Article Text

Abstract
Background: Forced expiratory volume in 6 s (FEV6) has been proposed as a more easily measurable parameter than forced vital capacity (FVC) to diagnose airway disease using spirometry. A study was undertaken to estimate FEV6 repeatability, to identify correlates of a good quality FEV6 measurement and of volumetric differences between FEV6 and FVC in elderly patients.
Methods: 1531 subjects aged 65–100 years enrolled in the SA.R.A project (a cross-sectional multicentre non-interventional study) were examined. FEV6 was measured on volume-time curves that achieved satisfactory start-of-test and end-of-test criteria. Correlates of FEV6 achievement were assessed by logistic regression.
Results: Valid FEV6 and FVC measurements were obtained in 82.9% and 56.9%, respectively, of spirometric tests with an acceptable start-of-test criterion. Female sex, older age, lower educational level, depression, cognitive impairment and lung restriction independently affected the achievement of FEV6 measurement. Good repeatability (difference between the best two values <150 ml) was found in 91.9% of tests for FEV6 and in 86% for FVC; the corresponding figures in patients with airway obstruction were 94% and 78.4%. Both FEV6 and FVC repeatability were affected by male sex and lower education. Male sex, airway obstruction and smoking habit were independently associated with greater volumetric differences between FEV6 and FVC.
Conclusions: In elderly patients, FEV6 measurements are more easily achievable and more reproducible than FVC although 1/6 patients in this population were unable to achieve them.
Statistics from Altmetric.com
Spirometry is the most frequently performed respiratory function test and has a primary diagnostic role in the elderly since many factors (co-morbidity, blunted sensitivity to dyspnoea, polypharmacy) variously confound or conceal the clinical expression of respiratory disorders in this age group.1 2 However, performing a reliable spirometric test involves strict patient cooperation to satisfy current guidelines for acceptability and repeatability.3 A vigorous physical effort and, occasionally, the prolongation of expiration for up to 20 s are needed to obtain complete lung emptying to measure forced vital capacity (FVC). Unfortunately, elderly subjects or patients with severe respiratory diseases quite frequently cannot make such an effort.4 5 For this reason, there is an increasing interest in more easily measurable spirometric parameters that could replace FVC in the elderly. Among these, forced expiratory volume in 6 s (FEV6) has been shown to be able to predict lung function decline in adult smokers6 and to be a reliable surrogate for FVC in the spirometric diagnosis of airway obstruction and restriction.7–12 Reference equations and lower limits of normality for FEV6 and for FEV1/FEV6 have recently been produced in selected populations.13–16 However, to date no study has focused on the factors related to a good quality FEV6 and to the correlates of volumetric differences between FEV6 and FVC in elderly patients.
We analysed the spirometric findings obtained in the Italian multicentre SAlute Respiratoria nell’Anziano, Respiratory Health in the Elderly (SA.R.A) study to identify factors that influence the achievement of an acceptable FEV6 measurement and to assess FEV6 repeatability. We also attempted to quantify the differences between the best FEV6 and FVC, as well as between the best FEV1/FEV6 and FEV1/FVC, and to search for inherent explanatory factors.
METHODS
Analysed data were derived from a sample of 1971 subjects aged 65–100 years enrolled in the SA.R.A. multicentre case-control study. Details on the recruitment criteria, studied population and diagnostic procedures are available elsewhere.1 Spirometric tests were not performed in 101 subjects because of early interruption of expiration, physical impairment, inability to understand the instructions, lack of collaboration and refusal; 1870 spirometric measurements were therefore obtained and retained for analysis. Briefly, the sample included 1054 subjects (56.4%) with normal spirometric parameters (429 healthy and 625 with non-respiratory diseases), 509 subjects (27.2%) with an obstructive pattern and 307 (16.4%) with a restrictive pattern (for criteria see below).
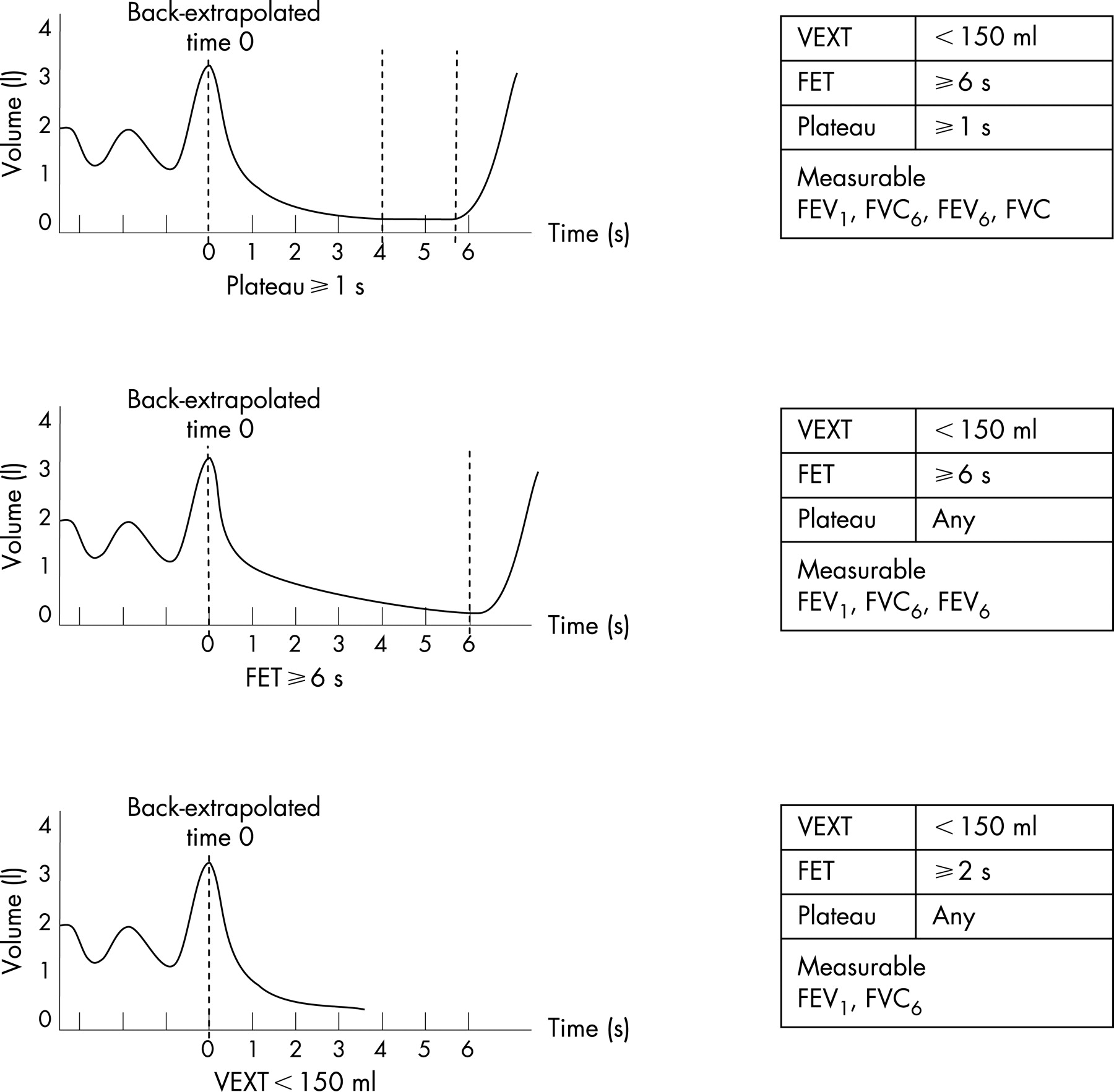
Spirometric tests were performed according to the guidelines of the American Thoracic Society (ATS).17 A rigorous quality control programme was implemented throughout the study; the results have been published elsewhere.1 Spirometric flow-volume curves were considered acceptable if they had extrapolated volume (VEXT) <5% of the FVC or 0.150 l (start-of-test criterion) and a forced expiratory time (FET) ⩾6 s or an obvious plateau in the volume-time curve (end-of-test criterion) in the absence of cough, glottis closure or other significant interruptions of the manoeuvre. In accordance with the recommendations of the ATS,17 we did not exclude curves which did not satisfy the repeatability criteria in order to avoid the exclusion of data in which an abnormal lung function causes a greater coefficient of variation than in normal subjects. There are different proposed surrogate measures of FVC such as FVC6 (maximum volume exhaled at any time during the first 6 s)13 or FEV6 (volume forcefully exhaled at exactly 6 s after back-extrapolated time 0). We chose the latter because it is the measure proposed by the ATS and the European Respiratory Society (ERS)3 and has been shown to be a reliable surrogate of the FVC.7–12 Figure 1 shows examples of valid sessions for the measurement of FVC6, FEV6 and FVC. FEV1 and FEV6 were measured on all acceptable curves. FVC was measured only on curves with an end-expiratory plateau ⩾1 s, ie, an end expiratory phase ⩾1 s with a volume change lower than the minimal detectable volume of 0.026 litres.18

We defined airways obstruction as FEV1/FVC below the lower limit of normal (LLN: mean − 1.645*SD) of the SA.R.A. study reference population19 and restriction as FVC below LLN with normal or increased FEV1/FVC.18 Severity of airways obstruction was evaluated on the basis of FEV1 expressed as % predicted3: mild (⩾70%), moderate (60–69%), moderately severe (50–59%), severe (35–49%), very severe (<35%) (fig 2).

The following data that might affect the quality of measurements were collected: sociodemographic characteristics (sex, age, instruction level), smoking habit, spirometric index of airway obstruction (FEV1 and FVC % predicted), anthropometric characteristics (body mass index (BMI), waist/hip ratio, occiput wall distance), mood state (15-item Geriatric Depression Scale (GDS)20), cognitive function (Mini Mental State Examination (MMSE)21) and physical performance (Barthel’s index,22 6 min walking test (6MWT)23).
FEV6 and FVC repeatability were estimated by calculating the difference between the two highest values of the index obtained from each subject. A few subjects with a difference >1000 ml were considered outliers and not included in the analysis (N = 10 for FEV6 and N = 18 for FVC). Repeatability was also expressed using mean differences and 95% agreement limits according to the method of Bland and Altman.24 The analysis of intraindividual FEV6 repeatability was carried out in subjects with at least two valid FEV6 measurements (VEXT <150 ml and FET ⩾6 s; n = 1345). FEV6 repeatability was compared with the repeatability of FVC calculated in a subset of 1135 subjects with two or more valid FVC measurements (VEXT <150 ml and plateau ⩾1 s).
Analysis of data
Differences between groups were analysed using Pearson χ2 for dichotomous variables and the Student t test or Mann-Whitney test for continuous variables, as appropriate. Multivariable logistic analysis or linear regression was used for the identification of independent correlates of outcomes. Variables entered in the models were chosen on the basis of univariable analysis results. Independent variables were considered statistically significant if the odds ratio (OR) was different from 1 and if the 95% confidence interval (CI) did not include 1.
All the analyses were performed using Epi Info (CDC, Atlanta, Georgia, USA and WHO, Geneva, Switzerland) and Stata (Stata Corporation, College Station, Texas, USA) software packages.
RESULTS
FEV6 achievement
Among the 1870 subjects who performed spirometry, 1531 (81.9%) obtained VEXT <150 ml in at least three curves and 1485 (79.4%) obtained FET ⩾6 s in at least three curves. Among the 1531 subjects with VEXT <150 ml in at least three curves, 1269 (82.9%) obtained FET of ⩾6 s in at least three curves and 871 (56.9%) attained a plateau of end expiration ⩾1 s in at least three curves (fig 3).

The main demographic and clinical characteristics of the 1531 subjects with a positive start-of-test criterion are shown in table 1. Most of the subjects had a lower educational level and were former or current smokers. Nutritional status (as reflected by BMI) was, on average, good. Mood depression, corresponding to a GDS score >5, was found in 20% of men and 36.5% of women, while cognitive impairment affected about one participant out of seven.
The mean FEV1% was 86.5% (5th and 95th percentiles 37.3% and 126.6%, respectively), while the mean FEV1/FVC% was 64.2% for men (5th and 95th percentiles 34.6% and 89.1%, respectively) and 74.4% for women (5th and 95th percentiles 52.9% and 89.1%, respectively). Most of the patients with airways obstruction were men, and obstruction was severe or very severe in over 40% of them.
Table 2 compares the characteristics of people who could or could not achieve a valid FEV6 measurement. Older people and those with a lower educational level, a restrictive respiratory pattern and physical or neuropsychological impairment were less likely to achieve a valid FEV6. According to results from a multivariable logistic model, female sex, older age, lower educational level, depression, cognitive impairment and restrictive spirometric pattern were all independently and negatively correlated with the achievement of a valid FEV6 measurement (table 3).
Intraindividual FEV6 and FVC repeatability
The mean (SD) difference between the two best values of FEV6 was 62 (84) ml (coefficients of variation 1.35%). The number of spirometric measurements with a difference between the two best values of FEV6 <150 ml was 1236 (91.9%). In the subset of subjects who had two or more measurable FVC values, the mean (SD) difference between the two best values was 72 (87) ml (coefficients of variation 1.21%), while the number of spirometric measurements with a difference between the two best values of FVC <150 ml were 976 (86% of the total). The repeatability of FEV6 was high even in subjects with airway obstruction (<150 ml in 94% of tests), whereas the repeatability of FVC in the same group was lower (78.4%). Table 4 shows the mean differences between the two best FEV6 and FVC measurements, together with 95% agreement limits and centile distribution stratified by gender.
Several factors were associated with poor FEV6 repeatability in the univariable analyses (table 5). Only male sex (OR 1.04; 95% CI 1.11 to 2.68) and lower educational level (OR 1.76; 95% CI 1.08 to 2.85) remained associated with lack of repeatability of FEV6 in a multivariable model corrected for age, cognitive function, Barthel index and 6 MWT.
Differences between the largest FVC and FEV6, between FEV1/FEV6 and FEV1/FVC, and correlates of differences
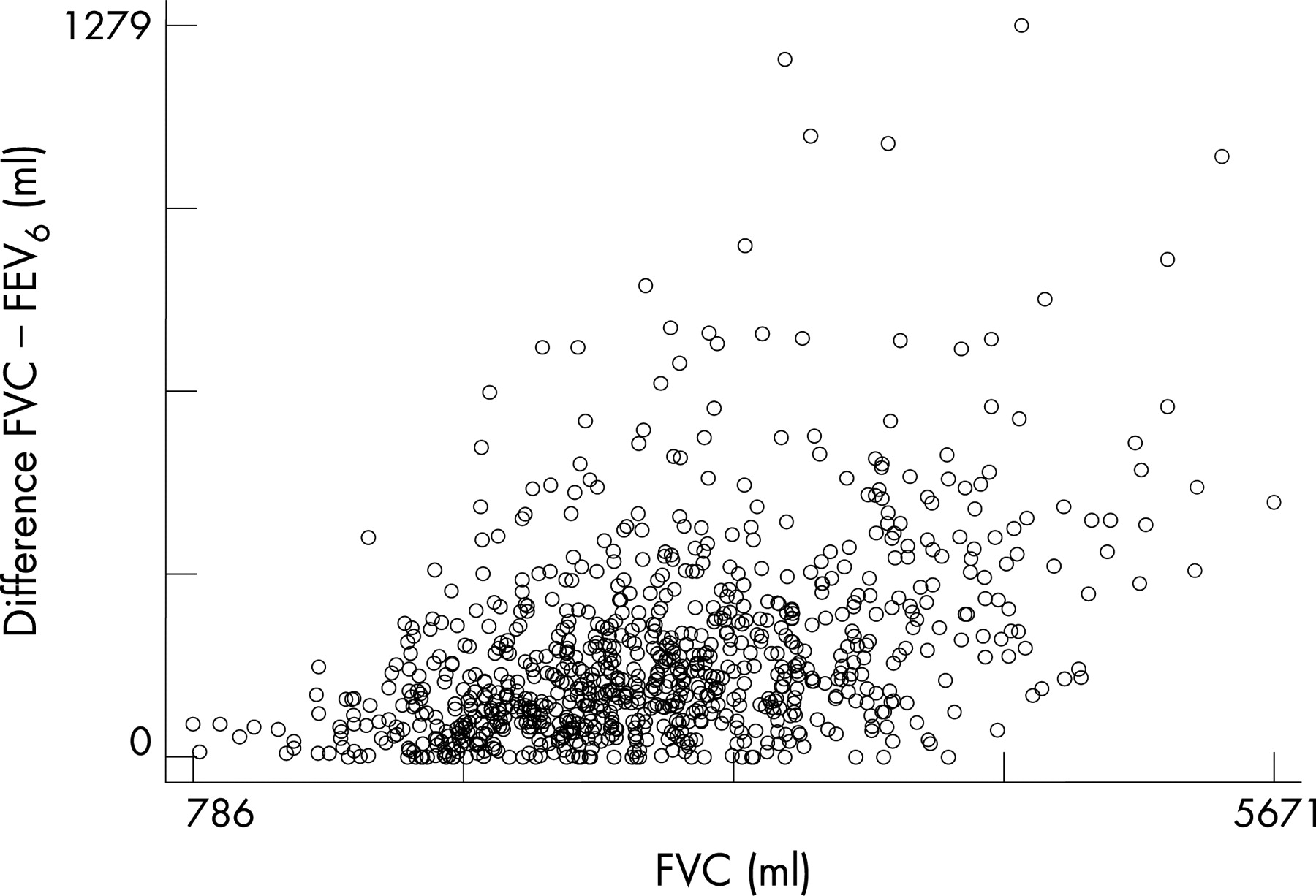
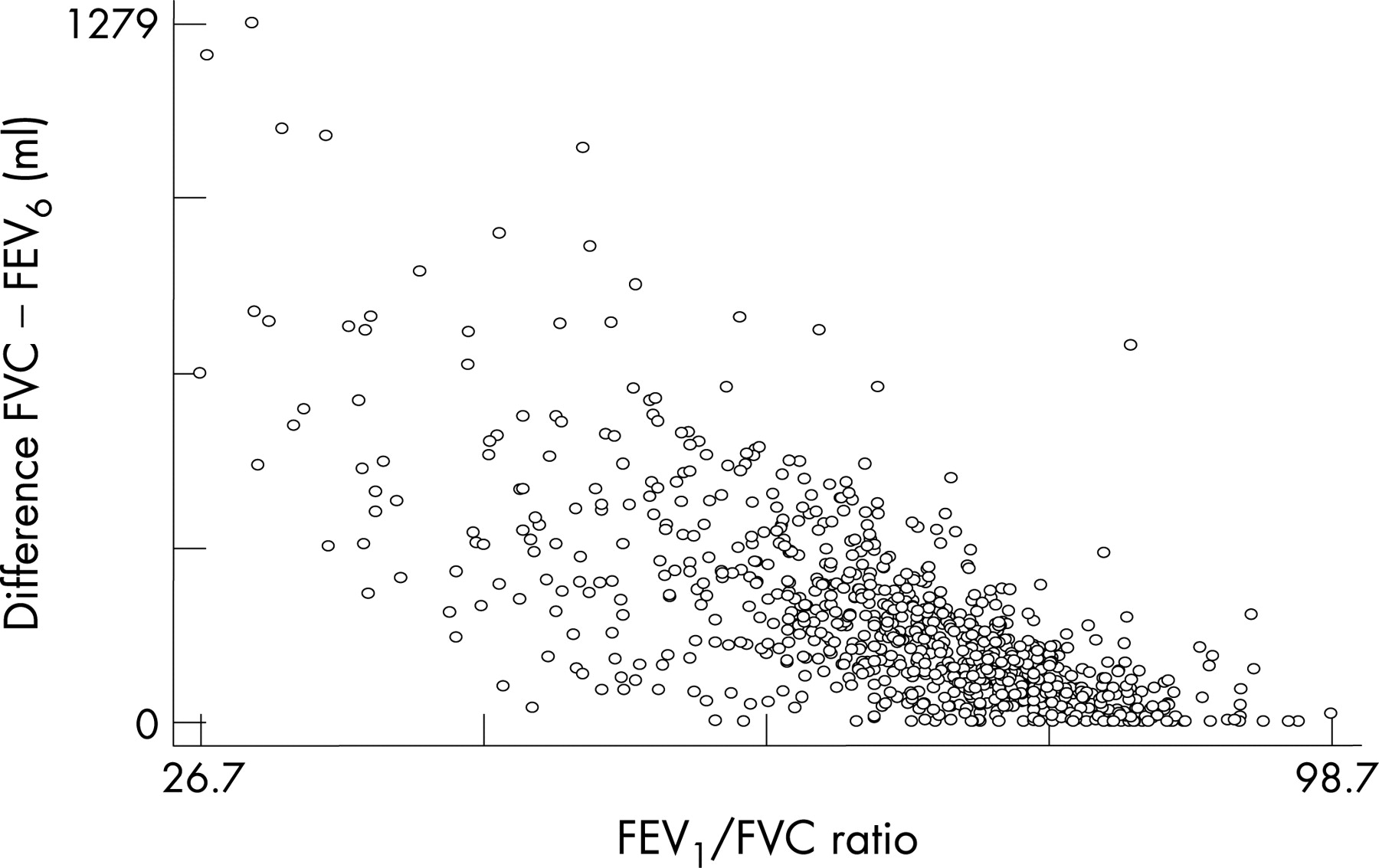
Among the 871 spirometric measurements with three acceptable curves and a plateau of ⩾1 s in at least three curves, the mean (SD) difference between FVC and FEV6 was 182 (171) ml (range 0–1279). The mean (SD) difference between FEV1/FEV6 and FEV1/FVC was 4.14 (3.10)% (range 0–17%). As expected, the difference between FVC and FEV6 increased as the absolute values of FVC increased (fig 4). In a linear multivariable regression, male sex, airway obstruction and smoking habit emerged as independent correlates of a larger difference between FVC and FEV6 and between the best FEV1/FEV6 and FEV1/FVC (p<0.001). The difference between FVC and FEV6 was 0 in 23 subjects but exceeded 1000 ml in 5 subjects, all characterised by severe obstruction (mean (SD) FEV1/FVC 35.2 (9.0)%). The positive relationship between the difference FVC-FEV6 and the degree of airway obstruction was confirmed by the significant correlation shown in fig 5.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
The findings of our study indicate that, in elderly subjects, FEV6 measurements are more easily achieved and are more reproducible than FVC. The potential implication of this result is evident, since FEV6 was obtained in more than 80% of spirometric measurements with acceptable start-of-test criteria whereas a reliable FVC measurement was obtained in <60% of tests.
To our knowledge, this is the first study to address the factors that influence the achievement and repeatability of FEV6 measurements in the elderly. Factors that negatively affected attainment of an expiration of at least 6 s, which is the only end-of-test requirement for FEV6, were female sex, older age, lower educational level, depression, cognitive impairment and a restrictive spirometric pattern. The mechanism by which age affects the achievement of FEV6 is unclear. In older subjects, airway closure occurs at lung volumes above functional residual capacity, impairing the FEV6 manoeuvre. In fact, some studies have shown that the decline in lung function accelerates with age.25–29 Our results support this explanation: among people aged 77 years or older (corresponding to the 75th percentile of age distribution), 75% of participants achieved an acceptable FEV6 compared with 83% in the entire sample (data not shown). However, since even the most accurate multivariable analysis could miss important explanatory variables, older age might also be considered a “summary index” of conditions hampering the achievement of FEV6.
The cooperation of the patient is an essential requirement for a reliable test: cognitive impairment is a well recognised negative correlate for achieving FEV6.1 30–32 Conversely, depressed mood has not previously been recognised as a negative correlate for achieving any spirometric measure. Lack of motivation to perform the spirometric manoeuvre might underlie the negative relationship between depression and achievement of FEV6. The fact that less educated subjects achieved a satisfactory FEV6 measurement less frequently than more educated subjects probably reflects education-related differences in the ability to understand and perform the spirometric manoeuvre.
Patients with a restrictive functional pattern had difficulties in performing a measurable FEV6 manoeuvre; in 64/272 the FVC manoeuvre lasted <6 s. It is conceivable that patients with a restrictive pattern have less air to expire and therefore need less time to do it. Furthermore, restrictive lung diseases are frequently associated with increased lung stiffness which could make the expiration explosive and therefore shorter. Our sample included only patients with a mild to moderate restrictive respiratory pattern, and it is conceivable that a greater proportion of patients will not achieve a FET ⩾6 s and a measurable FEV6 in samples including severely restricted patients. Our findings are indirectly supported by the observation of Vanderwoorde et al8 that FEV6 had lower sensitivity for a diagnosis of a restrictive pattern than for a diagnosis of an obstructive pattern.
Women achieved FEV6 less frequently than men. This could be explained by the fact that women tend to have lower levels of FVC than age-matched men. Smaller lungs could complete emptying in <6 s more easily, and therefore women are more likely to achieve an adequate plateau, thus allowing FVC to be measured, even if the manoeuvre is interrupted before the FEV6 can be measured. In the SA.R.A. population, 24.2% of women with FET <6 s had a plateau compared with 9.1% of men (p<0.001). Our results therefore indicate that FEV6 might not be a suitable surrogate for FVC in elderly women and in people with a restrictive pattern. A possible solution to the problem could be to re-define FEV6 as the largest volume exhaled anytime during the first 6 s (ie, FVC6 referred to above13). This could be obtained in a larger number of subjects, including mainly women and patients with spirometric restriction.
Our results confirm the findings of Swanney et al7 that FEV6 measurement was more reproducible than FVC. The repeatability of both FEV6 and FVC were affected by male sex and lower education. Since men have larger lung volumes than women, and because FEV6 is obviously less than FVC, it seems logical that FVC and FEV6 should have different criteria for reproducibility and these should also be gender-specific. To express reproducibility as a percentage of the best value instead of using the cut-off point of 150 ml could be a possible solution.
In our study the mean difference between the best FEV6 and FVC was 182 ml, while Demir et al33 reported a mean (SD) difference of 95 (121) ml in 5114 adult patients of mean (SD) age 49.95 (15.48) years and Enright et al6 found that, on average, the FEV6 was 112 ml smaller than the FVC in adult smokers. A potential reason for this discrepancy could be our decision to calculate FVC only when a 1 s plateau was reached, thus excluding curves in which FVC could be underestimated because of an early interruption of expiration. The possibility that the observed differences could be linked to different male/female ratios between study samples can also be excluded: indeed, the proportion of women in our sample was 53.7% compared with 53.6% in the study by Demir et al. In the sample studied by Enright et al, only 37.5% were women; however, given that the difference between FVC and FEV6 is higher in men, the greater fraction of men in the sample studied by Enright et al would be expected to increase rather than to decrease such difference.
On the other hand, the severity of airway obstruction was directly related to the difference between FVC and FEV6. The expiration time is, on average, proportional to the severity of airway obstruction and, thus, the proportion of FVC expired in the first 6 s is expected to decrease in parallel with FEV1. Interestingly, all subjects having a difference between FVC and FEV6 of more than 1 litre were among those with the most severe obstruction. Demir et al33 also found a greater difference between FVC and FEV6 in patients with airway obstruction. Similarly, Enright et al6 found that the difference between the two spirometric indices was, on average, 6–9% larger in smokers with more severe airway obstruction. In comparison with previous studies6 33 our sample consisted of subjects with less severe airway obstruction (mean FEV1 86.5%), whereas Demir et al reported a mean FEV1 of 72.9 (24.4)% predicted and in the study by Enright et al the mean (SD) FEV1 was 74.8 (9.5)% predicted in men and 74.9 (9.3)% predicted in women. Our study therefore emphasises the inverse relationship between FEV1% predicted and the difference between FVC and FEV6 by confirming it in a population with less severe airway obstruction.
We found that, in addition to airway obstruction, male sex and smoking habit were positive correlates of the difference between FVC and FEV6. The greater lung volumes and the resulting expiration times in men and the risk of airway disease in smokers are possible explanations for these findings.
This study has some limitations. First, we defined restriction according to spirometric evidence, but only the measurement of total lung capacity can provide a definitive diagnosis.34 However, this limitation would have a greater effect on a study assessing the diagnostic accuracy of FEV6 than on our study which aimed to identify factors associated with achieving a satisfactory measurement of FEV6. Second, in our study FVC was considered reliable only if the subject reached a plateau ⩾1 s. This criterion is very restrictive and excludes the operator’s option considered a possible alternative by the ATS/ERS statements.3 At any rate, it seems an acceptable choice for the sake of standardisation since, in a multicentre study, it would not have been possible to evaluate the subjective terms of judgement adopted by individual operators. Third, we cannot exclude the possibility that, in selected cases, we might have observed glottis closure and not a true plateau. Finally, a high proportion of our patients with chronic obstructive pulmonary disease had severe or very severe obstruction (over 40% of them had FEV1 <50% predicted). As suggested elsewhere,18 35 36 we identified airways obstruction using the LLN of FEV1/FVC of our reference population of elderly people,19 which was lower than the classic 70%, thus reducing the proportion of people with mild obstruction.
In conclusion, FEV6 can be a valid alternative to FVC in the identification of airway obstruction in elderly patients because the spirometric manoeuvre is easy to perform and it satisfies the criteria for repeatability and diagnostic accuracy. However, very old poorly educated and cognitively impaired subjects, women and patients with a restrictive respiratory pattern have more difficulty in achieving a satisfactory FEV6. The measurement of FEV6 therefore represents an important step forward with regard to FVC, although it may not be the ideal surrogate for FVC in subjects who are very old and frail.
REFERENCES
Footnotes
SA.R.A. Study Group: Coordinators: V Bellia (Palermo), F Rengo (Napoli). Scientific Committee Members: R Antonelli Incalzi (Taranto), V Grassi (Brescia), S Maggi (Padua), G Masotti (Florence), G Melillo (Naples), D Olivieri (Parma), M Palleschi (Rome), R Pistelli (Rome), M Trabucchi (Rome), S Zuccaro (Rome). Participating centres, principal investigator and associated investigators (in brackets): (1) Div. Medicina I, Osp. Geriatrici INRCA, Ancona; D L Consales (D Lo Nardo, P Paggi). (2) Div. Geriatria, Osp. Civile, Asti; F Goria (P Fea, G Iraldi, R Corradi). (3) Catt. Geront. e Geriatria, Policlinico Universitario, Bari; A Capurso (R Flora, S Torres, G Venezia, M Mesto). (4) V Div. Geriatria, Osp. Malpighi, Bologna; S Semeraro (L Bellotti, A Tansella). (5) I Div. Med. Generale, Osp. Civile, Brescia; V Grassi (S Cossi, G Guerini, C Fantoni, M De Martinis, L Pini). (6) Clinica Pneumologica, Fondazione ‘E. Maugeri’, Telese (BN); G Melillo (R Battiloro, C Gaudiosi, S De Angelis). (7) Ist. Med. Int. e Geriatria, Osp. Cannizzaro, Catania; L Motta (I Alessandria, S Savia). (8) Ist. Geront. e Geriat., Osp. Ponte Nuovo, Univ. Florence; G Masotti (M Chiarlone, S Zacchei). (9) Div. Geriatria, Osp. Morgagni, Forli; V Pedone (D Angelini, D Cilla). (10) Div. Geriatria, Osp. Galliera, Genova; E Palummeri (M Agretti, P Costelli, D Torriglia). (11) G.ppo Ricerca Geriatrica, Osp. Richiedei, Gussago (BS); M Trabucchi (P Barbisoni, F Guerini, P Ranieri). (12) Div. Geriatria, Osp. Generale, L’Aquila; F Caione (D Caione, M La Chiara). (13) I Div. Geriatria, Osp. San Gerardo, Monza; G Galetti (A Cantatore, D Casarotti, G Anni). (14) Catt. Gerontologia e Geriatria, Univ. Federico II, Napoli; F Rengo (F Cacciatore, A I Pisacreta, C Calabrese). (15) Ist. Med. Int., Osp. Geriatrico, Padova; G Enzi (P Dalla Montè, S Peruzza, P Albanese, F Tiozzo). (16) Ist. Mal. App. Resp., Osp. Rasori, Parma; D Olivieri (V Bocchino, A Comel, N Barbarito). (17) Ist. Geront. e Geriatria, Policlin. Monteluce, Perugia; U Senin (F Arnone, L Camilli, S Peretti). (18) Div. Geriatria, Osp. Israelitico, Roma; S M Zuccaro (M Marchetti, L Palleschi). (19) Div. Geriatria, Osp. Gen. Addolorata, Roma; M Palleschi (C Cieri, F Vetta). (20) Ist. Med. Int. e Geriatria, Polic. Gemelli, Roma; P U Carbonin (F Pagano, P Ranieri). (21) Ist. Sem. Med. e Geriatria, Pol. Le Scotte, Siena; S Forconi (G Abate, G Marotta, E Pagni). (22) Fond. San Raffaele, Cittadella della Caritè, Taranto; R Antonelli-Incalzi (C Imperiale, C Spada). (23) Catt. Geront. e Geriatria, Osp. Maggiore, Milano; C Vergani (G Giardini, M C Sandrini, I Dallera). (24) Catt. Mal. App. Resp., Osp. V. Cervello, Palermo; V Bellia (F Catalano, N Scichilone, S Battaglia). Coordinating Centre: Istituto di Medicina Generale e Pneumologia, Catt. Mal. App. Respiratorio, Universitè degli Studi di Palermo.
Funding: Supported by research funds of DIMPEFINU, Universitè di Palermo
Competing interests: None.