WR tests at the previously defined WR to the limit of tolerance (Tlim). During these tests they were randomly assigned to receive sham ventilation or the preselected levels of PAV.
Non-invasive positive pressure ventilation
PAV was applied via a tight-fitting partial face mask with pressure levels being delivered by a mechanical ventilator (Evita-4, Draeger Medical, Lübeck, Germany). PAV provides ventilatory assistance in terms of flow assist (cm H2O/l/s) and volume assist (cm H2O/l) which can unload the resistive and elastic burdens, respectively.11 13 Volume assist was initially set by increasing the level of assist by 2 cm H2O/l until “run-away” was demonstrated; in this phase, flow assist was maintained at 1 cm H2O/l/s. Afterwards, flow assist was set by increasing its value by 1 cm H2O/l/s until “run-away” occurred with volume assist being kept fixed at 2 cm H2O/l. A fraction (80%) of these values was used initially with flow and volume assist settings adjusted for patient comfort to avoid “run-away” during exercise (see Results section for the actual values used during exercise).
Non-invasive sham ventilation was applied by the same equipment using the minimal inspiratory pressure support (5 cm H2O of inspiratory pressure support and 2 cm H2O of positive end-expiratory pressure) to overcome the resistance of the breathing circuit, as informed by the ventilator manufacturer. The patients and the accompanying physician were unaware of the ventilation strategy (PAV or sham) under use; this was accomplished by visually isolating the ventilator and its monitor from them.
Measurements
Pulmonary function
Post-bronchodilator spirometric tests were performed using the CPF System (Medical Graphics Corporation (MGC), St Pauls, Minnesota, USA). Carbon monoxide transfer factor (Tlco) was measured by the modified Krogh technique and the static lung volumes were obtained by body plethysmography (Elite System, MGC). Observed values were compared with Brazilian standards.14 15 Arterial oxygen and carbon dioxide tensions (Pao2 and Paco2) were determined in standard anaerobic conditions (mm Hg).
Cardiopulmonary exercise test (CPET)
Symptom-limited cycle ergometric CPET tests were performed using a computer-based exercise system (CardiO2 System, MGC). The following data were recorded as a mean of 15 s: oxygen uptake (V̇o2, ml/min), minute ventilation (V̇E, l/min), respiratory rate (RR, rpm) and tidal volume (VT, litres). Oxyhaemoglobin saturation (Spo2, %) was determined by pulse oximetry (POX 010-340, Mediaid, Torrance, California, USA) with its analogue signal being directed to the cardiopulmonary exercise system. From these data, the arterial oxygen content was estimated as Cao2est (ml%) = 1.39(Hb) × Spo2. Subjects were also asked to rate their “shortness of breath” at exercise cessation using a 0–10 Borg category ratio scale.
In the maximum progressive exercise test the rate of power increment was individually selected (usually 5–10 W/min) to provide an exercise duration of 8–12 min. Peak V̇o2 was the highest value found at exercise cessation: predicted values were those of Neder et al16 for the adult Brazilian population. The constant WR tests were performed at 70–80% of the previously determined peak WR to Tlim (min). Capillary samples were collected from the ear lobe for blood lactate measurements (mEq/l) at exercise cessation (Yellow Springs 2.700 STAT Plus, Yellow Springs Instruments, Ohio, USA).
Skeletal muscle oxygenation
Skeletal muscle oxygenation profiles of the left vastus lateralis muscle were evaluated with a commercially available near-infrared spectroscopy (NIRS) system (Hamamatsu NIRO 200, Hamamatsu Photonics KK, Japan). The theory of NIRS has been described in detail elsewhere.10 17 Briefly, one fibreoptic bundle carries the NIR light produced by the laser diodes to the tissue of interest while a second fibreoptic bundle returns the transmitted light from the tissue to a photon detector in the spectrometer. The intensity of incident and transmitted light is recorded continuously and, together with the relevant specific extinction coefficients, used for online estimation and display of the changes from the resting baseline of the concentrations of oxyhaemoglobin ([O2Hb]), deoxyhaemoglobin ([HHb]) and total haemoglobin ([Hbtot]). The last variable has been used as an index of local blood volume as [Hbtot] = [O2Hb] + [HHb]. From these values an additional index of muscle oxygenation was calculated (tissue oxygenation index (TOI) = 100 × ([O2Hb]/[Hbtot]).10 16 17 The values were recorded as a change (Δ) from baseline in units of μM/cm. In order to reduce intrasubject variability and improve intersubject comparability, Δ[O2Hb] and Δ[HHb] values were expressed as the percentage of the maximal value determined on a post-exercise maximal voluntary contraction (MVC) or on early recovery (Δ [Hbtot]).18 Additional methodological considerations of this technique can be found in the online supplement.
Central haemodynamics
Cardiac output (l/min) and stroke volume (l) were measured non-invasively throughout the constant WR tests using an impedance cardiography device (PhysioFlow PF-05, Manatec Biomedical, France). These data were also used to estimate oxygen delivery (Do2est = cardiac output × Cao2est, l/min). The PhysioFlow device and its methodology have been thoroughly described elsewhere.19 Before each exercise test the system was autocalibrated taking into consideration age, stature, body mass and blood pressure values: verification of the correct signal quality was performed by visualising the ECG tracing and its first derivative (dECG/dt) and the impedance waveform (ΔZ) with its first derivative (dZ/dt).20 Additional methodological considerations of this technique can also be found in the online supplement.
Statistical analysis
SPSS Version 13.0 statistical software was used for data analysis. The results are presented as mean (SD) or median (range) for symptom scores. In order to contrast within-subject exercise responses, paired t or Wilcoxon tests were used as appropriate. Time course values during the submaximal exercise tests were expressed as a percentage of isotime, defined as the shorter test between the two experimental conditions in a given subject. Repeated measures analysis of variance (ANOVA) was used to compare the cardiovascular and leg oxygenation variables throughout exercise at quartiles of isotime. The level of statistical significance was set at p<0.05 for all tests.
RESULTS
Population characteristics
Patients had moderate to severe airflow obstruction with increased static lung volumes and moderate reductions in Tlco. Seven patients were classified as GOLD stage 2 and the remaining patients were classified as GOLD stages 3–4.12 All patients presented with reduced maximal exercise capacity (peak V̇o2 below the lower limit of normality).16 Pulmonary ventilatory limitation, at least as suggested by increased V̇Emax/MVV ratio (>0.8), was found in all subjects. Eight patients had mild exercise-related oxyhaemoglobin desaturation (peak Spo2 ranging from 89% to 86%). Breathlessness and leg effort were similarly described as the exercise limiting symptoms. A detailed description of the main resting and exercise characteristics is given in the online supplement.
Effects of PAV metabolic, ventilatory and perceptual responses
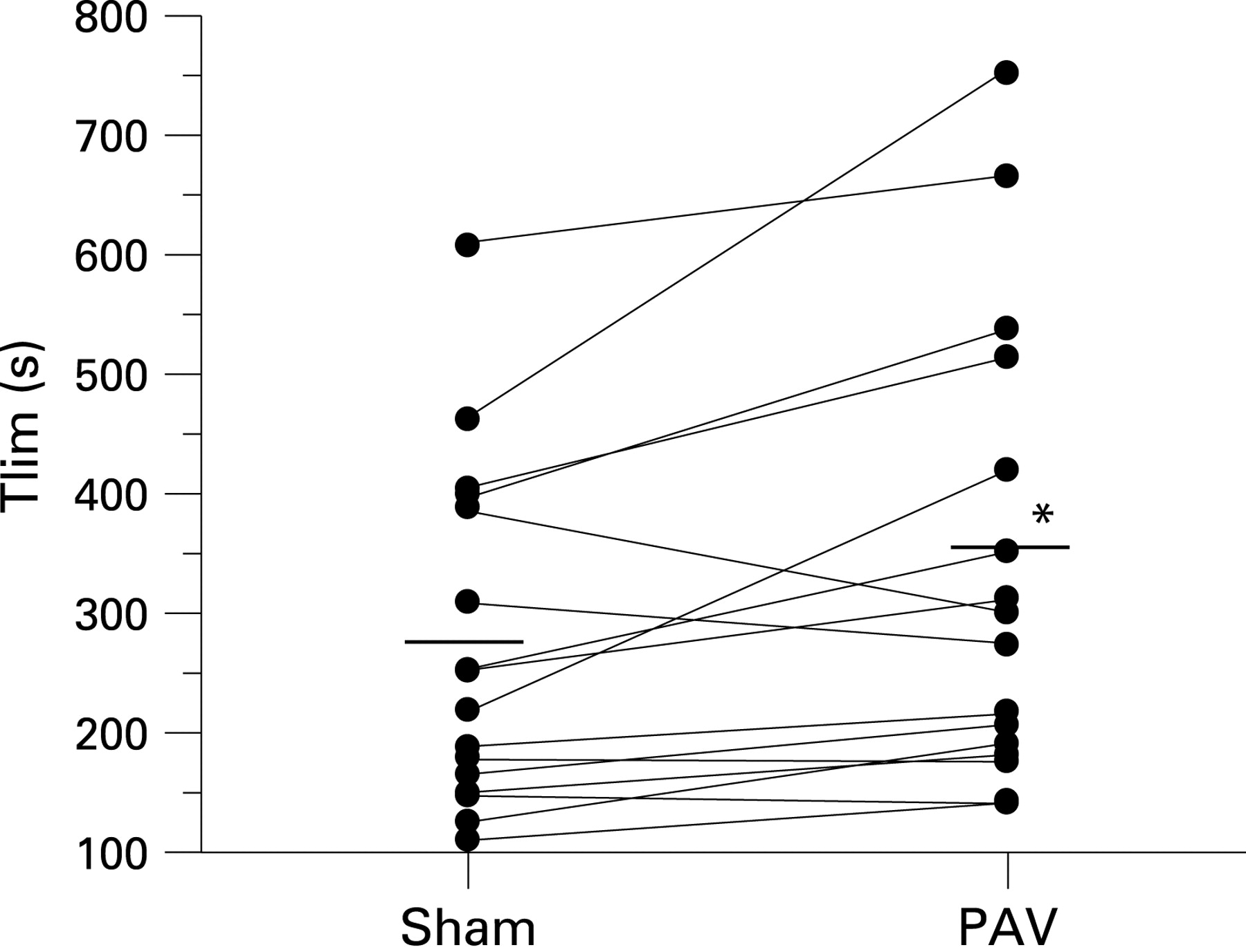
All patients successfully tolerated the two non-invasive ventilation modes during exercise. The actual values for volume assist and flow assist during PAV were 5.8 (0.9) cm H2O/l and 3.5 (0.8) cm H2O/l/s, respectively. PAV was associated with a significant increase in exercise tolerance compared with sham ventilation: 337 (189) s vs 273 (142) s (p = 0.01). In fact, Tlim improved in 13/16 patients with PAV compared with sham ventilation (fig 1). The reasons for stopping exercise were similar with PAV and sham ventilation (sham ventilation: dyspnoea (n = 6), leg fatigue (n = 8), both (n = 2); PAV: dyspnoea (n = 8), leg fatigue (n = 6), both (n = 2)).

As shown in table 1, V̇o2 was significantly increased at isotime and Tlim with PAV. In contrast, V̇E values were increased only with PAV at Tlim. There were, however, no significant differences in breathing pattern between the two interventions. In addition, leg effort and breathlessness at isotime and corrected for Tlim were significantly reduced with PAV compared with sham ventilation (table 1).
Systemic oxygen delivery and muscle oxygenation
There were no significant effects of PAV on the cardiovascular responses compared with sham. As shown in table 2, stroke volume and cardiac output did not differ between the interventions at isotime and at Tlim. Similar to the maximal exercise test, only eight patients had mild changes in Spo2 (exercise–rest = −4% to 3%). There was also no significant change in Spo2 with PAV compared with sham ventilation (table 2): median (range) intrasubject difference in Spo2 between the two interventions throughout exercise was 0% (−2% to 2%). Consequently, estimated systemic oxygen delivery (Do2est = cardiac output × Cao2est) remained unchanged with PAV at isotime and Tlim (table 2): median (range) intrasubject difference in Do2est between the two interventions was 0.12 l/min (−0.20 to 0.18).
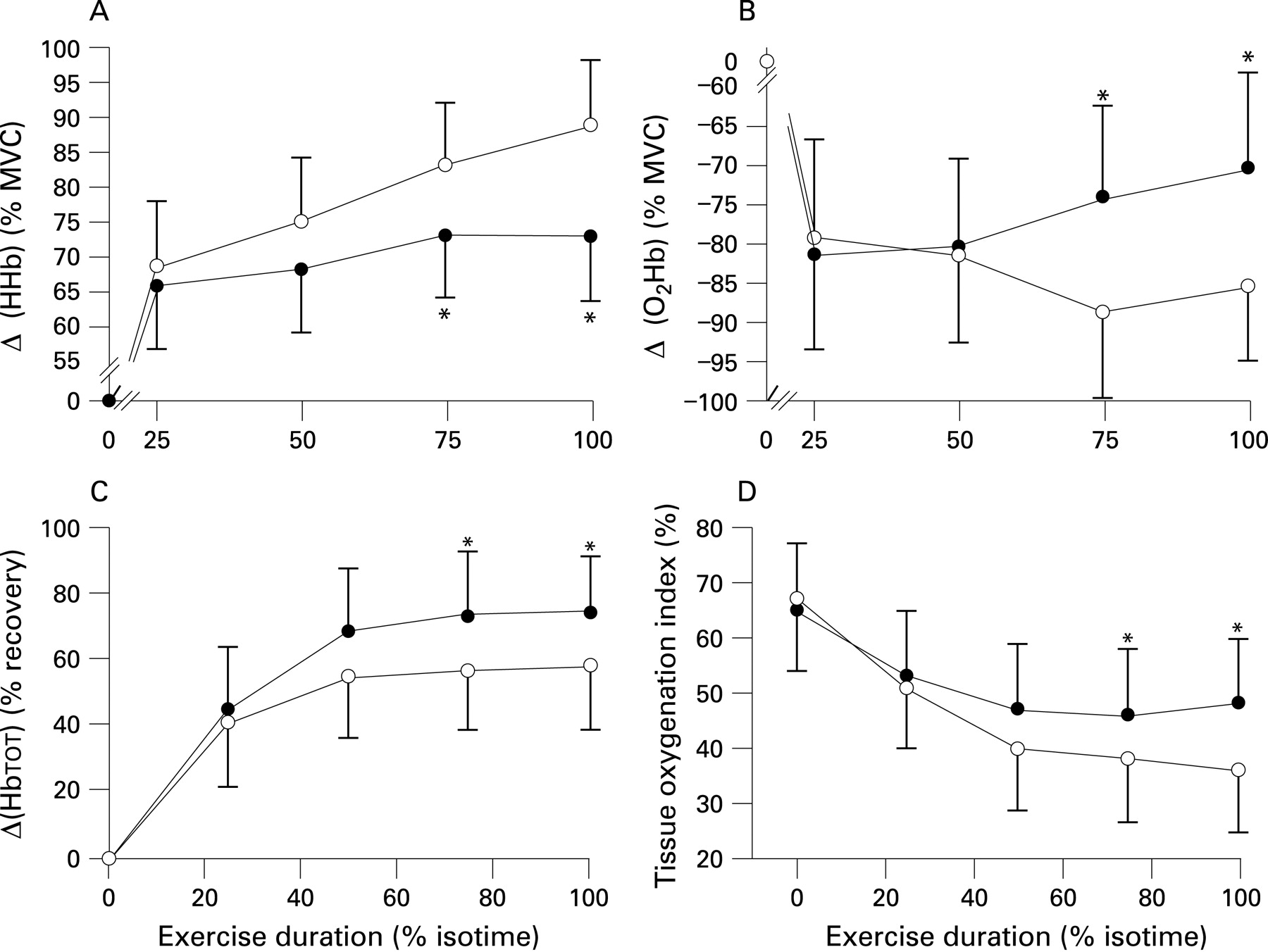
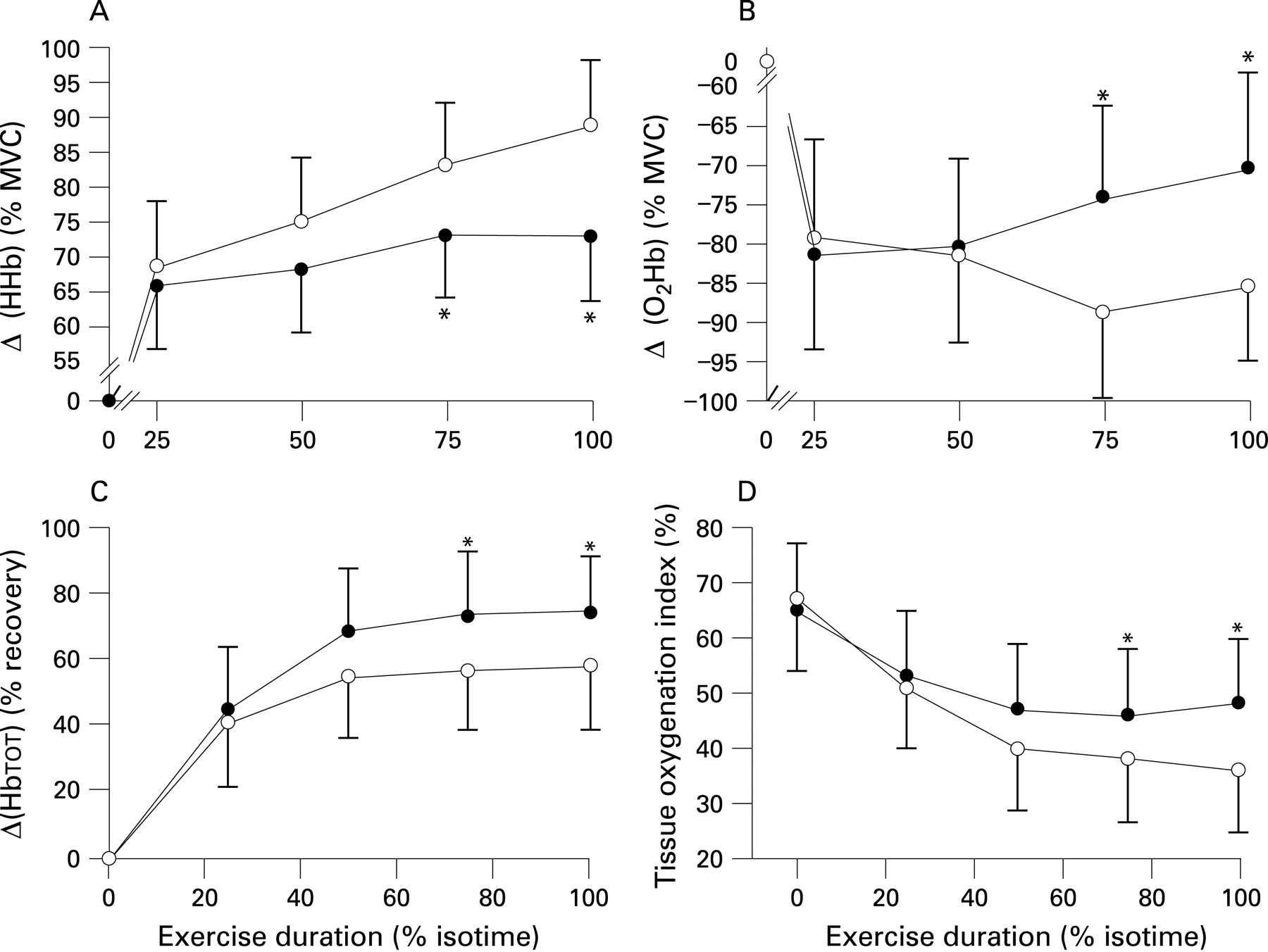
In relation to muscle oxygenation by NIRS, PAV was associated with lower Δ[HHb] at 75% isotime, isotime and at Tlim. These changes were accompanied by a significant reduction in the exercise-related decrease in Δ[O2Hb] (table 2 and figs 2A and 2B, respectively). Consequently, TOI was improved with PAV at these time points (fig 2C). Moreover, Δ[Hbtot], an index of local blood volume, was also significantly increased with PAV (fig 2D). Consistent with these data, lactate values corrected for Tlim were reduced with PAV compared with sham ventilation (table 2).
{kind=link}
{kind=link}
DISCUSSION
This study shows that respiratory muscle unloading during exercise (PAV) can improve leg muscle oxygenation (Δ[O2Hb] and TOI) and local blood volume (Δ[Hbtot]) in patients with moderate to severe COPD. These findings, however, were not related to enhanced systemic Do2 (cardiac output × Cao2) to the working muscles. Alternatively, they might indicate that respiratory muscle unloading diminished the blood flow requirements of the respiratory muscles with a consequent redistribution of the available cardiac output from ventilatory to locomotor muscles. From a clinical perspective, our data indicate that strategies aimed at reducing the work of breathing during exercise may present with beneficial effects on energy supply to the peripheral muscles in this patient population.
Methodological considerations
We used PAV in order to unload the respiratory muscles during exercise.11 13 Previous studies have found that PAV was superior to other non-invasive strategies in reducing inspiratory muscle work in patients with COPD. In addition, it was found to be better tolerated by these patients, allowing them to exercise for longer and at significantly higher intensities.9 21 22 Unfortunately, however, we were unable to measure the work of breathing directly as small air leaks have profound effects on the levels of assistance by PAV. An oesophageal balloon therefore could not be placed as PAV had to be delivered through a tight-fitting facial mask by the system used in the present study.
We used NIRS to follow the muscle oxygenation patterns continuously during exercise.10 17 Although this technique is not able to differentiate between the signal attenuation due to haemoglobin and myoglobin, this confounding factor has been estimated as 10% of the whole haemoglobin signal,10 a non-critical issue in this within-subject study. In order to improve signal stability and reproducibility we incorporated a number of technical details including the correction of the observed values to maximum values found on post-exercise MVC or recovery. In addition, the changes found with PAV were well above the intrasubject coefficient of variation (CV) for the responses in each subject.
Similar considerations might be applied to cardiac output estimation by impedance cardiography as the system was highly stable during exercise in these patients. However, because of the controversies on the absolute accuracy of this methodology in patient populations,23 24 we first ensured that the system was responsive to small changes in the metabolic demand and the observed values were commensurate with the expected values from the submaximal relationship between the change in cardiac output and the change in V̇o2 (see online supplement).4 25 In addition, the stroke volume signal remained stable even when dynamic lung hyperinflation was induced in a subgroup of patients (see online supplement).
Energy supply to the locomotor muscles in COPD
It is widely recognised that skeletal muscle oxygenation depends on the dynamic balance between oxygen delivery and utilisation.10 In the present study PAV was associated with a blunted decrease in exercise Δ[O2Hb]% with a consequent improvement in TOI. In addition, Δ[HbTOT]%, an index of local muscle blood volume,26 was increased with PAV. As a corollary, leg effort- and Tlim-corrected blood lactate levels were diminished with PAV (tables 1 and 2). Moreover, total body V̇o2 was higher after respiratory muscle unloading (table 1). This finding seems to indicate that peripheral muscle oxygen consumption had been limited by supply before respiratory unloading in these patients, and this more than counterbalanced the potential reductions in respiratory muscle V̇o2 with PAV. Contrary to our hypothesis, however, these effects were not associated with discernible changes in systemic Do2est (table 2). Consequently, the enhancement in leg muscle oxygenation during PAV was not secondary to improved intrapulmonary gas exchange and/or enhanced central haemodynamic adjustments to exercise. These findings imply that an alternative mechanism should be sought to explain the improvement in leg oxygen supply with PAV in these patients.
In this context, it is conceivable that peripheral muscle oxygenation has been improved as a consequence of blood flow redistribution from the respiratory to the appendicular muscles. In other words, respiratory muscle unloading might have reduced the blood flow requirements of the ventilatory muscles with a resultant improvement in appendicular muscle perfusion.6 In fact, the increased work of the respiratory muscles during exercise may require up to 50% of the oxygen uptake of the body,27 28 and it is plausible that a fraction of the cardiac output can be diverted from the locomotor muscles to supply the increased energy demands of the ventilatory pump.3–6 In normal subjects a series of elegant experiments have shown that a respiratory muscle fatigue-induced metaboreflex could increase sympathetic vasoconstrictor outflow, reducing the perfusion of locomotor muscles during exercise (ie, a blood flow “stealing” effect).29–31 The “stealing” hypothesis is therefore an attractive explanation for our findings: improvement in the intradiaphragmatic milieu with respiratory muscle unloading may have mitigated the noxious metabolic influences leading to a lower leg sympathetic outflow and improved muscle blood flow. The “stealing” hypothesis, however, still awaits additional experimental evidence in these patients, probably by directly measuring the dynamics of diaphragm blood flow during exercise in COPD.32
Clinical implications
We found that a strategy targeted at reducing the work of breathing and dyspnoea was effective in improving the oxygenation status of the leg muscles. These results therefore emphasise the multifactorial nature of exercise impairment in patients with COPD and provide a rationale for the improvement in leg fatigability with selected interventions which primarily act on the respiratory system. For instance, Peters et al7 recently reported that the combination of bronchodilators and oxygen was superior to each one in isolation in reducing leg effort scores during exercise in normoxic patients with COPD. Other studies with heliox breathing and non-invasive positive pressure ventilation also found that these interventions were associated with improved Do2 to the working muscles and lower submaximal lactate values.3 4 8 9 Future clinical trials of the impact of interventions on the mechanical ventilatory responses should look more carefully at the relevance of improved peripheral muscle performance in increasing exercise tolerance in this patient population.
Study limitations
This study has some limitations which are inherent to its non-invasive nature. Although we indirectly estimated local muscle blood volume from the NIRS data, this technique is more sensitive than arterial femoral and whole limb plethysmographic estimates to follow subtle intramuscular changes in perfusion.33 An intra-arterial catheter was not inserted in our patients and Cao2 was estimated from continuous Spo2 readings. We believe that this provided an acceptable surrogate of the true Cao2 in our non-hypoxaemic patients. We also could not perform inspiratory capacity manoeuvres to estimate the operating lung volumes during exercise with PAV as the sudden increase in ventilation triggers the ventilator to provide additional volume assist. In practice, this is associated with pronounced over-assist, air leaks and acute maladaptation of non-invasive ventilation. Our results should not therefore be extrapolated to more hyperinflated patients than those evaluated in the present study, although the higher oxygen cost of breathing may indicate that the “stealing” phenomenon can also operate in that specific subpopulation. It should also be recognised that it is still unclear whether respiratory muscle unloading would improve peripheral muscle oxygenation during moderate exercise where the ventilatory demands are considerably lower.
In conclusion, respiratory muscle unloading by PAV was associated with increased peripheral muscle oxygenation under stable systemic oxygen delivery during high-intensity constant work rate exercise in patients with moderate to severe COPD. These findings might indicate that a fraction of the available cardiac output had been redirected from ventilatory to appendicular muscles as a consequence of respiratory muscle unloading.
Acknowledgments
The authors thank all colleagues from the Pulmonary Function and Clinical Exercise Physiology Unit (Division of Respiratory Diseases, Department of Medicine, Federal University of Sao Paulo (UNIFESP), Brazil) for their collaboration; Mrs Laura D Batista for her technical support; Mrs Dircilene P Moreira for competent secretarial assistance; and the patients for their effort and enthusiastic cooperation throughout the study.
REFERENCES
Supplementary materials
web only appendices 63/10/910
Files in this Data Supplement:
Footnotes
Funding: Supported by a research grant from Fundação de Amparo à Pesquisa do Estado de São Paulo, São Paulo, Brazil (FAPESP) No 05/00722-0. AB-S is a recipient of a Post-Doctoral Scholarship Grant from FAPESP. JAN is an Established Investigator (level II) of the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Brazil.
Competing interests: None.
Ethics approval: Patients gave written informed consent and the study protocol was approved by the medical ethics committee of the Federal University of São Paulo/São Paulo Hospital.