Article Text

Statistics from Altmetric.com
Oxygen therapy in COPD
DEVELOPMENT OF THE BRITISH THORACIC SOCIETY HOME OXYGEN DATABASE AND PREVALENCE OF HOME OXYGEN USE IN ENGLAND AND WALES
G. C. Donaldson1, G. Edmonds2, I. Balfour-Lynn3, P. Calverley4, R. Garrod5, M. Morgan6, J. A. Wedzicha1. 1University College London; 2City University; 3Royal Brompton Hospital; 4University of Liverpool; 5Kingston University and St George’s Hospital; 6University Hospitals of Leicester, UK
Introduction: A new service for the supply of oxygen therapy to patients at home started on 1 February 2006. Patients in England and Wales are supplied by four companies (Air Products, Allied Respiratory, BOC and Linde). These companies have agreed to provide anonymised data on patients to the BTS Home Oxygen database committee.
Methods: Data on patients with active orders in June 2007 were supplied. Patient’s service category data were excellent with only 33 missing records, and of these 27 had data on modality of supply, hours of use and litres of oxygen prescribed. Similarly, only 866 postcodes were possibly erroneous as they were unlinkable to the Office of National Statistics Postcode Directory File for February 2007. Another well-completed data field from the HOOF forms was date of birth; only 1045 records were missing and 118 obviously erroneous. NHS numbers were missing for 8107 records and another 8732 were not 10 characters in length. For three contractors, clinical diagnosis codes were present in only 29% of records. The number of patients in age groups 0, 1–4, 5–9, 10–14, etc and 85+ plus were counted after eliminating possible duplication of patients and linked to the most recent (2005) quinary mid-year residential populations estimates from the Office of National Statistics website (http://www.statistics.gov.uk).

Results: There were 76 753 home oxygen users, 3136 (4.1%) were paediatric patients aged below 17 years. The commonest age for home oxygen was 77 years (range 0–107). Prevalence fell from 0.73 per 1000 in the under 1 years to 0.58 per 1000 in the 1–4 year olds and remained constant at about 0.11–0.12 per 1000 until at about 45 years, when prevalence started to rise to a peak of 8.8 per 1000 in the 80–84 and 85+ age groups.
Conclusions: The BTS Home Oxygen database has been established and preliminary analysis shows adequate data collection. We have been able to establish for the first time the prevalence of Home Oxygen use in England and Wales. Prescribers are encouraged to carefully complete the clinical diagnosis information in question 14 of the HOOF form.
Funding: Funded by the Department of Health.
DO CURRENT BTS GUIDELINES FOR AIR TRAVEL CORRECTLY IDENTIFY PEOPLE WITH THORACIC SCOLIOSIS WHO BECOME HYPOXAEMIC (PAO2 <6.6 KPA) ON HYPOXIC CHALLENGE TESTING?
D. Bandyopdhyay, T. Quinnell, J. M. Shneerson, I. E. Smith. The Respiratory Support and Sleep Centre, Papworth Hospital, UK
Introduction: The BTS guidelines for flight assessment, largely based on evidence from people with COPD, recommend: no additional oxygen for air travel if the resting oxygen saturation (SpO2) is >95% and hypoxic challenge testing (HCT) for people with an additional risk factor, if the SpO2 is between 92–95%. In the summary for primary care, a walking distance of greater than 50 m without distress is suggested as reassuring and can obviate the need for an HCT. There are only anecdotal data relating to spinal deformity. We assessed these recommendations in people with primary, thoracic scoliosis.
Methods: People with thoracic scoliosis of varying severity were recruited to the study. Resting SpO2 and arterial blood gases (ABGs) breathing room air, spirometry and shuttle walking test distance (SWT) were measured. All subjects underwent an HCT breathing an FiO2 of 15% for 15 minutes, or until SpO2 fell below 85%, when ABGs were taken.
Results: Values are reported as means (SD) unless otherwise stated. Twenty people (11 female) with thoracic scoliosis aged 65 (9.9) years, were studied. The Cobb angle was 89 (31.4)°. Thirteen were on home nocturnal non-invasive ventilation (NIV), none used additional oxygen. The mean FEV1 and vital capacity were 0.8 (0.39) and 1.14 (0.42) l respectively, SpO2 was 93 (2.6) %, PaO2 9 (1.1) kPa and PaCO2 6.1 (0.44) kPa. The SWT distance was 262 (121) m. HCT was positive in 14 subjects (PaO2 <6.6 kPa), negative in 2 (PaO2 >7.4 kPa) and 4 had intermediate results. The walking distance bore no relation to the HCT result, all walked over 80 m. Eight of the 14 subjects with a positive HCT had a resting SpO2 greater than 95%. The use of home NIV did not predict the HCT outcome.
Conclusions: Despite a normal daytime SpO2 and fair exercise tolerance subjects with thoracic scoliosis may desaturate profoundly on an HCT. The current BTS guidance for air travel does not identify these people, who are at risk of severe hypoxaemia. There should be a low threshold for performing HCTs on people with scoliosis before giving them advice on air travel.
AN AUDIT OF OXYGEN USE IN EMERGENCY AMBULANCES AND IN A HOSPITAL EMERGENCY DEPARTMENT
K. E. Hale, B. R. O’Driscoll. Salford Royal Foundation Trust, UK
Background: Oxygen use in emergency medicine is important but poorly studied. It is not known how many patients receive oxygen in emergency ambulances or in emergency departments (EDs) in the UK. Patients with COPD are especially vulnerable to inappropriate oxygen therapy.
Methods: An audit proforma was used in the “majors” sector of a university hospital ED to look at use of oxygen in ambulances and in the ED. 1022 patients were studied in May and June 2007.
Results: (1) 921 patients (90% of all patients) had SpO2 recorded in the ambulance. (2) 159 patients (17%) had saturation <94% at some time in the ambulance. (3) 62 patients (7%) had an oxygen saturation <90% at any time, including 14 COPD patients. (4) 48 of 878 non-COPD patients (5%) had saturation <90% at any time. (5) 34% of patients arriving in the ED majors section had received oxygen in the ambulance. Of this group, almost half had oxygen therapy discontinued in the ED. (A further 3% of patients received Entonox, a mixture of oxygen and nitrous oxide). (6) Only 5% of patients had oxygen started de novo in the ED. (7) 62% of oxygen use in ambulances was in line with JRCALC guidance (Joint Royal Colleges Ambulance Liaison Committee). Most of the “breaches” involved the use of medium dose oxygen for non-hypoxic patients where current JRCALC guidelines specify high dose oxygen. (8) Of 43 patients with a diagnosis of COPD, only 58% were correctly identified in the ambulance. (9) 60% of COPD patients had saturation below 94% at some time and 33% fell below 90%. (10) All COPD patients who received oxygen were treated with simple face masks. 8% had an oxygen flow of 2 l/min (about 28% oxygen), 19% had 4 l/min (35–40%) and 73% had >4 l/min (>40% oxygen). The simple face mask is not designed for use at flow rates below 5 l/min because of the risk of re-breathing and increased resistance to inspiration. Therefore none of the COPD patients received appropriate oxygen therapy.
Conclusions: Oxygen is widely used in emergency ambulances in Salford. (34% of patients would translate to about 2 million episodes of emergency oxygen use in UK ambulances each year). About 33% of COPD patients and 5% of non-COPD patients had clinically significant hypoxaemia (saturation below 90% at any time). 42% of patients with COPD were not categorised as having COPD during ambulance transfers and most of those with recognised COPD were given more than 28% oxygen. The BTS has commissioned a national guideline for emergency oxygen use which will be published in late 2007.
RESPIRATORY ASSESSMENT CENTRE: A NOVEL WAY TO HANDLE RESPIRATORY EMERGENCIES IN A LARGE TEACHING HOSPITAL
C. J. Warburton, L. Davies, S. Agarwal, R. Angus, T. Jagoe. Aintree Chest Centre, UK
During the winter pressure period of 2006/7 the Aintree Chest Centre piloted a novel Respiratory Assessment Centre (RAC). This comprised a 14 bedded acute assessment area alongside the general MAU. The RAC was staffed from 09:00 to 17:00 seven days a week by two F2/ST1s, a respiratory specialist registrar and a consultant physician (for a month at a time in rotation). Respiratory nurse specialists also covered the unit on a rotational basis. Patients with respiratory conditions from the acute medical take were seen and assessed first by the RAC team who undertook two ward rounds per day and thence either discharged or admitted. A management plan was instituted wherever the patient was subsequently admitted.
Over the first four months a mean of 111 patients was assessed each week in the RAC, with a discharge rate of 31%. The number of COPD patients using our community based “hospital at home” team increased by 80% (mean 25 to 45 per month) from the comparable period in 2006. Overall, average length of stay for COPD fell from mean (SD) 7.9 (9.6), median 6 days to 7.0 (8.13), median 4 days (data from 2005/6 and 2006/7) The average length of stay on the chest wards fell for one ward area (36 beds) and remained static for the others (total 55 beds). Despite our best efforts only 70% of patients seen in the RAC had respiratory conditions, the remainder having general medical conditions. Patients in the general MAU with respiratory conditions were also seen by the RAC senior staff upon request.
We feel that the RAC improved the quality of care given to patients with respiratory disease within our Trust. Measures of service activity and outcomes also appear favourable. A critical mass both of respiratory admissions and respiratory physicians is required for this pattern of working; however by rotating this work between all respiratory physicians, career progression issues are avoided. The RAC model appears to be a viable way to deliver very early specialist input for patients presenting with respiratory disease to large hospital Trusts and offers advantages over the traditional MAU model.
SHOULD ALL CHRONIC OBSTRUCTIVE PULMONARY DISEASE PATIENTS WITH CARDIAC COMORBIDITIES HAVE AMBULATORY OXYGEN ASSESSMENT?
E. Tabiowo, L. Kemp, K. Morgan, J. Edge, V. Clarke, R. K. Kedia. Mid-Cheshire Hospital NHS Trust, UK
Introduction: Ambulatory oxygen refers to the provision of oxygen therapy during exercise and while performing activities of daily living. Current BTS guidelines on oxygen assessment indicate that ambulatory oxygen therapy is not recommended in patients with chronic lung disease and mild hypoxaemia (not on long-term oxygen therapy (LTOT)), no exercise-induced desaturation (EID) and patients with chronic heart failure.
Design and Objective: We carried out a prospective, observational study to assess the effect on ambulatory oxygen assessment and outcome in patients with COPD and cardiac comorbidities.
Material and Method: Thirty three COPD patients, who attended the oxygen assessment clinic at Mid-Cheshire Health Trust between February 2006 to October 2006, were included in the study. All patients had their spirometry measured, baseline arterial blood gas measurement, six-minute walk test (6MWT), and further LTOT assessment where necessary. Patients were divided into mild (FEV1 50–80%), moderate (FEV1 30–49%) and severe (FEV1 <30%) COPD based on the NICE criteria using the FEV1 predicted percentages. EID was deemed significant if there was a greater than 4% drop in oxygen saturation from baseline to a value level below 90%, in line with the BTS guidelines.
Results: Thirty three COPD patients assessed during the periods of February and October 2006 were included. 9 patients had mild COPD, 16 patients had moderate COPD, and 8 patients had severe COPD. On ambulatory oxygen: 4 (44.4%), 6 (37.5%) and 5 (62.5%) patients demonstrated significant EID in mild, moderate and severe group respectively. Further analysis of the mild group showed that 3 out of 4 (70%) patients who desaturated also had associated congestive cardiac failure (CCF) and/or ischaemic heart disease (IHD) as comorbidities. This is compared to 1 out of 5 (20%) patients who did not desaturate in the mild group. The mean PaO2 in the mild COPD subgroup was 8.03 kPa, with 2 of the 9 patients (22.2%) having a PaO2 less than 7.3 kPa (thereby meeting the LTOT criteria). Mortality during the follow-up period was 22.2% (2 patients) in the mild group and 6.3% (1 patient) in the moderate group. No deaths were recorded in the severe group during this period. Both deaths in the mild COPD group were in patients who also suffered from CCF. The only death in the moderate group was a patient who suffered from lung cancer.
Conclusions: This observational study shows that patients with mild COPD and cardiac comorbidities, can show significant levels of EID on ambulatory oxygen assessment, regardless of their PaO2. Hence, despite minimal airflow limitation, the presence of cardiac co-morbidities such as CCF necessitates the need for ambulatory oxygen assessment that can be beneficial to this patient group. We recommend that all patients with COPD with cardiac co-morbidities should be assessed with 6MWT for EID. In patients with EID, we recommend that further assessment for pulmonary hypertension with echocardiography be carried out, in addition to the prescription of ambulatory oxygen therapy.
AUDIT REVIEWING THE IMPACT OF LUNG ALERT CARDS AND AMBULANCE CREW EDUCATION ON INAPPROPRIATE OXYGEN PRESCRIBING IN PATIENTS WITH COPD
A. L. Kerry1, C. Lobo1, S. Milanes1, J. Curtis1, N. A. Maskell1. 1North Bristol Lung Unit, Southmead Hospital; 2Hawkes Bay Hospital
Background: Some COPD patients are sensitive to rises in inspired oxygen concentrations which may lead to CO2 retention and acute type 2 respiratory failure (T2RF). The JRCALC/ASA Ambulance Services Guidelines recommend that “known T2RF patients should be encouraged to carry some form of identification to aid in their care”. Due to the perception that high numbers of COPD patients were being admitted to hospital having had inappropriate oxygen administration, it was decided to audit this before and after the introduction of patient held “Lung Alert Cards” and education of the local Ambulance Service in oxygen administration in COPD.
Method: We identified patients admitted over two three-month periods January–March in 2005 and 2006 with a diagnosis of exacerbation of COPD on discharge or death and randomly selected 100 of these admissions and pulled the notes. Data were then extracted from the notes. We assessed oxygen administration by ambulance crew, incidence of acute T2RF, use of non-invasive ventilation (NIV) on arrival to hospital and length of stay (LOS).
Notes were available for review in 73/100 episodes (see table). The incidence of acute T2RF on admission fell from 31% in 2005 to 17% in 2006. The need for NIV in the first 24 h of admission also fell from 27% in 2005 to 14% in 2006. LOS was also one day less in 2006 compared to 2005.
Conclusion: The strategies employed to reduce oxygen toxicity in COPD patients coming to hospital—Lung Alert Cards and ambulance crew education—were associated with a reduction in the amount of inappropriate oxygen administration in ambulances, a fall in the incidence of type 2 respiratory failure and a reduction in need for NIV.
ASSESSMENT FOR AMBULATORY OXYGEN REQUIREMENT IN PATIENTS WITH COPD USING THE 6-MINUTE WALK TEST
L. A. E. Brown, P. J. Ryan. Hereford County Hospital, UK
Background: Six-minute walk tests (6MWT) are commonly used to assess the need for ambulatory oxygen for patients with COPD. It is not clear which parameters should be measured during a 6MWT and which are the most important for assessing the need for ambulatory oxygen. We retrospectively analysed 67 6MWTs in patients with COPD.
Methods: All patients attending our respiratory physiology department for 6MWTs between 2002 and 2006 were identified from the filed assessment forms. Patients had been referred for ambulatory oxygen assessment either directly from the chest clinic or as part of an assessment following admission for an acute exacerbation of COPD. The diagnosis of COPD was made by the respiratory team and confirmed with spirometry. All patients underwent the same protocol of unblinded 6MWT in air, followed by 10 min rest, and then a repeat test while wearing nasal oxygen delivered at 2 l/min. Resting oxygen saturation, minimum oxygen saturation during exercise, recovery time (return to resting oxygen saturation), exercise distance and Borg score were recorded both on and off oxygen. Oxygen saturation was measured using a Pulseox-7 pulse oximeter. All patients had spirometry but only some had transfer factor measured.
Results: Of the 67 patients 35 (52%) were male. The mean age was 70.6 years (SD = 10.4 years). The mean FEV1 was 0.84 l/m (SE 0.05) and mean % predicted FEV1 was 37.9 l/m (SE 2.2). The mean FVC was 2.0 l/m (SE 0.08) and mean % predicted FVC was 67.6 (SE 2.2). On air the mean resting oxygen saturation fell from 93.2% to 86.8% with a mean exercise distance of 173 metres (SE 10.5), recovery time of 87 seconds minutes and Borg score of 3.3. The fall in oxygen level with exercise was strongly correlated to the resting oxygen level (r = 0.69, p<0.01) but none of the lung function measures except FVC. On oxygen the mean resting oxygen saturation fell from 96% to 91.5% with a mean exercise distance of 201 metres (SE 11.3), recovery time of 70.5 seconds and Borg score of 3.3. The mean improvement in exercise distance on oxygen was 28 m (SE 3.0, range −34 to 84 metres). Bivariate analysis showed that the improvement in exercise distance on oxygen was significantly correlated to fall in oxygen saturation with exercise in air, though this correlation was not strong (r = 0.265, p = 0.03). This is shown in the figure.
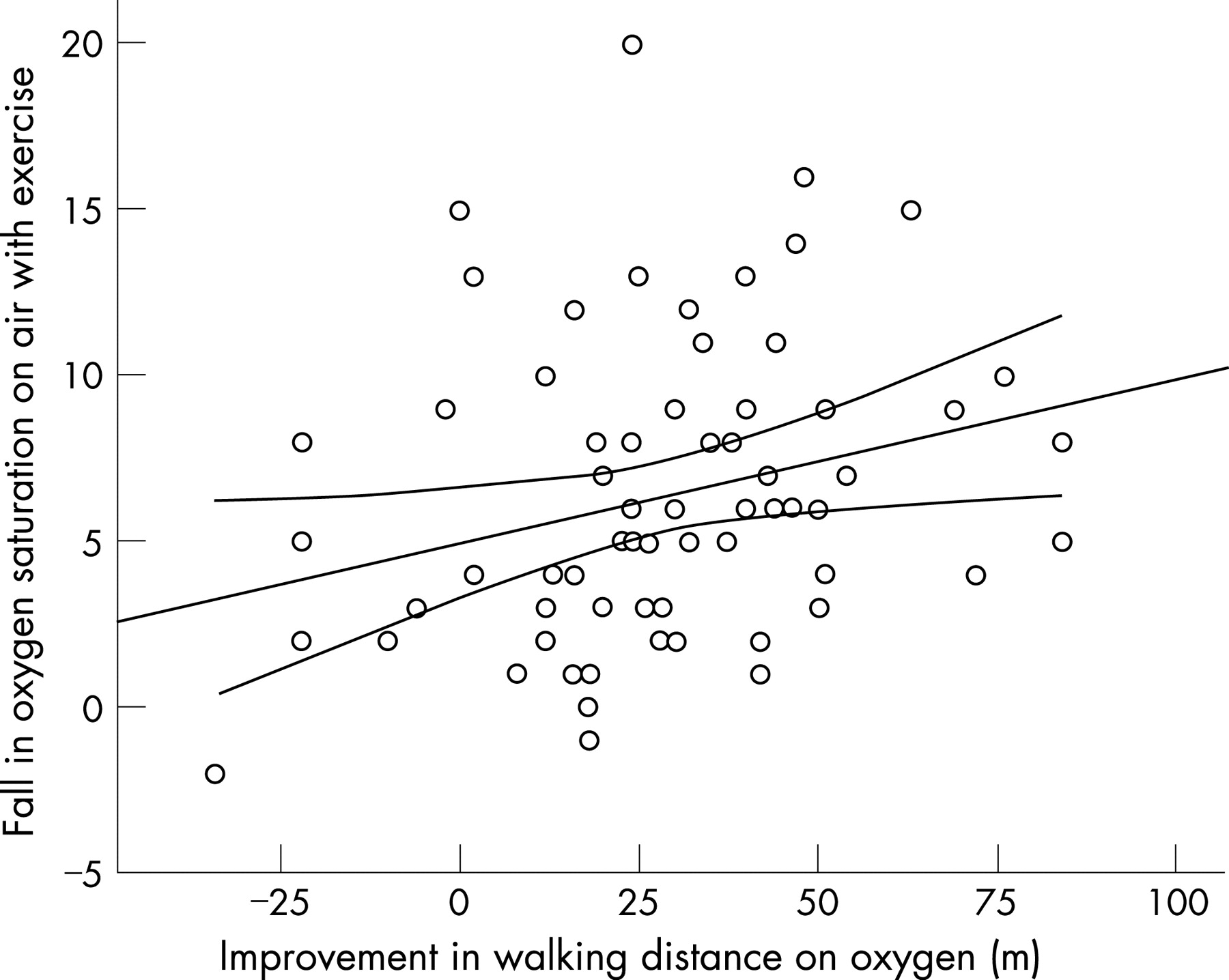
Conclusion: When measuring oxygen desaturation and exercise distance by the 6MWT in patients with COPD, there was a heterogeneous response poorly predicted by spirometric lung function testing and strongly correlated with resting oxygen saturation. For patients with COPD the fall in oxygen saturation during a six-minute walk test in air, only correlates weakly with the improvement in exercise distance when repeated on oxygen. Whether the prescription and subsequent usage of ambulatory oxygen in these patients can be predicted by measures recorded in the 6MWT is a question for an ongoing study.
APPROPRIATENESS OF EMERGENCY OXYGEN THERAPY FOR COPD PATIENTS
J. W. Dodd, H. C. Tribe, D. M. Halpin. Royal Devon & Exeter Hospital, UK
Introduction: Nearly a quarter of all patients admitted to hospitals with breathlessness have chronic obstructive pulmonary disease (COPD) of whom approximately 50% have a degree of hypercapnoea. The use of emergency oxygen therapy is thought to be both inconsistent and poorly understood. (Emerg Med J 2001;18 :333–9). Guidelines which divide management into three stages (pre-hospital, emergency department and pre-admission), have been prepared by the North West Oxygen Group (Emerg Med J 2001;18 :421–3) and the British Thoracic Society (BTS) are currently preparing national guidelines on this issue.
Aim: The primary aim of this study was to use the North West Oxygen Group guidelines to assess whether current oxygen therapy and patient assessment was optimal.
Method: A retrospective review of hospital and paramedic notes of all patients discharged with a primary diagnosis of COPD between February 2007–May 2007 from the Royal Devon & Exeter Hospital (RD&E), UK
Results: 130 cases were identified of which 70 notes were available to be reviewed by our team. Of these 53% were female, 47% male and the mean age was 71 years (range 35–94). 81% were recognised as having COPD by the ambulance team at the pre-hospital stage. 56% (39/70) were admitted via the emergency department and 41% (29/70) via the emergency medical unit, the remaining 3% of patients were admitted via the outpatients department and NHS walk-in centres. Pre-hospital stage: 1.4% of journey times to hospital were less than 15 min, most (46%) took between 30–60 min. 19 patients (27%) were given uncontrolled high flow oxygen (that is, >40%–60% (4–10 l/m), 21 (30%) were given controlled flow oxygen, 8 (11%) were managed without supplementary oxygen and in 22 cases (31%) oxygen therapy was not recorded. Emergency department assessment (ED) stage: 26% patients were seen <10 min. 49% were triaged as urgent. 21% (8/39) patients received uncontrolled high flow oxygen therapy two of whom required non invasive ventilation (NIV). 69% (27/39) were given controlled flow oxygen or room air only and 10% (4/39) oxygen therapy was not recorded. Emergency medical unit (EMU)/alternative emergency department assessment stage: 14% patients were seen <10 min but 41% waited >60 min to be seen by a doctor. 21% patients were triaged as urgent. 7% (2/29) were given high flow uncontrolled oxygen therapy of whom one required NIV. 86% (25/29) were managed with controlled flow or no supplementary oxygen. 7% (2/29) oxygen therapy was not recorded. 69% (48/70) of both ED and EMU patients had arterial blood gas (ABG) analysis 85% (41/48) of whom had their oxygen therapy titrated appropriately.
Discussion: In more urban areas of the UK most patients are transferred to hospital within 15 min. The RD&E served a mixed urban/rural population and it is suprising therefore that only 1.4% of patients reached hopital within 15 min. This is of particular concern given that almost 30% of patients potentially received inappropriately high oxygen therapy. Poor documentation was evident at all three stages of care with between 10% (in hospital) and 30% (pre-hospital) of cases without documentation of oxygen saturations or inspired oxygen therapy. Patients who appear unstable are often transferred directly to ED, which is likely to account for the difference in the percentage of patients triaged as urgent by ED and EMU. When ABGs were taken, oxygen therapy appeared to be titrated correctly on most occasions (85%), however there was a worrying delay in having a medical review, especially for patients admitted via EMU (41% patients waiting >60 min). This delay coupled with the long transit time compounds the risks posed to the patient with COPD. The use of high flow uncontrolled oxygen in hospital occurred in 13% (9/70) of patients, of this group 66% (5/9) had either no documented saturations or results >90% suggesting that they received unnecessarily high concentrations of oxygen resulting in two patients requiring NIV.
Conclusion: The use of emergency oxygen therapy in COPD patients transferred to and admitted to the RD&E differed significantly from the recommendations in the North West Oxygen Group guidelines. Particular problems arose because of long transit times, the use of uncontrolled high flow oxygen at the pre-hospital stage and delays in medical assessment. Once assessed the titration of oxygen appears to be appropriate.
SHORT BURST OXYGEN THERAPY DOES NOT RELIEVE BREATHLESSNESS AFTER EXERCISE IN PATIENTS WITH SEVERE COPD WHO ARE NOT HYPOXAEMIC AT REST
L. Mckinlay, S. Pulakal, P. M. Turkington, B. R. O'Driscoll. Hope Hospital, UK
Background: Short burst oxygen therapy (SBOT) may be ineffective in relieving breathlessness after exercise in patients with severe COPD who are not hypoxaemic at rest (O’Neill B. Respir Med 2006;100 :1129).
Methods: We studied 37 patients with severe COPD (FEV1 <40% predicted), resting oxygen saturation of ⩾93%. Patients undertook an exercise step test four times. After exercise, patients were given 4 l/min of oxygen from a simple face mask, 4 l/min air from a mask (single blind), air from a fan or no intervention. Pulse, rate, oxygen saturation and symptoms were monitored before, during and after exercise. Patients completed a Borg breathlessness scale (no breathlessness = 0, maximal breathlessness = 10).
Results: The mean BORG score was 1.5 at rest, and 5.1 at the end of exercise. The Borg score fell to baseline value by 4 min with no difference between the treatment groups at any time point even for the 13 patients who de-saturated below 90%. The mean time to subjective recovery (feeling same as before exercise) was 3.6 min with no difference between treatments. Mean time to pulse rate recovery was 2.6 min breathing air (95% CI 2.1 to 3.4) and 1.9 min breathing 28% oxygen (1.5 to 2.2). Patients were asked to rank the treatments for relief of breathlessness. Fifteen patients (40%) had no preferred treatment. Of the 22 patients who expressed a preference for a single treatment option, 8 preferred oxygen (22% of the entire group), 6 preferred the fan, 5 preferred room air and 3 preferred air via a mask (χ2 p = 0.42 comparing these four preferences).
Conclusions: This study suggests that non-hypoxic COPD patients get no symptomatic benefit from oxygen therapy after exercise, even if exercise has caused de-saturation below 90%. Use of air from a mask or from a fan had no placebo effect in this study. When combined with previous smaller studies, this negative result has major organisational and financial implications for the use of SBOT in the UK and elsewhere. We would suggest that SBOT should only be considered for patients who express a clear preference for oxygen compared with air in a single-blind n = 1 study.

A REVIEW OF THE FIRST YEAR OUTCOMES OF AN OXYGEN ASSESSMENT CLINIC IN A DISTRICT GENERAL HOSPITAL
J. Creasey, K. Archer, D. Mukherjee, B. Yung, J. Samuel, A. Elsheikh, S. Lincoln. Basildon University Hospital, UK
Background: The provision of domiciliary oxygen therapy underwent significant changes in England and Wales in February 2006. Oxygen guidelines recommend optimal follow-up of patients and in response, weekly oxygen clinics were established. A review of the first three months of this service was presented in 2006 and provided evidence to support the BTS recommendations.
Aim: To review the outcome of the first year of the oxygen clinic in a 652 bedded district general hospital and to establish a local dataset which may provide evidence for a permanent oxygen assessment service within the locality.
Method: Patients prescribed oxygen on discharge were given an oxygen clinic appointment 6 weeks post-discharge. Those with oxygen requirements seen in outpatients were seen in the next available oxygen clinic. The outcome of these assessments were recorded and reviewed.
Results: 112 patients (54 male, age range 51–94 years) attended the oxygen clinic. The attendance rate was 70%. Patients with COPD (75%) and pulmonary fibrosis (22%) formed the two main diagnostic groups. Oxygen therapy was continued at its pre-existing level in 40 patients (36%). 7% had changes made to the oxygen flow rate. In 22%, oxygen orders were changed (for example, long-term oxygen therapy to short burst). In 13% oxygen therapy was either stopped or not required. Overall advice on use and alterations to treatment were made in 51%. Three patients with Type II respiratory failure were admitted directly from the clinic.
Conclusion: This review provides further evidence that oxygen assessment is an essential part of oxygen therapy as more than half of those who attended the clinic had changes made to their oxygen orders. It also highlights the potential risks to patients in the community who are left without assessment. The high non-attendance rates may be an indicator of the need for patient review in the community.
DOMICILIARY OXYGEN PRESCRIPTION FROM SECONDARY CARE: ARE WE GETTING IT RIGHT?
A. Ashish, J. Koch, S. Baird, M. Haris, P. Deegan, M. J. Walshaw. Royal Liverpool and Broadgreen University Hospital, UK
Introduction: LTOT prescription changed from GPs to hospital practitioners in 2006 and a home oxygen order form (HOOF) was commissioned. Unless given for palliative care, LTOT prescription still required hypoxaemia (PaO2 <7.30 kPa), with a response to oxygen treatment (PaO2 >8.0 kPa), without significant hypercapnia (“oxygen titration” study). We assessed the completion of HOOFs and the appropriateness of oxygen prescriptions from our large teaching hospital.
Methods: We analysed 123 randomly selected HOOFs (39% of those generated February 2006 to April 2007) for data completeness. From clinical records we looked at blood gas analyses performed, and whether an oxygen titration study had been undertaken.
Results: In 74 (60%), the HOOF was filled out by a respiratory team, 44 (35%) by a non-respiratory team, and in 5 (4%) the origin was unknown. COPD was the commonest diagnosis (51, 41%), then ILD (13, 10%), heart failure (7, 6%), palliative care (9, 7%), and other conditions (5, 3%): 36 (29%) had no diagnosis. PRHOs completed 62 HOOFs (50%), SHOs 11 (9%), SpRs 13 (10%), consultants 12 (10%), clinical physiologists 17 (14%), and senior nursing staff 6 (5%). Only 18 PRHO forms (29%) and none by nursing staff were correct: respiratory doctors were better than other teams (37/74 vs 10/44, χ2 = 8.56, p<0.01), and clinical physiologists were better than everyone else (15/17, χ2 = 14.0, p<0.001). Based on blood gases and palliative care prescriptions, 70 (57%) were deemed appropriate: 18 (14%) were clearly inappropriate and in 35 (30%) no blood gas analysis had been undertaken. Of 64 LTOT prescriptions, only 12 (18%) had undergone an oxygen titration study. Overall, respiratory physicians prescriptions were more appropriate (43/74) than those issued by non-respiratory physicians (17/44; χ2 = 4.2, p = 0.04), and patients were more likely to be followed up (41 vs 10, χ2 = 12.0, p<0.001).
Conclusions: Despite restricting the prescription of home oxygen to the secondary care sector, there is a high incidence of incorrect HOOFS and inappropriate prescription. Respiratory team are more likely to fill forms and prescribe home oxygen correctly. More formal training, especially of junior doctors may minimise inappropriate prescribing of this costly resource in the future.
PREDICTING THE DEVELOPMENT OF HYPERCAPNIA IN PATIENTS UNDERGOING LTOT ASSESSMENT
J. A. Roberts, N. Linaker, R. ODriscoll, P. M. Turkington, C. Reid, L. Mckinley, N. Diar Bakerly. Salford Royal Foundation Trust, UK
Introduction: Long-term oxygen assessment (LTOT) varies between hospitals. Two retrospective analyses suggested that a small number of patients develop acidosis after overnight oxygen (Marshall et al, 2006, Kashkhusha et al, 2006). Our current practice is to admit all patients for LTOT assessment overnight to assess the risk of hypercapnia.
Aims: To identify the subgroup of patients who would benefit from overnight oxygen assessment by retrospectively looking at their baseline characteristics.
Methods: We reviewed all LTOT assessments carried out on our patients between January 06 to July 07. Data were collected on a database then analysed. Our assessment included baseline blood gases, which were repeated after 2 h of oxygen therapy (2–4 l/min) and repeated again after overnight oxygen treatment in hospital.
Results: (1) Forty three patients were referred; 5 were excluded as found to have a satisfactory PO2 level (>7.3) on air on the day of assessment. (2) COPD was the primary diagnosis in 97% of cases. (3) LTOT was not recommended for 7 (18%) patients due to the development of unsafe hypercapnia (PCO2>7 kPa) and/or respiratory acidosis (PH<7.35) (5 cases on the 2-h blood gases and 2 cases on the morning blood gases after overnight oxygen). (4) The later 2 cases had baseline FEV1 ⩽30% and a rise of >1 kPa in PCO2 after 2 h on 2 l/min O2. (5) FEV1 ⩽30% and the rise in PaCO2 >1 kPa after 2 h of 2 l/min O2 had sensitivity and specificity of 100%, 59% and 100, 83% respectively for incidence of hypercapnia and/or respiratory acidosis after overnight oxygen. (6) The total number of patients, who had both of baseline FEV1 ⩽30% and a rise of PCO2>1 kPa after 2 h on 2 l/min, was 5 (13%).
Conclusions: The use of overnight LTOT assessment may possibly be reserved for those patients who develop a rise in PCO2 >1 kPa after 2 h of oxygen 2 l/min and have baseline FEV1 ⩽30% predicted. This would reflect the need of overnight assessment for only 13% of our patients who are referred for LTOT assessment. Further research with larger number of patients is required.
IS THERE EVIDENCE TO SUPPORT TYPE I RESPIRATORY FAILURE PATIENTS BEING ASSESSED DIFFERENTLY FOR LONG-TERM OXYGEN THERAPY ASSESSMENTS TYPE II FAILURE PATIENTS?
S. A. Kirk, S. P. Wimpress. Glenfield Hospital, UK
Introduction: Long-term oxygen therapy (LTOT) is the administration of supplemental oxygen for the treatment of respiratory failure. Guidelines for the prescription of LTOT were developed by the Royal College of Physicians in 1999. Advice such as the patients it is appropriate for, the inclusion criteria and the benefits it may have, are all clearly outlined. However the actual assessment procedure to prescribe the correct level of oxygen, required by the patient, is not stated. This audit aims to find out if the protocol used within our respiratory department can be modified for patients in Type I respiratory failure, therefore reducing the length of the test. With Type I respiratory failure, the administration of oxygen therapy ought not lead to a significant increase in their pCO2. However patients in Type II respiratory failure, oxygen therapy may lead to worsening of their hypercapnia.
Method: The patients made two visits to the department, at least three weeks apart, at both visits blood gases by earlobe capillary sampling were measured. If on the second visit their results indicated they were still in Type I respiratory failure, they were administered oxygen at a flow rate of 2 l/min from an oxygen concentrator, for 60 min, blood gases were taken at both 30 min and at 60 min.
Results: There were 56 patients included in this audit (32 male and 24 female). The mean baseline blood gas readings were pO2 7.04 kPa and pCO2 5.48 kPa. After 30 min of oxygen mean gases were 9.37 kPa and 5.5 kPa respectively. After 60 min they showed a pO2 of 9.55 kPa and a pCO2 of 5.56 kPa. The baseline, 30 min and 60 min blood gases showed no significant change in pCO2. However there was a marginal difference in pO2 between the 30 min and 60 min. Therefore the data was re-analysed, the patients were split into two groups depending whether their baseline pO2 was </>7 kPa. There were 27 patients in the group with pO2 <7 kPa and 29 patients with pO2 >7 kPa, the same statistical analysis was used. The group with a pO2 <7 kPa again showed no significant change in pCO2, however there was a significant difference between the pO2 measured at 30 min and 60 min. The group with a pO2 of >7 kPa, showed no significant difference between the pO2 at 30 min and 60 min oxygen therapy. This suggests that in patients with a baseline pO2 of >7 kPa, the correct level of oxygen can be determined after only 30 min of oxygen delivery.
Conclusion: We conclude that the LTOT assessment of patients in Type I respiratory failure can indeed be modified so that in patients with a pO2 of >7 kPa the blood gas can be performed after only 30 min of oxygen delivery thereby shortening the assessment procedure which is beneficial for both patient and assessor.
Lung cancer services
THE NATIONAL LUNG CANCER AUDIT; RESULTS AND PROGRESS FOR THE SECOND YEAR, 2006
N. Chanarin1, R. Stanley2, M. Peake1. 1Royal College of Physicians; 2The Information Centre for Health and Social Care
Introduction: The National Lung Cancer Audit is an audit of lung cancer run jointly by the Royal College of Physicians and The Information Centre for health and social care. The audit presented its first year results (patients presenting 2005) in 2006. This abstract presents results from the second year for patients with date of first presentation in 2006. Results are compared against 2005.
Results: In June 2007 the total number of records on the database was 46 512. In 2005 77% of eligible trusts entered data, this has grown to 91% in 2006. Patient numbers have increased, 12 759 were recorded in 2005 growing to 19,887 in 2006. Of these 17 022 had a “date first seen” recorded making them suitable for analysis. In 2005 this represented 40% of the expected number of lung cancer patients in England. In 2006 this was 61%. Referral patterns are unchanged. The most common presentation remaining direct referral from GP, 49.9% of presentations. Patient journey times are similar. Time from referral to first definitive treatment 45 days in 2005, 43 days in 2006. Data completeness has improved. Items such as recording of treatment have improved considerably, however the number of records with all case mix factors completed is still low.
Conclusions: The aims for 2006 were to increase patient numbers, raise participation and improve data completeness. This has been achieved. Participation is now very high and data completeness has started to improve. This will begin to permit risk adjustment of outcomes by trust and network to be published. It is hoped that this will explain previously observed geographical variations in lung cancer outcomes.
IMPROVEMENTS IN MANAGEMENT OF LUNG CANCER PATIENTS FOLLOWING REORGANISATION OF SERVICES AT ST JAMES'S UNIVERSITY HOSPITAL, LEEDS
A. Hardy, P. Plant. St James's University Hospital, Leeds, UK
Introduction: Lung cancer services have recently been restructured with a new fast track clinic from November 2006 allowing rapid access to protected CT and bronchoscopy slots and local PET scanning since early 2007. An audit in May 2007 assessed the impact of these changes.
Methods and Results: 112 consecutive referrals to the fast track clinic were included. 40% were subsequently diagnosed with lung cancer. 45% were referred via the fast-track CO2 form. Mean waiting from referral to clinic was 9.3 days (7.2 days for CO2 referrals), with 90% seen within 14 days and 47% within 7 days (98% and 68% for CO2). 76% had a CT requested from clinic. 67% of these had their CT the following day in a protected slot. Median delay from clinic to CT fell from 10 days in October 2006 to 1 day (range 1–16) in May 2007. 46% patients had a bronchoscopy requested from clinic. 77% had this on day 2 (range 1–12 days). 96% patients had CT prior to bronchoscopy compared to 0% previously. PET usage has increased from 9% to 15% patients and median delay from clinic to PET has fallen from 25 days to 10 days (range 2–51). Median time to triage for all referrals is 17 days, with 79% triaged within 31 days. 14 patients were referred to thoracic surgery and 8 of 41 (20%) lung cancer patients had a curative resection. For those referred for surgery the median triage time was 25.5 days (range 7–70) with 64% triaged within 31 days. 75% of patients had surgery within 62 days of referral. 22 of 41 (54%) lung cancer patients were referred to oncology. Median triage time was 20 days (range 11–55). 82% were triaged within 31 days and 90% received treatment within 62 days.
Conclusions: Compliance with national targets has improved. For CO2 referrals, 98% are seen within 14 days of referral, and 91% receive treatment within 62 days. For all patients diagnosed with lung cancer, 92% received treatment within 62 days of referral compared to 34% prior to October 2006.
AN AUDIT OF USE OF CONCURRENT CHEMO-RADIOTHERAPY WITH CISPLATINUM AND VINORELBINE WITH 55 GY IN 20 FRACTIONS IN SEVEN UK TREATMENT CENTRES
V. Kelly1, J. Hicks1, R. Mcmenemin3, G. Skailes, C. Barnett5, S. Simpson5, J. Maguire1, J. Maguire5. 1Liverpool Lung Cancer Unit; 3Newcastle Oncology Centre; 4Preston Oncology Centre; 5Clatterbridge Centre for Oncology, UK
Introduction: We have audited treatment related toxicity in patients treated with chemo-radiotherapy in centres which had not yet opened SOCCAR.
Method: A data collection form was sent to clinicians who had treated patients with concurrent chemo-radiotherapy prior to trial entry. Information was entered onto a database and analysed using SPSS statistical software.
Results: Information was received on 85 patients treated with concurrent chemo-radiotherapy in seven radiotherapy centres. Early oesophagitis was reported in 71 patients: grade 1 in 18, grade 2 in 41 cases and grade 3 in 12. There was no grade 4 or 5 oesophagitis. Early pneumonitis was reported in 24 patients: grade 1 in 21 cases and grade 2 in 3. There was no grade 3, 4 or 5 pneumonitis. Two deaths at 78 and 84 days in one centre were attributed to aspergillosis but were associated with gross violations of the SOCCAR protocol—that is, use of neo-adjuvant chemotherapy, failure to record lung function or transfer factor, failure to use prophylactic antibiotics and treatment of an excessive v20 in one case and a major geographical miss in the other.
Conclusions: Clinicians at six radiotherapy centres have reported acceptable levels of toxicity with concurrent chemo-radiotherapy using the SOCCAR protocol. This is a safe and effective treatment, but requires careful patient selection and adherence to the protocol regimen.
ORGANISATION OF LUNG CANCER SERVICES IN MERSEYSIDE AND CHESHIRE: THE LUNG CANCER NURSES' VIEW
M. Asim, S. Durairaj, N. Sinnott, M. J. Walshaw, M. J. Ledson. The Cardiothoracic Centre-Liverpool, UK
Introduction: The lung cancer nurse specialist (LCNS) provides support and information, helping patients understand their illness. They are more in touch with patients’ views than clinician managers, and mirror their requirements from the diagnostic process. As service reorganisation to include dedicated “one stop” rapid access clinics and parallel onward referral arrangements in response to waiting time targets has caused debate within the healthcare community, we canvassed the views of LCNSs working in the Merseyside and Cheshire Lung CNG.
Methods: A 14-point questionnaire (waiting time targets, the provision of rapid access, immediate post-diagnosis and ongoing post-treatment management) was sent to all 15 LCNSs working in 7 lung cancer units (140 to >400 cases per year, 1 to 2.5 WTE LCNSs each).
Results: Of 11 (73%) anonymous replies, 8 (73%) were in favour of the 14 day, 6 (54%) of the 31 day, and 9 (82%) of the 62 day target. All indicated that patients should be seen in a dedicated clinic, and 10 (91%) that these should be “one stop” (consultation/CT scan/bronchoscopy (if indicated) on the same day). Nine (81%) thought that patients should be able to consult the relevant clinician (thoracic surgeon, oncologist, or palliative care physician) on the same day. Furthermore, 10 (91%) indicated that these specialists should sit in parallel clinics (same clinic block at the same time). All thought that nurse-led follow-up clinics were appropriate, 10 (91%) attached to a chest physician-led clinic, and all found their jobs satisfying, citing providing support and information to patients as the most rewarding part, while lack of administrative and secretarial support was the most stressful.
Conclusions: As a group, Merseyside and Cheshire CNG LCNSs support the concept of rapid access “one stop” clinics with onward referral to parallel specialist clinics, and most are comfortable with the Government waiting time targets. They support the concept of nurse-led follow-up clinics post-treatment, within the supportive environment of a physician-led clinic. Inadequate secretarial and administrative support was highlighted; inevitable problems for an important group of healthcare professionals who continue to be undervalued by healthcare management.
INCIDENCE AND DEMOGRAPHICS OF MESOTHELIOMA ON THE WIRRAL
S. Agarwal, J. A. Corless, D. Langton. Arrowe Park Hospital, UK
Introduction: The Wirral is a peninsula in the North West of England with a population of ∼360 000. Due to local industries such as shipbuilding rates of asbestos-related lung disease on the Wirral have traditionally been regarded as above average. We sought to investigate the incidence and demographics of new diagnosis of mesothelioma over the last six years since January 2001. Data were retrieved from the lung cancer management system.
Results: From January 2001 the total number of new cases identified was 61. Annual incidence of mesothelioma from 2001 to 2006 was 9, 7, 5, 12, 18, 9 respectively (mean = 12, median = 9). 88% (54) were males. Median age was 72 (range 51 to 90). A history of definite asbestos exposure was noted in 66% (34). 83% of cases were initially referred via the patient’s general practitioner with the remainder admitted acutely to hospital before first diagnosis. 94% had definite histological confirmation with a radiological only diagnosis in 6.5% (4). Histological typing confirmed it to be mesothelioma (unspecified) in 47, epitheloid in 8 and sarcomatous in 2 cases. The median time to reach the diagnosis was 36 days (range 6 to 264). 47 patients have now died with a median survival of 258 days (range 31–972). The addresses were plotted on the map using Microsoft Auto Route software. The majority of patients with mesothelioma live on the eastern half of the Wirral. The geographical spread closely correlates with areas of deprivation, high smoking rates and also previous high occupational users of asbestos, particularly the shipyards.
Conclusions: Our figures demonstrate burden of mesothelioma is higher than the national average. There does not however appear to be any current evidence of a rise in cases in keeping with national predictions. Cases of mesothelioma on the Wirral are higher in areas of high deprivation and smoking rates and close to previous shipbuilding activity.

ABNORMAL RESULTS OF GP-REQUESTED CHEST X RAYS COPIED TO THE HOSPITAL CHEST CLINIC: IS THERE A SIGNIFICANT DELAY BEFORE PATIENTS ARE REFERRED FROM THE COMMUNITY?
R. Bourkiza, K. Archer, B. Yung, A. Elsheikh, D. Mukherjee, J. Samuel. Department of Respiratory Medicine, Basildon University Hospitals Foundation NHS Trust, UK
Background: Many factors are responsible for the relatively poor survival rate of the UK lung cancer patients. The delay in patients being referred to the chest physicians may be a contributing factor. There are anecdotal reports of delay in patients being referred to chest clinics from primary care physicians despite having been found to have abnormal chest x rays (CXRs) suggestive of a diagnosis of lung cancer. The general practitioners (GPs) in our hospital catchment area can request CXRs to be done at our hospital and results of the CXRs are sent/faxed to the GPs. Since year 2005, any abnormal GP-requested CXR reports suggestive of the presence of lung cancer are copied to the chest clinic and GPs are advised to refer patients urgently to the chest clinic.
Aim: To establish whether patients found to have abnormal CXRs suggestive of underlying cancer (whose CXR reports were copied to the chest clinic) were referred urgently as recommended.
Method: A prospective survey covering the period of December 2006 to May 2007 was carried out. The reports of all GP-requested CXRs with abnormal results suggestive of underlying cancer copied to the chest clinic were collected. The investigators checked the hospital PAS system to establish whether the patients had been referred to the chest clinic at intervals of five working days since reports had been issued. After 15 working days, if a patient had not been referred, the GP who had requested the CXR was contacted to establish whether he/she was aware of the abnormal CXR report and whether any action had been taken. Reasons for the non-referrals were sought.
Results: During the study period, 50 abnormal CXR reports were copied to the chest clinic involving 50 patients (28 male, mean age: 70 years, range: 40–91 years). The CXRs were performed after a median of one working day (range 0–17 days) after requests were made. The reports were issued to the GPs after a median of three working days (range 0–16 days) after the CXRs were performed. The chest clinic received copies of the abnormal reports after a median of 1 working day (range: 0–8 days). Of the 50 reports returned to the GPs with recommendations of urgent referrals to the chest clinic, 48 patients (96%) were referred after a median of 1 working day (range: 0–15 days) since reports were issued. Of the 48 referrals received, 44 (92%) were referred via the 2 week wait (2WW) route. We found no significant delay in referral in the group of patients referred via the non-2WW route compared to those referred via the 2WW route. All 48 patients (including the four patients not referred via the 2WWw route) were seen within 2 weeks of referrals being received. 29 of the 48 patients (60%) were subsequently found to have cancer of which 27 patients had primary lung cancer. No referrals were received at the chest clinic for 2 patients (4%) so their GPs were contacted. We found that one patient was referred to a neighbouring hospital. One patient was a known case of bowel cancer with a new finding of lung metastasis and was referred directly to her oncologist.
Conclusion: This survey confirms that GPs receiving abnormal CXR reports responded appropriately by referring patients to the secondary care in a timely fashion. The system in place in our locality therefore appears to be working well.
A COMPARISON OF CANCER REGISTRY AND HOSPITAL-BASED LUNG CANCER CASE ACQUISITION FOR FOUR HOSPITALS IN WALES IN 2005
N. A. McAndrew1, I. Williamson2, S. Linnane3, E. Evans4, E. Lim1. 1Wrexham Maelor Hospital; 2Royal Gwent Hospital; 3Cardiff and Vale NHS Trust; 4Swansea Hospitals NHS Trust, UK
Accurate lung cancer case registration provides the denominator for outcome comparisons in diagnosis and treatment. Wales currently uses two systems to collect lung cancer data/registrations. All hospitals use a clinical database Cancer Network Information System Cymru (CaNISC) serving MDTs, where locally inputted data are transferred to a central server. The separate cancer registry is the Welsh Cancer Intelligence and Surveillance Unit (WCISU). This audit compares case registration on WCISU (centrally) with that on CANISC (locally) for patients newly diagnosed with lung cancer in 2005. WCISU uses the following data sources: Patient Episode Database Wales (PEDW) derived from hospital codings; pathology reports from 12 out of 14 trust laboratories (histology but not cytology) and the Office of National Statistics (ONS) provides details of death certificates. WCISU does not currently use CaNISC. This audit excludes WCISU DCO (Death Certificate Only) cases—that is, those that had no second corroborating source of data.
Analysis of data from four hospitals/trusts (Newport, Swansea, Cardiff, Wrexham) found that discrepancies in the databases fell into clear groups. These included: (1) failure of MDTs to register cases that WCISU successfully recorded; (2) WCISU recording cases that were not lung cancer, with particular difficulties with “unknown primary”; (3) WCISU missing a small number of cases; (4) CaNISC cases with wrong year of diagnosis; (5) technical difficulties with WCISU “pulling through” CaNISC data.
More detailed analysis in Wrexham, Cardiff and Swansea (∼220 discrepant cases using case notes, pathology and radiology systems, ONS data and MDT meeting minutes) explored the reasons for the above. Cases were missed locally for two main reasons—an MDT member failing to bring the case to the MDT and cases that never had any MDT member input (these were almost all “clinical and radiological only” cases so would not be picked up by pathology surveillance). WCISU also recorded cases as lung cancer “incorrectly”—some were recorded locally as “unknown primary” and in Wrexham two cases of metastatic renal carcinoma were incorrectly recorded as “lung cancer” on the death certificate. WCISU missed four cases in Wrexham—three had no histology/cytology and two had no mention of lung cancer on the death certificate. Simple clerical errors resulted in a number of cases being put in the “wrong year”. Some difficulties were found with date of diagnosis around the turn of a year. WCISU also ascribed cases to the four Trusts/hospitals that were diagnosed at other hospitals.
The audit identified several areas that can be addressed to improve accuracy and ascertainment of lung cancer data collection in Welsh Trusts and by WCISU:
This audit illustrates ways in which both registry data and local case registration can be improved. It also shows that whilst registry case registration is better it is still incomplete.
This comparison is being repeated for 2006 data but results of the 2005 audit are just being circulated and changes to practice made. The re-audit of 2007 and 2008 data will complete the cycle to see if the audit had been effective in implementing a positive change in practice.
REASONS FOR DIAGNOSTIC DELAY IN LUNG CANCER
A. S. Jackson, T. B. Ho. Frimley Park Hospital, UK
Introduction: Government targets for the diagnosis and treatment of lung cancer state that patients should receive their first treatment for lung cancer within two months from referral by the general practitioner. By 2008 the goal is to reduce this to one month. At Frimley Park Hospital, we are currently achieving the two-month target, but feel that to reduce this down to one month with the current system may be difficult. Therefore, the aim of this audit was to look at reasons for delay in diagnosing patients with lung cancer, with a view to making the system more efficient and minimising patient anxiety.
Methods: We looked at patients at Frimley Park Hospital who received their first treatment for lung cancer in the six-month period from the beginning of June to the end of November 2006. We measured the number of days from date first seen in clinic to the date of the procedure that provided the diagnosis. During this time, 12 patients out of a total of 50 had a delay in diagnosis longer than one month. Two of these were excluded, as hospital notes were unavailable. Characteristics of the patients are shown in the table. A significant number of patients had Stage IV or extensive disease and received palliative treatment.
Results: The most common reason identified for a delay in diagnosis was having to undergo more than one diagnostic procedure. Other reasons identified included admission to hospital, management outside the lung cancer multidisciplinary team, and treatment for pneumonia. In most cases the patient underwent a bronchoscopy followed by a computerised tomography (CT) guided biopsy. However, the average wait for a bronchoscopy was nine days, while the wait for a CT guided biopsy was two weeks.
Discussion: NICE guidelines recommend that CT imaging should be performed prior to undergoing a bronchoscopy. This recommendation is based on evidence from two clinical trials showing that this increases the sensitivity of bronchoscopy. In this district general hospital, patients usually attend clinic before having a CT scan, and a bronchoscopy is planned and occasionally performed before the CT scan. Patients then undergo a CT guided biopsy if the bronchoscopy does not yield a diagnosis. On retrospective review of CT imaging, CT guided biopsy or lymph node biopsy may have been the more appropriate first line investigation in six of these patients. This finding supports the recommendation that imaging should be reviewed prior to planning diagnostic procedures and we are now implementing this in our hospital. This should significantly reduce waiting time for a number of patients.
Conclusions: In summary, the most common reason for delay in diagnosis was having to undergo more than one diagnostic procedure, and these patients often had more advanced disease and were managed palliatively. Ensuring that appropriate imaging is performed prior to planning diagnostic procedures can reduce delay and lessen patient anxiety. One method of achieving this is through the introduction of early diagnosis clinics as recommended by NICE.
URGENT 2 WEEK LUNG CANCER REFERRALS FAIL TO IDENTIFY MOST PATIENTS SEEN IN SECONDARY CARE CANCER SERVICE
P. Cadden, M. Najib, E. Wilcock, K. Longmate, A. Wardman, S. Madi, I. Aziz, R. Sundar. Royal Albert Edward Infirmary, UK
Background: Lung cancer is a major cause of morbidity and mortality in the UK. Strategies to improve prognosis and access to treatment have included two-week urgent referrals. Local experience suggested to us that in the Wigan area this was not identifying most of the patients who were coming under the care of the secondary care lung cancer multidisciplinary team.
Aims: To audit the number of patients being seen and identifying areas to target to improve future access and prognosis.
Methods: A two-year retrospective audit of all lung cancer patients treated at our local district hospitals. We documented gender, age, symptoms on presentation, mode of referral, investigations performed, histological diagnosis and treatment pathway.
Results: In total 458 patients were identified for the period 1 June 2004 to 31 May 2006. 56% were male and most patients were over 65. Most patients were referred as inpatients (55%), via the Emergency department (34%) and by other consultants (21%). Routine GP referrals accounted for 12% of cases. 17% of patients were referred directly from radiology department with abnormal chest x ray appearances. Only 16% of cases were referred as urgent two week cancer referrals. Presenting symptoms included dyspnoea (39%), cough (27%), haemoptysis (14%), weight loss (19%), pain (21%), dysphonia (7%) and abnormal plain chest radiograph (81%). Over the two years 19% of patients were staged to undergo curative treatments.
Conclusions: We have implemented an abnormal chest x ray meeting so all abnormal plain chest x rays are discussed and prioritised each week. It is not beneficial for patients to have to wait for symptoms to progress to a point where they need to have an unscheduled healthcare episode. In view of the high number of patients self-presenting to the hospital in our area we are putting in place an awareness program for local patients and GPs to emphasise the importance of plain chest x rays and early referral in identifying patients with lung carcinoma. We feel that in those patients that present with chest symptoms and are current or significant ex-smokers an early chest x ray is indicated.
AUDIT OF LUNG CANCER WAITING TIMES AT A DISTRICT GENERAL HOSPITAL
K. Mortimer, S. Mallawathantri, A. Rousell, N. Ali, G. Cox. King's Mill Hospital, UK
Background: The Department of Health Cancer Waiting Time (CWT) targets specify a maximum 62-day wait from urgent (two-week wait) GP referral for suspected cancer to first definitive treatment and a maximum 31-day wait from diagnosis (decision to treat) to first definitive treatment. Waiting Time Adjustments (WTAs) are allowed for certain circumstances that are out of the control of the NHS.
Methods: We undertook an audit of all urgent GP referrals with a final diagnosis of lung cancer in 2005 and 2006 to determine: (a) the extent to which CWT targets were met; (b) the reasons for missing CWT targets; (c) the effects of and reasons for WTA; (d) the time between the decision to provide a specific treatment and implementation of treatment.
Results: The main reason for missing CWT targets was the need for multiple tests to make a diagnosis in more complex cases while the main reasons for WTA were patient fitness, patients needing time to think and missed appointments.
Conclusions: Average waiting times were within the CWT targets and were shorter in 2006 than in 2005 probably reflecting the appointment of a full time cancer tracker and MDT coordinator, the use of the live Orion tracker system and the development of a local PET service. CWT targets were missed mainly due to difficulties establishing a diagnosis in more complex cases. WTA has little effect on time from referral to treatment. Treatment is provided promptly following the decision to treat.
WHAT HAPPENS TO LUNG CANCER PATIENTS AFTER TREATMENT? AUDIT AT 4 YEARS
A. McIver, M. Ellison, H. Bonwick, J. Hughes, V. Kelly, M. J. Walshaw. The Cardiothoracic Centre-Liverpool, UK
Introduction: Although the lung cancer diagnostic and treatment pathway is streamlined, there is little research on the subsequent patient journey which ends in death for the vast majority. We looked at this aspect in our large lung cancer unit.
Methods: Outcome of diagnoses within our catchment area in 2003 was audited. Entries from the Cancer Registry and our database were searched to ensure a complete denominator: treatment, survival, and place of death data were collected yearly until 2007 (4 years).
Results: There were 354 cases (199 male (59%)): 197 (58%) non-small cell, 53 (15%) small cell, and 104 (29%) clinical diagnosis. Mean diagnostic time was 28 days (median 16). At diagnosis, PS = 0 in 50 (14%), = 1 in 106 (30%), = 2 in 90 (25%), = 3 in 51 (15%), = 4 in 3 (1%), and 54 (15%) were not recorded. 29 (8.2%) underwent curative surgery alone, 5 (1.4%) surgery with adjuvant oncology, 234 (66.1%) oncological treatment (of which 70 had specialist palliative care (SPC) input), 34 (9.6%) SPC alone, and 52 (11.1%) were not recorded. For survival data see table. Of the 316 deceased, 159 (50%) died at home, 118 (37%) in hospital and 39 (12%) in a hospice. Of these groups, 36%, 28%, and 28% respectively had SPC input at diagnosis.
Conclusions: Survival in the surgical and oncological groups was respectable, with >50% undergoing attempted curative resection alive at 4 years. The low resection rate (9.6%) reflects our inner city catchment area, with high comorbidity and late presentation. Despite this, the majority of patients died at home, out of keeping with national figures: this may reflect the supportive services model we have adopted as part of our MDT approach. Further attention should be paid to the “downstream” part of the lung cancer patient journey, which is of increasing duration for the majority of patients.
GLOBAL PALLIATIVE CARE NEEDS IN LUNG CANCER PATIENTS ARE ASSOCIATED WITH PRESENCE AND SEVERITY OF RESPIRATORY SYMPTOMS BUT NOT INFLAMMATORY RESPONSE OR ALBUMIN LEVEL
D. Buchanan1, A. Thompson1, R. Milroy2, P. Levack3. 1University of Dundee; 2Stobhill Hospital; 3NHS Tayside, UK
Introduction: Lung cancer is the commonest cause of cancer related deaths in Scotland, the UK and worldwide. It is a disease of high symptom burden, psychosocial effects and poor prognosis. Palliative care has an increasing role in multidisciplinary lung cancer management. The palliative outcome scale (POS) has been developed and validated in several clinical settings as a tool to identify and quantify palliative needs. Elevated C-reactive protein (CRP) and reduced albumin are associated with shorter survival. This study compared respiratory symptoms, POS, CRP and albumin in lung cancer patients attending an out-patient clinic.
Methods: 115 patients attending a lung cancer clinic completed a questionnaire containing the POS and three questions rating the severity of dyspnoea, cough and haemoptysis. CRP and albumin of each patient at diagnosis was measured.
Results: The presence and severity of dyspnoea, cough and haemoptysis were associated with increased palliative needs as measured by POS. (POS 0–4 vs 5–9, p = 0.002, POS 5–9 vs 10–14, p<0.001, POS 10–14 vs 15+, p = 0.042). Albumin and CRP were not associated with POS.
Conclusion: Raised CRP and low albumin are known adverse prognostic factors in lung cancer but do not predict overall palliative care needs as measured by POS. The symptoms of dyspnoea, cough and haemoptysis in lung cancer out-patients are associated with their palliative needs. These results emphasise the importance of identifying the presence and severity of physical symptoms. This simple approach may allow early identification of patients who are likely to benefit from specialist palliative care services irrespective of their individual prognosis.
Improving outcomes in lung infection
STATIN USE REDUCES MARKERS OF SYSTEMIC INFLAMMATION AND 30-DAY MORTALITY IN PATIENTS WITH COMMUNITY ACQUIRED PNEUMONIA
J. Chalmers, A. Singanayagam, A. Hill. Royal Infirmary of Edinburgh, UK
Introduction: Previous retrospective studies have shown a reduced incidence of community acquired pneumonia (CAP) and improved outcomes in patients taking HMG co-A reductase inhibitors (statins), thought to result from anti-inflammatory effects. We tested the hypothesis that markers of systemic inflammation would be lower in patients with CAP taking statin therapy and that this would be associated with superior outcomes.
Methods: We performed a retrospective study of 514 patients over the age of 50 with a diagnosis of CAP between February 2005 and February 2007. C-reactive protein and fibrinogen were measured on admission as markers of systemic inflammation. The outcomes of interest were: admission CRP and fibrinogen; need for mechanical ventilation and/or inotropic support; development of complicated pneumonia (lung abscess, empyema or complicated parapneumonic effusion); 30-day mortality. Multivariate logistic regression was performed adjusting for age, sex, comorbidity, smoking status and pneumonia severity.
Results: Data are presented as median interquartile range (IQR). Patients receiving statins were significantly older 74 years (61–81) vs 70 (61–79), p<0.01, more were male (53% vs 46%, p<0.01), more had chronic cardiac disease (28.4% vs 11.6%, p<0.0001) or stroke (15.4% vs 9.7%, p = 0.05). The severity of pneumonia using CURB65 score was not significantly different between groups- 2 (2–3) on statins vs 2 (1–3) not on statins. C-reactive protein and fibrinogen levels were significantly lower in patients receiving statin therapy (see table). There was no significant difference in rates of complicated pneumonia (1.8% on statins vs 5.9%) or requirement for invasive ventilation and/or inotropic support between groups (10.5% on statins vs 12.8%). On multivariate analysis there was a reduction in 30-day mortality in patients receiving statin therapy (11.7% on statins vs 16.8%, OR 0.48 (0.25–0.90), p = 0.02).
Conclusion: Markers of systemic inflammation and 30-day mortality are reduced in patients with CAP treated with statins.
DOES DOCUMENTING THE CURB-65 SCORE IMPROVE APPROPRIATE INITIAL EMPIRICAL ANTIBIOTIC THERAPY IN THE MANAGEMENT OF COMMUNITY ACQUIRED PNEUMONIA?
O. J. Eneje1, A. Colville3, B. D. Patel2. 1Royal Devon & Exeter Foundation Trust; 2Department of Respiratory Medicine, Royal Devon & Exeter Foundation Trust; 3Department of Microbiology, Royal Devon & Exeter Foundation Trust
Introduction: The BTS recommend the use of the CURB-65 to identify patients at risk of a poor prognostic outcome from community-acquired pneumonia (CAP) and to guide appropriate choice of antibiotic therapy. We assessed if the CURB-65 system was being effectively used to guide appropriate antibiotics prescription in patients admitted with CAP to our hospital.
Method: Retrospective case note and drug chart review of all patients admitted with CAP to the emergency medical unit during December 2006. Data obtained included demographics, previous antibiotic therapy, baseline observations, investigation results and documentation of the CURB-65 on admission. If the CURB-65 was not documented it was calculated making the assumption that, unless otherwise stated, the patient was not confused.
Results: Forty eligible cases (57.5% male) were identified, median age 76.0 (IQR 25) years. Admission CURB-65 was documented in 10 cases, only one patient had a documented mini-mental test. CURB-65 scores were calculated for the remaining 30 individuals. Twenty-one (52.5%) patients were started on appropriate antibiotics according to documented or estimated CURB-65 score, this increased to 32 (80%) following consultant review. In only two cases was it documented why an alternative antibiotic was used. 70% of patients with a documented CURB-65 on admission received appropriate antibiotics, compared with 46.7% of those in who the CURB-65 was not documented (p = 0.2, χ2). Ten patients had severe CAP (CURB-65 >2), but in only 4 was the CURB-65 documented on admission and 3 of these received appropriate antibiotics. Of the remaining 6 patients, only 2 were initiated on appropriate therapy. The overall mortality was 15%, of which 2 had a documented or estimated CURB-65 >2 on admission.
Discussion: The overall rate of conformity to hospital guidelines for the initial management of CAP was low (52.5%), but increased to 80% following consultant review. Documentation of the CURB-65 score on admission improved compliance with the guidelines (not statistically significant). Only two cases had a documented clinical justification for deviation from antibiotic guidelines. An increase in use of the CURB-65 by junior medical staff may increase concordance with antibiotic policy in the treatment of CAP.
IS TIMING OF INITIAL ANTIBIOTIC ADMINISTRATION RELATED TO OUTCOME IN COMMUNITY-ACQUIRED PNEUMONIA?
S. E. Hill, M. Woodhead. Manchester Royal Infirmary, Manchester, UK
Introduction: Common sense suggests that delays in antibiotic administration in infections may be associated with worse outcome. There is some research evidence to support this in CAP which has lead to all National and International Guidelines making a recommendation about the importance of early antibiotic administration.
Aims: To examine time of antibiotic administration in relation to outcome in adult patients with CAP.
Methods: This was a retrospective case control study. Cases coded as ICD10 J10-J18 were identified from the Hospital Information database for 1 January 31 December 2006 and case records examined. Cases were excluded if notes were not available, if the diagnosis was wrongly coded, if significant information was missing, if immunocompromised, nosocomial infection or if considered to be a terminal event. Data were extracted manually and recorded in an Excel spreadsheet and analysed using parametric and non-parametric statistical tests.
Results: 489 cases were found of which 129 (27%) had died. All 129 dead notes were sought and 54 included in the analysis (37 not found and 38 excluded for above reasons). One in three live notes were sought and 150 of 266 examined were included (53 not found and 63 excluded for above reasons). Patients that died were older (median age 81 vs 65, p = 0.7; and were significantly more likely to be in CURB-65 group 3 (score 3–5) (54% vs 12%) than Group 1 (0–1) (15% vs 57%) p<0.001. There was no difference in the median time to first antibiotic administration between dead (3 h 29) and live (3 h 24) patients p = 0.7, but a significantly greater proportion of those who died only received first antibiotics after 8 hours (20% vs 8%). In a previous audit prior to the introduction of the 4-h A&E waiting rule, 22% of patients only received antibiotics after 8 h suggesting that speed of antibiotic administration had improved (p = 0.06). Factors significantly related to delay in first antibiotic prescription included lower CURB-65 score, p<0.0001, (CURB-65 1 3 hrs56, CURB-65 2 3 h 38, CURB 3 2 h 53), IV vs PO (p<0.0001), A&E prescription vs MAU (p<0.0001) and time of arrival (p<0.0001). Those arriving between 21:00 and 09:00 had a longer delay before first antibiotic. CURB-65 score was only recorded in 15% of those that died and 20% of the living and in 18% of these it was recorded incorrectly (usually incorrectly high).
Conclusions: Time to delivery of first antibiotic to patients with CAP appears to have improved, but a worrying proportion still only receive first antibiotics after 8 h from admission. This might be improved by more rigorous use of CURB-65 scoring, and first administration before patients leave the emergency department.
ARE WE PRESCRIBING TOO MANY ANTIBIOTICS FOR ACUTE HOSPITAL ADMISSIONS WITH COMMUNITY ACQUIRED PNEUMONIA?
A. Choudhury, S. Fong, S. Saha, W. Ahmed, C. Brook, T. Fernandez, L. Kuitert.Royal London Hospital, Barts and The London NHS Trust, UK
Introduction: British Thoracic Society (BTS) guidelines recommend the use of severity assessment scoring to guide management and choice of antibiotics for community acquired pneumonia (CAP) (Thorax 2001;Suppl 4:S56). The guidelines suggest there may be a trend towards over-prescribing of antibiotics in CAP.
Aim: To determine appropriateness of antibiotic prescribing for CAP.
Methods: We carried out a prospective audit for 8 weeks beginning January 2007 on patients given antibiotics for suspected CAP that required hospital admission. Data were collected from medical records at time of post-take ward round. Only patients with clear consolidation on plain chest x ray were included. CAP severity was assessed using the 5-point CURB65 score. (C: Increased Confusion, U: Urea>7.0, R: Respiratory rate>30, B: BP systolic<90, 65: Age >65 years). The score would be calculated by the auditing doctor if not recorded by the admitting doctor. Management by acute medicine, respiratory and non-respiratory teams at time of post-take ward round was compared.
Results: Sixty four patients (median age 74 years, males 37 (58%)) were admitted with CAP. Only 6/64 (9%) of cases had a CURB-65 severity score recorded by the admitting doctor. Parenteral administration and the use of two concomitant antibiotics were common in patients with low CURB-65 scores. Despite the BTS guidelines, cephalosporins were regularly prescribed in patients with severe pneumonia (CURB-65 >2). Respiratory teams were less likely than medical teams to prescribe intravenous antibiotics in patients with CURB-65 <3 and more likely to in the severe group (CURB-65 >2); similarly they prescribed much fewer cephalosporins.
Conclusions: In our hospital, failure to implement severity scoring for CAP resulted in over-prescription and inappropriate selection of antibiotics in non-severe patients. Respiratory teams followed the guidelines more closely than general medical teams. More education for both respiratory and non-respiratory specialists is needed to ensure severity scoring and appropriate management thereafter becomes routine practice for CAP.
MANAGEMENT OF COMMUNITY ACQUIRED PNEUMONIA: APPROPRIATE USE OF SEVERITY ASSESSMENT TOOL
V. S. Sreeguru Lakshman, M. Asim, M. Mcgovern, P. Stockton. Whiston Hospital, UK
Introduction: CAP is associated with significant mortality, morbidity, and burden on health care resources. British Thoracic Society (BTS) published guidelines for the management of CAP in 2001 (updated in 2004).
Aim: Establish whether we were following the BTS guidelines and using a validated assessment tool—that is, the CURB-65 score.
Method: Retrospective study. Patients admitted (April 2005–April 2006) with a confirmed diagnosis of CAP identified from the hospital database. Data collected using a modified BTS CAP audit tool.
Results: Fifty patients. Mean age 60 years (16–94). 16 (32%) were males and 34 were (68%) females. Mean length of stay was 14 days (1–63 days). 29 (58%) had significant co-morbidities. 33 (66%) current/former smokers, 13 (26%) non-smokers, 4 (8%) no smoking history recorded. CURB-65 score was documented in only 7 (14%). We retrospectively calculated the score for the remainder from data available in the medical records. 15 (30%) had a score of 0; 14 (28%) had a score of 1; 9 (18%) had a score of 2; 11 (22%) had a score of 3; 1 (2%) had a score of 4 and no patient had a score of 5. 72% had arterial blood gases done and 58% were found to be hypoxic (PaO2 <10). 45 (90%) had senior review (SpR/Consultant) within 24 h, 3 (6%) within 2 days and 2 (4%) within 3 days. 34 (68%) had follow-up appointment. 12/33 (36%) of smokers (current and former), who would be considered high risk for underlying cancer, had no follow-up arrangements made.
Conclusions: Improvements are required in the severity assessments and the documentation of the CURB-65 score at the time of admission. Over 50% of patients had a CURB-65 score of ⩽1, and could have been managed in the community. Over one third of smokers (high risk for underlying cancer) did not undergo a follow up chest x ray and assessment. We have introduced guidelines to facilitate appropriate evidence-based management of CAP within our Trust. We are promoting awareness regarding our pre-existing post-pneumonia clinic and use an x ray coding system to highlight abnormal x rays.
SEVERITY ASSESSMENT AND ADHERENCE TO TREATMENT GUIDELINES HAS POSITIVE IMPACT ON TREATMENT OUTCOME IN HOSPITALISED COMMUNITY-ACQUIRED PNEUMONIA PATIENTS
V. Dudzevicius, N. Krishnaraj, G. Antunes, S. A. Murphy. The James Cook University Hospital, UK
Aim: To evaluate the rates of assessment of community-acquired pneumonia (CAP) severity and impact of adherence to the BTS guidelines on the outcome.
Materials and Methods: Retrospective study was done in 90 cases of patients hospitalised with diagnosis of pneumonia. 20 patients were excluded because of other diagnoses. 70 cases were eligible for further analysis. CURB-65 score assessment on admission and treatment according to BTS guidelines were analysed. Impact of CURB-65 score, antibacterial treatment route and length on mortality and relapse or readmission was analysed by means of logistic regression. Statistical analysis was done using SPSS software.
Results: CURB-65 score was recorded in 13.2% (n = 9) of all patients: 26% (n = 6) of patients admitted to Respiratory Medicine ward; 6.3% (n = 1), Medical Assessment Unit; 15% (2), other medical wards; and 0%, Elderly Care/surgical/ITU wards. Treatment guidelines were fully or partially met in 93.8% (n = 61) of patients. Hospital mortality rate was 12.3%. There were no deaths in patients with CURB-65 score less than 2 points (p<0.05). Mortality rates were 25% and 11.5% in non-compliant vs fully/partially compliant with BTS guidelines treatment group (p>0.05). Higher rates of relapse/readmission were found in noncompliant vs. compliant with BTS (100% vs 20.4%, p<0.05) or given oral vs intravenous antibiotics on admission (32.1% vs 17.2%, p<0.05) groups. Increasing CURB-65 score was positively (OR 2.89; CI 1.21 to 6.89, p = 0.017) and antibacterial treatment duration was negatively (OR 0.73; CI 0.56 to 0.96, p = 0.025) related to in-hospital mortality.
Conclusions: CURB score was assessed in minority of CAP patients admitted to hospital, especially admitted to other than Respiratory wards. Mortality was significantly related to increasing CURB-65 score points. Relapse or readmission was more frequent in patients not treated according BTS guidelines and not given intravenous antibiotics on admission.
DO SPIROMETRY, COUGH AND PATIENT PERCEIVED SYMPTOMS CHANGE FOLLOWING INTRAVENOUS ANTIBIOTICS FOR AN ACUTE EXACERBATION OF BRONCHIECTASIS?
O. Hewitt1, J. M. Bradley2, J. Ferguson3, S. E. Elborn1. 1Regional Respiratory Centre, Belfast Trust, Belfast City Hospital; 2University of Ulster; Regional Respiratory Centre, Belfast Trust, Belfast, City Hospital; 3Regional Respiratory Centre, Belfast Trust, Belfast City Hospital, UK
Introduction: Bronchiectasis results in increased frequency of exacerbations often requiring intravenous (IV) antibiotics. During an exacerbation, patients experience worsening of symptoms and spirometry which subsequently improve following IV antibiotics. These outcomes are frequently used to assess individual patients’ response to treatment.
Aims: To assess changes in spirometry, cough and symptoms following IV antibiotics; a secondary objective was to establish if there was a relation between change in spirometry and change in cough and symptoms.
Methods: From January to May 2007 all patients attending a specialist bronchiectasis service with an acute exacerbation of bronchiectasis (O’Donnell et al) requiring IV antibiotics completed spirometry, the Leicester cough questionnaire and were asked questions relating to four key bronchiectasis symptoms (quality of life, sputum clearance, change in symptoms and overall tiredness). Patients were assessed at the beginning and end of IV therapy. The Leicester cough questionnaire contains three domains, domain scores range from 1–7 (higher scores indicate less severity); bronchiectasis symptoms domain scores range from 1–5 (higher scores indicate severity).
Results: Data from 50 patients mean (SD) 59 (10) years were analysed. The mean baseline FEV1 % 52 (26)%. There was a significant improvement in FEV1 following IV antibiotics 3.5 (9.5)% p = 0.01. There was a significant improvement in the Leicester questionnaire domain scores following IV antibiotics: physical, 0.63 (0.97); psychological, 0.86 (1.29); and social, 0.74 (1.29). There was a significant improvement in three of the four key bronchiectasis symptoms following IV antibiotics: quality of life 0.64 (1.63), symptoms 0.77 (1.40), and tiredness 0.70 (1.24). There was no relation between change in lung function and change in cough or symptoms.
Conclusion: Individual changes in spirometry following IV therapy are small. Improvements in cough and other symptoms related to bronchiectasis are not captured by changes in spirometry. Inclusion of cough and symptoms scores in assessing outcome of treatment and response to IV antibiotics may be valuable in capturing the benefit of treatment more fully.
OUTCOMES OF EXACERBATIONS OF NON-CYSTIC FIBROSIS BRONCHIECTASIS MANAGED WITH TWO WEEKS' INTRAVENOUS ANTIBIOTIC THERAPY
M. Murray, A. Hill. Royal Infirmary of Edinburgh, Edinburgh, UK
Aims: The aim of the study was to assess the efficacy of two weeks’ intravenous antibiotic therapy in patients with non cystic fibrosis bronchiectasis presenting with an exacerbation. Endpoints were sputum microbiology, 24-h sputum volume, FEV1, FVC, distance achieved in the incremental shuttle walk test and cough severity as measured by the Leicester Cough Questionnaire (LCQ).
Methods: Patients presenting with an exacerbation of bronchiectasis between January 2007–June 2007 and received two weeks’ antibiotic therapy were assessed. The antibiotic therapy given was based on current or, if necessary, previous sputum microbiology and all patients received 14 days of antibiotics. At baseline (within 24 h of starting antibiotics) and at the end of antibiotic therapy (day 14) patients had spirometry, shuttle walk test, 24-h sputum collection, sputum sent for microbiological culture and completed the LCQ.
Results: Fifteen patients were treated. The mean (SD) age was 67 (11) years. 80% had pathogens in their sputum at the start of the exacerbation. Sputum bacteriology included Pseudomonas aeruginosa (PA) 46.6%, Haemophilus influenza, Staphylococcus aureus, Moraxella catarrhalis, Escherichia coli and Serratia species 6.7% respectively. Patients with PA received two antibiotics (Ceftazidime and Gentamicin). All other patients received a single antibiotic according to organism sensitivities. Following two weeks’ antibiotic therapy, eradication was achieved in 66.7%, with no significant pathogens identified in the sputum (p<0.005). 13.3% were no longer expectorating sputum. The remaining 20% continued to have the same pathogens isolated from the sputum- in all cases PA. The effects on 24-h sputum volume, FEV1, FVC, incremental shuttle walk test and the LCQ is shown in the table.
Conclusions: Two weeks of intravenous antibiotic therapy in exacerbations of non cystic fibrosis bronchiectasis led to significant sputum bacterial clearance. Despite no improvement in spirometry, there was a reduction in 24-h sputum volume, an improvement in exercise capacity and a reduction in cough severity.
MEASUREMENT OF TREM-1 IN EXACERBATIONS OF BRONCHIECTASIS
R. Siva, W. Monteiro, C. Payne, D. Parker, I. D. Pavord, S. P. Range, C. E. Brightling. Institute for Lung Health, Glenfield Hospital, UK
Introduction: TREM-1 is a glcoprotein expressed on monocytes, macrophages and neutrophils. Its expression is increased on exposure to extracellular bacteria. Raised TREM-1 has been shown to be a predictive biomarker for pneumonia and we have previously measured TREM-1 during exacerbations of COPD. In this study we aimed to investigate the relationship between TREM-1 and markers of bacterial infection and airway inflammation in patients with an exacerbation of bronchiectasis, both before and after antibiotic therapy.
Method: We recruited 17 patients mean (range) age 58 (40–75) with HRCT confirmed bronchiectasis. 11 patients had never smoked, 5 were ex-smokers, 1 currently smoked. On admission we measured spirometry, temperature, WCC, CRP, and symptom score using visual analogue scales. Spontaneous sputum was obtained for culture and we measured sputum colour score, differential cell count, bacterial load, and TREM-1 using an ELISA. These measurements were repeated after 10 days of intravenous antibiotic therapy.
Results: Overall mean bacterial load fell from 3.0×107 cfu/ml to 2.9×106 cfu/ml, p = 0.004. Sputum neutrophil % decreased by 18.5 (95% CI 3.5 to 33.4, p = 0.019). CRP improved by 15.3 (95% CI 0.1 to 30.6, p = 0.049. Symptom score improved from 203.9 to 141.8, mean difference 62.1 (95% CI 25.6 to 98.7, p = 0.003). There was no statistical difference in change in sputum colour score, WCC, or FEV1. Overall TREM-1 increased by 1036.7 pg/ml (95% CI 945.6 to 2999.1, p = 0.28). There was a trend towards an association between change in TREM-1 and change in sputum neutrophil % (r = −0.53, p = 0.061).
Conclusions: There was no significant association between change in TREM-1 and change in bacterial load or neutrophilic airway inflammation during exacerbations of bronchiectasis. The role of TREM-1 as a biomarker for bacterial infection needs further investigation.
THE BURDEN OF LUNG DISEASE IN A COHORT OF PATIENTS WITH PRIMARY ANTIBODY DEFICIENCY ON LONG-TERM IMMUNOGLOBULIN REPLACEMENT
W. N. Lee1, M. J. Thomas2, M. Brownlie2, E. Ross1. 1Department of Respiratory Medicine, Gartnavel General Hospital; 2Department of Immunology, Western Infirmary
Background: Antibody deficiency is a rare cause of recurrent or severe respiratory tract infections. Some patients have persistent respiratory symptoms despite optimal immunoglobulin replacement. We therefore established a joint immunology/respiratory clinic to assess patients receiving immunoglobulin replacement therapy.
Aim: To evaluate the prevalence and pattern of lung disease in our cohort of patients with primary antibody deficiency on long-term immunoglobulin replacement.
Design: A retrospective analysis of clinical data was performed.
Results: Detailed clinical information was available for 48 patients: Common variable immune deficiency (34/48), X-linked agammaglobulinaemia (8), Di George Syndrome (1) and Good’s Syndrome (2). Two patients had drug-induced hypogammaglobulinaemia. One patient had an undefined immunodeficiency. The median age was 44 (range 18 to 88). Six patients were diagnosed before age 16 years. 25 patients were diagnosed between ages 20 and 50 years. 38 patients presented with recurrent lower respiratory tract infections. 17 also had recurrent upper airways infections. Pulmonary function was documented in 40 patients with median FEV1 (% predicted) 97% (range 20% to 102%). Seventeen patents (17/48) had established bronchiectasis, evident on CXR and/or HRCT chest. There was no clear relationship between age at diagnosis and impairment of pulmonary function, or presence of bronchiectasis. Three patients had a nodular pattern of pulmonary disease which mimicked sarcoidosis. The organisms isolated from sputum include Haemophilus influenzae (26/33), Streptococcus pneumoniae (6/33), Moraxella catarrhalis (4/33) and Group C Streptococcus species (1/33). The duration of immunoglobulin replacement ranges from 8 months to 41 years with target trough IgG level >6 g/l. 7 patients had persistent respiratory infections despite optimal immunoglobulin replacement. Five of them were offered an open trial of azithromycin 500 mg three times weekly with clinical improvement in four.
Conclusions: Antibody deficiency should be considered in patients with recurrent upper and lower respiratory tract infections even in the absence of bronchiectasis and impaired pulmonary function. A number of patients have persistent respiratory symptoms despite optimal immunoglobulin replacement. They may benefit from regular azithromycin. A joint approach to the follow-up of these patients may reduce the impact of respiratory infections and allow further study of the natural history of pulmonary disease complicating antibody deficiency.
EFFICACY OF NEBULISED COLOMYCIN IN PATIENTS WITH NON-CYSTIC FIBROSIS BRONCHIECTASIS COLONISED WITH PSEUDOMONAS AEURIGONOSA
R. Dhar, G. Anwar, S. Santana, S. Bourke, G. Afolabi, R. Rutherford. North Tyneside Hospital, UK
Introduction: Nebulised colomycin is frequently employed as an anti-pseudomonal strategy in patients with adult non-cystic fibrosis bronchiectasis but the efficacy of this treatment is unclear.
Methods: Exacerbation frequency, hospital admissions, sputum microbiology and sputum volume were retrospectively recorded in 24 patients who had received at least 6 months’ colomycin therapy between January 2000–April 2007.
Results: Twenty four patients (10 M and 14 F), mean age (SD) 66 years were assessed. Five patients had idiopathic and 19 patients non-idiopathic bronchiectasis. Mean length of data collection pre- and post-commencing colomycin was 21.3 months and 18.9 months respectively. Following at least 6 months’ therapy, sputum volume significantly reduced from 29.0 to 14.6 (p<0.001) ml/day. The frequency of sputum positivity for Pseudomonas aeurigonosa significantly reduced from a mean of 99 days to 307 days (p<0.001) after introduction of colomycin and exacerbation frequency from 46 days to 119 days (p<0.001). The frequency of hospital admissions also significantly declined from 3.16 to 1.08 per year (p = 0.001). Mean FEV1 was well preserved through the duration of observation mean 0.65 L versus 0.67 L (p = 0.96). Only 5 patients had overlapping chronic macrolide therapy. Two patients were intolerant of chronic colomycin therapy.
Conclusion: Nebulised colomycin significantly reduces sputum volume, exacerbation frequency, and hospital admissions in adult patients with bronchiectasis.
CYTOMEGALOVIRUS VIRAEMIA AND BRONCHIOLITIS OBLITERANS SYNDROME
R. L. H. Cowan1, C. T. Leonard2, J. Fildes3, J. Morris2. 1University of Manchester; 2University Hospital of South Manchester NHS Foundation Trust; 3Transplant laboratory, University Hospital of South Manchester, UK
Background: The leading limit to long-term survival in lung transplant (LTx) recipients is chronic rejection. This presents clinically as a progressive decline in lung function referred to as bronchiolitis obliterans syndrome (BOS). Cytomegalovirus (CMV) is a well-recognised pathogen in this population. With quantitative polymerase chain reaction (QPCR) technology, CMV viral load can be calculated and is known to correlate with the development of CMV disease. CMV pneumonitis is a recognised risk factor for the development of BOS. However, there are conflicting data on the effects of prolonged asymptomatic low level CMV DNAaemia on long-term outcomes in LTx patients.
Aim: To determine whether or not the level of CMV DNAaemia is related to development of BOS in LTx patients.
Method: The records of LTx recipients surviving more than 6 months since the introduction of CMV QPCR monitoring were reviewed (n = 116). Exposure to CMV at 3, 6 and 12 months post-transplant was quantified by calculating the area under the curve (AUC) of QPCR results. Percentage decrease in FEV1 at 2 and 5 years was calculated. Total AUC was calculated and standardised for the time over which the samples were collected. Patients were grouped into high and low total CMV exposure groups. Patients with values which were greater than the mean were assigned to the high exposure group (n = 33) and patients with a value less than the mean were assigned to the low exposure group (n = 83).
Results: No significant correlation was found between any of the quantitative measures of CMV exposure and decrease in FEV1 at 2 and 5 years. Kaplan-Meier analysis comparing the time to BOS onset showed no significant difference between the two CMV exposure groups (fig 1). Similar analysis comparing patient survival showed greater survival in patients from the low level exposure group (p = 0.024) (fig 2). Univariate Cox regression analysis also showed increasing CMV exposure to be a risk factor for reduced survival (RR 2.792, 95% CI 1.453 to 5.365, p = 0.002).
Conclusion: In this population, there is no association between CMV DNAaemia and development of BOS. This may reflect the effective action of anti-CMV treatment strategies employed by the centre over the last 9 years. It is also possible that CMV has no role in the development of BOS. Further research is needed in this area if the long-term implications of CMV are to be fully understood.

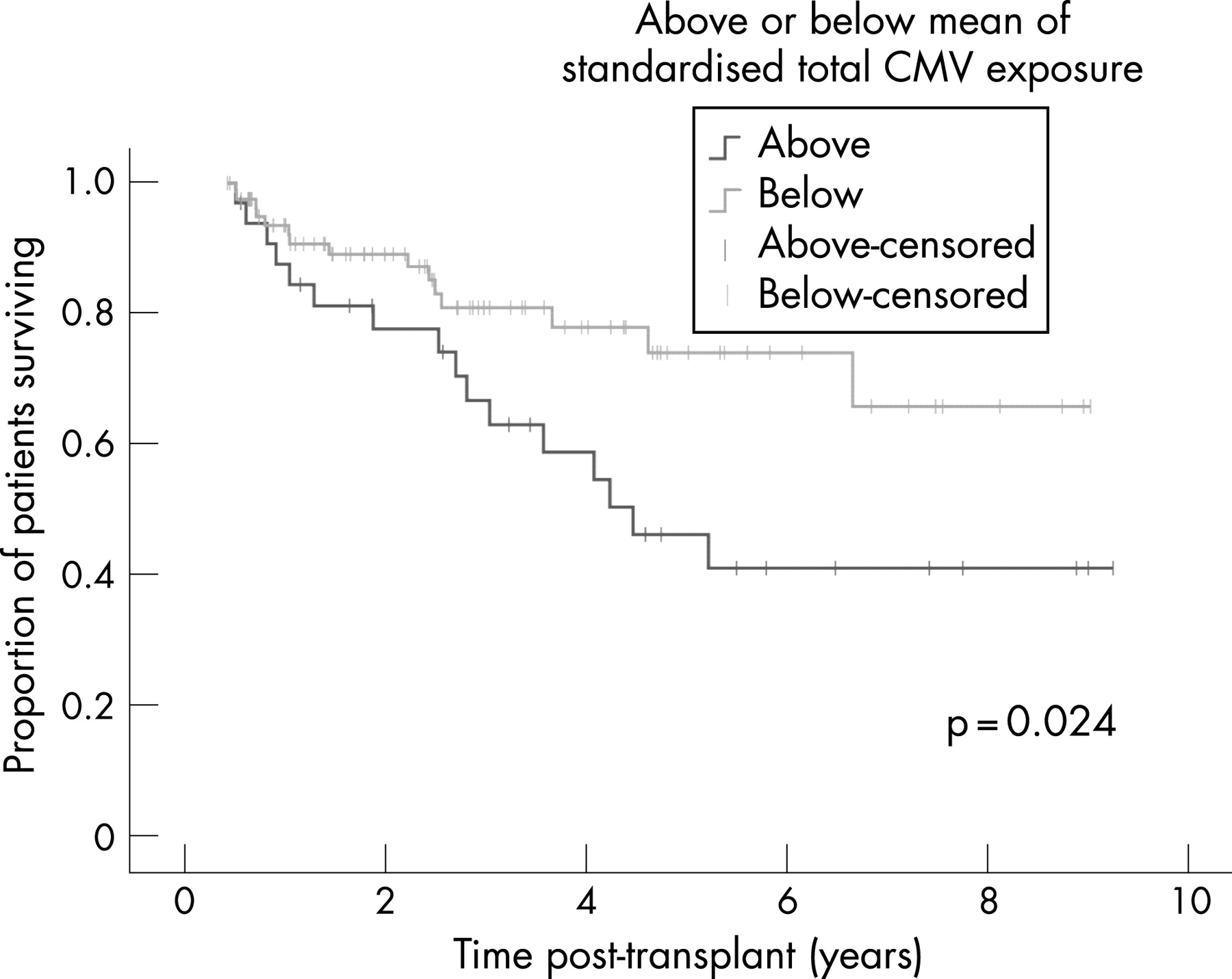
SAFETY AND EFFICACY OF INTRAVENOUS COLISTIN IN COMBINATION WITH OTHER ANTIBIOTICS IN LUNG TRANSPLANT RECIPIENTS
K. Welsh, L. Spencer, B. Isalska, C. Leonard, M. Al-Aloul. Manchester Transplant Unit, Wythenshawe Hospital, UK
Introduction: The increasing prevalence of multidrug-resistant Pseudomonas aeruginosa (Psa) complicates the management of post lung transplant (LTx) bronchial sepsis. Colistin, a polymixin antibiotic to which virtually all Psa isolates remain sensitive, is a potential solution. However, its nephrotoxic potential may limit its intravenous (IV) use in LTx recipients, in whom there is a high prevalence of renal dysfunction secondary to cyclosporin A (CyA). To examine this further, we conducted a retrospective review of our use of IV colistin in LTx between 2005–7.
Methods: Twenty seven patients (13 males, 16 bronchiectasis, 5 emphysema, 6 pulmonary fibrosis, 19 double LTx, 11 abnormal baseline creatinine (mean 189 μmol/l)) received 42 courses of IV colistin (mean daily dose 3 mega units (mU) (range 1–6 mU), mean duration 15 days (range 4–53), total 1972 mU over 639 patient days) at a mean of 671 days (range 0–4269) post LTx. Psa was cultured in 35 episodes and all strains were sensitive to colistin. Colistin monotherapy was used in 4 episodes; IV tazocin, meropenem, ceftazidime and/or ciprofloxacin were added in the remainder. IV Ganciclovir was coadministered in 5 episodes; anti-hypertensives in 7.
Results: All exposures were tolerated well with clinical resolution of sepsis. White cell count (WCC) and C-reactive protein (CRP) improved significantly (p<0.001). Mean (SD) WCC before and after treatment were 12.1 (5.1) and 8.9 (5.0) ×109/l respectively. Corresponding CRP values were 114 (88) and 22 (23) mg/dl. Irrespective of time since LTx, there was no change in renal function during IV colistin therapy; percentage change from baseline in urea, creatinine, estimated glomerular filtration rate from Cockcroft-Gault and the 4-variable Modification of Diet in Renal Disease formulae: −6% (p = 0.419), −3% (p = 0.659), −3% (p = 0.595) and −3% (p = 0.690) respectively. CyA was given at a mean daily dose of 289 (113) mg yielding trough and 2-h post dose serum levels of 201 (81) and 721 (258) ng/ml respectively, in line with current guidelines on immunosuppression dosing.
Conclusions: Our data suggest that IV colistin, in moderate doses over a wide range of treatment duration, is safe and effective in LTx recipients receiving concurrent cyclosporin therapy, and should be considered for microbiologically confirmed gram-negative sepsis.
Respiratory paediatric investigations
CLINICAL PRESENTATION AND COURSE OF HUMAN METAPNEUMOVIRUS IN PAEDIATRIC PATIENTS IN NORTH EAST ENGLAND
J. K. E. Townshend1, J. Clark1, C. O'Brien1, M. Mckean1, C. Taylor2. 1Newcastle Upon Tyne Hospitals NHS Trust; 2Health Protection Agency Laboratory, North East, UK
Introduction: Respiratory infections are a leading cause of morbidity and mortality in the Paediatric population and viruses are among the most common pathogens affecting the respiratory tract of young infants. Despite common respiratory viruses being routinely identified as causative organisms in respiratory infections, there still remains a significant number of viral respiratory tract infections where the aetiology remains undetermined. Human metapneumovirus (hMPV) was identified as a new respiratory pathogen in 2001 in infants with acute respiratory infections and has since been shown to cause respiratory illness through out the world. It is responsible for between 5–20% of respiratory illnesses in hospitalised infants, and as such is second only to respiratory syncytial virus (RSV) as a causative pathogen in this age group. The presentation and clinical course of hMPV has never been described in the UK.
Aims: To determine the clinical presentation and course of hMPV in upper and lower respiratory tract illness in the paediatric population in the North East of England over a one-year period.
Methods: The study was a retrospective case note review of all Paediatric inpatients who detected hMPV from April 2005–April 2006 in the Newcastle Foundation Trust hospitals. During the study period, all respiratory secretions from children admitted to hospital with bronchiolitis or respiratory symptoms were collected and routinely examined by immunofluorescence in the Health Protection Agency in Newcastle-upon-Tyne for hMPV. The patient notes of the 65 confirmed cases of were analysed retrospectively for previously defined characteristics.
Results: Population: 69 paediatric patients detected hMPV in the study period out of a total of 1022 samples tested, suggesting an incidence of 6.7%. Of these, 4 sets of notes were unobtainable, 65 patients were therefore included in the study. The M:F ratio was 1.8:1 with a median age 10 months (range 1–201 months). The median birth gestation was 39 weeks (range 24–42). 38% (25) had pre-existing comorbidity, 48% of which were respiratory (chronic lung disease, structural airway abnormalities, wheezing episodes) and 24% of which were neurological. Clinical presentation: 89% of isolations occurred between Nov-June with the highest frequency between December–April. There were, however, isolations through out the year. Cough was the most common presenting symptom (55/65), followed by breathlessness (33/65) and elevated temperature (32/65). Other common presentations included coryza (19) and wheeze (17). At presentation, the mean heart rate and respiratory rate were 18 bpm and 55 bpm higher respectively than average for the age of the child. The median saturations were 92% (SD 6.8%) and the mean temperature was 37.5°C (SD 0.14°C). Initial diagnosis was thought to be either LRTI (40%), Bronchiolitis (34%), URTI (14%) or episodic viral wheeze (6%). Clinical course: The median duration of illness (defined as days of illness prior to presentation until day of discharge) was 7 days (range 2–44 days). The maximum recorded temperature was 38.3°C (SD 0.13°C). 64% of children needed supplementary oxygen for a median duration of 3 days (range 1–17 days), 88% of these required greater than 2 l/min. 57% of patients (37) needed feeding support either in the form of NG or IV fluids. 17% (11) of children required respiratory support in the form of ventilation. Of these 64% had a pre-existing respiratory pathology, compared with 28% of the total population. A child was not more likely to be ventilated if a second pathogen was isolated, however, although only 3 children isolated both RSV and hMPV, 75% of these children required ventilation. 46 children received antibiotics.
Discussion: This study is the first to describe the clinical presentation and course of hMPV in the UK. It has investigated the presence of hMPV in all samples, not solely negative samples as in other studies and as such provides a more accurate representation of the true incidence of the virus in our population. In addition we have reported on isolations through out the year, confirming the peak incidence in December–April, but showing isolations throughout the year. Clinical characteristics reported in previous studies were similar in our population, for example age at presentation and most common presenting symptoms of cough and coryza. However, more than one third of our population had a pre-existing medical illness, which does not support the findings of other studies, that hMPV affects mainly healthy children. Some previous studies have reported an increase in disease severity with co-infection with RSV. Only 3 children in our population isolated both hMPV and RSV, making observations of disease severity in this group difficult, however the dramatic increase in ventilation rates in this subgroup suggests the possibility of RSV as a marker for more severe disease. In conclusion, our study supports previous findings that hMPV is a significant respiratory pathogen in children under 1 year of age.
SELECTED ION FLOW TUBE MASS SPECTROMETRY BREATH ANALYSIS IN CHILDREN: BAG OR BOX?
B. J. Enderby2, P. C. Boit2, W. Lenney2, P. W. Jones1, D. Smith1. 1Keele University; 2University Hospital North Staffordshire, UK
Introduction: The paediatric lung remains somewhat of a black-box. The tools that we have to monitor it are imprecise and lack sensitivity. We desperately need a sensitive, non-invasive technology to provide us with information about physiological and pathological changes occurring within children’s lungs. Selected ion flow tube mass spectrometry (SIFT-MS) offers the potential to identify volatile organic compounds (VOCs) that may act as surrogate biomarkers of infection and inflammation. This technique is non-invasive, highly senstitive and can provide on-line data. SIFT-MS is increasingly being used in adults in various disease-states. It has rarely been used in children. The first step is to establish sound methodology that allows gas beyond the dead-space in the respiratory tract to be sampled consistently. This requires slow, controlled inhalations and exhalations, which younger children often find difficult to achieve. In those unable to comply, we have been using specially-designed Nalophan bags to collect samples of breath. We have compared data collected by children breathing directly into the SIFT-MS instrument with breath samples collected in the Nalophan bags.
Study Design: Twenty four healthy children with a mean age of 10 years provided on-line breath samples, followed by Nalophan bag samples. The bag samples were incubated at 37°C during their analysis. The concentrations of VOCs were calculated using the on-line SIFT-MS kinetics database. The table summarises the findings for three VOCs; acetone, ammonia and isoprene. The video demonstrates the two sampling techniques required to obtain the data.
Conclusion: These data are comparable to those found in healthy adults for acetone and ammonia but the mean isoprene concentration (a marker of cholesterol synthesis) is markedly lower. The greatest standard deviation is seen in the bag ammonia concentration, which could be explained by cooling and subsequent condensation of this highly soluble gas. Variation of specific VOC concentrations is considerable. This may be due in part to intra-patient variation owing to variable technique. This may be due to between and within-patient technique but may also be due to natural biological variation. An individual’s variation in VOC profile over time would be more informative and we are pursuing such studies in healthy children and in those with asthma and cystic fibrosis. The use of an incentive device in training children to breathe in a controlled way into the instrument may also be of benefit.
MEASURING MARKERS OF OXIDATIVE LUNG INJURY IN CHILDREN USING SELECTED ION FLOW TUBE MASS SPECTROSCOPY
B. J. Enderby, P. C. Boit, W. Lenney, P. W. Jones. University Hospital North Staffordshire, UK
Introduction: Selected ion flow tube mass spectrometry (SIFT-MS) is an exciting new advance in breath analysis. This highly sensitive and non-invasive technique offers the possibility of identifying volatile organic compounds (VOCs) in breath which may act as surrogate biomarkers of disease. SIFT-MS is being used increasingly in adult medical research. We are one of only two centres worldwide using it in children. Before using SIFT-MS in children with chronic lung diseases, we felt that the quantification of breath constituents in healthy children was an essential starting-point. In this study, we looked at the concentrations of several key VOCs in order to determine their mean values and absolute range.
Study Design: Twenty two children provided on-line breath-samples on three consecutive occasions within an 8-h time period. A simple counting technique was used to encourage them to breathe in controlled inspiratory and expiratory cycles. The concentrations of VOCs present, were calculated using the on-line SIFT-MS kinetics database. The results are shown below, with adult reference ranges listed for comparison.
Results: Data for all VOCs studied (except for isoprene) are comparable with that from healthy adults. Isoprene levels are markedly lower in children. Although the origin of isoprene in breath is not clearly understood, it is considered to be a by-product of cholesterol synthesis and also a marker of oxidative lung damage. As with adult data, the within-patient variation in mean isoprene levels was wide. The coefficient of variation for isoprene was 173%, compared to only 46% for acetone.
Conclusions: While isoprene has been shown to have its own circadian rhythm and also to vary during exercise, the reason for this wide variation within subjects is not fully understood. We are now conducting longitudinal studies to monitor the concentrations of isoprene and other VOCs in children with cystic fibrosis and asthma, to see if this and other surrogate biomarkers of inflammation and infection can be identified at elevated levels.
FACTORS INFLUENCING CHANGE IN PEAK EXPIRATORY FLOW DURING CHEST PHYSIOTHERAPY IN MECHANICALLY VENTILATED CHILDREN
R. K. Gregson1, 2, 3, H. Shannon1, E. Main1, E. Main2, J. Stocks1. 1Portex Anaesthesia, Intensive Therapy and Respiratory Unit, UCL Institute of Child Health; 2Physiotherapy Department, Great Ormond Street Hospital for ChildrenNHS Trust; 3School of Medicine, University of Southampton
Background: One of the aims of chest physiotherapy in ventilated subjects is to increase peak expiratory flow (PEF) and expiratory flow bias, thereby mobilising secretions towards the oropharynx for removal by suction. Effectiveness of physiotherapy is likely to be influenced by interactions between the timing, magnitude and pattern of chest wall vibrations and lung inflations.
Aim: To investigate factors influencing change in PEF during physiotherapy in mechanically ventilated children.
Methods: Physiotherapy forces and simultaneous changes in airflow were measured in ventilated children, using a novel lightweight force-sensing mat and respiratory profile monitor.1 Repeated measures ANOVA compared respiratory data collected during baseline ventilation prior to treatment, with those obtained during manual inflations with and without vibrations. Multiple linear regression was used to predict the relative contribution of age, body weight, inflation volume and vibration force on PEF in the presence and absence of chest vibrations. Expiratory flows predicted from these equations were compared with observed values, both within and between subjects.
Results: Measurements were made in 55 ventilated children (median age 1.6 years (range 1 week–13.7 years)). PEF increased significantly from baseline during lung inflations (mean % change (95% CI 34% (19 to 50%)) increasing further with force application (129% (106 to 152%), p<0.05). After correcting for body weight, the increase in PEF was significantly related to magnitude of applied force and inflation volume (VI) and inversely related to age (p<0.001 for all). Thus the effect of force was greater in younger children with, for example, application of 60N force increasing PEF by, on average, 1.38 l/min/kg in those <2 years, but by only 0.24 l/min/kg in older children.

Discussion: Use of this novel method of assessing applied force and simultaneous respiratory changes during treatment, provides the means of objectively assessing why some treatments enhance respiratory function whilst others do not, which could be used both in clinical management and research. The increased efficiency of force application in younger subjects is probably related to the higher chest wall compliance in this age group.2
Funding: Sport Aiding Medical Research for Kids (SPARKS), Physiotherapy Research Foundation, Great Olmond Street Hospital Research Fellowship.
A CASE-CONTROL STUDY OF OBSTRUCTIVE SLEEP APNOEA HYPOPNOEA SYNDROME DEMONSTRATED LEFT VENTRICULAR HYPERTROPHY AND LEFT ATRIAL DILATATION IN SUBJECTS WITHOUT KNOWN CARDIAC DISEASE
S. Kesavan, A. Malin. Royal United Hospital, UK
Introduction: Obstructive sleep apnoea hypopnoea syndrome (OSAHS) is associated with an increased cardiovascular morbidity and mortality due to the occurrence of heart failure and cardiac arrhythmias. But there is a paucity of literature concerning the effect of OSAHS on left atrial and left ventricular structure prior to the development of symptomatic heart disease. We carried out an echocardiographic study designed to identify left heart changes specific for OSAHS patients without known cardiac disease.
Methods: The control group included 45 obese patients with no clinical evidence of OSAHS and were matched for age, gender, blood pressure and body mass index (BMI). The study group involved 45 patients with a clinical diagnosis of OSAHS. The diagnosis of OSAHS was based on an overnight pulse oximetry and clinical assessment. Patients underwent transthoracic echocardiography for the measurement of left atrial size (LA), left ventricular end systolic (LVESD) and left ventricular end diastolic dimensions (LVEDD). Exclusion criteria included evidence of heart failure, atrial fibrillation and other cardiac arrhythmias, cerebrovascular accident, valvular heart disease, ischaemic heart disease, pregnancy and hyperthyroidism.
Results: Subjects with OSAHS when compared to controls, demonstrated an increase in the LA size (>4.2 cm, p = 0.0001, 95% CI 0.36 to 0.94) and an increased LVESD (>3.76 cm, p = 0.0002, 95% CI 0.29 to 0.90) and LVEDD (5.4 cm, p = 0.005, 95% CI 0.0002 to 0.6002). Hypertrophy of the interventricular system (>1.1 cm, p = 0.004, 95% CI 0.04 to 0.20) and the posterior wall (>1.1 cm, p = 0.0005, 95% CI 0.1001 to 0.2600) were also noted.
Conclusion: OSAHS was strongly associated with an increase in the left atrial and left ventricular dimensions. OSAHS appears to be a significant independent predictor of left atrial dilatation and left ventricular hypertrophy when compared to controls. This may be due to an increased afterload and transmyocardial wall stress associated with the direct effect of chronic recurrent apnoeic episodes over a prolonged period of time. The coinciding epidemics of obesity and atrial fibrillation underscore the clinical importance of these results.
SLEEP-RELATED DISORDERED BREATHING IN CHILDREN WITH CROUZON SYNDROME
S. Al-Saleh, A. Riekstins, C. Forrest, J. H. Phillips, I. Narang. The Hospital for Sick Children, UK
Background: Crouzon syndrome (craniofacial dysostosis) is an autosomal dominant genetic disease associated with craniofacial malformations including maxillary hypoplasia, craniosynostosis, hydrocephalus and chiari malformation. Sleep-related disordered breathing (SRDB), specifically obstructive sleep apnea (OSA) has been described in a few case reports; most of these reports did not include assessment by polysomnography (PSG)
Aim: To evaluate the prevalence and severity of SRDB in children with Crouzon syndrome
Methods: We undertook a retrospective chart review of 16 patients with Crouzon syndrome who were referred for a sleep study due to symptoms suggestive of OSA including snoring. All data from PSG were analysed including age, weight, height, BMI, obstructive apnoea-hypopnoea index (AHI), central apnoea index (CAI), sleep latency and efficiency, mean oxygen saturation (SaO2) and transcutaneous carbon dioxide (TcCo2) readings.
Results: Sixteen patients (8 females) had their first PSG at mean age 4.7 years (range 1–12.7 years). The mean weight was 19.2 (range 8.2–60.7), mean height was 100.4 (range 76–154) and mean BMI was 17.4 (range 13.3–25.6). The mean sleep latency was 9.6 min and mean sleep efficiency was 85.9%. Out of 16 studies reviewed, 12/16 patients (75%) had evidence of SRDB. The mean AHI was 12.1 (range 0–62) and mean CAI was 3.5 (range 0–45). The maximum SaO2 ranged between 95–100% and minimum SaO2 sat ranged between 50–94%. The TcCo2 ranged between 28–60 mmHg.
Conclusion: Children with Crouzon syndrome had normal sleep efficiency. However, this retrospective chart review confirms a high prevalence of SRBD, specifically moderate to severe OSA in this population. Children with Crouzon syndrome with any history of snoring should be referred for polysomography to evaluate for SRBD.
ACHIEVING COMPLIANCE IN THE NON-COMPLIANT PAEDIATRIC PATIENT REQUIRING NOCTURNAL NON-INVASIVE PRESSURE VENTILATION: A FAMILY-CENTRED APPROACH
A. M. Riekstins, M. J. Castellarin, A. Baker, I. Narang. Hospital for Sick Children, UK
Non-invasive positive pressure ventilation (NIPPV) is a treatment option for both nocturnal hypoventilation and obstructive sleep apnea in children who are not suitable or do not respond to surgical or medical intervention. Recent literature has shown the benefit of NIPPV therapy in both long-term outcomes and improvement of quality of life Thus initiating and maintaining NIPPV is of clinical significance. However, adherence to NIPPV is an ongoing challenge in the paediatric population. Compliance may be compromised due to intolerance of the NIPPV interface, limited anticipatory guidance or inadequate child and family education. Often the plan of care is not patient or family centred, leading to a less than successful intervention.
At the Hospital for Sick Children, we report a case series of 10 children with chronic morbidity, all deemed to require NIPPV by polysomnogram but without successful institution of NIPPV. Following the institution of an Advanced Practice Nurse and Respiratory Therapist led Compliance Clinic; all 10 patients were successfully established on NIPPV as shown with monitoring using simultaneous polysomnogram. The foundation of the NIPPV compliance clinic is patient centred. The clinic includes initial patient and family education, followed by a two-week trial at home with a NIPPV mask. During these two weeks, open communication and frequent follow-up via telephone occurs to optimise strategies to improve patient compliance. After a two-week period, the patient will undergo a trial of NIPPV therapy overnight with simultaneous polysomnogram in the sleep centre under the close supervision of a respiratory therapist and a sleep technologist. Using these strategies, NIPPV, even in the most challenging cases has proven to be a successful.
This abstract will specifically address our patient and family-centred approach toward NIPPV initiation and suggests strategies which health care providers can apply in clinical practice.
DOES HYPOXIC CHALLENGE AT SEA LEVEL CORRELATE WITH HYPOXIA IN FLIGHT AND AT ALTITUDE IN HEALTHY CHILDREN?
E. Scrase1, A. Laverty1, S. Sonnappa2, J. C. D. Gavlak1, J. Stocks2. 1Great Ormond Street Hospital for Children; 2Institute of Child Health, UK
Background: Modern aircraft are pressurised up to 2438 metres, equivalent to breathing 15.1% oxygen. A hypoxic challenge in a body plethysmograph is recommended in children with lung disease to assess fitness to fly with or without supplemental oxygen. There is a lack of data on the range of normal desaturation in children during air travel, and studies on healthy subjects have been recommended.
Methods: Nine healthy children mean age 9 (range 6–13) years had oxygen saturation and heart rate monitored by pulse oximetry (Minolta Pulsox 300) while breathing 15% O2 in the plethysmograph for 20 min. Pulse oximetry was repeated at rest on the flight and at a similar altitude in Nepal during a trekking holiday.
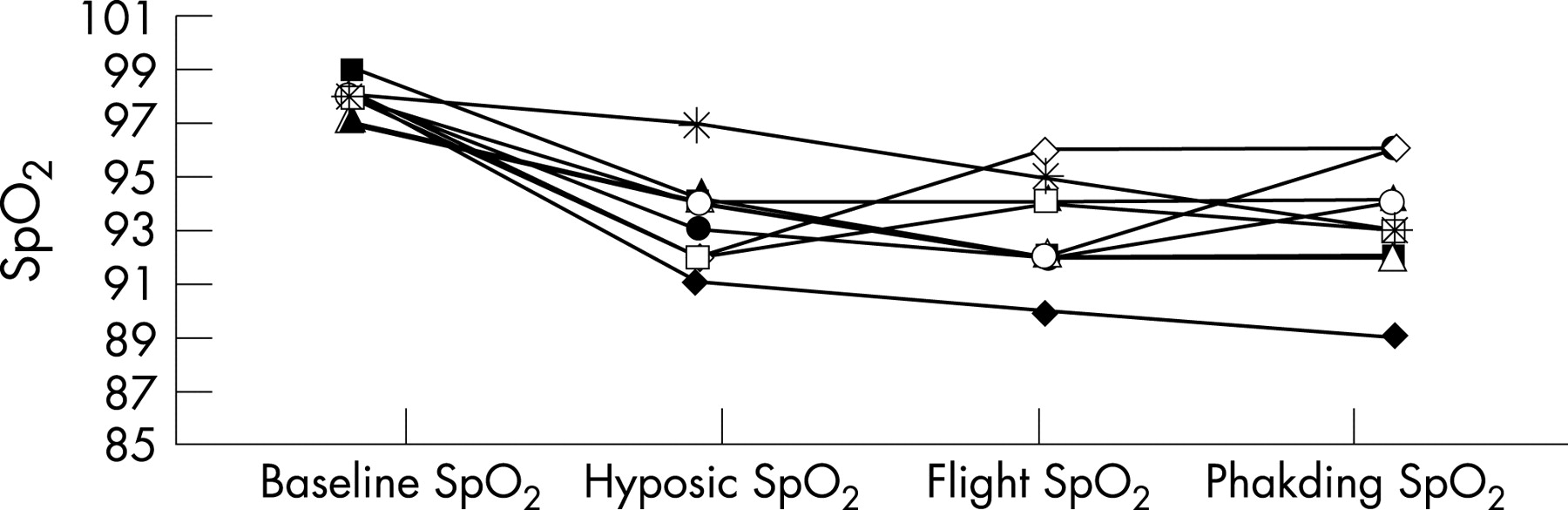
Results: There was marked variability in response to the laboratory hypoxic challenge, but no child desaturated below 90%, the cut-off for supplemental oxygen during pre-flight assessments of children with lung disease. In comparison with baseline levels, SpO2 was significantly lower during the hypoxic challenge (median difference −5.0%, IQR −3.0 to −6.0; p = 0.008), during the flight (median difference −5.0% IQR −3.0 to −6.5; p = 0.008), and at Phakding (median difference −5.0% IQR −2.5 to −6.0; p = 0.007). The child with the lowest desaturation during the hypoxic challenge remained the lowest during the flight and at altitude, but among this small group of healthy children, there was no significant relationship between oxygen saturation during the hypoxic challenge and that recorded during the flight and at altitude in Phakding.
Conclusion: There is a reduction in oxygen saturation during air travel and at altitude in healthy children. While the hypoxic challenge did not predict the degree of desaturation during the flight or at altitude, among this small group of healthy children, it correctly classified all nine as fit to fly.
Tuberculosis diagnosis and management
EFFECT OF THE NICE TUBERCULOSIS GUIDELINES 2006 ON CONTACT TRACING AND NURSING WORKLOAD IN SE LONDON
O. Emanuwa, H. J. Milburn. GKT Medical School, King's College London, UK
Introduction: Before publication of the National Institute for Health and Clinical Excellence (NICE) Guidelines for management of tuberculosis (TB) in March 2006, tracing of contacts of index cases of TB followed the British Thoracic Society (BTS) Guidelines. The BTS recommended screening of close contacts of cases of smear positive and negative pulmonary TB (PTB) but not routine screening of contacts of non-pulmonary disease (NPTB). NICE, however, recommends screening of “household contacts of any person with active TB, irrespective of the site of infection.” The aims of this study were to determine whether this change in recommended practice had: (1) significantly increased contact tracing activity; (2) identified more cases of active TB; and (3) increased numbers prescribed chemoprophylaxis.
Methods: Data were collected on PTB and NPTB index cases notified between 1 October 2005 and 31 September 2006 and their contacts. These were split into two groups: (A) those notified between 1 October 2005 and 31 March 2006 (before NICE); and (B) those notified between 1 April 2006 and 31 September 2006 (following NICE). We measured numbers of contacts screened; given a tuberculin skin test (TST) &/or CXR; referred to a doctor; treated with chemoprophylaxis; given BCG vaccination; discharged with advice (DCWA); failed to attend 3 consecutive appointments (FTA×3). We also estimated the average time spent by nurses on each contact tracing procedure
Results: A total of 188 index cases and 518 contacts were assessed. In Group A 189 contacts of 106 index cases were screened (1.79 contacts/index) and in Group B 319 contacts of 82 index cases (3.9 contacts/index; p<0.01). In Group A 33% of index cases were NPTB while 43% were NPTB in Group B.
No additional cases of active TB were identified in either Group A or Group B. Following the NICE Guidelines, more contacts were seen by the TB nurses. This led to increased numbers receiving TST and CXR but not an increase in proportions having a CXR. There was no increase in prescriptions for chemoprophylaxis but greater numbers given BCG vaccination. The rate of failure to attend also increased.
Nurses measured the total mean time taken to trace one contact (including telephone calls, filling in forms) as 77.5 minutes. This meant that the increased numbers traced following introduction of NICE resulted in 168 extra hours worked in 6 months or 8 weeks 2 working days over a year.
Conclusion: Implementation of the NICE Guidelines resulted in increased workload for the TB nurses with no associated increase in detection and treatment of active cases of TB, but increased rates of BCG and education may improve prevention in the long term. The cost of implementing NICE needs to be addressed.
EVALUATION OF A ROUTINE WHOLE-BLOOD INTERFERON-GAMMA ASSAY IN A HOSPITAL-BASED POPULATION FOR THE DIAGNOSIS OF LATENT TUBERCULOSIS INFECTION
N. E. Costa-Gomes1, M. J. Pavitt1, J. Groth2, C. F. J. Rayner3. 1St George's University of London; 2St George's NHS Trust, London, UK
Background: Both preventing and predicting the progression of Mycobacterium tuberculosis (MTB) from its latent to active form of infection is vital to any effective control programme. QuantiFERON-TB Gold (QFT-G: Cellestis Ltd, Carnegie, Australia), an interferon gamma release assay, has recently been developed to improve latent MTB detection.
Objective: The aim of this study was to assess the efficacy of QFT-G in comparison to the tuberculin skin test (TST) in patients presenting with possible latent TB infection (LTBI), evaluating the use of QFT-G as a sequential test to a positive or borderline TST in line with NICE guidelines (NICE, March 2006).
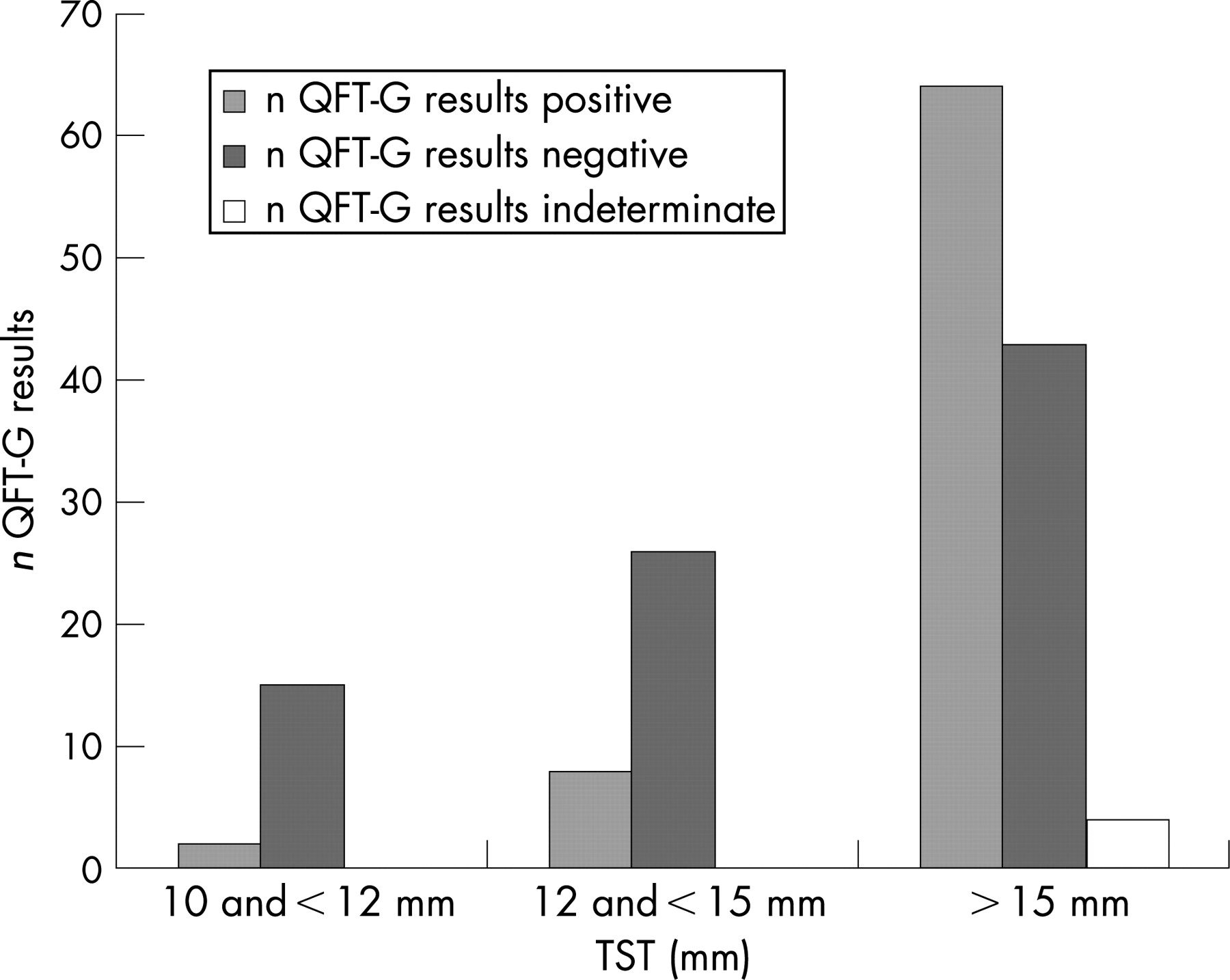
Methods: 280 patients were seen over an 11-month period from a UK hospital. 82 were excluded due to either declining a Mantoux test, a skin induration diameter of less than 10 mm. Of the 198 remaining subjects, 23 were immunocompromised and 13 were symptomatic but Mantoux negative. These cohorts were analysed separately. The main outcome measure was the percentage agreement between the two tests in the various subpopulations (BCG status, contacts, healthcare workers, immunocompromised and symptomatic but TST negative).
Results: The cumulative agreement between the TST and QFT-G in the 162 subjects was 45.7% with 84 of the OFT-G results being negative. Concordance increased if results were analysed separately according to size of reaction with 57.7% agreement in TST results >15 mm (see fig). This was more evident among the 60 contacts (65% concordance with TST >15 mm). There was a 46.1% (BCG positive) and 47.8% (BCG negative) agreement between the tests according to BCG history. Healthcare workers represented a small population with the lowest concordance. 56 patients had available culture results, the QFT-G showing greater concordance than the TST. Interestingly, 2 patients with confirmed non-tuberculous mycobacterial infection had negative QFT-G results. Among the immunocompromised cohort a negative QFT-G result was found in 82.6% of cases and indeterminate results were 3.47 times more likely than in the immunocompetant group. From these data, the QFT-G would have treated 84 fewer subjects with a total saving of £21,235.
Conclusion: We report here the results of a UK hospital-based study of QFT-G testing in standard practice. The evaluation of the QFT-G as a sequential test to a positive TST has shown that the TST overestimated the number of MTB cases in comparison to the QFT-G. The use of the QFT-G can prevent the unnecessary treatment of patients with potentially harmful therapeutics. The overall concordance between the two tests was lower than found in many controlled trials indicating that in a population with a variety of probabilities of LTBI, specificity is compromised. In addition, it was found that the QFT-G produced a greater proportion of negative and indeterminate results in immunocompromised patients. This occurred despite a higher concordance with cultures than the TST, indicating that although QFT-G may not function optimally in this subset of patients, it probably performs better than TST. Further work is required to determine the place of QFT-G in the screening of contacts and healthcare workers, especially in terms of the effect of serial testing.
SENSITIVITY, SPECIFICITY AND JUSTIFICATION OF THE T-SPOT TB ASSAY CUT-OFF USING RECEIVED OPERATOR CHARACTERISTIC (ROC) ANALYSIS
I. Durrant, J. Pullen, C. Granger. Oxford Immunotec, UK
Introduction: T-SPOT®.TB, one of the new blood-based diagnostic assays, enumerates T cells specific for antigens secreted by the Mycobacterium tuberculosis complex. This test has been shown to detect both active and latent forms of the disease.
Methods: In order to justify a cut-off for reactivity based on a spot count threshold, samples were collected from culture confirmed tuberculosis (TB) patients (n = 185) and from patients with a medical history indicating a very low possibility of TB exposure (n = 485). The data were analysed using the received operator characteristic (ROC) method.

Results: A cut-off of >5 spots/250000 PBMC (for a reactive result) was justified and the area under the curve (AUC), indicating the degree of confidence in the ROC analysis, at this cut-off, was 0.987. The spot count range was generally from 5 to >200 spots for confirmed TB cases and between 0 and 7 spots for uninfected controls. The overlap (covering <4% of results) of the bimodal sample data ranges indicated a “grey zone” where the result should be considered as borderline (5–7 spots). Sensitivity and specificity were calculated as 96.0% and 99.1%, respectively. A frequency histogram of spot counts for suspected LTBI cases (n = 4180 samples) was compared to the frequency histogram of spot count results for active TB and low risk controls. The suspected LTBI sample spot counts demonstrated a similar bimodal distribution pattern to that seen with known cases, as expected from a test intended to aid discrimination between LTBI suspects that are truly infected and those who are not. The overlap point, or cut-off, was exactly analogous to the overlap point observed between active TB cases and low risk controls.
Conclusion: This is the first description of the statistical justification for the cut-off for one of the new blood-based TB tests. The introduction of a grey zone for borderline results appears to be justified. The overlap in spot count value distribution curves for those with a confirmed TB diagnosis compared to LTBI suspects indicates that both assay cut-off and sensitivity and specificity claims, based on confirmed cases, can be extrapolated to LTBI diagnosis with a high degree of confidence.
A COMPARISON OF INTERFERON-GAMMA RELEASE ASSAYS AND DIAGNOSTIC ALGORITHMS FOR LATENT TUBERCULOSIS
M. P. R. Berry1, M. I. Y. Wickremasinghe1, J. Merritt1, K. Pike1, S. Wattam1, M. Mercer1, S. R. Anderson2, A. Jepson1, O. M. Kon1. 1St Mary's Hospital; 2North West London Health Protection Unit, London, UK
Rationale: Accurate identification and preventative treatment of individuals at risk of developing active tuberculosis (TB), known as latent TB infection, is fundamental for the control of this disease. Recent guidance has suggested the use of novel Interferon Gamma Release Assays for the diagnosis of latent infection, either alone or following a positive tuberculin skin test.
Objectives: We wished to compare the two commercially available assays in a standard UK contact tracing investigation and to interpret the results according to both of the proposed testing models.
Methods: We compared the results of testing with skin test, and two different assays: Quantiferon-TB Gold In-Tube and TSPOT.TB in the context of a routine point source contact tracing investigation of 117 individuals.
Results: Screening using the test followed by a confirmatory assay allowed a reduction of over 75% in the number of individuals identified as having latent infection (see table). Different individuals were identified as infected by each assay and overall agreement between assays was only slight (κ = 0.19, p = 0.045). In all those who were skin test negative but assay positive and were re-tested at 3 months we observed reversion of the assay response to negative.
Conclusion: It is unclear which assay, if any, could be used as a sole test for the identification of latent infection. We recommend the use of a two-step approach using skin test followed by assay, or vice versa.
THE DIAGNOSTIC EFFICACY OF FINE NEEDLE ASPIRATION UTILISING CYTOLOGY AND TB CULTURE IN TUBERCULOUS LYMPHADENITIS
E. P. Asimacopoulos, M. Berry, M. Roesner, M. O'Donoghue, A. Jepson, J. Mccarthy, O. M. Kon. St Mary's Hospital, London, UK
Objective: To retrospectively assess the efficacy of fine needle aspiration utilising cytological and microbiological examination as a diagnostic tool in tuberculous lymphadenitis in the setting of a central London teaching hospital.
Methods: Patients reported to the London Tuberculosis Register with tuberculous lymphadenitis by St Mary’s Hospital, London, between the period of January 2001 and June 2007, were identified. Using the hospital computerised databases, the cytopathological and microbiological reports of 108 of these patients were found. The criteria for a diagnosis of TB lymphadenitis was based on a compatible clinical history, tuberculin positivity and either a indicative cytological result or positive microbiology.
Results: In 82 of the 108 (76%) cases, fine-needle aspiration cytology (FNAC) showed evidence of a tuberculous process (ie, granuloma formation with or without caseation). In 62 cases, Mycobacterium tuberculosis was cultured from the fine-needle aspirates, and 47 of these 62 (76%) cases showed corresponding cytological evidence of a tuberculous process. There were 33 cases (31%) which were diagnosed by cytology but not microbiology, and conversely 15 cases (14%) which were diagnosed by microbiology but not microbiology. Twelve of the 108 cases (2%) had inadequate cytological findings. It was found that four of these 12 fine needle aspirates were performed by a clinician, five by a radiologist and two by a cytologist.
Conclusion: In our retrospective analysis, cytological and microbiological results correlated well, but each still gave an exclusive diagnosis of tuberculous lymphadenitis in our cohort. When combining both modalities, the diagnostic efficacy of fine needle aspiration rises to 88%. A definitive microbiological diagnosis was achieved in 57% of the cases and had the added advantage of supplying drug sensitivity data. We therefore conclude that samples should be provided for both cytological and microbiological examination when using fine-needle aspiration to diagnose possible tuberculous lymphadenitis. This study also identified that some excision biopsies may not be warranted and that the adequacy of samples may be operator related.
SPINAL TUBERCULOSIS: A DIAGNOSIS NOT TO BE MISSED—A REVIEW OF CASES
A. M. Sutcliffe1, H. Morton2, A. M. Anderton2, U. C. Leivers2, J. T. Macfarlane2. 1University of Nottingham; 2Nottingham University Hospitals NHS Trust, UK
Introduction: Spinal tuberculosis (TB) is uncommon, presentation may be insidious and result in delays and serious complications.
Methods: We set out to determine whether there were any “red flag” features at first presentation, any avoidable delays in management and if management concurred with current (BTS/NICE) guidelines, by reviewing 15 available records for all 16 patients treated for spinal TB at two large UK teaching hospitals during a 5 year period.
Results: For the 15 cases, the mean age was 40 years (range 1–86); 6 female; ethnic origins, Caucasian (4), Indian subcontinent (6), Sub-Saharan Africa (5, including the 3 HIV positive cases). The patients were referred to 6 different specialties initially, 9 via their GP, 4 via emergency department, 2 were inpatients for other reasons at symptom onset. Eleven patients had red flag features at presentation, including 8 referred urgently via GP; 5 after first GP consultation, but 3 after GP contact for 86, 139 and 184 days. Spinal imaging involved 13 MRI and 4 CT scans; only 5/15 chest x-rays were abnormal. Seven patients had a biopsy and 5 an aspirate from the affected area. Diagnosis was microbiological in 10 patients (8 biopsy/aspirate, 1 bronchial washings, 1 cerebrospinal fluid), histological in 2 patients and clinico-radiological in 3; 6 patients had TB at other sites, including all 3 HIV positive patients. All 9 patients without neurological involvement were treated for 6–12 months; 5/6 patients with neurological involvement for 12 months. Four patients had residual neurological deficit and 2 persistent spinal deformity. One patient required spinal surgery.
Conclusion: Most patients were referred urgently by their GPs, and had red flag features present, but with delays in 3/8 cases. Referrals occur to a variety of specialties, and diagnosis is difficult, requiring specialist imaging and sampling and a microbiological/histological/clinico-radiological diagnostic approach. Practice appears to be to treat for up to 12 months and there is a significant complication rate. As cases of extrapulmonary TB are increasing in the UK and most patients do not have co-existing pulmonary TB, a high index of suspicion is needed, especially in “at risk” groups.
CONTACT TRACING IN AN HIV POSITIVE POPULATION: A COMBINED APPROACH USING MANTOUX, GAMMA INTERFERON ASSAY (T-SPOT TB), CHEST X RAY AND SYMPTOM QUESTIONNAIRE
L. V. Baker1, R. Enuechie2, A. Nundoll2, R. Royal2, C. Mazhude1. 1University Hospital Lewisham; 2Lambeth, Southwark and Lewisham Community TB team, London, UK
Introduction: Tuberculosis (TB) contact tracing in an HIV positive population is notoriously difficult. Anergy to tuberculin skin testing is reported in 10–50% of patients with a well preserved CD4 count, and 80–90% of individuals with CD4 counts <200. Radiological features of active pulmonary TB may be subtle, and extrapulmonary disease is common. Patients who have received prior BCG vaccination may have a falsely positive tuberculin test. The NICE guidelines (March 2006) recommend use of gamma-interferon based assays in this population.
Methods: We performed contact screening in an HIV outpatient clinic following exposure to infectious pulmonary TB. Immunocompromised contacts (CD4 count <350) at risk were identified using the Interdepartmental Working Group on Tuberculosis guidelines—the control of TB in the UK (1998) and screened 6 weeks after last contact using Mantoux test (10TU), Tspot-TB assay (Oxford Immunotec), chest x ray and a symptom questionnaire. Indeterminate or borderline Tspot-TB assays were repeated after a further 6 week interval.
Results: 74 patients attended. 46(62%) were African, 60 (81%) had prior BCG vaccination, CD4 counts at the time of screening ranged from 4–611, median 280. 11 patients had symptoms, 10 had abnormal CXR. 73 Mantoux tests were performed, 68 were read (16 measured >14 mm, 5 measured 6–14 mm, 43 were 0 mm). 72 T-spot tests were performed (15 reactive, 46 non-reactive, 6 borderline, 4 indeterminate). 67 patients had both Mantoux and Tspot-TB testing. The combined results are shown in the table. Patients with symptoms or an abnormal CXR were investigated. Only 1 Tspot-TB test remained indeterminate on retesting. Indeterminate test results were associated with CD4 counts above 200. Anergy was identified in 4 patients (5.5%), all of whom had CD4 counts above 200, 38 patients had true negative Mantoux tests (0 mm, non-reactive Tspot-TB), 5 patients (6.9%) had probable false positive Mantoux reactivity, all had received prior BCG. 16 patients were offered chemoprophylaxis (2 declined), 1 patient was identified with active pulmonary TB.
Conclusion: The T-spot TB assay performed well. It greatly improves confidence in screening this population, distinguishing false positive and negative Mantoux reactivity, thereby allowing better rationalisation of chemoprophylaxis.
NEW ENTRANT SCREENING STRATEGIES FOR TUBERCULOSIS: A WORTHWHILE CAUSE?
S. A. Srivastava1, R. J. Whitfield2, C. F. J. Rayner1. 1St George's Hospital; 2Mayday Hospital, London, UK
Introduction: Tuberculosis (TB) is the leading infectious cause of death, and in parts of London there are up to 70 cases per 100,000 population per year. There are approximately 97 million people passing through the UK each year. Current immigration rules state those intending to stay for longer than 6 months, and who arrive from countries with a high TB incidence (>40 cases per 100,000 population per year), should be referred to the Port Health medical inspector for screening. This is approximately 270,000 entrants each year. We report the experience of assessing suspected pulmonary TB in immigrants that have been referred from Port Health over the past year, at two South London hospitals—St George’s and Mayday.
Methods: Over the past 12 months, a total of 34 patients were seen. These patients had been referred to the chest clinic on the basis of a chest radiograph taken at Port Health which was thought to be abnormal. All patients were assessed by specialist nurses, and had repeat chest radiography. Patient outcomes were looked at retrospectively.
Results: Seventeen patients had normal chest radiographs and 12 had evidence of previous pulmonary TB. Other diagnoses included sarcoid, usual interstitial pneumonia and soft tissue lesions awaiting follow-up. Out of 34 patients, two (0.06%) were treated for TB, and one (0.03%) for latent TB. All three had Mantoux >15 mm, and positive Quantiferon tests.
Conclusion: The treatment rate from patients referred was 0.06%. In 2004, the Health Protection Authority found the diagnosis rate of TB in patients referred for radiography at Heathrow to be 0.001% (Port Health and Medical Inspection Review, 2006). All 34 patients were referred with abnormal chest radiographs—these are reported by the Port Health medical inspector. When reported by a chest radiologist, 17 (50%) had normal radiography. Screening via this method is inefficient, and not cost effective to the Health Protection Unit and the TB services. It would be more appropriate to encourage entrants to register with a primary care physician, and for consideration of TB to be part of the patients’ review, especially if symptomatic.
NURSE LED RAPID ACCESS CLINIC REDUCES WAITING TIMES AND ENSURES TIMELY AND EFFECTIVE DIAGNOSIS AND MANAGEMENT OF TUBERCULOSIS
M. Cootauco, J. Groth, C. F. J. Rayner. St George's NHS Trust, London, UK
Tuberculosis (TB) rates continue to increase in the UK; the London region accounted for 43% of 8113 cases in 2005 (46.3 per 100,000). Most TB cases occur in young adults and in non-UK born who may be slow to access care. National and regional targets have an ultimate goal to reduce, and ultimately eliminate, TB in the UK. To achieve these goals TB services aim to reduce new infections, provide high quality treatment for all and to maintain low levels of dug resistance. To meet these demands within a tight financial and staffing framework, a change in TB service structure was developed to enable rapid and accessible care for all.
Methods: The service was designed to be led by the TB nurse specialists with supervision from the lead clinician. A prospective audit was undertaken to assess if the aims of the service were being met. Referrals with suspected TB were triaged by the lead clinician and lead TB nurse. The initial assessment used a standardised assessment proforma which directing investigations. Referrals were accepted from any source. Once initial assessment and investigations were undertaken the case was discussed with the lead clinician and either treatment initiated or further investigations planned and documented with rapid communication to the GP and the Health Protection Unit (HPU).
Results: Over a 6 month period 150 patients were referred: 40% GP, 13% occupational health, 13% A&E and radiology, 20% from all other sources. All patients were seen within 7 days of referral. 21% were started on full treatment, 30% given prophylaxis and 28% discharged. 30% required more detailed assessment in a doctor led clinic and 4% were referred to other clinical departments. All patients with smear positive disease were commenced on treatment within 7 working days of the original referral. The service change was cost neutral and patients reported good satisfaction with the service.
Conclusion: This change in service structure enabled rapid assessment and initiation of treatment of patients with possible TB without extra cost. This is an effective utilisation of TB Clinical Nurse Specialist skills to provide patient centred expert care within a multidisciplinary setting.
DO TRADITIONAL HEALERS INFLUENCE THE MANAGEMENT OF TUBERCULOSIS PATIENTS? TREATMENT DELAY AND PATIENT CONSULTATION PATTERNS IN RURAL ZIMBABWE
K. M. Scott1, R. M. Smith2, M. Glenshaw3, E. Manomano3, R. D. Barker2. 1Kings College, London School of Medicine at Guy's, Kings and St Thomas's Hospitals; 2Department of Respiratory Medicine, Kings College Hospital, London, UK; 3Murambinda Mission Hospital, Zimbabwe
Background: In rural Southern Africa traditional healers are more numerous than medical professionals and are widely consulted. Previous research has shown that tuberculosis (TB) patients often consult traditional healers and that in some cases this leads to treatment delays and increased morbidity. Engaging with traditional healers may improve patient outcomes. At a rural district hospital in Buhera, Zimbabwe a pressing need to improve both the case-finding and cure rates of TB has been identified. The overall recorded incidence of TB in the district is approximately 422/100,000/year; a significant under-diagnosis when compared to World Health Organization estimates (674 cases per 100,000 population per year). This translates to a case detection rate of 62%. Cure rates currently fall below 50%. Involving local traditional healers may be one means of improving patient outcomes.
Aims: This study aimed to assess the extent to which TB patients diagnosed at the hospital had consulted traditional healers and whether this caused treatment delays. This data collection was part of a routine audit of consultation patterns which aimed to assess the need for community based interventions in the future.
Method: Following a diagnosis of TB, patients are required to register with the district office. As part of this process, a randomly selected subgroup of patients were asked to specify whether they consulted a traditional healer, a primary health clinic or both prior to presentation. “Treatment delay” was recorded as the time between first seeking help (first consultation with either a traditional healer or a nurse in a primary health clinic) to diagnosis at the district hospital. Complete data were available for 922 patients (out of 1715) who registered between January 2005 and December 2006.
Results: 56% of patients reported consulting a traditional healer (as opposed to the health service) prior to diagnosis. The median delay for patients who consulted a primary health clinic as the first point of call was 13 days (25th, 75th centile: 7, 23) compared with a median delay of 15 days (25th, 75th centile: 8, 30) for those who consulted a traditional healer. After ranking all of the data, the mean rank of the treatment delay for those who consulted a primary health clinic was 307.98 compared to a mean rank of 374.57 for those consulting a traditional healer. The difference between the groups was found to be significant using a Mann Whitney U test (parametric assumptions were not met) (Z = −0.44, p<0.001).
Conclusion: The widespread consultation of traditional healers reported in this study reproduces findings elsewhere in Southern Africa, emphasising the important role of traditional healers in many rural communities. Anecdotal evidence from healthcare staff at the hospital suggests that most TB patients are ambulatory upon diagnosis; the more unwell patients may not be able to access the hospital services due to distance and other hurdles. The involvement of traditional healers in the TB control programme may be an opportunity to improve the referral process, case detection and outcomes of the TB patients in this district. Some TB programmes in the region have involved traditional healers within the existing services as Directly Observed Therapy (DOTS) supervisors. Others have been educated about when it is appropriate for an individual to be referred to a hospital. This study justifies further research in this area to gain a better understanding of the practices of traditional healers, their role within the community and to develop appropriate interventions involving traditional healers.
Pulmonary circulation: clinical aspects
INFECTION AFFECTS ENDOTHELIUM-DEPENDENT PULMONARY VASCULAR RESPONSES IN REJECTING SINGLE LUNG TRANSPLANTS
V. P. Rao2, H. K. Kim1, Y-S. Park1, H. D. Tazelaar1, V. M. Miller1, C. G. A. Mcgregor1. 1Mayo Clinic, USA; 2University of Nottingham, UK
Introduction: Both infection and rejection affect morbidity and mortality following lung transplantation. Following evidence of phenotypic heterogeneity of the vascular endothelium, experiments were designed to study organ-specific effects of infection on endothelial function in rejecting lung allografts.
Methods: After single lung transplantation, dogs (n = 15) were immunosuppressed with methylprednisolone, cyclosporine and azathioprine for 5 days at which point immunosuppression was withdrawn to allow acute rejection of the grafts. On postoperative day 8, the lungs were explanted for histological and functional studies. A scale of 0 to 12 was developed to grade lung infection, based on the number and extent of neutrophil infiltration in alveoli. Animals with mean infection scores <4 were included in Group A (n = 7) and animals with mean infection scores >5 were included in Group B (n = 8). For functional studies, pulmonary arteries of transplanted lung were cut into rings and suspended for pharmacological characterisation in organ chambers.
Results: Rejection grades of all animals were ⩾2 and not different between the groups. Endothelium-dependent contractile responses to endothelin-1 and angiotensin I were attenuated in animals from Group B compared to Group A. This difference was absent when the endothelium was removed and in the presence of L-NMMA, a nitric oxide synthase inhibitor. Endothelium-dependent relaxation to the calcium ionophore A23187 decreased with increasing infection scores (p<0.05). Relaxations to adenosine diphosphate or responses of the smooth muscle to nitric oxide were not different between the groups.
Conclusion: Infection affects pulmonary vascular reactivity in rejecting lung allografts and these effects are mediated in part by the vascular endothelium. Site-specific differences in endothelial responses to specific risk factors could identify potential diagnostic and therapeutic targets aimed at reducing morbidity following lung transplantation.
VENTRICULAR MASS INDEX MEASURED USING MAGNETIC RESONANCE IMAGING CORRELATES WITH PULMONARY ARTERY PRESSURE IN PATIENTS WITH SYSTEMIC SCLEROSIS AND SUSPECTED PULMONARY ARTERIAL HYPERTENSION
D. Hagger1, N. Woodhouse1, C. A. Elliot2, J. Wild1, I. Armstrong2, C. Hill3, C. Davies3, D. G. Kiely2. 1University of Sheffield Academic Unit of Radiology; 2Sheffield Pulmonary Vascular Disease Unit, Royal Hallamshire Hospital; 3Dept Radiology, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Magnetic resonance imaging (MRI) has been used extensively to assess cardiac function. We have examined whether volumetric measurements made using MRI could be used to identify patients with pulmonary arterial hypertension (PAH) in a group of patients with systemic sclerosis and suspected pulmonary hypertension identified using a screening protocol.
Methods: MRI scans were performed within 1 month of cardiac catheterisation on a 1.5 T, Philips Eclipse scanner using a gated spoiled gradient echo multi-slice sequence. Volumetric measurements of the cardiac volume were made from the MR images by an individual blinded to the results of the cardiac catheter. The cardiac mass indices were deduced from the volumetric measurements.
Results: 40 patients (8 men) with systemic sclerosis and suspected PAH (PAH-SSc) mean (SD) age 61 (13) years underwent right heart catheterisation and MRI. For the group: mean (SD) pulmonary artery pressure (MPAP) 39 (17) mm Hg; right atrial pressure (RA) 8 (5) mm Hg; cardiac index (CI) 3.0 (0.9) l/min/m2; pulmonary capillary wedge pressure (PCWP) 9 (3) mm Hg; and pulmonary vascular resistance (PVR) 504 (102) dynes.s.cm−5. 27 patients had PAH defined as a MPAP ⩾25 mm Hg and PVR ⩾240 dynes.s.cm-5. There was a weak correlation between right ventricular end-diastolic mass (RVEDM) and MPAP (r = 0.56, p<0.0005) and RVEDM and PVR (r = 0.34, p<0.05). The correlation was improved when the ventricular mass index was used RVEDM/left ventricular end diastolic mass (LVEDM): VMI and MPAP (r = 0.66, p<0.0005) and VMI and PVR (r = 0.65, p<0.0005). The specificity, sensitivity, positive predictive value (PPV) and negative predictive value (NPV) of the VMI in identifying patients with PAH-SSc is shown in the table.
Conclusion: In systemic sclerosis VMI correlates moderately with MPAP and PVR. The VMI cannot be used to confidently exclude PAH. However in patients identified from a screening programme as at increased risk of pulmonary hypertension a VMI ⩾ 0.7 is highly predictive of the presence of PAH.


THE NATRIURETIC RESPONSE ON ACUTE ASCENT TO HIGH ALTITUDE
M. Toshner1, J. K. Baillie2, J. Suntharalingam1, J. J. Morton4, A. A. R. Thompson3, A. J. Peacock4. 1Papworth Hospital; 2Borders General; 3Sheffield Teaching Hospital NHS Trust; 4Western Infirmary, UK
Background: Natriuretic peptides are released in response to atrial and ventricular stretch and, in addition to having diuretic effects, attenuate hypoxic pulmonary vasoconstriction and therefore play a role in maintenance of pulmonary vascular tone. Atrial natriuretic peptide (ANP) is increased in hypobaric hypoxia at altitude; however the response of brain natriuretic peptide (BNP) is not known. As BNP is predominantly secreted by the ventricles it is of further interest as a surrogate marker of ventricular function. There is evidence that hypoxia impairs ventricular diastolic and systolic function and is well documented to result in pulmonary hypertension, although this is most pronounced in the context of high altitude pulmonary oedema (HAPE).
Methods: Eight healthy volunteers with no previous history of HAPE spent 4–5 days at 3650 m in La Paz, Bolivia before ascending by vehicle to 5200 m where they spent the next 7 days. Sea level pre-expedition measurements were made of pulmonary artery systolic pressure (PASP), ANP and NT-pro BNP (a more stable BNP precursor). This was repeated on ascent to 5200 m on days 5, 8 and 12. None of the patients developed HAPE. All investigations were performed at rest. PASP was estimated by measuring tricuspid regurgitant jet on 2D echo (portable Accuson Cypress) and verified by a blinded second observer. Serum samples were centrifuged and transferred on dry ice to the UK. Data analysis was by repeated measures ANOVA.
Results: PASP was raised at altitude; day 5 mean 37.7 mm Hg (p 0.042), day 8 38.8 mm Hg (p 0.044), day 12 35 mm Hg (p 0.037) vs sea level 15.8 mm Hg. The ANP rise seen did not reach significance (p = 0.48). NT pro BNP (pg/ml) showed a small drop; day 5 12.9 (p 0.45), day 8 9.2 (p 0.048), day 12 6.33 (p 0.001) vs sea level 15.7.
Summary: This study is in line with previous observations of raised PA pressure at altitude. NT proBNP did not rise in resting subjects at altitude despite raised PA pressures.
Conclusion: In normal subjects not susceptible to HAPE, NT pro-BNP does not rise indicating well preserved ventricular function.
COMPARING 6 MINUTE WALK AND HYPOXIC CHALLENGE IN PATIENTS WITH PULMONARY ARTERIAL HYPERTENSION
E. Soon1, M. Toshner1, J. Suntharalingham2, J. Pepke-Zaba1. 1Papworth Hospital; 2Royal United Hospital, UK
Introduction: There are no specific UK recommendations for pulmonary arterial hypertension (PAH) patients planning air travel. The British Thoracic Society (BTS) guidelines advise that patients with a significant risk factor and saturations of less than 95% on air be formally assessed. A common method of assessment is to perform a hypoxic challenge. Akero et al demonstrated in chronic obstructive pulmonary disease (COPD) patients that aerobic capacity was the only factor that positively correlated with in-flight blood oxygen levels after 4 hours of flight. We investigated the value of 6 minute walk (6MWD) and hypoxic challenge (HC) testing in identifying PAH patients who desaturate.
Methods: Data were gathered retrospectively from PAH patients who attended for hypoxic challenges from 2001 to 2007. 22 patients were found to have had 6 minute walks done within 3 months of their hypoxic challenge. These patients had no other lung disease, normal lung function tests, and no other factor that would limit their 6MWD other than PAH. Baseline saturations and the lowest saturation demonstrated during hypoxic challenge and 6 minute walk were recorded. 12 patients had concomitant right heart catheterisation (RHC).
Results: The baseline haemodynamics and results are summarised in the table. There was no correlation between mean pulmonary artery pressure (mPAP), cardiac output (CO) and saturation drop during either 6MWD (r = 0.08 and −0.02, respectively) or HC (r = −0.17 and −0.11, respectively). Patients with idiopathic PAH (IPAH), connective tissue disease (CTD) and post-pulmonary endarterectomy (PEA) have a significantly greater saturation drop during 6MWD than in response to hypoxic challenge. Patients with distal chronic thromboembolic disease (CTEPH) behave differently and have a significantly greater saturation drop in response to a hypoxic challenge than a 6MWD. The saturation drop during both 6MWD and HC was not related to the haemodynamics from RHC at rest.
Conclusion: These data suggest that patients with pulmonary hypertension due to IPAH, CTD and post-PEA who desaturate significantly on 6MWD will require oxygen in-flight and do not need further assessment with hypoxic challenge. This merits a more detailed investigation in how PAH patients are assessed for air travel.

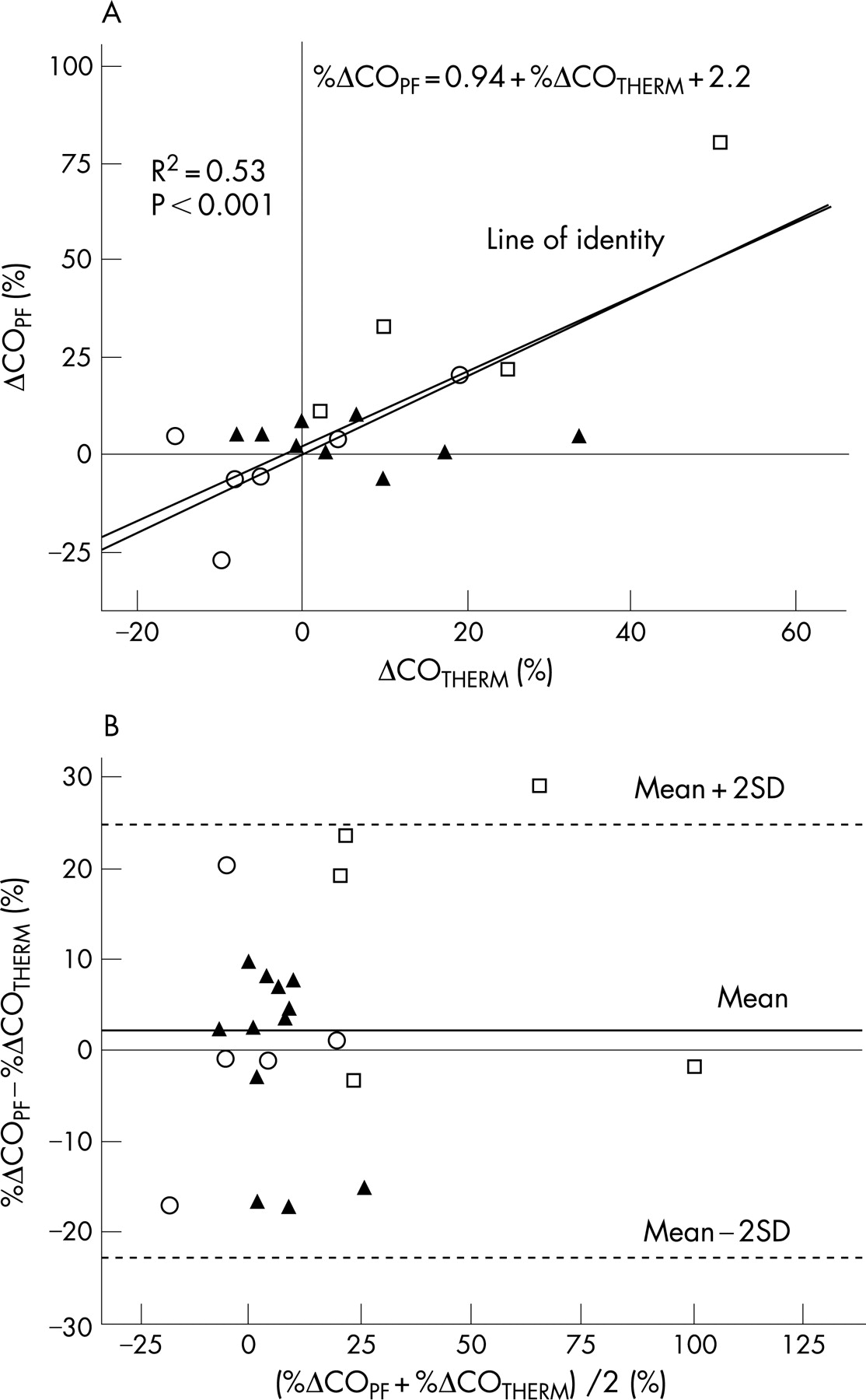
REDUCED INCREMENTAL SHUTTLE WALKING TEST DISTANCE IS ASSOCIATED WITH A WORSE SURVIVAL IN PULMONARY ARTERIAL HYPERTENSION ASSOCIATED WITH SYSTEMIC SCLEROSIS
C. A. Elliot1, C. Billings1, I. Armstrong1, J. Waterhouse1, C. Billings1, M. Akil2, D. G. Kiely1. 1Sheffield Pulmonary Vascular Disease Unit, Royal Hallamshire Hospital; 2Dept Rheumatology, Royal Hallamshire Hospital, Sheffield, UK
Background: In pulmonary arterial hypertension (PAH) associated with systemic sclerosis (SScl) assessing disease severity and prognosis can be difficult.
Aim: To investigate whether baseline exercise capacity measured with the incremental shuttle walking test (ISWT) can help assess disease severity and prognosis in SScl with PAH.
Methods: Retrospective analysis of patients with SScl, diagnosed and treated in our centre with PAH (mean pulmonary artery pressure (MPAP) >25 mm Hg at rest, pulmonary capillary wedge pressure (PCWP) <15 mm Hg) with ISWT performed within 90 days of cardiac catheter.
Results: 84 patients (85% female) with age (mean (SD)) 63 (11) years had right atrial pressure (RA) 7.65 (5.5) mm Hg, MPAP 41 (12) mm Hg, PCWP 8.5 (3.6) mm Hg, pulmonary vascular resistance (PVR) 675 (428) dynes, cardiac index (CI) 2.7 (0.86) l/min/m2 and mixed venous oxygen saturation (MVO2) 65 (9)%. Median baseline ISWT distance was 120 m. Patients with an ISWT >120 m had a survival advantage over those with an ISWT <120 m (Kaplan–Meier analysis; p = 0.032) with a 1 and 2 year survival rate of 94% and 82% vs 72% and 52%, respectively. In addition, those with an ISWT <120 m were older, but also had significantly worse haemodynamics than those with an ISWT >120 m. Age 67 (12) vs. 60 (10) years (p = 0.004), MPAP 45 (12) vs. 38 (11) mm Hg (p = 0.007), PVR 845 (446) vs. 513 (342) dynes (p<0.001), CI 2.5 (0.89) vs. 2.9 (0.77) l/min/m2 (p = 0.03), MVO2 63 (10) vs. 67 (6)% (p = 0.045).
Conclusion: In PAH associated with SScl a poor baseline ISWT distance identifies individuals at increased risk of more severe PAH and a worse prognosis.
THE PHYSIOFLOW 1 THORACIC BIOIMEPEDANCE DEVICE FOLLOWS TRENDS IN CARDIAC OUTPUT CHANGES IN PATIENTS WITH PULMONARY HYPERTENSION
R. Syyed, D. Welsh, A. J. Peacock. Scottish Pulmonary Vascular Unit, UK
Introduction: We investigated whether the physioflow 1 thoracic bioimpedance device was a suitable method of measuring cardiac output (CO) in patients with pulmonary hypertension.
Methods: We simultaneously measured CO, using a standard thermodilution technique and by thoracic bio-impedance, in patients with pulmonary hypertension, while supine at rest. There were 25 subjects, measured on a total of 27 different occasions (10 male/15 female, mean (SD) age 61 (14) years). 18 patients were simultaneously analysed while undergoing a physiological procedure, (7 receiving oxygen, 11 receiving nitric oxide and 4 during exercise, represented by a cycle, triangle and square respectively), and the percentage change from baseline compared.
Results: The physioflow 1 (PF) overestimated CO when compared to the thermodilution method (Therm) (mean (SD) 1.34 (1.50) litres/min) (see fig 1A,B). However the percentage change from baseline was much more accurate (mean (SD) 2.1 (12.5)%) (see fig 2A,B).
Conclusion: These findings suggest that cardiac output as derived from the physioflow 1 in patients with pulmonary hypertension is not accurate enough for clinical use, but this device can accurately follows percentage change in cardiac output when compared to standard techniques.
ELEVATIONS OF PROTHROMBOTIC FACTOR VIII IN HEREDITARY HAEMORRHAGIC TELANGIECTASIA: ASSOCIATION WITH AGE AND PULMONARY ARTERIOVENOUS MALFORMATIONS, BUT NOT PULMONARY ARTERY PRESSURE
C. L. Shovlin, J. E. Jackson. Hammersmith Hospital and Imperial College, London, UK
Introduction: High levels of factor (F) VIII are associated with first and recurrent episodes of venous thrombosis. We have demonstrated that FVIII:Ag is elevated in individuals with hereditary haemorrhagic telangiectasia (HHT), and associated with long-term risk of pulmonary emboli and deep venous thrombosis. Pulmonary hypertension, which occurs in HHT, is also associated with high FVIII.
Methods: Association studies were performed in the previously described series of 125 HHT-affected individuals with no recent ill-health, intervention or venous thromboemboli. Patient-specific variables were recorded as part of ongoing prospective studies, including pulmonary artery pressure (PAP) recorded at pulmonary angiography (to embolise PAVMs) within a year of FVIII:Ag measurements. Confocal microscopy studies were performed in normal pulmonary artery endothelial cells.
Results: 87/125 (70%) of HHT-affected individuals had FVIII:Ag measurements exceeding the normal laboratory range of 0.45–1.58 u/ml. In the HHT group, the overall range was 0.52–4.87 (Q1 1.51, Q2 1.77, Q3 2.27) u/ml. Only one patient in whom FVIII was measured had significant pulmonary hypertension, associated with FVIII:Ag of 1.77 u/ml. In univariate analyses, elevated FVIII:Ag was associated with increasing age and pulmonary arteriovenous malformations (AVMs, see table). There was no association demonstrated between FVIII:Ag and PAP (see table), acute phase response, or disseminated intravascular coagulation. Multiple regression analyses confirmed the increase of FVIII:Ag with age (hazard ratio 0.008 (95% confidence interval (CI) 0.004 to 0.013), p = 0.00045). The best model suggested that the unexpected association of pulmonary AVM with the level of FVIII:Ag was age-independent (hazard ratio for no pulmonary AVM: −0.276 (95% CI −0.51 to −0.043), p = 0.021). Confocal microscopy studies support a pulmonary artery origin for FVIII.
Conclusion: Elevation of FVIII:Ag in HHT cannot be explained by known precipitants, but further suggests pulmonary vascular regulation of systemic FVIII:Ag levels.
DIFFERENTIAL TREATMENT REFERRAL RATES FOR PULMONARY ARTERIOVENOUS MALFORMATION PATIENTS, ACCORDING TO MEDICAL RECOGNITION OF NEUROLOGICAL RISK
C. L. Shovlin. Hammersmith Hospital and Imperial College, London, UK
Background: Paradoxical embolic strokes and brain abscesses affect high proportions of individuals with pulmonary arteriovenous malformations (PAVMs). Embolisation can be used to treat PAVMs. Many individuals are not considered for treatment.
Methods: Factors influencing referral patterns for PAVM treatment were analysed in 219 consecutive individuals with PAVMs reviewed between May 1999 and 2005, followed up until May 2006. Symptoms and age at presentation, time of presentation and treatment referral, stroke/abscess history, and oxygen saturation (SaO2) measurements were recorded among patient-associated variables. Univariate analyses and Anderson-Gill models assessed constant and time-dependent potential predictive variables for stroke/abscess. Patients were stratified into four diagnostic presentation groups, excluding individuals in whom a stroke or brain abscess directly precipitated the diagnosis of PAVMs, or where PAVMs were diagnosed in the surgical treatment era (pre 1985). For presentation pattern analyses, overall p values were calculated by ANOVA and Bonferroni post-test corrections applied.
Results: Ischaemic stroke or brain abscess affected 57/219 PAVM patients. Fifteen events occurred in patients with a pre-existing diagnosis of PAVM in whom referral for treatment had not been considered. Of the 219 individuals with PAVMs, 46 (21.5%) were diagnosed because of respiratory symptoms. The remainder were diagnosed by incidental investigations (n = 73, 33.3%), or PAVM screening programmes in families with hereditary haemorrhagic telangiectasia (HHT, n = 100, 45.7%). If at the time of PAVM diagnosis, the individual gave a past medical history of stroke or brain abscess, the mean PAVM diagnosis to PAVM treatment interval was 1.1 (95% CI 0.7 to 1.6) years. This was as fast as for HHT screening programme diagnoses (1.7 (95% CI 0.5 to 2.9) years). In contrast, for individuals with no previous stroke/abscess history, the diagnosis to treatment interval was significantly longer. The presence of respiratory symptoms did not influence this interval which was 6.8 (95% CI 4.1 to 9.5) years for individuals with respiratory symptoms (dyspnoea or haemoptysis), and 7.5 (95% CI 4.3 to 10.8) years for asymptomatic individuals. This was in spite of the fact that the group with dyspnoea or haemoptysis at presentation were significantly younger and had lower oxygen levels than the other groups.
Conclusion: Medical appreciation of neurological risk influences the likelihood that an individual with PAVMs will be referred for treatment.

MATERNAL DEATH DURING PREGNANCY: SURVIVAL ADVANTAGE FOR WOMEN WITH PRE-EXISTING DIAGNOSES OF PULMONARY ARTERIOVENOUS MALFORMATIONS OR HEREDITARY HAEMORRHAGIC TELANGIECTASIA
C. L. Shovlin1, V. Sodhi2, A. Mccarthy2, J. E. Jackson1, M. N. Sheppard4. 1Hammersmith Hospital and Imperial College; 2Queen Charlotte's Hospital; 4Royal Brompton Hospital and Imperial College, London, UK
Introduction: Fatal haemorrhages from silent pulmonary and cerebral arteriovenous malformations (AVMs) have been reported during pregnancy. These risks are poorly appreciated by respiratory and medical communities.
Methods: Pregnancy outcomes were studied in 484 pregnancies in 113 consecutive women with PAVMs reviewed between 1999 and 2006, and 86 haemorrhagic telangiectasia (HHT) affected female relatives. Outcomes measures of maternal death, haemoptysis, haemothorax, and stroke were analysed in three groups: (1) a prospective group who received pre-pregnancy intervention (n = 23); (2) a retrospective group with a “survival from pregnancy to review” bias (n = 239); and (3) a first-degree relatives group with neither bias, but likely to have under-recognised individuals affected by HHT (n = 222).
Results: The rates of major PAVM bleeds were 1.36% (0.17, 2.54) for PAVM/HHT pregnancies, and 1.02% (0.13, 1.92) for all HHT pregnancies. One woman in the prospective group required emergency embolisation at 20 weeks gestation due to massive haemoptysis which subsequently settled. Two women in the retrospective group required emergency angiography or lobectomy at 6 to 7 months gestation; both pregnancies subsequently proceeded normally. There were two maternal deaths due to massive haemoptysis in the relatives group: both occurred at the start of the third trimester. In all cases, herald bleeds occurred at least 24 hours in advance of the final event. The overall maternal death rate in HHT pregnancies was 1.00% (95% CI 0.13 to 1.92). All deaths occurred in women who were previously well. In addition to the two due to PAVM haemorrhage, two were due to cerebral AVM haemorrhage (overall frequency of major stroke 1.24% (95% CI 0.25 to 2.23) for all HHT pregnancies, and one due to an acute transmural myocardial infarction in a 16-year-old with normal coronary arteries and right ventricle. Prior awareness of HHT or PAVM diagnosis (facilitating emergency intervention) led to improved survival in women experiencing a life-threatening event (p = 0.034, Fisher’s exact test).
Conclusion: While most HHT and PAVM pregnancies proceeded normally, the rare occurrence of major complications, and improved survival outcome following prior recognition, carry implications for obstetric and anaesthetic management of pregnancy in a woman with pulmonary AVMs and/or HHT.
MASS SPECTROMETRY: A NON-INVASIVE MEASURE OF PULMONARY BLOOD FLOW IN PATIENTS WITH PULMONARY HYPERTENSION
T. J. Corte, C. Harries, D. Cramer, S. Ward, M. Gatzoulis, S. J. Wort. Royal Brompton Hospital, London, UK
Introduction: Respiratory mass spectrometry (RMS) is a simple, non-invasive and reproducible measure of pulmonary haemodynamics, including pulmonary blood flow (QPF).1 2 In patients with pulmonary hypertension (PH) where repeated right-heart catheterisation (RHC) is not routinely performed, a non-invasive measure of QPF is a desirable tool for clinical practice.
Methods: All patients with PH referred for RMS during 2006–7 were included (n = 15). All patients also had concurrent pulmonary function, echocardiography, and submaximal exercise test data, and 14 patients had concurrent BNP levels. Relationships between QPF and other non-invasive variables indicating pulmonary vascular dysfunction were examined.
Results: All patients had PH on echocardiogram (mean (SD) tricuspid gradient (TG, n = 8) was 90 (27) mm Hg, pulmonary acceleration time (PAT, n = 8) was 56.6 (16.6) ms). Underlying aetiology for PH included Eisenmenger syndrome (n = 11), idiopathic pulmonary arterial hypertension (n = 2), chronic thromboembolic PH (n = 1), and HIV-related PH (n = 1). Mean RMS QPF was 2.9 (0.7) litres/min. Mean DLco was 65.9 (13.5)%, FVC 79.9 (20.8)%, and median BNP 23.5 (7.5 to 88.4). Exercise capacity was impaired: median World Health Organization functional class 2 (1–4); and 6 minute walk testing (6MWT), mean (SD) minimum oxygen saturation was 70 (13)%. QPF correlated with DLco (r = 0.56, p = 0.03), resting pulse oximetry (r = 0.67, p = 0.01), and 6MW minimum saturation (r = 0.78, p<0.01). No significant correlation was found between QPF and echocardiographic parameters, BNP or 6MW distance (perhaps reflecting the small sample size).
Conclusion: QPF is a simple, reproducible and non-invasive measurement, which may be useful in clinical practice. RMS measurement of QPF correlates with other non-invasive indices used clinically in PH, including DLco, resting pulse oximetry, and 6MW minimum oxygen saturation. Further testing is required to determine its relationship with echocardiographic and right heart catheter measures of PH severity.
Non-invasive ventilation: audit and practice
AIRWAY CLEARANCE IN BRONCHIECTASIS: IS NON-INVASIVE VENTILATION A USEFUL ADJUNCT IN MODERATE TO SEVERE DISEASE
F. M. Moran1, S. E. Elborn2, I. Bradbury3, A. Piper4, O. Hewitt2, J. M. Bradley5. 1School of Health Sciences, University of Ulster; 2Regional Respiratory Centre, Belfast Trust, Belfast City Hospital; 3Queen's University; 4Royal Prince Alfred Hospital & University of Sydney, Australia; 5University of Ulster & Regional Respiratory Centre, Belfast Trust, Belfast City Hospital, UK
Rationale: Evidence to support the use of non-invasive ventilation (NIV) as an adjunct to airways clearance in patients with bronchiectasis is limited.
Aim: To assess if airway clearance using NIV was non-inferior to the active cycle of breathing techniques (ACBT) in patients with moderate to severe bronchiectasis during an acute exacerbation.
Methods: Twenty patients with bronchiectasis (FEV1 <60%) requiring intravenous antibiotics were randomised to: Group 1 (n = 10), ACBT; or Group 2 (n = 10), NIV and ACBT. Outcomes measures included respiratory muscle strength (PIMax and PEMax); spirometry; arterial blood gases; oximetry(SpO2); breathlessness scores; patient perception of tiredness, benefit and ease of treatment; auscultation; number of coughs per treatment; duration of treatment; sputum production, wet and dry weight. The Lifeshirt (respiratory impedance plethysmography) recorded: inspiratory tidal volume; minute ventilation; end expiratory lung volume (qDEEL); respiratory rate; fractional inspiratory time (Ti/Tt); mean inspiratory flow; peak expiratory flow of tidal volume; phase angle; heart rate; arterial oxygen saturation.
Analysis: SPSS mixed effects ANOVA, paired t-tests and Pearson’s r.
Results: Baseline demographics are shown in the table. There were no between group treatment differences from day 1 to final day except PIMax: group 1 vs group 2; −17 (95% CI −5 to −29) p = 0.01; post-treatment SpO2: group 1 vs group 2; 1 (95% CI 3 to 0.1) p = 0.04. Lifeshirt data identified between group treatment differences in qDEEL during breathing control (BC) and thoracic expansion exercises (TEE). BC: group 1 vs group 2; 53 (95% CI 11 to 94) p = 0.04; TEE: group 1 vs group 2; 87 (95% CI 21 to 153) p = 0.02. There were between group treatment differences in Ti/Tt in BC: group 1 vs group 2; −0.04 (95% CI −0.07 to −0.01) p = 0.01.
Conclusion: Airway clearance using NIV may be non inferior to ACBT in patients with moderate to severe bronchiectasis during an acute exacerbation. Dynamic lung function during airway clearance treatment with NIV resulted in increases in inspiratory muscle strength and a reduction in hyperinflation. Therefore, patients who have difficulty expectorating sputum may be offered positive pressure support as an alternative treatment if standard airway clearance is not sufficient.
A BENCH TEST TO ESTABLISH THE CORE PRINCIPLES OF ADAPTIVE SERVOVENTILATION
N. Oscroft, T. G. Quinnell, J. M. Shneerson, I. E. Smith. Papworth Hospital NHS Foundation Trust, Cambridge, UK
Introduction: Adaptive servoventilation (ASV) is a novel mode of non-invasive ventilation (NIV) designed to adapt pressure support (PS) to achieve a preset target minute ventilation (TgV). This may optimise ventilation; however, no published data confirm ASV compensates appropriately for changes in pulmonary mechanics and circuit leak, which are often encountered in clinical practice.
Methods: A non-invasive ventilator featuring an ASV mode (AutoVPAP, Resmed) was assessed. A test lung with varying compliance and non-linear resistors (Michigan Instruments) and pneumotachograph (Hans Rudolph) were used. Three lung model settings were chosen: (1) a low resistance (rp 5 + rp 20) and high compliance (0.2 litres/cm H2O); (2) high resistance (rp 5 + rp 50) and high compliance; and (3) high resistance and low compliance (0.1 litres/cm H2O). To assess the range of minute ventilation possible with different lung settings the ventilator was assessed in the spontaneous/timed mode. ASV was then tested with varying TgV. In both modes, a standard expiration valve was present, the respiratory rate was 15, inspiratory time 1 second and PS varied between a minimum of 3 and maximum of 21 cm H2O. Additional circuit leak varied between 10–15 litres/minute.
Results: In the S/T mode the following ranges of ventilation (litres/minute) were achieved (median and interquartile range) (see table 1). In the ASV mode the following values were recorded (see table 2).
Conclusion: The ASV mode was able to adapt PS levels to achieve TgV, when lung compliance and resistance altered, within the limits of the ventilators capabilities. Leak compensation was good. The impact of patient ventilator interactions requires clinical assessment.

DOES WEIGHT LOSS PREDICT CESSATION OF NON-INVASIVE VENTILATION FOR OBESITY RELATED HYPOVENTILATION?
T. W. Felton, A. Corney, C. Stuart-Buttle, A. McPartlin, A. Bentley. Wythenshawe Hospital, Manchester, UK
Introduction: Factors leading to cessation of non-invasive ventilation (NIV) for obesity hypoventilation syndrome (OHS) have not been previously reported. Anecdotal evidence suggests that weight loss is a key issue. We investigated the role of weight loss and the influence of other pathologies causing type 2 respiratory failure on rates of discontinuation of NIV.
Method: A review of the OHS NIV service was performed. Details on weight, lung function, ventilator type and settings, blood gases and comorbidities were collected on 150 patients with OHS. Comparison was made between the group of patients where NIV was discontinued and those who remained on NIV.
Results: While on NIV patients lost on average 12 kg. In 44 (29%) of patients NIV was discontinued due to resolution of type 2 respiratory failure. Patients with an overlap syndrome of chronic obstructive pulmonary disease (COPD) and OHS are on average less obese with a body mass index (BMI) of 41 kg/m2 compared to those patients with pure OHS whose average BMI was 48 kg/m2. Of the 52 patients with COPD and OHS only 16 were able to discontinue NIV. There was no significant difference in weight loss between those with COPD and OHS who came off NIV and those that remained on NIV. Patients with OHS but without COPD lost weight with an average BMI falling from 47.9 kg/m2 to 40 kg/m2 in those who discontinued NIV. The BMI of those who remained on NIV dropped from 48.8 kg/m2 to 43.6 kg/m2. On average, those patients with OHS took 205 days before discontinuing NIV while those with the overlap syndrome of OHS and COPD took 462 days. There is no difference in any lung function measurements between those with COPD and those without or between those that discontinue NIV and those that do not.
Conclusion: In patients with OHS and COPD, weight loss and lung function data do not predict the likelihood of discontinuing NIV. In those patients with OHS but without COPD weight loss is important in determining those patients who can come off NIV. The absolute BMI “goal” of 40 kg/m2 appears more important than the change in weight for determination of discontinuation of NIV.
NON-INVASIVE VENTILATION AS CEILING OF TREATMENT IN ACUTE EXACERBATION OF COPD: IS THERE A RELATIONSHIP BETWEEN STARTING PH AND MORTALITY?
S. Khalid, J. Bright, D. Toye, Ng Man. Kwong, P. O'Donnell. Fairfield General Hospital, UK
Background: NIV is widely utilised across the UK as ceiling of treatment in patients with respiratory failure who are not considered suitable for invasive ventilation. In a previous prospective multicentre randomised trial it was found that at start of NIV, there is an association of low pH and a raised CO2 with treatment failure and the need for intubation. In another previous trial looking at NIV versus traditional treatment, there was no difference in outcome noted between the two treatment arms possibly as the degree of acidosis was quite modest (pH 7.33 ±0.01). This trial indicated that the benefit of NIV over traditional treatment requires presence of a certain degree of acidosis. The current British Thoracic Society (BTS) guidelines recommend any patient which has a ceiling of treatment at IPPV and has severe acidosis (pH <7.3) should be managed on HDU/ITU based on the above evidence as IPPV can be started if NIV fails.
Objectives: The objective of this study was to assess if there is a difference in mortality between the patients who had severe acidosis (pH of <7.25 which was the cut-off used in previous study) and those with lesser degree of acidosis. We also looked at the effect of the degree of acidosis on the duration of treatment.
Methods and results: Retrospective study of all patients with an acute acidotic exacerbation of COPD who had NIV as the ceiling of treatment over a 14 month period (1 January 2004 to 28 February 2005). These were the patients who failed to improve despite maximum standard treatment with controlled oxygen therapy, antibiotics, steroids and nebulised bronchodilators and were then given NIV. A total of 42 patients were identified. These were divided into two groups initially depending upon whether their pH was <7.25 (n = 26) and those with pH ⩾7.25 (n = 16) at the time of being started on NIV. The two groups were well matched with regards to median age (69.65 years for <7.25 group, 70.06 for ⩾7.25 group) and other baseline characteristics. The mortality data in these two groups was compared by using the Fisher’s exact test (see table) and it was found that there is no significant difference in mortality between the two groups. In patients who survived, we also analysed the relationship between the starting pH and the length of period for which NIV was required to correct acidosis. This is shown in the graph. From this graph it is obvious that there does not seem to be any relationship between the starting pH and the duration for which NIV is likely to be required.
Conclusion: From this study we conclude that in patients who are not suitable for invasive ventilation, the presence of severe acidosis should not be considered a contraindication to non-invasive ventilation. Also in this group of patients, we found that there does not seem to be any significant difference in mortality based on the degree of acidosis and hence the severity of acidosis should not influence the decision to use NIV as the ceiling of treatment. The findings of this trial should be confirmed in a larger, ideally prospective study.
INTUBATION RATE, MORTALITY AND BLOOD GAS OUTCOMES IN EXACERBATION OF COPD PRESENTING WITH HYPERCAPNIC RESPIRATORY ACIDOSIS TREATED BY NIV: A 3 YEAR SURVEY
D. Banerjee1, B. Beauchamp2, S. Madathil1, N. Nathani1. 1Sleep and Ventilation Unit, Birmingham Heartlands Hospital; 2Department of Physiotherapy, Birmingham Heartlands Hospital, UK
Introduction: Established guidelines suggest that non-invasive ventilation (NIV) should be considered in those patients with an acute exacerbation of chronic obstructive pulmonary disease (COPD) presenting with hypercapnic respiratory acidosis (Pco2 >6.0 Kpa and pH <7.35). At the Birmingham Heartlands Hospital, a multidisciplinary 11-bedded NIV unit on a respiratory ward was established in 2004. The NIV unit has close links to critical care to allow escalation of care. A survey of outcomes for all patients with COPD related acute respiratory failure needing NIV was carried out.
Methods: Data of all COPD patients with acute respiratory acidosis needing NIV between August 2004 and July 2007 (3 years) were analysed. Intubation rate, in-hospital mortality rates and blood gas data (pre-NIV and 1 hour after establishment of NIV) were analysed.
Results: In the 3 year period, there were 523 admissions needing NIV for acute respiratory failure. This does not include those patients in a pre-arrest situation and needing intubation immediately. 376 (72%) were exacerbation of COPD, 38 (7%) obesity related respiratory failure, 20 (4%) thoracic cage deformities, 18 (3%) primarily bronchiectasis, 10 (2%) neuromuscular disorder, and 61 (12%) were other causes. Of the 376 COPD admissions, there were 10 (2.7%) intubations (3 of which died), and 48 (13%) deaths. Causes for intubations were persisting acidosis despite NIV (n = 5), severe hypoxia due to pneumonia (n = 4), and one gastrointestinal bleed resulting in a risk to the airway. Primary reasons for mortality were 12 (25%) severe frailty and old age, 16 (33%) severe “end stage” COPD, 14 (30%) co-existing major comorbidities, 4 (8%) malignancy, and 2 (4%) unexpected cardiac arrest. In 45 patients where deaths occurred, NIV was made ceiling of care. Non-surviving admissions were more acidotic before and after 1 hour of NIV (see tables 1–3)
Conclusion: (1) This group had a low intubation rate when treated with NIV. Persisting acidosis and severe hypoxia due to pneumonia were the commonest reasons for a failure of NIV resulting in intubation. (2) Despite NIV, there is a 13% mortality rate in this group, the majority being due to frailty and old age, end stage disease and severe comorbidities. (3) The group that did not survive hospital admission were more acidotic than survivors.
SURVEY OF KNOWLEDGE OF HEALTH CARE PROFESSIONALS MANAGING PATIENTS WITH ACUTE HYPERCAPNIC EXACERBATION OF COPD REQUIRING NON-INVASIVE VENTILATION
E. Ballard1, L. Mcdonnell1, S. Keilty2, A. C. Davidson3, N. Hart3. 1Department of Physiotherapy St Thomas’ Hospital; 2Department of Critical Care St Thomas’ Hospital; 3Lane Fox Respiratory Unit St Thomas’ Hospital, London, UK
Background: The British Thoracic Society (BTS) guidelines for “NIV in acute respiratory failure” (BTS Standards of Care Committee Thorax 2002) reports that non-invasive ventilation (NIV) can be provided in a number of locations, including the intensive care unit (ICU), high dependency units (HDU) or the respiratory ward, but that such areas should have staff with appropriate knowledge and experience. The guidelines also suggest that patients with more severe acidosis (pH<7.3) should be managed in HDU or ICU as risk of failure higher. In our institution the mean pH of chronic obstructive pulmonary disease (COPD) patients starting NIV is 7.27 (Jolley et al, Thorax 2002) and a policy of initiation of NIV in either the emergency department or critical care areas, including ICU, HDU or respiratory intensive care unit (RICU), has been adopted. We carried out a survey to ascertain the knowledge of staff managing these patients.
Method: A questionnaire was initially piloted on 50 medical, nursing and physiotherapy staff in August 2006 and adapted following feedback and analysis. The subsequent questionnaire was designed to assess knowledge in four areas; indications, technical, practical and published evidence. These questionnaires were distributed by email or in person to all relevant staff and returned anonymously. Follow up emails were sent until at least 7 questionnaires were returned from each group. Completed questionnaires were received from 94 individuals and scored with weighting towards clinical relevance and current evidence base. To generate comparative analysis the groups were compared with a control group who were made up of medical senior house officers and specialist registrars working outside critical care and respiratory medicine.
Results: See tables 1 and 2.
Conclusion: In comparison to the control group, there is a wide spread of knowledge across the multidisciplinary group involved in the initiation of NIV for acute hypercapnic respiratory failure in COPD. The respiratory physiotherapists and specialist registrars achieved the best results overall in the technical, practical and published evidence sections, but all groups were similar, or worse, than the control group in the indications section. Medical HDU nurses and critical care SHOs showed equivalence to the control group despite being the major group initiating NIV and receiving targeted training. Interestingly, the respiratory and critical care consultants were not significantly different from the control group for the published evidence section. The observation from these data indicates that further educational support is required for all the groups, but the content of the training can be adjusted according to the group.
We thank Anita Simonds for her insightful comments in the design of the questionnaire.
INITIATION OF NON-INVASIVE VENTILATION IN THE EMERGENCY DEPARTMENT DURING ACUTE EXACERBATION OF COPD MAY INFLUENCE HOSPITAL MORTALITY
S. E. J. Keilty1, S. G. Ellum1, S. Langord3, A. Newton2, N. Hart4, A. C. Davidson4. 1Patient at Risk Team, Department of Critical Care, St Thomas’ Hospital; 2Emergency Department, St Thomas’ Hospital; 3High Dependency Unit, Department of Critical Care, St Thomas’ Hospital; 4Lane Fox Respiratory Unit, Department of Critical Care, St Thomas’ Hospital, London, UK
Background: At our institution, we audit the acute non-invasive ventilation (NIV) service annually. Data obtained from 2004–2005 showed that <50% of the referrals were from the emergency department (ED). Therefore, an area for service improvement focused on changing referral practice. Previously we reported referrals for NIV from the medical wards was delayed or even neglected (Jolley et al. Thorax 2002). We hypothesised that directing attention on referrals from the ED would facilitate early access to NIV.
Methods: In January 2006, the team’s proposed changes to the service were established: (1) Named “link” ED consultant: (2) Teaching sessions to promote understanding and indications for NIV for junior doctors in ED, critical care, respiratory and general medicine; (3) General presentation of NIV service data to highlight awareness; (4) Teaching sessions for ED nurses. Data were collected prospectively. Hospital mortality was monitored as an outcome measure. We compared 2004–2005 audit (pre-intervention) with the 2006 audit (post-intervention; January 2006–December 2006).
Results: ED referrals increased from 42% to 72% with medical ward referrals falling from 45% to 17%. In the post-intervention group 53% were started on NIV in the ED compared with 33% previously. Despite the similarity in the severity of acidosis, we showed an absolute rise in hospital survival of 5%, from 65% to 80%. Furthermore, we observed a relative increase in the medical HDU nursing staff initiating NIV, from 17.6% to 30%.
Conclusion: A multifaceted approach to service modification may impact on hospital outcome. Changes in referral practice and location for initiation of NIV can be achieved by increasing awareness among ED staff, and general and respiratory physicians. Improved hospital survival with service changes was not associated with lower level of respiratory acidosis at initiation of NIV and thus may reflect other differences between the two groups.
OXYGEN THERAPY BEFORE INITIATION OF NON-INVASIVE VENTILATION IN COPD PATIENTS PRESENTING WITH RESPIRATORY FAILURE
M. Haris, N. Stevenson, A. Safdar, S. Jones, J. G. Williams. North Cheshire Hospitals NHS Trust, UK
Background: Respiratory failure is a common manifestation of acute exacerbation of chronic obstructive pulmonary disease (AECOPD), with up to 20% of patients developing respiratory acidosis. COPD patients are reliant on hypoxic respiratory drive, and uncontrolled oxygen therapy has proven to precipitate hypercapnic respiratory failure. Although non-invasive ventilation (NIV) has been shown to be an effective treatment for respiratory failure, baseline pH is an important factor in determining the success of NIV.
Aims: To evaluate whether controlled oxygen therapy in AECOPD before initiating NIV influenced outcome.
Methods: A retrospective audit of 61 consecutive patients with AECOPD who received NIV for type 2 respiratory failure was performed. Patients were subdivided into those receiving controlled (⩽28% venture mask or ⩽4 litres nasal specs) or uncontrolled oxygen therapy before starting NIV. Outcome measures included mortality and pH. Data were analysed using non-parametric tests (SPSS).
Results: 61 patients with a mean (SD) age 69 (11) years (female: male 34 (56%): 27 (44%)) were studied. Mean (SD) pre-admission % predicted FEV1 was 43 (22)%. The majority (94%) were current or ex-smokers. Performance status 3 (IQR 3–4).
Conclusion: Even in these enlightened days uncontrolled oxygen therapy is still being given by those responsible for initiating treatment for AECOPD. Uncontrolled oxygen therapy is associated with a significantly increased degree of respiratory acidosis requiring NIV, and therefore increased mortality risk. There was no significant difference in the length of stay. All patients with AECOPD should have controlled oxygen therapy, aiming at arterial oxygen saturation of 90%. NIV should only be initiated in patients in whom respiratory acidosis persists despite maximal medical treatment on controlled oxygen therapy.
AN EXPLORATORY STUDY OF PSYCHOSOCIAL FACTORS IN THE PROCESS OF WEANING FROM MECHANICAL VENTILATION
D. Wade1, T. Sherry2, K. Lei2, L. Campbell-Stephen2, N. Hart1, J. Weinman3. 1Lane Fox Respiratory Unit, Department of Critical Care, St Thomas Hospital; 2Intensive Care Unit, Department of Critical Care, St Thomas Hospital; 3Department of Health Psychology, Institute of Psychiatry, Kings College London, UK
Background: Weaning from mechanical ventilation can be a difficult, time-consuming task for around 25% of patients. Furthermore, the more ventilation is prolonged, the greater the risk of long-term psychological illness and death. In about 20% of patients who fail to wean, there are no clearly identifiable physiological factors delaying weaning. Although the effect on weaning of psychosocial factors has been evaluated in a few studies, available data are limited. The aim of the current study was to explore the effect of psychosocial factors on weaning outcome, using quantitative and qualitative data, to inform future large-scale investigations.
Method: Study 1—A small prospective study was carried out at St Thomas’ Hospital intensive care unit (ICU). Independent variables were anxiety, depression, positive emotion, self-efficacy and social support from staff. Two dependent variables, number of days to wean and weaning success or failure, were recorded. Study 2—A cross-sectional study of patients who had failed to wean in the ICU was carried out using a semi-structured interview design. The interviews explored emotions, communication and social support during weaning. Data were analysed using a qualitative method, interpretative phenomenological analysis (IPA).
Results: Study 1—A total of 28 patients were approached, but 7 were excluded. Mean age was 61 years. Weaning failure rate was 28.6% and mean days to wean 8.57 (7.7). In a multiple regression, significant predictors of number of days to wean were anxiety (p = 0.020), self-efficacy (p = 0.022) and positive emotion (p = 0.030). Study 2—Six patients were interviewed. Mean age was 56.5 years and time receiving ventilation ranged from 4–26 weeks. The 5 master themes emerging from IPA analysis were “fear and danger”; “disorientation”, “loss and helplessness”, “inability to communicate”; and “availability of support”.
Conclusion: Patients weaning from mechanical ventilation in intensive care may suffer psychological distress that is exacerbated by their inability to communicate. Disorientation and anxiety may interfere with the weaning process while patient self-efficacy and social support from staff could protect against psychological distress and reduce failure to wean. These results should be regarded as pilot data and further studies using larger samples should be carried out.
D Wade is a Health Psychologist Trainee who is funded by a Service Innovation Grant provided by the Guy’s & St Thomas’ Charity.
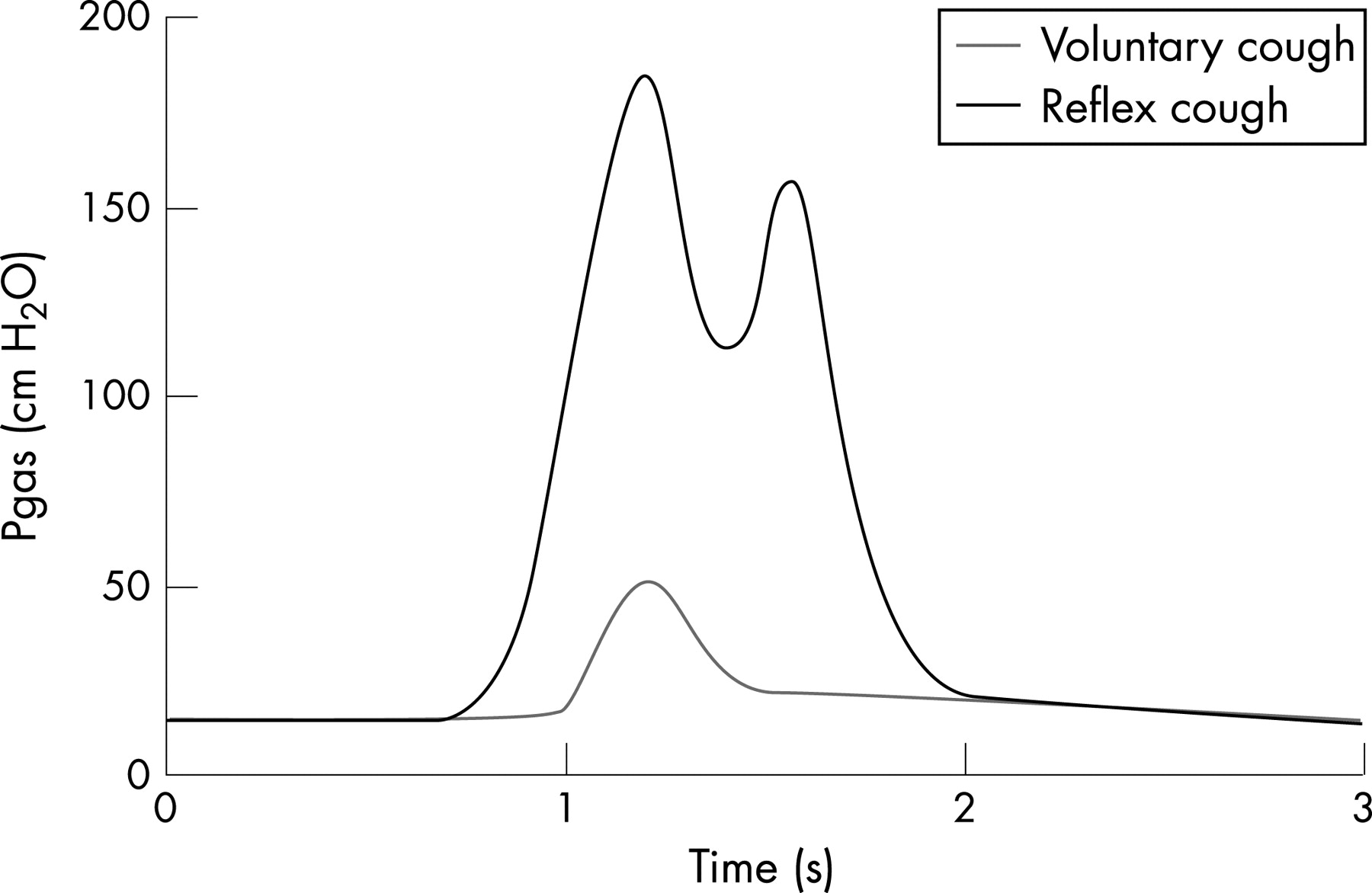
THE USE OF A NON-INVASIVE VENTILATION (NIV) PROFORMA IMPROVES SUCCESSFUL WEANING FROM NIV ON A RESPIRATORY WARD
A. Lane1, P. Murray1, M. Wood1, J. Bott2. 1Ashford and 2St Peters Hospitals NHS Trust, UK
Introduction: Non-invasive ventilation (NIV) is an established treatment for acute respiratory failure (ARF). A small prospective audit was previously carried out in 2004 to investigate the appropriateness, safety and efficacy of the NIV service on the respiratory ward. In response to the audit results, an NIV working party developed a proforma based on the British Thoracic Society (BTS) NIV recommendations to outline the assessment and treatment process for patients requiring NIV.
Method: Data were collected prospectively using the BTS audit tool from 80 consecutive patients requiring NIV between March 2005 and February 2006 (46 weeks). 15 incomplete data sets were excluded.
Results (n = 65): All patients were commenced on appropriate mode of ventilation. There were significant improvements in pH (p = 0.002), Pco2 (p = 0.002) and Po2 (p = 0.002). Of 20 patients with relative contraindications to NIV, excluding focal consolidation, 18 failed. N = 21 showed signs of focal consolidation on chest radiograph. Of these, 8 (38%) were successfully weaned.
Discussion: Overall, more patients were successfully weaned with proformas. The number of patients with contraindications given NIV markedly reduced compared to 2004; however, 90% of patients with contraindications (excluding focal consolidation) failed NIV. This concurs with the recommendation that NIV is not appropriate in the presence of contraindications unless the ceiling of treatment. The higher success rate for physiotherapists may be due to greater specialist knowledge of NIV than junior doctors/non-respiratory doctors initiating NIV out of hours/weekends, or that patients were sicker or had more contraindications (warrants further investigation).
Conclusion: The use of a hospital proforma, based on BTS guidelines, improved the success rate of NIV in a district general hospital respiratory ward. Patients with focal consolidation had good outcomes with NIV; those with contraindications did not.
USING A PROTOCOL REDUCES WEANING TIME IN NON-INVASIVE VENTILATION PATIENTS MANAGED ON MEDICAL WARDS
D. Daley1, K. Marshall1, K. Bryan2, W. Mcallister1. 1Royal Surrey County Hospital; 2University of Surrey, Guildford, UK
Introduction: Non-invasive ventilation (NIV) has become the gold standard for treatment of hypercapnic ventilatory failure in patients with chronic obstructive pulmonary disease (COPD) (Brochard 1995). Randomised controlled trials have shown that NIV reduces the need for tracheal intubation and reduces mortality and morbidity in patients with ventilatory failure (Lightowler 2003). NIV has also been shown to reduce weaning time from invasive ventilation in COPD patients (Nava 1998) but there are no studies investigating weaning time from NIV. The British Thoracic Society guidelines (2002) say that “Mention of weaning from NIV in papers or guidelines is vague and inconsistent”. NIV is increasingly provided on medical wards in many hospitals. Specialist respiratory teams are not always available to make decisions on weaning (National COPD Audit 2004). This creates inequity of care, particularly out of normal working hours, potentially slowing down the weaning process by either; weaning too slowly, or inappropriately rapidly, which may cause deterioration and prolong time on NIV. Weaning plans or protocols have been shown to assist clinical decision-making and provide a standardised care. Henneman (2001) showed a reduction in weaning time from formal ventilation in an ITU. If this is the case in ITU where a high level of clinical expertise is available around the clock, it may be even more applicable to the management of NIV on medical wards.
Aim: To explore whether using a protocol reduced weaning time for NIV.
Methods: A cohort study design was used. All adult patients treated with NIV on the medical wards were included. The first group included patients admitted between October 2005 and May 2006. The standard daily weaning method was used in which a weaning plan was decided by the senior physiotherapists and respiratory consultants. Following the introduction of the protocol, the second group of patients admitted between June 2006 and January 2007 were weaned according to the protocol. Both groups received standard medical treatment and NIV. There were 46 patients in Group 1 (COPD 28, LVF 11, other 7) and 45 patients in Group 2 (COPD 26, LVF 13, other 7). Clinical characteristics for both groups were not statistically significant. Pre-NIV pH for group 1 was 7.26 (range 7.07–7.38) and for group 2 was 7.24 (6.9–7.34). The mortality rate was 28% in group 1 and 24% in group 2.
Results: Results showed a statistically, significant reduction in the mean (SD) time on NIV from 6.04 (2.9) in group 1 to 3.64 (2.8) in group 2 (p<0.001). Further analysis of diagnostic subgroups showed a reduction in mean (SD) time on NIV for: (1) COPD patients in group 1 of 6.89 (3.1) days and in group 2 of 4.56 (2.90) days (p = 0.007). (2) LVF patients in group 1–4.45 (2.3) days and in group 2–2.61 (2.2) days (p = 0.065).
Conclusion: The BTS NIV guidelines (2002) advocate that NIV is managed in one dedicated area within a hospital. Critical care networks advocate that NIV should be managed in a level 1 area. In a hospital treating 100 NIV patients per year on level 1 and employing a step down policy to medical wards once weaned, £87,500 savings could be made with this reduction in number of days spent on NIV. There is, however, no national bench mark for length of time on NIV and this reduction may not be reflected elsewhere. There is much discussion about the benefits and possible harmful effects of using protocols. Our experience, although anecdotal, was that a protocol which enabled clinical reasoning gave staff at all levels more confidence and brought about improvement in communications and a more cohesive approach to managing our patients.
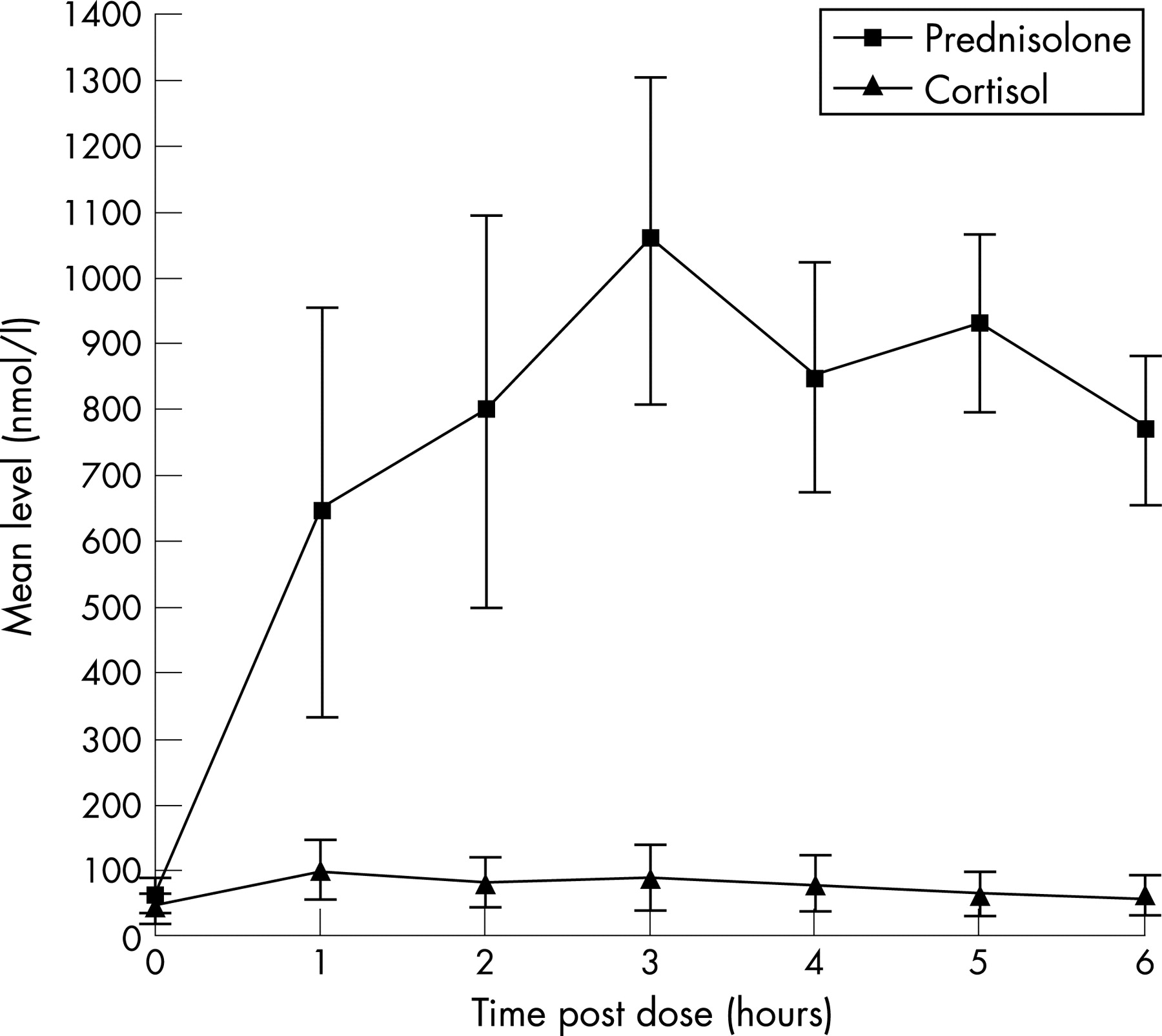
Respiratory physiology
USE OF THE DIAPHRAGM ELECTROMYOGRAM TO ASSESS THE RESPONSE TO BRONCHODILATOR THERAPY IN ASTHMA AND COPD
C. J. Jolley1, J. S. Steier1, J. Seymour1, K. Ward1, M. I. Polkey2, Y. M. Luo3, J. Moxham1. 1King’s College London School of Medicine, King’s College Hospital; 2Respiratory Muscle Laboratory, Royal Brompton Hospital, London, UK; 3Guangzhou Institute of Respiratory Disease, China
Introduction: Patients with asthma and chronic obstructive pulmonary disease (COPD) often report improvements in symptoms out of proportion to changes in standard lung function. Levels of neural respiratory drive (NRD), measured by quantifying the diaphragm electromyogram (EMGdi), are potentially a more sensitive measure of change in ventilatory load. We hypothesised that decreases in EMGdi would be greater than improvements in standard lung function following bronchodilator therapy in patients with asthma or COPD.
Methods: EMGdi was recorded at rest in 10 asthmatics (median FEV1 67.3 (30.0–130.4) %pred) and 3 patients with COPD (median FEV1 36.7 (20.7–58.8) %pred), before and 20 minutes after 2.5 mg nebulised salbutamol, using a multipair transoesophageal electrode. EMGdi was normalised to peak EMGdi recorded during maximal inspiratory manoeuvres, and corrected for inspiratory time and respiratory rate (EMGdi%index μV/min).
Results: See table. When patient groups were combined, reductions in EMGdi%index were greater than increases in FEV1 (p = 0.02) or peak flow rate (PEF) (p = 0.005).
Conclusion: EMGdi%index is potentially a sensitive biomarker of bronchodilator response, possibly more so than standard lung function in patients with airways obstruction, detecting subtle improvements in lung mechanics even in patients with “irreversible” disease.
EXPIRATORY MUSCLE AND COUGH FUNCTION AFTER ACUTE ISCHAEMIC STROKE
K. Ward1, J. Seymour1, C. Jolley1, J. Steier1, L. Kalra1, M. Polkey2, J. Moxham1. 1King’s College London; 2Royal Brompton Hospital, London, UK
Introduction: Stroke patients commonly aspirate and weak cough is associated with a higher incidence of lower respiratory tract infections (LRTIs) in this group. LRTIs cause more than 50% of in-hospital deaths after stroke. Effective cough requires coordinated inspiration, glottic closure and forced expiration. It has been shown that voluntary cough peak flow rate is lower in acute stroke patients compared with normals and that long-term stroke survivors have reduced expiratory mouth pressure (PE max). Reflex (involuntary, non-volitional) cough can be elicited in acute stroke patients with weak or absent voluntary cough, but the physiological basis for these differences has not been fully described. A study to assess expiratory muscle function in both stroke patients and healthy subjects, using both volitional and non-volitional physiological tests, was therefore devised.
Hypothesis: We hypothesised that poor performance on volitional tests of respiratory muscle function is a consequence of impaired ability to recruit and control the muscles rather than a reflection of true weakness.
Methods: Volitional tests—Maximum expiratory mouth pressure (PE max) and maximum voluntary cough gastric pressure (VC Pgas) were measured for each subject. Non-volitional tests—Maximum reflex cough gastric pressure was recorded (RC Pgas) for each subject. Reflex cough was induced using nebulised 5–20% tartaric acid, titrated to the strength required to produce ⩾5 coughs. Maximum gastric pressure was also measured after magnetic stimulation of the tenth thoracic nerve roots (Tw T10 Pgas). Stimulation of these nerve roots causes bilateral activation of the abdominal muscles including the recti and obliques and a consequent rise in gastric pressure in subjects with an intact peripheral nervous system and healthy muscles.
Results: Thirteen inpatients (4 female) with acute middle cerebral artery infarcts and 15 normal subjects (5 female) were studied. Mean (SD) age of the stroke patients was 60 (13) years and that of the normals was 55 (17) years. Although the normals tended to be younger the age difference was not statistically significant (p = 0.1066). Mann–Whitney U tests were used to compare differences between stroke patients and controls. Values shown in the table are medians (range) and the units of pressure are cm H20.
Conclusion: Although stroke patients may perform poorly on volitional tests of expiratory muscle function and cough, the results from non-volitional tests indicate that the muscles themselves are not weak. Instead, there could be disordered voluntary activation of the expiratory muscles after stroke.
MULTI-DIMENSIONAL ASSESSMENT OF CLINICAL DYSPNOEA
J. Yorke1, S. Moosavi4, C. Shuldham2, C. Haigh1, M. Lau-Walker2, P. Barnes4, P. W. Jones3. 1University of Salford; 2Royal Brompton and Harefield NHS Trust; 3St George’s Hospital Trust; 1NHLI, Imperial College, London, UK
Background: Dyspnoea consists of multiple dimensions: intensity, quality, and affective. In clinical practice and research, measurement focuses on intensity; in part because there is no tool available that measures the multidimensionality of dyspnoea.
Aim: To develop a tool that captures multiple dimensions of clinical dyspnoea.
Methods: Items suitable for inclusion in a multi-dimension dyspnoea instrument were identified following an extensive literature review. After removal of duplicates, 81 were assembled into a list and administered to 123 patients with COPD (mean (SD) age 69 (8) years, 62 male, mean (SD) FEV1/FVC 55 (12)%pred, mean (SD) MRC grade 3.0 (1.0)); 129 patients with interstitial lung disease (age 50 (12) years, 47 male, FEV1/FVC 72 (22)%pred, MRC grade 3.1 (2.0)) and 106 patients with chronic heart failure (age 68 (11) years, 72 male, mean (SD) ejection fraction 35 (15)%, MRC grade 2.6 (1)). Patients were asked to respond to each item using: none, mild, moderate, or severe. A hierarchical method of item reduction was used to exclude items if more than 60% of patients from each group rated them as “none” or if they were influenced by age or gender. Principal components analysis (PCA) was used to test for the presence of different domains and test internal consistency.
Results: 24 items were removed because of low response rate or gender or age bias. Of the remaining 57 items, 30 were experienced by all three patient groups, and 14 items were specific to a single disease. PCA of these 57 items produced a 3-component solution (Cronbach’s α = 0.974). Component 1 (n = 25) related to various qualities of dyspnoea, eg, “work/effort”, “air hunger”; Component 2 (n = 12) related to affect, eg, “panicky”, “frightening”; Component 3 (n = 6) related to a mixed item collection including “constricted breathing”, “light-headedness”. Fifteen items did not reach the pre-specified >0.5 factor loading threshold onto any of the 3 components, eg, “puffed”, “gasping”.
Conclusion: This is the largest analysis of dyspnoea descriptors yet performed. The experience of dyspnoea among patients with cardiopulmonary disease includes separate qualitative and affective domains, demonstrating that dyspnoea is multi-dimensional. The identified dyspnoea descriptors will form the basis of a new instrument Multi-Dimensional Dyspnoea Questionnaire for the evaluation and quantification of dyspnoea.
USE OF THE ECCS REFERENCE EQUATIONS IN THE INTERPRETATION OF LUNG FUNCTION TESTS: TIME TO CHANGE?
C. Newall, A. Matthee, A. Sommariva, M. Slijepcevic, E. Neuhoff, D. Wessels. PAREXEL International
Introduction: The ECCS (Quanjer et al, 1983) prediction equations are used universally in the UK for the comparison of measured lung function indices to so-called “reference values”. However, these equations were developed over 20 years ago and may not be appropriate for the current population. Furthermore, the original equations do not include 18–25-year-olds and many lung function labs assume an age of 25 when calculating reference values for these individuals. The aims of this study were firstly, to investigate the applicability of the ECCS equations in healthy individuals from the current population; secondly, to develop new equations for the prediction of spirometry parameters; and thirdly, to investigate whether 18–25-year-olds should be included in the formulation of new equations.
Methods: We performed spirometry in 240 healthy, Caucasian, non-smoking males (mean age 30.6 years, range 18–47) according to ARTP guidelines (ARTP/BTS, 1994). Subjects were divided into 3 groups: Group 1, >26 years; Group 2, 18-25 years; Group 3, all subjects. In Groups 1 and 3 linear regression was used to develop summary equations for the prediction of spirometry parameters and all comparisons were performed using paired t tests.
Results: There were significant differences between the mean measured and ECCS predicted values for both FEV1 and FVC (Group 1) with the measured values being greater than predicted in 144/199 subjects for FEV1 and 164/199 subjects for FVC. This was similar for Group 3 where the measured values were greater than the ECCS predicted in 168/240 and 190/240 subjects for FEV1 and FVC, respectively. In Group 2, there were significant differences between the new predicted values obtained via linear regression in Group 3 and those obtained using extrapolation of the equations for Group 1. However, in both cases the actual measurements were similar to the predicted values.
Conclusion: We conclude that the ECCS reference equations underestimate lung function parameters in the majority of subjects which may result in under-diagnosis of lung disease when measured values are at the lower end of the ECCS defined ‘normal’ range. There is a need to develop a new set of prediction equations for use with today’s population.
DIMENSIONS OF BREATHLESSNESS AT REST AND ON EXERTION IN RESPIRATORY DISEASE
P. S. Albert1, S. Jack1, E. Bertella1, P. M. A. Calverley1, J. Smith2. 1University Hospital Aintree; 2Wythenshawe Hospital, Manchester, UK
Background: Dyspnoea is a major symptom experienced by patients with lung disease; however, the mechanisms remain obscure. Simon and colleagues have shown that patients with pathophysiologic conditions experience qualitatively different sensations of dyspnoea; however, it is not known whether descriptors at rest reflect those sensations on exercise. The aim of this study was to investigate whether descriptors of dyspnoea were comparable at rest and exercise in patients with lung disease.
Methods: 202 outpatients completed a questionnaire comprising 45 descriptors of breathlessness (Elliott 1991), (chronic obstructive pulmonary disease (COPD) (n = 65), asthma (n = 60), pulmonary fibrosis (PF) (n = 41) and idiopathic hyperventilation (IH) (n = 36)). Patients described breathlessness both at rest and on exercise. Recent spirometry and diagnosis were determined by review of medical records. Patterns in the descriptor responses were assessed using principle components analysis (promax rotation). This analysis reduces the large data set to a small number of components representing the dimensions of the sensation of breathlessness.
Results: On exercise, the analysis suggested 7 components of breathlessness, explaining 64.6% of the variance (KMO = 0.93, Bartletts p<0.001): (1) air hunger 39.8%; (2) affective 6.5%; (3) nociceptive 4.9%; (4) attention 4.2%; (5) regulation 3.2%; (6) miscellaneous 3.2%; and (7) sighing 2.8%. At rest, the analysis suggested 6 components, explaining 63.1% of the variance (KMO = 0.93, Bartletts p<0.001): (1) affective 41.5%; (2) air hunger 6.2%; (3) nociceptive 5.4%; (4) wheeze 3.7%; (5) regulation 3.2%; and (6) sighing 3.0%.
Conclusion: The sensation of breathlessness in chronic respiratory diseases is dominated by descriptions of air hunger on exertion but by affective descriptions at rest. On exertion, mechanical limitation may occur in the form of encroachment on inspiratory reserve volume as the expiratory lung volume approaches total lung capacity. This encroachment may lead to the sensation of air hunger. At rest voluntary mechanisms of ventilatory control are more dominant than on exertion, and this may explain the dominance of the affective component of breathlessness on exercise.
ADJUSTMENT OF DIFFUSING CAPACITY FOR CARBON MONOXIDE (DLCO) FOR HAEMOGLOBIN VALUE IN UK LABORATORIES
H. Patel, M. J. Cushley. Dudley Group of Hospitals, UK
Introduction: The American Thoracic Society/European Respiratory Society (ATS/ERS) guidelines on standardisation of lung function testing state that diffusing capacity for carbon monoxide (DLCO) change can be substantial as a function of haemoglobin concentration and DLCO results should be adjusted to a standard haemoglobin value of 14.6 g/dl for males and 13.4 g/dl for females.
Methods: To assess compliance with these guidelines we surveyed 225 respiratory laboratories in the UK asking whether DLCO adjustment for haemoglobin was part of their routine clinical practice. We also reviewed DLCO requests and results from our respiratory laboratory over the period March–May 2007.
Results: 101 (45%) completed responses were returned. 53 laboratories use a request form, which has a section for the haemoglobin value. 68 laboratories reported that the haemoglobin value was only rarely recorded on the request form with only 1 laboratory indicating the haemoglobin value was included the majority of the time. If the haemoglobin value was available 74 laboratories would adjust the DLCO value routinely as per the guideline, 8 would not provide an adjustment irrespective of the haemoglobin value, and 19 would adjust if the haemoglobin value was outside the range 11–19 g/dl. 322 DLCO tests were carried out at a large district general hospital over the 3 month period March–May 2007. 55 (17%) requests included the haemoglobin value on the form (a section for haemoglobin value is part of the request form). Using the hospital electronic results system a further 93 patients were identified as having had a haemoglobin value within the 2 weeks prior to the test. In 12 of the 148 patients the adjusted DLCO result changed the severity category of the reduction of DLCO.
Conclusion: The majority of UK laboratories do not adjust DLCO values for haemoglobin concentration. In 8% of cases in our hospital haemoglobin adjustment changed the severity grading of the decrease in DLCO, possibly influencing clinical management. Increasing use of electronic pathology results systems allows easy access to haemoglobin results enabling adjustment to be made in a substantial number of patients tested.
HYPERINFLATION IN HEALTHY ADULTS INDUCED BY BREATHING AGAINST A CONSTANT RESPIRATORY LOAD
T. Powell, E. M. Williams. University of Glamorgan, UK
Introduction: Overcoming raised airway resistance in chronic obstructive pulmonary disease (COPD) requires increased work of breathing and often hyperinflation is present, providing a mechanism for alleviating this extra work. A new method for applying a constant resistance (RK) throughout the respiratory cycle was used to raise airway resistance in healthy adult volunteers. The principal aim of this study was to assess the breathing pattern response to increased RK during a series of 6 minute trials. Early results prompted a secondary study to quantify the degree of hyperinflation associated with increased RK.
Methods: This study was ethically approved with all participants giving informed consent. After spirometry participants (n = 5, 3F, FEV1% pred 94–123) were seated and asked to breathe through the RK device (MicroRMA, Micro Medical, Kent, UK) at a breathing rate of 15 breaths/min paced using an electronic metronome. A series of seven 6 minute trials was completed in random order at a RK of 0, 0.25, 0.5, 0.75, 1.0 and 1.5 kPa.L.sec−1. After 6 minutes the cumulative energy and tidal volume, VT were recorded. A group of 6 (4F) healthy individuals (FEV1%pred 94–123) underwent spirometry and whole-body plethysmography (Master Screen Body, Jaeger, Germany) allowing the intra-thoracic gas volume (ITGV), residual volume (RV) and total lung capacity (TLC) to be assessed. Once the constant resistance device was attached distally to the occlusion valve, ITGV measurements were repeated at similar RK as before. A repeated measures ANOVA was used to assess for statistical significance (p<0.05).
Results: Participants responded to increased RK in the 6 minute trials by maintaining tidal volume at around 0.65 L (p = 0.613), increasing the cumulative energy used (p<0.01) and work (J/L) (p<0.01) (see table 1). With exposure to similar RK, TLC and RV remained constant (p>0.05), while ITGV increased significantly (p = 0.02) (see table 2).
Conclusion: In healthy subjects the work of breathing increases with increasing RK, with energy and work values increasing 4 fold between 0.25 to 1.5 kPa.L.sec−1. The tidal volume and breathing rate remained constant through all trials so any extra work of breathing must have been met by an increased driving pressure generated by the respiratory muscles. The increase in ITGV, particularly at the highest resistance, illustrates how the lungs become hyperinflated thereby reducing the work of breathing through storage of elastic energy. This hyperinflationary response mimics hyperinflation seen in COPD patients.
IS PACED BREATHING IMPORTANT WHEN APPLYING A CONSTANT RESISTANCE TEST?
T. Powell, E. M. Williams. University of Glamorgan, UK
Introduction: Using a new method of constant resistance (RK) throughout the respiratory cycle irrespective of flow, energy used for breathing was assessed during a series of 6 minute trials while seated and during a 6 minute treadmill walking test (6MWT). We aimed to quantify the work of breathing (as energy used) during these trials with increased levels of added RK and to define if paced breathing altered energy usage.
Methods: This study was ethically approved and all subjects (n = 5, 3F) gave informed consent. After spirometry (FEV1 % predicted 94–123) subjects were seated and asked to breathe through the Rk device (MicroRMA, Micro Medical) and complete a random series of seven 6 minute trials, with the RK set at 0, 0.25, 0.5, 0.75, 1.0 and 1.5 kPa.L.sec−1 and while walking on a treadmill at 4 km/h with the RK at 0, with a minimum 10 minute break between each trial. The trials were completed over 2 visits and the participants were asked to maintain a breathing rate of 15 breathes/min, paced by an electronic metronome. Over a further two visits participants repeated the seven trials in the same order but at a volitional or self-paced breathing rate. At 6 minutes in each trial, cumulative energy, tidal volume, and total breath number was recorded. A two-way repeated measures ANOVA was used to assess for statistical difference (Sigmastat V3, Systat, UK).
Results: There was a significant differences (p = 0.023) between paced and self-paced breathing in total energy used (p = 0.023) and VT (p = 0.012), but not between breaths per minute (p = 0.417) and work rate (p = 0.057) (see table).
Conclusion: The greatest differences between the paced and self-paced trials is seen when using a mid-range RK (0.5–1 kPa.L.sec−1), with self-paced breathing being the more efficient. At the higher RK breathing has to be forced and matches that of walking. Despite these differences the work of breathing (J/L) done in each condition is similar, suggesting that self-paced breathing can be used when using this device to apply a continuous resistance. This will make its application in patients with lung diseases such as chronic obstructive pulmonary disease (COPD) that much easier. In COPD it is known that lung mechanics are compromised making paced breathing more difficult.
MEASURING CARBON MONOXIDE TRANSFER HELPS TO UNDERSTAND THE PATHOPHYSIOLOGY OF LUNG DISEASE IN PATIENTS WITH SICKLE CELL ANAEMIA
C. I. Bloom1, A. R. Cummin2, K. Murphy2. 1Hillingdon Hospital; 2Charing Cross Hospital, London, UK
Introduction: The median age of survival of patients with sickle cell disease is 42 years in men and 48 years in women. Although more than 20% of adults with sickle cell anaemia die from pulmonary complications, including acute chest syndrome, sickle cell chronic lung disease and pulmonary hypertension, the pathophysiological processes are poorly understood. Lung function studies in adult sickle cell patients focus predominantly on spirometry; very little data are available on the carbon monoxide transfer factor (TL,CO) as well as CO transfer coefficient (KCO) measurements. Examination of the KCO and alveolar volume separately provides information on pathophysiology which cannot be obtained from their product, the TL,CO. In this study we examined the results of TL,CO and KCO measurements in adult patients with sickle cell disease to see if there was a pattern which might explain the pathophysiological process of chronic sickle cell lung disease.
Method: A retrospective study was carried out on adult patients with sickle cell anaemia referred for outpatient lung function tests, during the period 1996 to 2007. Spirometry was measured in the sitting position, using a closed-circuit spirometer. Diffusion studies were measured using the single-breath holding carbon monoxide method, and was corrected for haemoglobin concentration. The reference values used were for an Afro-Caribbean population. Other data collected included serum haemoglobin concentration and electrophoresis, acute chest syndrome history, spirometry and CO diffusion studies.
Results: 32 patients were included in the study, the mean age was 34 years and 53% were males. 30 patients had Hb-SS disease and 2 patients had Hb-SC disease, with a mean Hb concentration of 9.3 g/d. 58% had a history of acute chest syndrome, 5 patients were current smokers and 4 were ex-smokers. All patients were Afro-Caribbean, with a mean BMI of 23 kg/m. The mean (SEM) percent predicted for FEV1 was 81.8% (2.9), FVC 80.9% (2.25), and FEV1/FVC 82.9% (1.49). Two patients had an obstructive defect, as defined by a FEV1/FVC <70%, and 18 patients had a FEV1/FVC >80%. The mean (SEM) percent predicted for TL,CO was 82.6% (3.2), and KCO was 110.4% (3.2). The was no statistical difference between the mean KCO and TL,CO values between patients with or without a history of acute chest syndrome.
Conclusion: Patients with sickle cell anaemia had a lower than predicted alveolar volume and TL,CO, and a higher than predicted KCO. This is the pattern associated with loss of alveolar units. The KCO is higher than predicted consistent with an increased blood flow per unit volume to the lung tissue that remains. We propose that this loss of alveolar units is the consequence of chronic occult microvascular injury. The two previous small studies which included TL,CO and KCO data showed a lower than predicted TL,CO and slightly lower than predicted KCO.3 4 This is the pattern seen in secondary pulmonary hypertension and diffuse alveolar damage. It may be that these patients were more severely affected than the patients in our study. We suggest that measuring TL,CO and KCO gives useful information on the pathophysiology of the disease process causing chronic lung disease in sickle cell anaemia. Measurements of TL,CO and KCO might provide an early indication of the pulmonary vascular disease which could be used as guide for intervention with established treatments such as hydroxycarbamide (hydroxyurea), and potential future treatments such as sildenafil.
Asthma: clinical trials
PREDNISOLONE PHARMACOKINETICS IN SEVERE ASTHMATICS: DELAYED ABSORPTION AND FAILURE TO SUPPRESS ENDOGENOUS CORTISOL
P. Macedo, D. Campbell, S. R. Durham, K. F. Chung, A. Menzies-Gow. Royal Brompton Hospital, London, UK
Background: The pharmacokinetics (PK) of prednisolone in severe asthma has not been formally established. PK studies have been predominantly carried out in healthy volunteers and mild asthmatics. The half life of prednisolone is between 2–3.5 hours. Compliance has therefore been assessed by measuring prednisolone levels at 2 hours post dose—levels should be high with corresponding suppressed endogenous cortisol (<20 nmol/l). Formal prednisolone absorption studies are performed when levels do not correlate with patient history.
Aims: To establish if previous low/undetectable prednisolone levels in severe asthmatics were due to non-compliance or abnormal pharmacokinetics.
Methods: Retrospective analysis of prednisolone and cortisol levels in 10 severe asthmatic patients (BTS/SIGN guidelines Step 5) who underwent formal absorption studies was performed. Each patient had baseline blood tests before being witnessed taking their maintenance dose of prednisolone. Blood tests were repeated at hourly intervals for 6 hours. Prednisolone and cortisol levels were measured by high performance liquid chromatography.
Results: 90% of patients were female, with a mean age 35 years, mean asthma duration of 22 years and mean FEV1 of 63% predicted. Nine patients were on prednisolone (mean duration 5.5 years), mean dose 35 mg per day (range 10–60 mg). Four patients were on enteric-coated (EC) tablets. One patient had been on dexamethasone prior to the study. The fig demonstrates the mean prednisolone/cortisol levels for all patients. Four patients had peak levels within 3 hours, two at 4 hours, three at 5 hours and one at 6 hours post dose. There was no correlation between peak levels and dose taken. EC preparations did not affect absorption. Only 20% of patients had cortisol levels <20 nmol/l throughout the study. In 70% of patients, cortisol levels took at least 3 hours post prednisolone to start to fall—none were completely suppressed.
Conclusion: In our retrospective analysis, 60% of patients had delayed prednisolone absorption and 80% did not have appropriately suppressed cortisol levels. One-off prednisolone/cortisol levels at 2 hours post dose may not be a reliable tool to establish compliance. A prospective study on the pharmacokinetics of prednisolone in severe asthma is required.
USAGE OF A NEW ELECTRONIC ASTHMA ACTION PLAN IN PRIMARY CARE
N. J. Roberts1, G. Evans2, P. Blenkhorn2, M. R. Partridge1. 1Imperial College London, NHLI Division at Charing Cross Hospital; 2University of Manchester, Dept Informatics, UK
Background: Self management education including the use of a written asthma action plan improves outcomes for those with asthma. We have developed and assessed an electronic pictorial asthma action plan. The software enables patient and health care professional together to construct a personalised plan. The package also contains prescription information which automatically checks the dosages used, maximises therapy in each of the zones of the action plan, and calculates peak flow levels at which action should be taken.
Methods: 21 general practices in West London were approached by letter and 10/21 (47%) responded to a request to trial the electronic asthma action plan (E-AAP). The software was installed on all clinic computers and after a 4 month period, usage data were collected. A questionnaire was given to all doctors and nurses to assess their views.
Results: 190 plans had been printed by 43 healthcare professionals (32 doctors, 11 nurses), with doctors printing proportionally slightly more (139/190 (73%)) than the nurses (37/190 (27%)). In those that used the software the rate ranged from 1–28 plans being printed by individual staff. Most of the plans were printed in the format of picture and text together 116/190 (61%), with a smaller proportion printing the pictorial plans without words (31/190, 16%) or text alone (26/190, 14%). 32 health care professionals completed a questionnaire about the E-AAP (21 doctors and 11 nurses). 18/32 (56.3%) stated that they had not used the software at all and 14/32 (44%) used it between 1–5 times. 25/32 (78.1%) thought that similar plans for children would be useful and 21/32 (65.6%) stated that COPD plans would be helpful.
Conclusion: Nearly half of all healthcare professionals given access to easy to use E-AAP software used it to produce personalised pictorial asthma plans for their patients. The package overcomes problems of access to paper templates and the calculating of peak flow rates and prompts users on the correct completion of an action plan. The pictorial format ensures the usefulness even for those who may have impaired literacy skills.
Funding: Trevor Clay Memorial Grant – BLF.
REAL LIFE EFFECTIVENESS IN ASTHMA OF SYMBICORT MAINTENANCE AND RELIEVER THERAPY: RESULTS OF THE RELEASE STUDY
I. Small. Peterhead Health Centre, UK
Introduction: The properties of the components of Symbicort® (budesonide/formoterol) allow it to be used as both a maintenance therapy and a reliever therapy in the management of asthma. It can act as a traditional reliever due to the fast onset of action of formoterol, as a preventer due to the inhaled corticosteroid (ICS) budesonide, and as a controller due to the long duration of action of formoterol. This new asthma management approach to asthma has been supported by the Global Initiative for Asthma (GINA) guidelines (GINA 2006).
Methods: The aim of this phase III open-label, naturalistic, UK multicentre study was to compare budesonide/formoterol maintenance and reliever therapy (Symbicort SMART®) (budesonide 200 µg/inhalation and formoterol 6 µg/inhalation), with previous therapy in patients with an RCP-3 score >0. The mean baseline FEV1 measurement was 2.66 litres (95% CI 2.60 to 2.73). The primary outcome measure was a change in Asthma Control Questionnaire (ACQ) score from baseline to 26 weeks. Secondary measures included the change in Asthma Quality of Life Questionnaire Standard (AQLQ(S)) domain and overall scores, Satisfaction with Asthma Treatment Questionnaire (SATQ) scores, individual and total RCP-3 scores from baseline, as well as study medication use.
Results: After 26 weeks of treatment with budesonide/formoterol maintenance and reliever therapy (n = 571), there were significant and clinically relevant improvements in asthma control compared with previous asthma therapy (see table). Treatment benefits on ACQ and AQLQ scores were well-established after 4 weeks with continued improvement over 6 months (see table). These results were independent of previous therapy with ICS alone or with a long-acting β2-agonist (LABA), either additionally or as a combination product. Total RCP-3 score significantly improved compared to previous asthma therapy (mean change −0.9, p<0.0001). The mean as-needed use as a reliever was <1 inhalation/day with little evidence of overuse. Patients were more satisfied with budesonide/formoterol maintenance and reliever therapy than their previous asthma therapy in all respects, with significant changes in SATQ overall and domain scores. Budesonide/formoterol maintenance and reliever therapy was well tolerated over the 26-week treatment period, with only 9 (1.57%) patients discontinuing due to causally related adverse events.
Conclusion: In a real life setting budesonide/formoterol maintenance and reliever therapy provided sustained improvements in clinical control compared with all previous asthma therapies.
THE EFFECTIVENESS OF A DIFFICULT ASTHMA SERVICE FROM THE PATIENT’S PERSPECTIVE
B. Hargadon, P. Haldar, S. Mckenna, M. Shelley, H. Pateman, M. Bourne, I. Pavord. University Hospitals of Leicester, UK
Introduction: Difficult asthma is a multifaceted disorder that has led to the development of specialist services aimed at providing a detailed assessment of factors associated with poor asthma control, together with a multidisciplinary approach that is tailored to individual needs. Studies have shown this approach is effective for identifying poor compliance, alternative and additional diagnoses and coexistent psychosocial problems. However, little is known about the patient’s perspective of being managed in this setting.
Methods: We conducted a survey of 76 patients (29 male, mean age 49.4 years) that have attended the Glenfield Hospital difficult asthma clinic for over 12 months. Patients were asked to complete a questionnaire of their experience with different aspects of the service and its impact on their asthma control. Psychological services are not a component of the multidisciplinary care pathway provided by the clinic. We chose to examine the impact of the clinic on changes in psychological status, by asking patients to complete HADS and Nijmegen questionnaires and comparing scores with the same questionnaires that the patients completed at their baseline clinic assessment.
Results: Patients were comfortable with tests performed routinely at clinic visits. However, sputum induction was considered uncomfortable in a significantly greater proportion (26%) when compared with spirometry (9%) or FeNO (15%). 77% felt their asthma control was better or much better since attending the clinic. The remainder felt there had been no change.
Based on the results of the psychometric questionnaires 21% had anxiety disorder (HADS–A >11, UK prevalence 13%), 11% depression (HADS-D >11, UK prevalence 11.4%) and 37% hyperventilation (Nijmegen >23) at first assessment. A significant improvement in psychosocial scores was seen in patients with pathological HADS at baseline (HADS-A mean change −2.65, p = 0.001; HADS-D mean change −2, p = 0.028).
Conclusion: The Glenfield difficult asthma service is welcomed by patients who generally feel intensive assessment is both acceptable and worthwhile. This is associated with a perception of improved asthma control. Despite the absence of a specialist psychological service, the clinic significantly improved psychological status for patients with clinically important psychological symptoms.
A UK SURVEY OF ORAL CORTICOSTEROID USE IN PATIENTS TREATED WITH OMALIZUMAB
R. Niven1, D. Mcbryan2. 1North West Lung Centre; 2Novartis UK
Background: Anti-IgE therapy with omalizumab is included at step 5 of the GINA 2006 treatment guidelines for patients with severe persistent allergic (IgE-mediated) asthma who remain uncontrolled despite treatment with high-dose inhaled corticosteroids, long-acting β2-agonists and other controller medications. Maintenance oral corticosteroids (OCS) are also included at this step, but these are associated with clinically significant side effects. Indeed, the BTS/SIGN 2005 guidelines state that the aim of long-term OCS therapy is to control asthma using the lowest possible dose or, if possible, to stop OCS completely. Both published and anecdotal evidence suggests that omalizumab therapy enables reduction or even cessation of maintenance OCS in some patients. To explore this further, an observational survey was carried out in a cohort of severe asthma patients receiving omalizumab in the UK.
Methods: Nine clinical centres (eight adult and one paediatric) were included in the survey, representing those in the UK with the most experience of prescribing omalizumab (in terms of numbers of patients being treated) and accounting for approximately half of all the omalizumab-treated patients in the UK at that time. Clinicians selected to lead the survey at each of the proposed centres were invited to participate and all agreed to take part. Using a questionnaire, the following information on patients who had continued with omalizumab therapy beyond 16 weeks was requested: total number receiving omalizumab therapy; number on OCS at baseline (initiation of omalizumab therapy); dose of OCS at baseline; number in whom OCS had subsequently been stopped by a clinician; number in whom the OCS dose had subsequently been reduced by a clinician but not stopped; current reduced dose of OCS in these patients; time period over which this reduction had been achieved; number in whom OCS dose had not been reduced. Based on previous clinician feedback, it was assumed that OCS dose reduction would not be attempted before a 16-week omalizumab responder assessment. OCS doses were converted to prednisolone equivalent calculated using a conversion table (BNF 53 Section 6.3.2 (March 2007)). One patient on maintenance triamcinolone by subcutaneous injection was included in the final analysis following conversion of the triamcinolone dose to an equivalent dose of prednisolone. As triamcinolone has glucocorticoid and anti-inflammatory profile similar to prednisolone, the inclusion of this patient was considered to be justified.
Results: A total of 65 patients were reported to be receiving omalizumab therapy. Of these, 33 were taking maintenance OCS at baseline. The mean OCS dose at baseline in all 33 patients was 22.6 mg, and at the time of data collection it had fallen to 11.6 mg, representing a mean absolute reduction of 11 mg (mean relative reduction = 48.6%). Eight patients (24.2%) taking OCS at baseline had stopped OCS. The mean OCS dose at baseline in this group was 15.3 mg. OCS dose was reduced in 18 patients (54.5%). The mean OCS dose at baseline in this group was 27.4 mg, and at the time of data collection it had fallen to 14.1 mg (absolute reduction = 13.3 mg; mean relative reduction = 48.7%). The mean time taken to achieve this reduction was 18.8 weeks. OCS dose had not been reduced in 7 patients (21.2%). In total, 26 (78.8%) patients on OCS at baseline were able to stop or reduce their OCS dose.
Conclusion: In UK practice, this naturalistically set small observational survey found that OCS use can be reduced or stopped in a large proportion (78.8%) of omalizumab-treated patients with severe persistent allergic (IgE-mediated) asthma who have continued omalizumab therapy beyond 16 weeks. These OCS dose reductions are likely to be clinically meaningful.
TREATMENT AND FOLLOW-UP OF ACUTE SEVERE ASTHMA: WHO DOES IT BEST?
H. Burhan, Q. Alam, M. J. Walshaw. Royal Liverpool University Hospital, UK
Introduction: The British Thoracic Society/Scottish Intercollegiate Guidelines Network (BTS/SIGN) asthma guidelines state that acute severe asthma patients should have GP follow up within 2 days and chest physician follow up within 4 weeks of discharge. We had the impression that the latter occurs infrequently and wished to investigate the reasons for this.
Aim: To determine whether patients admitted with an acute severe exacerbation of asthma were discharged in accordance with the BTS and SIGN Guidelines on Asthma.
Methods: We analysed 106 consecutive admissions coded as “acute severe exacerbation of asthma” from a large university teaching hospital over a 3 month period (July–September 2006), looking for compliance with the guidelines relating to discharge and follow-up.
Results: 36 notes were not available for analysis, 13 were miscoded, and 8 patients took their own discharge: of the remaining 47 cases (mean age 36.7 years, range 16–67, 16 male), 21 were triaged to chest wards while the remainder were treated in the emergency department or on the acute medicine ward.
Conclusion: Patients admitted with acute severe asthma looked after by chest physicians are discharged largely in keeping with BTS/SIGN criteria, unlike those cared for by other specialities. Rate of follow-up within 4 weeks is poor, and a worrying number of patients take their own discharge. Better liaison between primary and secondary care is required to ensure that patients are adequately followed up and that patients who take their own discharge are aware of the seriousness of their underlying diagnosis.
SEASONAL ALLERGIC RHINITIS IN ADULTS AND ADOLESCENTS
S. A. Salvilla2, S. S. Panesar2, S. Dhami1, A. Sheikh1. 1University of Edinburgh; 2Imperial College London, UK
Background: Seasonal allergic rhinitis (SAR) or “hay fever” is a common disorder manifesting with sneezing and an itchy, blocked or runny nose; it can also cause ocular symptoms. There is increasing evidence that most people are suboptimally managed resulting in avoidable morbidity, quality of life and school/work performance.
Methods: We worked with the BMJ’s Clinical Evidence and conducted a systematic review and evidence synthesis of all randomised control studies evaluating the effectiveness of topical or systemic antihistamines, decongestants, leukotriene antagonists, ipratropium bromide, intranasal and systemic corticosteroids. For a study to be included all patients had to be ⩾12 years with a clinician confirmed diagnosis of hay fever. The minimum length of follow-up was stipulated as being 2 weeks. Our primary outcome measure was the validated Juniper Rhinitis Quality of Life Questionnaire. Secondary outcomes of interest included visual analogue rhinitis symptom scores completed by the doctor and/or patient, medication usage and medication usage scores, days off school/work and adverse drug events.
Results: Antihistamines (76 RCTs), intranasal corticosteroids (67 RCTs) and a combination of pseudoephedrine with oral antihistamine (10 RCTs) are all effective in treating SAR. Numerous RCTs and two systematic reviews have found that intranasal corticosteroid use results in a greater reduction in nasal symptoms, but not ocular symptoms, when compared to oral antihistamines alone or used in combination with decongestants or leukotriene receptor antagonists. Systemic corticosteroids, leukotriene receptor antagonists with or without oral antihistamines are likely to be beneficial. Topical levocabastine is also of benefit in reducing rhinitis symptoms but there is at present conflicting evidence on the usefulness of other topical treatments (azelastine and ipratropium bromide) and oral decongestants on their own.
Conclusion: There is strong and consistent evidence to show that intranasal corticosteroids and oral antihistamines are both highly effective in the treatment of SAR and these should therefore be regarded as first-line agents; of the two, nasal corticosteroids are superior.
DEVELOPMENT OF AN ALGORITHM FOR THE ASSESSMENT OF RESPONSE TO TREATMENT WITH OMALIZUMAB
N. Thomson1, R. Niven2, L. Heaney3, A. Greening4, D. Mcbryan5. 1Gartnavel General Hospital; 2North West Lung Centre; 3Belfast City Hospital; 4Western General Hospital; 5Novartis UK
Introduction: Omalizumab, an anti-IgE antibody, has proven efficacy as add-on therapy in the treatment of severe persistent allergic (IgE-mediated) asthma, and represents a new treatment option for the most severe asthma patients who remain uncontrolled despite best available therapy. The Scottish Medicines Consortium (SMC) recently indicated that the proposed method of assessing a patient’s response to omalizumab after 16 weeks is overly subjective, and advised that the responder assessment should be strengthened to improve its objectivity.
Methods: Seven senior clinicians, based in Scotland, with a special interest in severe asthma, met with the aim of producing an objective algorithm to determine patient response to omalizumab after 16 weeks of therapy. The group identified key response indicators and appropriate metrics to evaluate and measure response based on a review of published work and expert opinion. The Mini Asthma Quality of Life Questionnaire (Mini-AQLQ) was selected as a suitable quality of life assessment instrument, with a ⩾0.5-point change in score being taken as clinically significant. In assessing asthma control, the Asthma Control Test (ACT) was favoured by the majority as it assesses symptoms over the previous 4 weeks, and has been shown to be responsive to changes in asthma control over time. A ⩾2 point improvement was regarded by the group to be clinically meaningful. Patients should have at least 4 weeks free from exacerbations before entering the assessment period. Thus, although assessments are made at week −4, it was agreed the baseline assessments should be at week 0. The algorithm was reviewed by a body of experienced severe asthma clinicians from England, Wales and Northern Ireland. There was broad agreement that it could be adopted for use throughout the UK.
Algorithm for the assessment of response to treatment with omalizumab: The final decision to continue with omalizumab therapy should be based on the key assessment criteria and a physician assessment of overall treatment response, the latter informed by the supportive assessments.

Key assessments:
(1) ACT: 5-items, self-administered survey, assesses previous 4 weeks.
(2) Mini-AQLQ: 15 items, assesses previous 2 weeks.
(3) Physician Global Evaluation Of Treatment Effectiveness: an overall clinical evaluation of improvement in asthma control at 16 weeks compared with baseline, based on all available information: patient interview, review of patient notes & diary (if used), and key & supportive response indicators; graded excellent, good, moderate, poor, or worsening; excellent/good evaluation indicates response to omalizumab treatment.
Supportive assessments:
(4) PEF: peak expiratory flow, performed within 15 minutes of waking on Mon, Wed, Fri.
(5) Exacerbations: worsening of asthma requiring additional oral corticosteroids. Patients should be exacerbation free for 4 weeks before baseline assessment.
(6) HCU: unscheduled healthcare utilisation: hospitalisation for asthma; A&E attendance; GP visit.
Conclusion: An algorithm has been developed which provides an objective tool to assess the response to omalizumab therapy after 16 weeks and which is considered applicable to every day management of severe persistent allergic asthma in the UK.
Education and training: issues in respiratory disease
IS IT IMPORTANT THAT RESPIRATORY PHYSICIANS REVIEW ALL GP REFERRAL LETTERS?
H. J. Steer, E. Bowie, V. Masani. Royal United Hospital, Bath, UK
Background: Patients referred by their GP with suspected lung cancer are seen within two weeks in the Urgent Suspected Lung Cancer (USLC) clinic. It is intended that these referrals are sent using an emailed or faxed proforma. In addition, all other GP referrals received by the department are reviewed by a consultant, and those with concerning symptoms who have not been referred using the USLC proforma, are triaged by the consultants into this pathway.
Aim: To evaluate the proportion of patients diagnosed with lung cancer who were referred by GPs using the USLC proforma, compared with those triaged into the USLC pathway after consultant review of the GP referral letter.
Method: Referral letters of all new patients seen in the USLC clinic for the year 2005 were reviewed and divided into three groups: (1) patients referred by their GP using the USLC proforma (email or fax); (2) patients referred by their GP not using the USLC proforma, but on review of the referral letter were clearly intended for referral to the USLC clinic; (3) no indication in the referral letter that the patient had suspected lung cancer, but triaged into the pathway after consultant review. Patient diagnoses were obtained from the lung MDT records and the hospital computer system.
Results: A total of 300 GP referrals were seen in the USLC clinic, yielding 89 patients with a diagnosis of primary lung cancer. Group 1 contained 125 patients, 50 of whom were diagnosed with lung cancer. Group 2 contained 113 referrals, 23 of whom were diagnosed with lung cancer. Group 3 contained 62 patients, 16 of whom were diagnosed with lung cancer. Overall 56% of lung cancers were referred directly by the GP using the USLC proforma, and 44% were triaged into the pathway after consultant review of the referral letter.
Conclusion: Without consultant review of all GP referrals, 44% of patients diagnosed with lung cancer would have been seen in a routine clinic and their diagnosis delayed. It is important that respiratory physicians continue to screen all referrals; which is increasingly relevant with the advent of “Choose and Book”.
UNDERSTANDING OF DISEASE IN PATIENTS NEWLY DIAGNOSED WITH TUBERCULOSIS IN EAST LONDON
R. H. Johns, S. Wurditu, G. Arnold, M. Darmalingam. Whipps Cross University Hospital NHS Trust, London, UK
Introduction: Tuberculosis (TB) is a preventable and curable infectious disease. Of 8171 new cases in England, Wales and Northern Ireland in 2006, 42% were in London, where TB has doubled in frequency since the late 1980s. Most cases (75%) occur in a non-UK born population, from a poor socioeconomic background with limited previous access to education, and who lack English as a first language. Poor understanding of disease may promote social stigmatisation, lack of empowerment, and poor treatment compliance. In London, only 79% of reported cases complete treatment.
Methods: To examine prevailing understanding of disease, we interviewed 28 patients newly diagnosed with TB attending Whipps Cross University Hospital (either in-patients or out-patients), between December 2006 and April 2007, prior to usual extensive nurse-led TB counselling. All patients understood English and consented to involvement in the study, which was approved by the local research department. Questions related to the cause, symptoms, spread and treatment of TB.
Results: Patients were 56% male and 44% female. 75% had pulmonary TB, and 25% had predominantly extrapulmonary TB. Mean (SD) age was 40 (15) years. English was not the first language of 59% of patients, 85% of whom were not born in the UK. 54% knew a close family member or friend who had previously had TB. 25% (7/28) were unable to describe at least one relevant symptom of TB. The most commonly reported symptoms were cough (7/21) and tiredness/weakness (7/21). Only 18% (5/28) realised TB could affect other organs besides lungs. 32% (9/28) did not know whether pulmonary TB was infectious, and 14% (4/28) thought it was not. 50% (14/28) did not know how TB was contracted. Only 52% (11/21) of those with pulmonary TB realised they could pose an infection risk to close contacts. 64% (18/28) knew TB could kill if not treated, but 32% (9/28) were not aware TB was curable. Only 46% (13/28) knew treatment lasted longer than one week, and only 32% (9/28) realised a full course of treatment was necessary even after symptoms had disappeared.
Conclusion: Patients newly diagnosed with TB in London have limited comprehension of TB symptoms, infectious spread, and the importance of a prolonged treatment course. Effective education targeting these aspects may enhance patient empowerment and compliance, and improve local TB control.
DEVELOPMENT OF A MULTIMEDIA RESPIRATORY RESOURCE TOOL FOR USE IN PRIMARY CARE
J. Dhami1, C. E. Wells2, W. Kong1, I. Mariaki1, S. Prigmore2, C. F. J. Rayner2. 1Wandsworth tPCT; 2St Georges Healthcare Trust, UK
Background: Those working in primary care are expected to manage patients with a considerable variety of conditions while keeping abreast of the latest national guidelines, management pathways and local referral processes. A major perceived barrier to practising evidence based care is the time and effort involved in accessing appropriate, reliable and up to date guidance. (O’Donnell CA, J Eval Clin Pract, 2004)
Aims: International, national and local respiratory guidelines have been available for many years (Pierson DJ, Respir Care, 2006) (Van Loo J, Health Info Libr J, 2006) The community respiratory team wanted to develop a single respiratory resource tool that would be both easy to access and use by the many different healthcare professionals working with respiratory patients. The aim was to produce a tool to coordinate management of patients with COPD or asthma, based on national guidelines (British Thoracic Society Asthma guidelines, November 2005 update; NICE COPD guidelines, February 2004) and containing local referral processes, disease information details and advice leaflets.
Methods: Two formats were explored (1) a paper-based format and (2) a CD-ROM; the CD-ROM was chosen as it was felt this would be smaller to store, less expensive to produce and would encourage a paperless system. For those who like to keep a paper system all PDF files could be printed and placed into a folder. It was also felt that by using the CD-ROM option updates could be done more regularly and also offered plenty of scope for expanding the contents. The contents of the resource tool were selected after having considered local needs and following best practice, this included patient information leaflets, PERF diaries and charts, inhaler and nebuliser device instruction sheets, local referral forms and national guidelines. Links to original sources of information, websites and training sites were also included. The guidelines quoted were chosen in concordance with local secondary care establishments to provide a consistent approach to patient care across the primary care trust (PCT).
Results: The resource tool was distributed as planned to all surgeries and community clinics in the locality and is now widely used. The demand for the disc was great among those working in PCT clinics so the content has been made available on the PCT intranet site.
Conclusion: After an initial four-month use an evaluation form has been sent out to all general practice surgeries to seek feedback regarding the usefulness, relevance of contents, relevance of links and the ease of use of the resource tool. The disc appears to have been well received by healthcare professionals and feedback to date has been very positive; results are still coming in and being evaluated formally (see fig).

TRAINING ABROAD: IS IT THE END?
T. P. Havelock1, M. Wakatsuki1, H. Marshall2, S. Bell3. 1Queen Alexandra Hospital; 2Southampton University Hospitals Trust; 3Portsmouth Hospitals Trust, UK
Introduction: Training abroad is important, but the opportunity to do so is under threat. Modernising Medical Careers (MMC) streamlines medical training and removes “gaps” where trainees seek opportunities abroad. Are these gaps important? Do trainees want to work abroad? Ironically MMC has also in the short term created a cohort of unemployed doctors who are looking abroad for training experiences. Where do trainees work abroad? Is the training of high quality?
Aims: To find out how many respiratory registrars from the Wessex Region had worked abroad, where and when they did this work. To find out how many wished to work abroad and the reasons they had not yet done so.
Methods: A cross-sectional electronic questionnaire survey of 33 Respiratory Specialist Registrars in the Wessex Region from 20 June 2007 until 17 July 2007 with one general reminder and one personal reminder to each non-respondent.
Results: Twenty four (73%) completed questionnaires were received, 19 (79%) of the respondents were UK graduates. 8 (32%) had worked abroad, 73% between SHO and Registrar stage, in a total of 11 posts 73% of which were 6–11 months in duration (one respondent worked abroad before coming to the UK and was excluded from the following analysis). 60% of posts offered some teaching and educational supervision for more than one hour a week of which 63% was rated as “good” or “excellent”. Two posts were accredited for training by the Royal College of Physicians; one retrospectively and one prospectively. 71% of trainees reported that they did not have trouble attaining a training post on their return to the UK and all would recommend working abroad to a colleague. Of the 16 respondents who did not travel abroad 50% had not done so for financial reasons and 44% family reasons. 88% of the respondents would like to work abroad in the future.
Discussion: This study shows that the majority of trainees want to work abroad and confirms the quality of the experience that they have had educationally, professionally and personally. We assume that the group of respiratory registrars in Wessex is representative of medical trainees nationally but this is obviously an area for further study. Previously working abroad has taken place when trainees are between rotations; now the guidance from the Departments of Health in the Gold Guide is that it will be taken as out-of-programme experience (OOPE). This will be at the discretion of the Deaneries who are under huge political and financial pressure to maximise the throughput of their training schemes and keep OOPE to a minimum. If experience abroad is truly valued by the authorities in postgraduate medical training then the same authorities must put their money and actions behind their statements. Unless they do so, this invaluable opportunity to broaden and enrich the education of medical trainees and to globalise the skills and experience of the future NHS workforce will be lost.

COMPREHENSION OF PICTORIAL ASTHMA ACTION PLANS BY SOMALIS AND MALAYSIANS
N. J. Roberts1, P. S. Wong2, Z. Mohamed3, R. Li-Cher Loh3, M. R. Partridge1. 1Imperial College London, NHLI Division at Charing Cross Hospital; 2International Medical University; 3University of Manchester, UK
Background: Self-management education including receipt of a written asthma action plan improves outcomes for those with asthma but not everyone can use the written word. We devised a set of pictorial representations of each of the components of a typical action plan and now report testing the plans with Somali and Malaysian patients with asthma.
Methods: Participants completed a guessability and translucency questionnaire for all 27 pictograms. Patients were then shown a complete pictorial asthma action plan and the concept of self-management explained. Understanding of the action which the patients would take in each clinical situation was assessed. Information regarding age, gender and school leaving age was recorded.
Results: Ten Somalis with asthma living in Manchester (mean age 43.5 (SD 13.4) years; 1 male, 9 females) and 19 patients with asthma attending an Outpatient clinic in Malaysia were studied (mean age 49.2 (SD 10.8) years; 6 males, 13 females). The Somali group had had little formal education; in the Malaysian group the mean school leaving age was 15 (SD 3.25) years. Guessability and translucency results showed that most of the pictograms were well understood and thought to be good representations. The Somali group scored over 5 for translucency scores for all but eight of the 27 pictograms. They had difficulty with pictograms depicting “taking extra doses of reliever medication”, the daytime/night-time use of inhalers and the caution sign. The Malaysian group rated the pictograms highly, but some left blank responses for some items such as the dry powder inhaler, reflecting uncommon use of this inhaler device in that country. All could state their medication, increase their inhalers in Zone 2, take appropriate action for Zone 3 and could suggest when to seek emergency treatment.
Conclusion: The pictorial plans were well understood in both groups and comprehensibility was similar among patients in these two cultural groups to that which we have previously demonstrated in a UK population.
INTERCOSTAL DRAIN INSERTION: A SURVEY OF GENERAL MEDICAL REGISTRARS IN THE MID TRENT REGION
E. L. Roddy, G. M. Cox. Kingsmill Hospital, UK
Introduction: Over recent years, standard chest tube insertion using large bore drains and blunt dissection has been replaced in many hospitals with insertion using a Seldinger method which, although the drains themselves are more expensive (£40 vs £5), has comparable efficacy and safety when compared with standard drain insertion and is perceived as less stressful for both patient and doctor! However, there are few data looking at this and ahead of a planned larger study we wanted to get an idea of current practice in our region as well as registrar’s confidence in chest drain insertion, which is increasingly being seen as the preserve of respiratory physicians rather that generalists.
Methods: All general medical registrars attending one of the regional study days were asked to fill in an anonymous questionnaire asking about chest drain insertion at their current hospital on the rotation, as well as their own personal experience of chest drain insertion: how many drains of each type they had inserted, when they last inserted a drain, how confident they felt with the Seldinger versus the standard method using a visual analogue scale, and an estimate of the time it would take them to insert a chest drain.
Results: Out of a total of 114 general medical registrars in the region, 43 answered the questionnaire giving a response rate of 38%. The year of training ranged from year one to year five with a median number of registrars in year three, and all hospitals on the rotation were represented with registrars from all subspecialties replying. Only one hospital out of seven in the region did not use Seldinger drains as the first-line ward chest drain. Registrars had each inserted an average of 15–20 large bore drains and 10–15 Seldinger type drains. Out of 43 respondents, 16 (37%) had not inserted a chest drain in the last six months, and of the 14 (33%) of respondents who had inserted a chest drain in the last month, 10 (71%) were respiratory registrars. On the visual analogue scale where 0 was not at all confident and 10 was very confident, registrars scored their confidence in inserting standard large bore chest drains at a mean of 6.31 versus 8.29 for Seldinger drains. This shows a significantly higher confidence level for inserting drains using the Seldinger method.(p = 0.001) Registrars also felt that the Seldinger drains were quicker to insert safely: 10–20 min per procedure versus 20–30 min for a standard chest drain using blunt dissection.
Conclusions: Despite a lack of evidence suggesting superiority of Seldinger chest drains in the management of pleural disease, and the higher cost of the new drains, there has been a widespread change in practice in our region, with the vast majority of hospitals now using Seldinger drains. Confidence in inserting large bore drains was much lower than for Seldinger drains, apart from in the subgroup of respiratory registrars, and the larger drains were felt to take longer to insert. This has implications for training and on-call insertion of chest drains, as most registrars will train in hospitals that use only Seldinger drains. We are currently carrying out a study directly comparing the two types of drains in terms of insertion times, efficacy and complication rates, before practice changes irrevocably towards Seldinger drain insertion.
A COMPARISON OF JUNIOR TRAINEES’ KNOWLEDGE OF NON-INVASIVE VENTILATION VERSUS THROMBOLYSIS
K. Furley, D. Parkinson, L. Sayers, N. Upile, G. Burns. Royal Victoria Infirmary, UK
Introduction: It has been identified at both local and national level that the use of non-invasive ventilation (NIV) in appropriate patients presenting with an exacerbation of chronic obstructive pulmonary disease (COPD) is suboptimal. This remains the case even when a service offering delivery is available. Anecdotal evidence suggests that this stems from a knowledge deficit amongst junior doctors responsible for the acute management of patients.
Aim: This study investigates relative awareness among (final year) undergraduates and junior doctors of two distinct but similarly efficacious, potentially life saving, emergency medical therapies: NIV in COPD exacerbations and thrombolysis in acute myocardial infarction.
Methods: Scenario-based questionnaires were distributed to 25 final year medical students and 33 foundation year 1 (F1) doctors. Results were analysed using a non-parametric Wilcoxon signed rank test.
Results: Recognition of the indication for thrombolysis (97% of F1s and 96% of undergraduates) was significantly greater than recognition of the indication for NIV (45.5% of F1s and 40% of undergraduates) in the respective settings. Previous studies show NIV reduces numbers of patients requiring ventilation by 44%, and six-week mortality by 50%. This clearly demonstrates the efficacy of treatment, but also the scale of excess resources incurred by a lack of awareness.
Conclusions: The reasons for this difference in awareness are multiple but may reflect the low profile COPD has suffered from in the past. This must change. Undergraduate and postgraduate teaching must stress the importance of this life saving intervention. Respiratory Physicians have a duty to “champion” this cause both locally and nationally.
Cystic fibrosis in children
ELASTASE INHIBITOR DX-890 PREVENTS IL-8 RELEASE STIMULATED BY NEUTROPHIL ELASTASE BUT NOT IL-8 RELEASE STIMULATED BY CYSTIC FIBROSIS SPUTUM
F. Dunlevy, E. Ennis, J. S. Elborn. Queen's University Belfast, UK
Introduction: Persistent inflammation of the cystic fibrosis (CF) airway is characterised by massive neutrophil influx and elevated neutrophil elastase (NE) concentrations. NE stimulates release of pro-inflammatory mediators, including IL-8, from bronchial epithelial cells (BECs), thus sustaining inflammation. This study investigated IL-8 secretion from BECs in response to NE and CF sputum sol. The ability of DX-890, potent small protein inhibitor of neutrophil elastase, to prevent NE and CF sol-induced IL-8 release was studied.
Methods: Normal (HBE) and CF (CFBE) bronchial epithelial cell lines (gift from D Greunert, San Francisco, USA) were stimulated with NE (50 nM, 4 h) or CF sputum sol (diluted 1:100, 4 h). In further experiments, cells were pre-incubated with DX-890 (200 nM or 1 μM) for 30 min, and stimulated as above. IL-8 in culture supernatants was assayed by ELISA.
Results: Treatment with NE or CF sol upregulated IL-8 secretion from both cell lines (p<0.005). Compared to control (media alone) CFBE released more IL-8 in response to NE/CF sol than HBE cells (p<0.005). 200 nM DX-890 prevented NE-induced upregulation of IL-8 release in both cell lines (p<0.03). 250 nM DX-890 abolished NE activity in CF sol 1:100; however 1 μM DX-890 did not prevent CF sol-induced IL-8 release (see table).
Conclusions: DX-890 prevented NE-induced upregulation of IL-8 release from HBE and CFBE cells, but not CF sol-induced IL-8 release. Results suggest that NE is not the principle component in CF sputum sol responsible for IL-8 release from BECs.
Acknowledgement: DX-890 was a gift from Dyax Corp, who co-funded this study with the Department of Education and Learning (NI).
COMPARISON OF THE ORAL GLUCOSE TOLERANCE TEST AND SERIAL GLUCOSE MONITORING IN CYSTIC FIBROSIS PATIENTS
K. Mohan, H. Miller, P. Dyce, M. J. Ledson, M. J. Walshaw. The Cardiothoracic Centre-Liverpool, UK
Introduction: The oral glucose tolerance test (OGTT) was developed to identify glucose intolerance in non-CF patients but is now recommended for annual diabetes screening for CF at age >12. However, its value in the diagnosis of CFRD is questioned, and continuous glucose monitoring systems, suggest that it may underestimate CF glycaemia. To investigate, we compared the diagnostic yield of OGTT with serial glucose monitoring (SGM) in adult CF patients.
Methods: We prospectively compared OGTT and SGM in patients who were admitted with a pulmonary exacerbation. OGTT was performed within the first week in a standard fashion (1.75 g glucose per kg bodyweight, (maximum 75 g) ingested within 5 min after an overnight fast). SGM was performed routinely throughout the admission, where blood glucose levels were checked 2 h after each meal and before bedtime.
Results: Twenty patients (mean age 22 (range 19–31), BMI 20.3 (16.1–29.6), FEV1 59% (38–85), FVC 77% (56–103), 11 female) with exocrine pancreatic insufficiency and no history of CFRD were evaluated. 17 received prednisolone 30 mg/day. SGM (mean 10 days per patient (7–18), 572 blood glucose recordings (mean 29 per patient (14–69)), revealed elevated postprandial blood glucose in all patients. There were 105 hyperglycaemic recordings (⩾11.1 mmol/l, mean 5 per patient (0–18)). 15 (75%) had 2 or more values ⩾11.1 mmol/l. Furthermore, all patients demonstrated elevated blood glucose (7.8 to <11.1), (117 episodes (mean 6 per patient (2–13)). However, based on WHO criteria, OGTT revealed impaired glucose tolerance in only 3 patients, and the fasting plasma glucose was normal in all patients. HbA1C was raised in 5 (30%) (mean 5.9%, range 5.2–6.5).
Conclusion: We have shown a high prevalence of hyperglycaemia within the diabetic range using serial glucose monitoring in these CF patients, which was not detected by the OGTT. SGM could be easily incorporated in clinical practice to detect inter-prandial and post-prandial glycaemic peaks which would otherwise be missed with conventional glycaemic tests.
MANAGEMENT OF CYSTIC FIBROSIS RELATED DIABETES IN THE UK
K. Mohan, P. Dyce, H. Miller, M. J. Ledson, M. J. Walshaw. The Cardiothoracic Centre-Liverpool, UK
Introduction: Cystic fibrosis related diabetes (CFRD) has a poor prognosis and clinical decline can predate diagnosis by several years. UK CF Trust Diabetes Working Group recommendations (2004) indicate that the glucose tolerance test (OGTT) be used for screening, OGTT followed by serial glucose monitoring (SGM) for diagnosis, and insulin for treatment. However, the evidence base is not comprehensive: we conducted survey of recognised UK CF centres to assess clinical practice and adherence to these recommendations.
Methods: A structured two-page CFRD management questionnaire (13 open and closed MCQs focussing on screening, diagnosis, treatment and monitoring) was sent to all 45 adult, paediatric and joint units recognised as specialist centres (>50 patients) by the UK CF Trust.
Results: Thirty seven complete responses (82%, catering for 5270 CF patients) were received: 16/19 adult (84%), 17/23 paediatric (74%) and all 4 joint CF centres. Screening: 35 (95%) tested patients annually, 12 (34%) using a single investigation, the remainder two or more—most common methods were: OGTT alone (23.5%); combination of OGTT, glycosylated haemoglobin (HbA1C), fasting plasma glucose (FPG) (11%); then random blood glucose (RBG) and a combination of OGTT, HbA1C and RBG (both 8%). Overall, 80% used OGTT, 49% HbA1C and 41% RBG either alone or in combination with other tests. Diagnosis: 18 (49%) used OGTT alone and 11 (30%) FPG alone. The recommended OGTT and serial glucose monitoring (SGM) was followed by only 11 (30%). Treatment: 36 (97%) preferred insulin, 21 (57%) never used oral agents but the remainder considered them in early CFRD, those with steroid induced diabetes and in patients unable to cope with insulin. Paediatric centres were less likely to use oral agents (4/17 vs 9/16; χ2 = 3.6, p<0.05). Monitoring: 34 (94%) assessed patients jointly with endocrinology teams and 29 (78%) performed an annual review. HbA1C and SGM were the most common tests used to monitor glycaemic control.
Conclusions: This survey indicates wide variation in practice and poor adherence to national recommendations, highlighting the need for further research into the screening and diagnosis of this common CF complication. Increased awareness and education of healthcare professionals in the CF community is also necessary.
AN AUDIT OF PROPHYLACTIC ANTI-PSEUDOMONAL ANTIBIOTIC USE IN AN ADULT CYSTIC FIBROSIS CLINIC
L. Shinn1, C. Ramsay2, M. Pasteur2. 1University of East Anglia; 2Norfolk and Norwich University Hospital, UK
Background: Cystic fibrosis (CF) sufferers have an increased susceptibility to chronic lung infections. Pseudomonas aeruginosa (PA) is the most commonly isolated pathogen in such cases, resulting in elevated rates of mortality and morbidity. It is widely accepted that the long-term use of nebulised anti-pseudomonal antibiotics leads to improved outcomes in chronic PA lung infection in CF patients and more recently, the adjunctive use of oral azithromycin has been shown to enhance these benefits even further. The aim of this study was to assess the use of nebulised anti-pseudomonal antibiotics and oral azithromycin in a population of adults with CF.
Methods: All hospital notes, microbiology reports (written and electronic) and UK CF database proformas were searched in order to divide all adult CF patients at a single CF clinic into groups dependent on their pseudomonas status. “Colonised” was defined as those producing three or more sputum samples positive for PA within a 12-month period; “isolated” defined as those who produced fewer than three positive samples in the same time frame; and “never isolated” defined as those who have never produced a sputum sample containing PA. The “colonised” group were subject to audit and the following target was set: 100% should be using both a long-term nebulised antipseudomonal antibiotic (colistin, tobramycin or gentamicin, either alone or in combination) and regular oral azithromycin.
Results: Forty five patients were attending the adult CF clinic. 71% (n = 32) were colonised with PA, 22% (n = 10) had isolated PA and 7% (n = 3) had never isolated PA. Of those colonised, 84% (n = 27) were using long-term nebulised anti-pseudomonal antibiotics in contrast to the 41% (n = 13) taking azithromycin. Only 31% (n = 10) of CF patients colonised with PA were meeting the audit target of using combined nebulised anti-pseudomonal antibiotic and oral azithromycin. 54% (n = 17) of colonised patients were using nebulised antibiotics only, 9% (n = 3) were solely taking oral azithromycin and 6% (n = 2) were using neither nebulised antibiotics nor oral azithromycin.
Discussion: The use of anti-pseudomonal antibiotics was found to be below the target set for the audit. This was particularly so for oral azithromycin while the use of nebulised anti-pseudomonals was higher but still below target. While some reasons for not using these antibiotics (such as non-adherence or intolerance) were known to the clinical team, review of the medical records often failed to clearly state why these antibiotics were not used in PA colonised patients. To improve patient care, systems should be in place by which those CF patients who are colonised with PA are easily recognised and subsequently receive the most effective treatment for their pulmonary infection. Care should be taken to clearly document decision making in this area.
REGIONAL IMPROVEMENTS IN PAEDIATRIC CYSTIC FIBROSIS OUTCOMES FOR THE YEARS 1992, 1998 AND 2005
R. Iles, R. Brown, D. McShane. Addenbrookes NHS Trust, Cambridge, UK
Methods: We reviewed regional audit data of Paediatric Cystic Fibrosis outcomes for the years 1992,1998 and 2005. Data were collected form Annual reviews.
Results: Cohort numbers were 118 children aged 0-5 years in 1992, 140 in 1998 and 143 in 2005. An increased adult survival was demonstrated, with a doubling of the proportion of patients aged 12-16 years.
There was a decline in height of 0.4 SD/yr in all cohorts, however at 16 years, patients were taller in 2005 (-0.4 SD) than in 1992 (-1.2 SD).
There was an improvement in the relative mean weight of teenage patients with cystic fibrosis, the mean SD in 1992 being -0.71, 1998, 0.52 and in 2005, 0.38 respectively. In 1992, there was a decline in weight SD from age 11 (-0.2 SD) to age 15 (-2.1 SD). This represented an average decline in weight away from the mean of 0.48 SD/year. In 2005 there was no net fall in SD scores at all over the same age range.
There was an improvement in mean FEV1 % predicted from 75.9% predicted in 1992, 84 % in 1998 and 86% in 2005. In the children aged 10-15 years, FEV1 improved from 60.3, to 80 and 82% respectively. Improvement was seen in velocity of change in FEV1 for the whole cohort, and cohorts aged between 5 and 10 years and 10 to 15 years.
In summary, there has been significant improvement in the key outcomes of height weight and lung function over the time period 1992 to 2005.
EFFECTS OF LUNG FUNCTION AND EXERCISE CAPACITY ON QUALITY OF LIFE IN CYSTIC FIBROSIS USING THE UK CYSTIC FIBROSIS QUESTIONNAIRE
D. S. Urquhart, B. Field, M. Bryon, A. Jaffe. Great Ormond Street Hospital, London, UK
Background: The UK Cystic Fibrosis Questionnaire (CFQ-UK) is a quality of life assessment questionnaire. Various quality of life dimensions are assessed including physical functioning, energy/well-being, emotions, social limitations, role, embarrassment, body image and treatment burden.
Aim: To assess the effects of CF lung disease on quality of life, using the CFQ-UK.
Methods: Thirty five children were surveyed using the CFQ-UK. The self-assessment CFQ-14+ was used for those >14 years, while parents completed the CFQ child P (6–13-year-olds) for the remainder. Incentive spirometry (Jaeger), and incremental cycle ergometry with breath-by-breath ventilatory gas analysis (MedGraphics) were performed on the day of completion of the questionnaire. Mann-Whitney U test was used for group comparisons, and Spearman rank test used for exploring correlation between variables (SPSS v13.0).
Results: Data were obtained on 35 children (17 female) with CF. Median (IQR) age of children was 12.7 (10.7–14.9) years. Median and interquartile range (IQR) for the average CFQ score of the study population was 70 (57–85)%. No significant differences in average CFQ score or its individual modalities were seen in those with normal (+/−2 SDs) FEV1 (n = 21) spirometry (average CFQ score 72 (63–86)%) when compared to subjects whose FEV1 was −2 SDs or lower (n = 14) (67 (51–80)%). Weak correlations were noted between FEV1 and average CFQ score (r2 = 0.13), and CFQ-Health (r2 = 0.13) and eating (r2 = 0.12) scores (all p<0.05). Correlation (r2 = 0.4, p<0.001) was noted between average CFQ score and peak oxygen uptake (ml/m2) during exercise (VO2peak) (fig). Similar correlations were noted between VO2peak and CFQ Physical (r2 = 0.4), Emotional (r2 = 0.35) and Health (r2 = 0.46) subsets (all p<0.001).
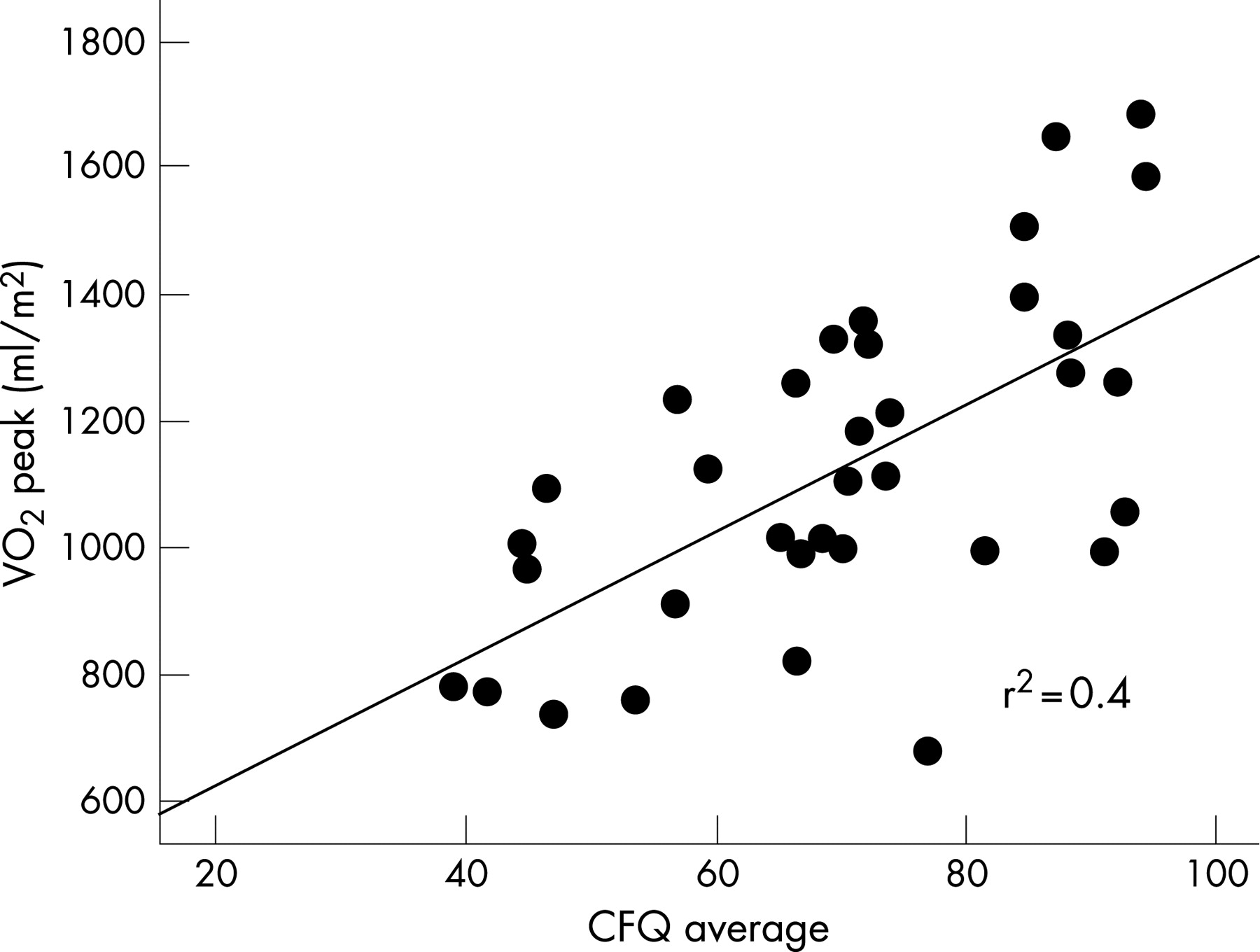
Discussion: Quality of life as assessed by the CFQ appears to be diminished in children with reduced exercise capacity. While this may reflect increased severity of CF lung disease, the relation of the CFQ to spirometric indices appears less clear. Elsewhere, improved health-related quality of life, as measured by CFQ is reported following an exercise training programme.
Conclusion: Children with CF and reduced exercise capacity have reduced quality of life. Exercise prescription may provide a potential therapeutic intervention by which to improve both exercise capacity and quality of life.
SELF-REPORTED FATIGUE AND QUALITY OF LIFE IN ADULT PATIENTS WITH CYSTIC FIBROSIS
N. S. Gale1, C.E.Bolton2, A.Prosser3, C.A.Davies3, S. Enright1, R. I. Ketchell3, D. J. Shale2. 1School of Healthcare Studies, Cardiff University; 2Respiratory Medicine, Cardiff University; 3Adult CF Centre, Llandough Hospital, UK
Background: Fatigue is commonly reported by patients with cystic fibrosis (CF). Determinants of fatigue and its links to quality of life (QOL) are unknown. We assessed fatigue, QOL and disease indicators in clinically stable patients.
Method: We studied 22 adults with confirmed CF (12 male), mean (SD) age 27.3 (7.3) years. The Multi Dimensional Fatigue index (MFI-20) and the CF Quality of Life Questionnaire (CF-QOL) were self-completed. The MFI-20 is validated in cancer and COPD, but its use in CF not explored. It utilises 20 questions (higher scores reflecting more fatigue) to determine five domains (each scored out of 20) including general and physical. Circulating interleukin-6 (IL-6) and tumour necrosis factor (TNF-α) soluble receptors (sr) I and II, albumin, CRP, spirometry, BMI and the Northern chest x ray score were determined.
Results: Mean (SD) FEV1% predicted was 64.2 (23.8)% and BMI 23.3 (3.6) kg/m2. The general fatigue score was 9.7 (3.4) and physical fatigue 9.3 (3.5), and the CF-QOL score 76.3 (17.8)%, (higher scores indicating a better QOL), with no gender differences in either score. Systemic inflammatory status was CRP 7.94 (2.51) μg/ml (n = 20), IL-6 7.94 (1.58) pg/ml, TNF-α srI 1258.93 (1.58) pg/ml and TNF-α srII 1995.26 (1.26) pg/ml, (geometric mean (SD), n = 19). General (r = −0.737) and physical fatigue (r = −0.751) were related to total CF-QOL, both p<0.001. General fatigue was related to albumin (r = −0.46, p<0.05), and physical fatigue to log10CRP (r = 0.47), the Northern score (r = 0.47) and FEV1(l) (r = −0.43), all p<0.05, while the CF-QOL was unrelated. Patients with mild airways obstruction (FEV1>50%, n = 16), had higher CF-QOL scores 80.8 (16.5) (p = 0.05) than those with more severe airways obstruction 64.5 (16.1), (n = 6). Physical fatigue tended to be greater (p = 0.07) in more severe airways obstruction, but not general fatigue. Frequent exacerbators (>3/year, n = 8) had greater general, 11.6 (2.2) vs 8.4 (3.5), physical fatigue 10.9 (4.4) vs 7.9 (2.0) and IL-6 levels, (all p<0.05), but similar CF-QOL to those with <3 exacerbations/year.
Conclusion: Fatigue in adults with stable CF was related to QOL, but only fatigue was related to disease severity and systemic inflammation. The succinct MFI-20 may reflect more the disease process than QOL assessment. Further research is required to fully evaluate its utility.
PROVISION OF CONTRACEPTION AND SEXUAL HEALTH SERVICES FOR WOMEN WITH CYSTIC FIBROSIS
S. J. Gatiss. Cystic Fibrosis Centre and Family Planning Service, Royal Victoria Infirmary, UK
Introduction: Despite thickened cervical mucus most women with cystic fibrosis (CF) are fertile and 75% of those who try to conceive become pregnant. Some have amenorrhoea but pregnancy can occur in advanced CF. Ideally pregnancy should be planned so that health can be optimised, teratogenic drugs avoided and genetic counselling considered. Specialist contraception advice is needed because of problems such as osteoporosis, diabetes, and hepatobiliary disease and interactions between antibiotics and oral contraception. To improve services we undertook a survey of contraception in women with CF.
Results: Of 55 women (mean age 29.7, range 18–51 years) 42 (76%) responded. Two non-responders were pregnant and one had had a hysterectomy. Of the 42 responders, 33 (79%) were sexually active, 13 (31%) had had 19 pregnancies, 18 (43%) hoped for future pregnancy, 15 (36%) wished to avoid pregnancy and 9 (21%) were undecided. Five pregnancies (26%) were unplanned (3 terminated) but none was due to contraception failure. Of the 21 (50%) currently using contraception, 7 used condoms, 7 took the combined pill (COCP), 2 took the progestogen pill (POP), 2 used progestogen injections and 3 partners had undergone vasectomy. None had had sterilisation or used an intrauterine system. Many had previously tried several methods and overall 25 (60%) had used COCP, 22 (52%) condoms, 7 (17%) depot contraception, and 6 (14%) POP. Adverse effects (bleeding, weight gain, headaches, mood swings) were reported by 40%. Sources of advice were their GP (50%), a family planning clinic (FPC) (17%), the CF centre (9.5%), friends (9.5%) and parents (7%) but 9 (21%) considered the advice inadequate and 24 (57%) reported not being told of interactions with antibiotics. The CF team discusses sexual health and advises patients to attend their GP or a FPC for contraception, but many fail to attend FPC appointments.
Conclusions: Women with CF have a high rate of unplanned pregnancy, have not received optimal advice, are not using the full range of modern contraception methods and only a minority have attended a FPC. New strategies are needed to improve contraception services for women with CF.
SWEAT CHLORIDE CONCENTRATIONS AND CFTR GENE MUTATIONS IN LATE DIAGNOSED CYSTIC FIBROSIS
D. T. Bradley1, D. Beattie2, C. A. Graham2, A. C. Magee2, S. A. Mckee2, C. C. Patterson3, J. Rendall1, J. S. Elborn1. 1Adult Cystic Fibrosis Unit, Belfast City Hospital; 2Northern Ireland Regional Genetics Centre, Belfast City Hospital; 3Department of Epidemiology and Public Health, Queen’s University, Belfast, UK
Introduction: Sweat chloride concentration [Cl-] is the gold standard investigation for the diagnosis of cystic fibrosis (CF). Sweat [Cl-] >60 mmol/l is considered diagnostic of CF, <40 mmol/l to be in the normal range and 40–60 mmol/l to be an intermediate range consistent with but not diagnostic of CF, atypical CF and CFTR related disorders. However, there is debate regarding the lower sweat [Cl-] used to define the intermediate range. This study reviewed sweat [Cl-] and genetic tests in children and adults who underwent sweat testing as part of a diagnostic evaluation to determine the prevalence of CFTR mutations and sequence variations at various sweat [Cl-].
Methods and Results: We considered 305 patients who had sweat testing between 1999 and 2006 and were aged 10 years or greater on 1 January 2006. The regional genetic database was searched for these patients. 166 had been tested for CF mutations. The patients were separated into four groups depending on their sweat [Cl-]: less than 30 mmol/l, 30–40 mmol/l, 40–60 mmol/l and >60 mmol/l. We found that 5% of patients with an available genotype and a sweat [Cl-] of <30 mmol/l were compound heterozygotes for CF. 16% of those with an available genotype and a sweat [Cl-] of 30–40 mmol/l were compound heterozygotes for CF (OR 3.85 p = 0.06). 15% of those with an available genotype and a sweat [Cl-] of 40–60 mmol/l were compound heterozygotes for CF (odds ratio 3.57 p = 0.11). 38% of those with an available result and a sweat [Cl-] >60 mmol/l were compound heterozygotes for CF (OR 12.73 p<0.0005). We found that the mean sweat [Cl-] for CF compound heterozygotes in our patient group was 52 mmol/l, the median was 45 mmol/l and the lower limit of the interquartile range was 31 mmol/l.
Conclusions: We therefore suggest that the intermediate range should be extended to 30–60 mmol/l.
ASSESSING ULTRASOUND AS A METHOD TO ENHANCE NON-VIRAL GENE TRANSFER TO THE LUNG
S. Xenariou1, U. Griesenbach1, H. D. Liang2, J. Zhu3, R. Farley1, L. Somerton1, C. Singh1, P. K. Jeffery3, M. Blomley2, E. Alton1. 1Department of Gene Therapy, Imperial College London; UK Cystic Fibrosis Gene Therapy Consortium; 2Ultrasound Group, Imaging Sciences Department, MRC Clinical Sciences Centre, Imperial College London; 3Department of Gene Therapy, Imperial College London
Related to our programme of cystic fibrosis gene therapy, we assessed whether ultrasound (U/S) can increase non-viral lung transfection. U/S is thought to enhance gene transfer by creating transient pores into the cell membrane, which allow more efficient uptake of the vector. U/S penetration in the air-filled lung is limited due to significant energy losses at air/tissue interfaces. We assessed whether the remaining energy that penetrates the tissue is sufficient to increase plasmid DNA (pDNA) gene transfer in vivo, in the mouse lung. Initially, we tested high-frequency (1 MHz) U/S in the presence of Optison microbubbles (an U/S contrast agent), a system which has been successfully used on skeletal muscle, tumours and myocardium. However, Optison alone had deleterious effects on our vector, reducing reporter gene expression by approximately 10-fold (p<0.001 compared to pDNA alone, n = 6–8 mice/condition). Nonetheless, proof-of-principle for U/S-mediated lung gene transfer was established. U/S exposure enhanced pDNA gene transfer approximately 15-fold compared to animals treated with Optison alone (p<0.001, n = 7–8 mice/condition), but this effect was entirely dependent on the presence of the microbubbles. In an attempt to overcome these limitations and further enhance the effect of U/S, we assessed low-frequency (30–35 KHz) U/S. The potential advantages of lowering U/S frequency include: (a) enhancing the formation of pores on cell membranes and (b) enhancing the penetration of U/S energy into the lung. Low frequency U/S was more effective than high frequency for pDNA gene transfer, as it enhanced reporter gene expression by fourfold (p<0.05 compared to the –U/S group, n = 7–8 mice/condition) even in the absence of Optison. In both cases, however, U/S exposure caused lung haemorrhage which increased in a dose-dependent manner. Therefore, further studies in large animal models are essential to address the efficacy and toxicity of this method.
BACTOFECTION INTO AIRWAY EPITHELIAL CELLS IN VITRO AND IN VIVO USING A GENETICALLY MODIFIED ESCHERICHIA COLI
M. D. B. Larsen1, U. Griesenbach1, S. Goussard2, D. M. Geddes1, C. Grillot-Courvalin2, E. W. F. W. Alton1. 1Department of Gene Therapy, Imperial College London; UK Cystic Fibrosis Gene Therapy Consortium; 2Unité des Agents Antibactériens, Institut Pasteur
Introduction: We assessed bactofection into airway epithelial cells in vitro and in vivo using E coli genetically engineered to enter non-phagocytosing cells (invasive strain).
Methods and Results: CFTE and 293T cells were infected with E coli (MOI 50–500) carrying a luciferase (lux) plasmid under control of the CMV promoter/enhancer (pCIKLux). 48 h post-infection (p.i.) both cell lines showed dose-related expression of lux even at the lowest MOI used (CFTE-MOI 50: 119.7 (24.0), uninfected: 1.3 (1.2) RLU/mg protein, n = 5, p<0.001) (293T-MOI 50: 628?040 (56?474), uninfected: 476 (192) RLU/mg protein, n = 5, p<0.001). For in vivo experiments mice were inoculated intranasally with 100 µl of bacteria expressing GFP under the control of a prokaryotic promoter (5×107–5×109 bacteria/mouse, n = 4) to visualise bacterial localisation in the lungs. The majority of bacteria were concentrated around the alveoli 1 hr p.i. However, bacteria were rarely associated with the conducting airway epithelium. To assess bactofection in vivo, the lungs of mice were infected with invasive E coli carrying pCIKLux (5×107–5×109 bacteria/mouse) and culled 48 h p.i. Mice receiving the highest dose died within 2 h. Lux expression was detectable in mice receiving 2.5×109 E coli (E coli: 25.8 (2.7), uninfected: 0.15 (0.06) RLU/mg protein; p<0.01; n = 4–8). However, bacteria-mediated gene expression was significantly lower than cationic lipid GL67-mediated expression (p<0.01). Two terminations sequences were then inserted into the plasmid (pCIKLux-mod) in an attempt to abolish prokaryotic lux expression as the CMV promoter has been shown to generate low level protein synthesis in bacteria. To assess, if the observed lux expression in vivo was due to plasmid transfer from bacteria into eukaryotic cells, mice were infected with invasive and non-invasive E coli carrying pCIKLux-mod or pCIKLux (2.5×109 bacteria/mouse, n = 8–9/group). The introduction of termination sequences significantly reduced prokaryotic expression from the CMV promoter (E coli/pCIKLux: 30.0±14.4, E coli/pCIKLux-mod: 2.11 (0.45) RLU/mg protein; p<0.01; n = 8–9).
Conclusions: In summary, bactofection into airway epithelial cells is currently inefficient and gene expression levels are lower than achieved with the current gold-standard non-viral gene transfer agent GL67.
Cough: assessment and treatment
A FOLLOW-UP STUDY OF PATIENTS WHO HAVE HAD LAPAROSCOPIC FUNDOPLICATION AS A TREATMENT FOR THEIR COUGH
K. Archer, N. Chanarin. Colchester General Hospital, UK
Background: Cough is an extremely common symptom and when chronic, may persist for years. Up to a third of these chronic cases have been shown to be due to gastro-oesophageal reflux disease (GORD). Treatments include prokinetic agents and acid suppression. When medical treatment has failed laparoscopic fundoplication has been suggested. This abstract describes the outcome in 21 patients who had laparoscopic fundoplication for treatment of cough.
Methods: Between 2000 and 2005, 27 patients underwent laproscopic fundoplication. All were extensively investigated preoperatively, with no other pathology demonstrated apart from positive oesophageal manometry and pH studies. Patients were sent a questionnaire, which recorded basic demographics, their opinion of the surgery, the postoperative period, the success of the surgery and whether they would recommend the surgery to others. They were asked to complete two cough questionnaires (Leicester Cough Questionnaire, LCQ); one retrospectively from their recollection of cough severity prior to surgery and a second describing current symptoms. The local ethics committee approved the study.
Results: Twenty one patients responded (female = 13, age 40–78 years), LCQ data were complete in 18. The median duration of cough pre-surgery was 4 years. Median follow-up of 2 years. The perioperative period was described as bearable, 14 had postoperative swallowing problems, mostly resolving within 2 months. 13 patients (62%) were helped by the surgery, 5 of these were cured (24%). No patients reported that they would not recommend fundoplication to others in a similar situation. LCQ improved significantly following surgery (p = 0.0023). The average LCQ result was 58 (range 40–78) preoperatively, and 91 postoperatively (range 42–131), average increase of 33 (24.8%). The change in LCQ correlated with patient’s satisfaction with the surgery.
Conclusion: This retrospective study shows that in correctly selected patients laparoscopic fundoplication can be an effective treatment for chronic cough caused by GORD. Prospective studies are needed. Eight of our patients failed to improve emphasising the need for further investigation to characterise the group who respond best to this intervention.
LARYNGEAL APPEARANCES AND PROXIMAL REFLUX IN CHRONIC COUGH
S. Decalmer1, H. Jones1, M. Yaor2, L. A. Houghton1, A. E. Camilleri2, A. Woodcock1, J. A. Smith1. 1University of Manchester; 2University Hospital South Manchester, UK
Background: Gastro-oesophageal reflux is a common cause of chronic cough. Impedance/pH monitoring allows the proximal extent of reflux events to be measured. Proximal events may induce laryngeal inflammation and hence coughing. Exposure of the larynx to refluxate may be associated with particular examination findings and these can be documented by the Reflux Finding Score (RFS).
Aim: To evaluate the relations between reflux events and laryngeal findings in a group of patients with unexplained chronic cough.
Methods: Thirty five patients with chronic cough (>8 weeks) and 10 healthy controls underwent 24 h impedance/pH monitoring with measurements taken from 3–17 cm above the lower oesophageal sphincter. Bolus movement was defined as a rapid fall in impedance from baseline to a 50% threshold, in at least two consecutive (of the distal four) channels. Proximal reflux was defined as retrograde propagation of impedance drops extending to the most proximal recording channel, in the absence of swallowing. Cough patients had simultaneous 24 h ambulatory cough recording and documentation of laryngeal appearances (RFS) by a single ENT specialist.
Results: Thirty five cough patients, median age 58 years (range 26–79), 63% female and median cough duration 6 years (1.3–30) were recruited along with 10 healthy controls, median age 47.5 years (31–62), 50% female. Cough patients had a mean number of reflux episodes of 64.6 (25.1) and controls a median of 60 (range 40–180), (p = 0.76). Proximal reflux episodes were not significantly different between cough patients and controls (median 8 (0–54) and median 16.5 (1–33), p = 0.19). Twelve cough patients had an abnormal number of reflux events, (>73 episodes), median 88.5 (75–129). They experienced more proximal reflux than those with a negative study (median 12 (0–54) vs median 7(0–15) p = 0.04). Laryngeal appearances (RFS) did not significantly differ with presence or absence of reflux (p = 0.47). The RFS did not significantly correlate with number of reflux events (r = −0.23 p = 0.22), proximal reflux (r = −0.22, p = 0.24) or the objective cough rate (r = 0.10, p = 0.60).
Conclusions: Cough patients and controls had similar numbers of reflux events. Proximal reflux was present in both groups. Laryngeal appearances in cough patients were not related to the number of reflux events (whether proximal or not) or objective cough rates.
HOW TO QUANTIFY COUGHING? CORRELATIONS WITH QUALITY OF LIFE IN PATIENTS WITH CHRONIC COUGH
A. Kelsall, D. Webster, N. Brown, K. Mcguinness, A. Woodcock, J. Smith. University of Manchester, Manchester, UK
Introduction: Different methods have been used for quantifying coughing in sound recordings. The most intuitive method is to count the explosive cough sounds. As yet no method has been shown to be more valid than any other. We aimed to examine the relationships between three different units of cough and assess their ability to predict cough specific quality of life.
Methods: Seventy subjects (73% female, mean age 55 (SD 11.7) years with chronic unexplained cough (median cough duration 4.8 years (IQR 2.5–10.1 years) performed fully ambulatory 24-h sound recordings (IAudio, Cowon Systems Inc, Korea or Vitalojak, Vitalograph Ltd, UK). Sound recordings were manually counted by trained observers and coughing in each quantified as follows: (1) explosive cough sounds—the number of explosive sounds/h; (2) cough epochs—the number of periods/h of continuous coughing without a 2 second break; (3) cough seconds—the number of seconds/h containing at least one explosive cough sound. Subjects also completed cough visual analogue scales (VAS) and Leicester cough questionnaire (LCQ).
Results: The median number of cough sounds per hour was 15.9 (IQR 8.6–23.0), cough seconds 12.2 (IQR 6.8–8.1) and cough epochs 5.1 (IQR 2.9–7.1). All quantification methods were highly correlated, with cough sounds and cough seconds showing the strongest correlation, r = 0.99, p<0.001; cough seconds and cough epochs r = 0.92, p<0.001 and cough sounds and cough epochs r = 0.90, p<0.001. Mean LCQ scores were 12.3 (SD 3.8), median VAS daytime was 40.0 mm (IQR 21.5–62.8 mm) and night time 18.0 mm (IQR 5.3–45.8 mm). LCQ scores had an identical relation with both cough sounds and seconds; cough epochs correlated less well. VAS scores showed a similar pattern; night VAS generally correlated better than day.
Discussion: Cough sounds and cough seconds are very strongly correlated with one another, and moderately correlated with cough related quality of life and visual analogue scales. Cough epochs correlate the least well with the other methods and consistently patient perception of cough.
NOCTURNAL AND POST-PRANDIAL COUGH FREQUENCIES AMONG PATIENTS WITH DIFFERENT CAUSES OF CHRONIC COUGH
A. A. Raj1, T. Fisher2, S. Kabadiya2, S. S. Birring3, I. D. Pavord1. 1Glenfield Hospital; 2University of Leicester Medical School; 3King’s College Hospital, UK
Introduction: Chronic cough is a common symptom, which can be responsible for significant impairment of quality of life. Gastro-oesophageal reflux (GOR) is thought to contribute to some cases of chronic cough. GOR occurs particularly in the post-prandial period; nocturnal reflux is indicative of GOR disease. We set out to determine if the post-prandial period cough frequency or nocturnal frequency differed between patients subsequently diagnosed with chronic cough secondary to GOR compared to those with cough due to other causes or idiopathic chronic cough, based on the hypothesis patients with cough secondary to GOR would have an increased cough frequency in these time frames compared to patients with other categories of cough.
Methods: All patients underwent 24-h ambulatory cough monitoring with the automated Leicester Cough Monitor as part of their clinical work up. Patients were identified as having chronic cough secondary to GOR disease if they responded to empirical treatment with a proton-pump inhibitor and if other significant contributors to chronic cough had been excluded by history, physical examination (including ENT), appropriate imaging, lung function testing, methacholine challenge and induced sputum analysis.
Results: Forty three patients with untreated chronic cough underwent 24-h ambulatory cough monitoring; 5 had GOR disease diagnosed as the cause of their chronic cough. The table shows mean (SEM) cough counts/h calculated for the postprandial period, defined as the 2 h following the end of each meal and night-time, defined as the time from patient going to bed until they arose. There were no significant differences in post-prandial and nocturnal cough frequency in any patient category. There were no significant differences in the visual analogue scores for cough in any patient category.
Conclusions: Our findings do not support an important direct role for post-prandial or nocturnal GOR in generating cough in patients classified as having cough due to GOR disease.
DIAGNOSIS AND SUCCESSFUL MANAGEMENT OF PERSISTENT COUGH IN A DEDICATED COUGH CLINIC: A DISTRICT GENERAL HOSPITAL EXPERIENCE
A. E. Stanton, D. A. Taylor. Wycombe Hospital, UK
Background: Guidelines recommend trials of treatment as the mainstay diagnostic tool for patients with chronic cough and evidence from specialist clinics suggests this approach can achieve improved symptoms in over 80% of patients. Following the set up of a cough clinic in our district general hospital in August 2004 we examined if comparative level of success could be achieved in this setting.
Aims: 1. How successful is our cough clinic in improving patients cough severity? 2. How successful is a trial of treatment in making a diagnosis? 3. Can the cause of cough be accurately predicted from history at first presentation?
Methods: The following data were entered into a database at first clinic attendance: demographics, cough duration, cough severity scale (CSS, a visual analogue scale ranging 0–10), pre-treatment trial diagnosis. Patients received a detailed disease specific trail of treatment based on the initial clinical assessment. An improvement of ⩾3 on the CSS was felt to represent a clinically significant improvement. CSS and post-treatment trial diagnosis was recorded at further clinic visits until discharge. Data from referrals from August 2004–August 2005 were reviewed with missing data retrieved from case note review.
Results: Of 118 patients referred in this one-year period, 113 had available data (77 female, 41 male, aged 13–89, median age 63). Median cough duration was 23 months (range 3–600) with baseline median CSS 6 (range 0–10). The most frequent pre-treatment trial diagnoses were asthma (69), reflux (14) and upper airway cough syndrome (UACS, 11). A final diagnostic decision was made in 106 patients with 9 lost to follow-up. Baseline and final CSS data were available for 96 patients. Median final CSS was 1 (range 0–10, 95% CI for difference from baseline 3 to 5, p<0.0001). 64/96 patients (66.7%) had improved CSS (as defined by improved CSS ⩾3). The most frequent final diagnoses were asthma (51), reflux (15) and UACS (13). Additional diagnoses were bronchiectasis (9), ACE inhibitor induced cough (3), ILD (1), and other causes (5). The final diagnosis was not clear in only 6/106 (5.6%) patients. Overall post-treatment trial diagnosis was in agreement with pre-treatment trial diagnosis in 73/106 (68.9%) with 26/106 (24.5%) having a secondary contributing factor to their cough. Prediction was better for asthma (84.3%), than UACS (69.2%) or reflux (40%).
Conclusions: Overall cough severity was improved in the majority of patients following a successful response to treatment trial. It is not clear however how much of a change in the CSS constitutes a clinically significant improvement and further investigation of such a scale in the management of cough is warranted. In only a small proportion was the diagnosis unclear after trials of treatment. With careful initial assessment the initial diagnosis is a good predictor of final diagnosis.
CLINICAL FEATURES OF IDIOPATHIC CHRONIC COUGH
N. Y. Yousaf1, C. E. Brightling1, I. D. Pavord1, S. S. Birring2. 1Glenfield Hospital; 2King’s College Hospital, UK
Introduction: Idiopathic chronic cough (ICC) is a condition that is challenging to manage and causes considerable physical and psychological morbidity. Little is known about ICC and there is a paucity of effective therapeutic options. We set out to describe the clinical features of 180 well-characterised patients with ICC seen in a specialist cough clinic between 1999–2006. All patients were investigated using a standardised algorithm focusing on the three most common causes of cough: asthma, rhinitis and gastro-oesophageal reflux.
Results: 148 (82%) patients were female and patients had a mean (SEM) age 57 (1) years, age of onset of cough 51 (1) years and duration of cough 5 (1) years. 64 (34%) patients had a history of organ specific autoimmune disease (1 (0.6%) Addison’s disease, 3 (4.7%) coeliac disease, 9 (14%) type 2 diabetes mellitus, 2 (1.1%) type 1 diabetes mellitus, 6 (9.3%) hyperthyroidism, 31 (48%) hypothyroidism, 3 (4.7%) pernicious anaemia, 4 (6.2%) vitiligo, 1 psoriasis, 2 ulcerative colitis, 1 urticaria). 50 (28%) patients had positive autoantibodies and 39 (22%) patients were lymphopenic (lymphocyte count <1.5×109/l). Six patients with ICC had a past history of breast cancer for which they received radiotherapy but did not have evidence of pulmonary fibrosis or tumour recurrence on CT scanning. Patients with ICC (19 subjects (15 females) patients) that underwent cough reflex sensitivity measurement had heightened capsaicin cough reflex sensitivity; C2 and C5: 2.2 and 6.9 μmol/l respectively (mean C2 and C5 for age- and sex-matched normals: 47.9 and 416, respectively).
Conclusions: This study is the largest reported series of patients with ICC. Patients with ICC are predominantly females and our data suggest an onset of cough around the time of the menopause. We have confirmed previous reports of an increased prevalence of organ-specific autoimmune disease in patients with ICC. We have suggested the homing of inflammatory cells from the primary site of autoimmune inflammation in embryologically-related organs to the airways as a possible mechanism for the development of ICC. The lymphopenia in patients with ICC may be a due to sequestration of lymphocytes to the airways. Further studies are required to investigate pathogenetic mechanisms leading to the development of ICC that may identify novel therapeutic targets.
INTER- AND INTRA-OBSERVER VARIABILITY OF MANUAL COUGH COUNTING IN COUGH CHALLENGE TESTING
L. Polley1, C. Cardwell2, C. Butler1, N. Magee1, J. Macmahon1, R. Costello3, L. Mcgarvey2. 1Belfast City Hospital; 2Queen’s Univerity Belfast; 3Beaumont Hospital, UK
Background: Cough challenge testing with citric acid or capsaicin can provide semi-objective information on cough symptom severity and following therapeutic intervention can help to determine treatment efficacy. It has been shown that these are repeatable in individuals. However, the degree of inter-observer and intra-observer variability in cough counting during these challenges is not known.
Methods: In order to explore variability in cough counting, citric acid challenges were recorded on MP3 file format. Sound files (n = 40) containing the C2 (2 or more coughs) and C5 (5 or more coughs) thresholds obtained were selected and replayed on two separate occasions, two weeks apart to three observers (respiratory trainees, one of whom was the investigator and had prior experience in cough counting). All were shown an accepted clinical definition of cough. To standardise counting each participant was instructed to count the number of coughs for exactly 10 seconds after inhalations. Each participant activated their own stopwatch. There was no visual advantage to the investigator as counting occurred subsequent to the actual cough challenge. Participants were attributed the letters L (investigator), N and C. Intra-observer (eg, L1-L2) and inter-observer (eg, L1-N1) Kappa values were then calculated to give a measure of repeatability.
Results: There was a suggestion of increasing disagreement as the number of coughs rose. However, the numbers of observations were too small to confirm this (fig).
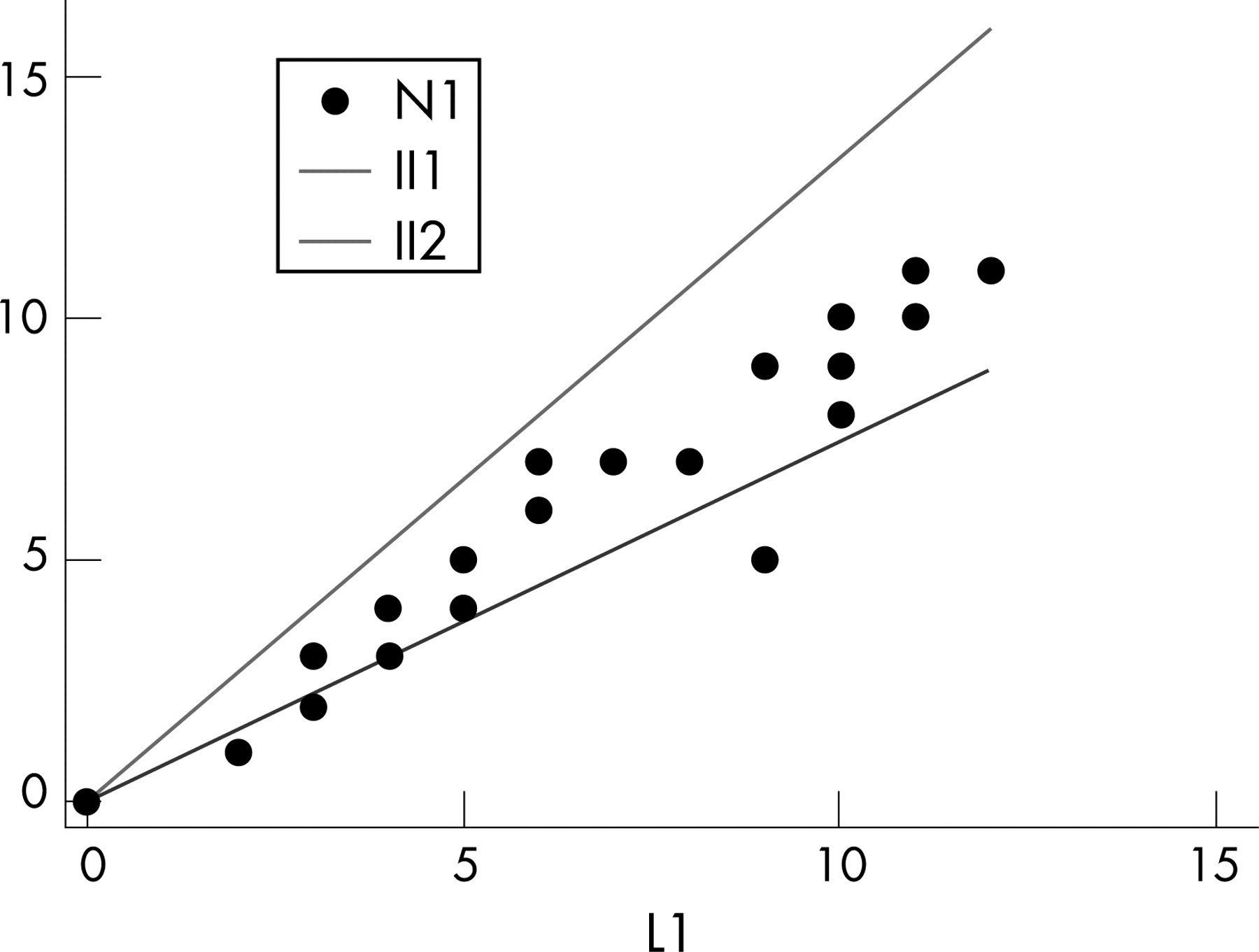
Conclusion: Cough counting of C2 and C5 values appears to have excellent intra and inter-observer repeatability, even without prior experience (that is, observers N and C). However, this repeatability may decrease at higher cough counts.
ANXIETY, DEPRESSION AND QUALITY OF LIFE MEASURES IN PATIENTS WITH CHRONIC PERSISTENT COUGH
S. Decalmer1, A. Kelsall1, K. Mcguinness2, A. Woodcock1, J.A.Smith1. 1University of Manchester; 2University Hospital South Manchester, UK
Background: Validated questionnaires have been developed to examine the impact of cough on quality of life and these are often used to measure cough and its response to treatment. High levels of depression and anxiety have been identified among patients with chronic cough but the impact of these factors on quality of life reporting has not been examined.
Methods: Patients with cough >8 weeks duration completed a cough related quality of life measure (Leicester Cough Questionnaire (LCQ)), the Hospital Anxiety and Depression Score (HADS) and 24-h ambulatory acoustic cough monitoring (Vitalojak, Vitalograph Ltd, UK). Cough recordings were manually analysed and the number of explosive cough sounds reported.
Results: Ninety nine patients were studied, mean age 55.7 (11.0) years, 66% were female and the median cough duration was 3.75 years (range 0.5–30). The median HADS anxiety score was 6 (range 0–21) and HADS depression 4 (range 0–17). HADS suggested a possible diagnosis of anxiety or depression in 33.7% and 13.3% respectively. The mean LCQ score was 12.0 (3.4). The median cough rate was 14.4 (range 2–233) cough sounds/h (median day rate 19.3 (range 2.4–244), night rate 3.5 (range 0–46.8)). Level of anxiety was not related to the amount of coughing (r = 0.06, p = 0.5), level of depression was trend significant (r = 0.19, p = 0.06). Anxiety and depression scores did correlate with cough related quality of life (r = −0.49, p = 0.001; r = −0.47, p = 0.001). Multiple linear regression showed that 42% of the variance in LCQ scores could be explained by a combination of anxiety (p<0.001) and cough rate (p<0.001), adjusted for age and gender.
Conclusion: Anxiety is more common than depression in patients with chronic cough but both are poorly related to the amount of coughing. Anxiety and depression scores have a significant impact on cough related quality of life. Therefore when using quality of life measures to assess symptoms and treatment response it must be appreciated that mood is influential.
THE EFFECT OF AMILORIDE ON CITRIC ACID INDUCED COUGH
L. Polley1, C. Cardwell2, J. Macmahon1, R. Costello3, L. Mcgarvey2. 1Belfast City Hospital; 2Queen’s University Belfast; 3Beaumont Hospital, UK
Background: Acid sensing ion channels (ASICs) are thought to have a mechanistic role in the generation of acid and mechanically induced cough. One study in asthmatic children has suggested that inhaled amiloride, an ASICs blocker, attenuates cough induced by acetic acid aerosol. The effect of amiloride on acid induced cough in adults is unknown.
Hypothesis: We hypothesised that ASICs are involved in citric acid induced cough, and that their activation may be attenuated by inhaled amiloride.
Methods: Three groups were investigated; 11 unexplained (idiopathic) cough (10 female, mean age 58.2 years), 11 cough variant asthmatics (5 female, mean age 51.8 years) and 18 healthy volunteers (14 female, mean age 35.2 years). Using a double-blind, randomised crossover design, all subjects underwent citric acid cough reflex sensitivity testing on two separate hospital visits one week apart. C2 and C5 cough thresholds were obtained as previously described. At visit 1, a baseline citric acid cough challenge was followed by pre-treatment inhalation of either nebulised amiloride (1.5 mmol/l, 5 ml) or phosphate buffered saline (PBS) placebo. This was followed within 5 min by a second cough challenge. One week later subjects repeated the same protocol with inhalation of the crossover agent. A one-way ANOVA was used to examine for differences between groups and a Hills-Armitage crossover analysis was used in order to explore any treatment or period effects. The study was powered to detect as statistically significant (at the 5% level) a 50% increase in C5 cough threshold.
Results: Idiopathic coughers had the lowest cough thresholds. However, only healthy and Idiopathic C5 thresholds differed significantly at baseline, p = 0.01 (see table). Amiloride did not significantly alter cough thresholds of any individual group.
Conclusion: This dose of amiloride does not alter citric acid cough threshold which may suggest that ASICs do not have a prominent role in mediating citric acid induced cough in adults.
THE EFFECTS OF VOLUNTARY COUGHING ON THE AIRWAYS IN MILD ASTHMA
P. A. Marsden1, A. A. Kelsall1, U. Alam2, A. A. Woodcock1, J. A. Smith1. 1University of Manchester; 2University Hospital of South Manchester, UK
Background: We have previously shown that in healthy subjects voluntary coughing caused small airway bronchodilation, a transient fall in eNO and a delayed fall in EBC pH (at 24 h). We hypothesised that cough in asthma may not just be a symptom, but also an important promoter of airway inflammation.
Methods: Eighteen physician diagnosed asthmatic subjects (n = 9 steroid naive; n = 9 <500 mcg beclomethasone dipropionate) underwent (in order of occurrence): exhaled nitric oxide (eNO), exhaled breath condensate pH (EBC) and lung function (sRaw, FEV1; FEF50; PEFR) measurements at day 0. One week later, following repeat baseline measurements, subjects were randomised to either: maximal voluntary coughing (2 periods of 10 seconds 1 min apart increasing by 2 periods each hour for 4 h) or control. At 4 h, 8 h and 24 h (after start of intervention) subjects performed eNO, EBC, sRaw and spirometry. PEFR was also repeated at 12 h. On day 15 subjects crossed over and an identical set of measures was performed. We assessed the effect of voluntary coughing compared to control for each endpoint using general estimating equations (where missing data were present) and AUC comparisons (where complete data sets were available) (STATA 9.0, Stata Corp, USA).
Results: Eight male, 10 female subjects, median age of 33 years (range 18–71) were studied. Mean duration of asthma was 18.4 years (8.2), lung function showed FEV1 (% predicted) 102.8 (13.0), FEF50 (% predicted) 77.7 (21.3), PEFR 498.8 l/min (113.4) and sRaw 0.82 Kpa−1s−1 (0.6–3.1). Median eNO was 21.4 ppb (6.4–79.6) and EBC pH 7.46 (6.79–7.74). For the voluntary cough day compared to the control day there were no significant changes (FEV1 p = 0.47, eNO p = 0.12, FEF50 p = 0.59, sRaw p = 0.46, EBC pH p = 0.73). There was a trend towards a significant change in PEFR p = 0.06; the largest difference occurred at 12 h (mean 438 l/min vs 473 l/min).
Conclusions: Voluntary coughing in mild asthma had no significant effects on measures of lung function or airway inflammation.
Sleep disordered breathing
PREVALENCE OF OBSTRUCTIVE SLEEP APNOEA IN A POPULATION OF MORBIDLY OBESE PATIENTS REFERRED FOR BARIATRIC SURGERY AND POSTOPERATIVE OUTCOMES
M. J. Irvin-Sellers, J. Pateraki, J. S. White, G. Miller. York District Hospital, UK
Background: Morbid obesity is a growing problem in Western Europe and the USA and carries health risks, including OSA. Buchwald’s meta-analysis of bariatric surgery found the percentage of patients in the population whose OSA resolved post surgery was 85.7%. There is little recent medical literature about resolution of OSA in patients undergoing bariatric surgery. We aim to determine the prevalence of OSA in a population of morbidly obese patients referred for bariatric surgery and investigate the possibility of resolution post-surgery.
Methods: This is a retrospective review of 100 patients referred for oximetry pre-bariatric surgery at York District Hospital. The review includes those who had repeat overnight oximetry post surgery to investigate resolution of OSA.
Results: 100 patients studied so far. 96 preoperative oximetries, 51 were abnormal. 16 referred for CPAP titration studies. Six were unable to tolerate the titration, 10 commenced on CPAP. All patients underwent Roux-en-Y as the surgical procedure. Patients on preoperative CPAP spent an average of 24 h on HDU post operatively. No respiratory complications. Of the 10 patients on CPAP 7 had oximetries repeated 12 months post-surgery. Six had resolved and 1 oximetry showed no resolution but did show improvement in oxygen desaturation. Two died (not respiratory related) and one failed to attend for repeat oximetry. Only four repeat oximetries were done on patients with previously abnormal tests not requiring intervention with CPAP, of these three had resolved and one was not reported.
Conclusions: This study illustrates there is a high prevalence of OSA in this obese population. The number of patients commenced on CPAP is small but repeat oximetries showed weight loss is associated with resolution of OSA. This is supported by the few patients not on CPAP who had repeat oximetry confirming resolution. Although this review is small so far, it does indicate that OSA resolves with weight loss post bariatric surgery.
AN EVALUATION OF THE “DYNAMAX” MANDIBULAR APPLIANCE IN OBSTRUCTIVE SLEEP APNOEA IN A DISTRICT GENERAL HOSPITAL
E. Thickett, S. Hirani, J. Hodgkins, A. J. Williams. Royal Bournemouth Hospital, UK
Introduction: Obstructive sleep apnoea (OSAS) affects 4–6% of the middle-aged UK population and is responsible for significant partnership disharmony. Nasal CPAP therapy is effective but; invariably has poor compliance in less severe cases, is bulky with poor portability and is frequently deemed socially unacceptable. The “Dynamax” mandibular appliance (DMA) is a current treatment for Skeletal 11 malocclusion characterised by mandibular retrusion. It has the advantage of both maxillary expansion and mandibular advancement and is developed and tailored on an individual basis by orthodontic sculpture. These facilities are available widely in hospital-based orthodontic departments. For these reasons we have explored its use in the treatment of mild to moderate cases of OSAS.
Study and Methods: Thirty five symptomatic patients (29 males) with mild to moderate OSAS, determined from sleep study analysis, had dental impressions taken and the “Dynamax” appliance constructed. Following fitting and instructions for use, all patients were entered into the study. After two months, repeat overnight oximetry was undertaken and both an Epworth sleep score (ESS) and quality of life questionnaire completed.
Results: The mean age was 51 (range 29–71) years. The mean ESS pre-treatment was 12/24 (range 7–19) with a significant fall post treatment by 7 (range 3–14) (p<0.0001). Pre-treatment oximetry data confirmed typical tracings and patterns of OSAS with a mean low oxygen saturation (SaO2) of 83% (range 71–90%). Post-treatment oximetry was available in 16 patients and showed significant improvement in the number of hourly SaO2 de-saturation dips and a mean increase of 4.7% in the lowest SaO2 recorded (p<0.0001). 30 (86%) of patients found the appliance of “great to moderate” benefit and 21 (60%) were able to tolerate and be fully compliant within days. Of 10 patients who had previously experienced CPAP, 80% of them felt it was easier to tolerate the DMA. 67% of these patients stated the appliance was more portable and acceptable to their bed partner. 70% of bed partners reported softer and less frequent snoring. 90% of the patients in this study wished to wear the DMA long-term.
Conclusions: The DMA provides a satisfactory alternative therapy in the treatment of OSAS of mild to moderate severity. This oral device is conveniently small and readily portable and well tolerated by patients and bed partners alike. It can be fashioned in orthodontic departments available in all district general hospitals and will enhance the provision and development of any local sleep service.
OVERTONE SINGING: A TREATMENT FOR SNORING AND OBSTRUCTIVE SLEEP APNOEA?
V. L. Cooper, M. W. Elliott, J. Malik. Leeds Teaching Hospitals NHS Trust, UK
Introduction: Treatment of snoring is difficult and where CPAP is not tolerated for sleep apnoea there are few effective alternatives. A recent study has shown the effectiveness of Didgeridoo playing. This study examined whether a series of vocal exercises is effective in the treatment of snoring and sleep apnoea.
Methods: Sixteen patients (14 male) were recruited. They underwent a full respiratory sleep study (Embletta) and completed the General Health Questionnaire (GHQ), Measure Yourself Medical Outcome Profile (MYMOP2), The Epworth Sleepiness Scale (ESS) and the Leeds Snoring Questionnaire (LSQ) which includes a section for partners to complete. Patients then underwent six lessons with a professional overtone singing tutor and were encouraged to practice for 15 min each day at home. The sleep study and questionnaires were then repeated.
Results: Baseline apnoea hypopnoea index (AHI) ranged from 1.9 to 64.1 (mean 21.4 (6.3)) events per hour. Nine patients completed the study, while seven either did not complete the singing lessons or failed to return for follow-up. After treatment there were no changes in any of the sleep study variables. The GHQ showed patients felt they were better able to concentrate and they were feeling happier overall. The MYMOP suggested patients felt their symptoms were less severe and their overall wellbeing was improved. The ESS decreased significantly from 13.7 (1.5) to 9.7 (1.4). Patients also felt that they snored less often, that the snoring annoyed their partner less, that they were less tired and less likely to fall asleep during the day (LSQ). Partners did not, however note any significant change.
Conclusions: These results suggest that although patients subjectively feel better there are no objective benefits and partners do not feel there is any improvement in snoring or sleep quality. The search for an effective treatment continues.
COMPARING PRIMARY AND SECONDARY CARE REFERRALS TO A SLEEP APNOEA CLINIC
B. Sekar1, L. Davies1, I. Bartle1, K. E. Lewis2. 1Carmarthenshire NHS Trust; 2School of Medicine, UK
Background: Sleep service provision across the UK is variable with many centres experiencing long delays to diagnosis and also to treatment. One way to improve service efficiency is to receive high quality referrals, correctly identifying only appropriate symptoms that require further investigation. We compared baseline characteristics and final diagnoses of those referred from primary care to those referred from secondary care to a once-weekly, sleep-disturbed-breathing (SDB) clinic, within a district general hospital, that covers three NHS Trusts serving a wide geographical area in South and West Wales (UK).
Methods: 779 patients were seen in our sleep clinic over four years (between 7 February 2003 and 27 April 2007). 589 patients were referred from primary care and 188 from secondary care (174 from ENT). We randomly selected 350 cases for analysis but could not obtain notes on 42 patients. We retrospectively compared patient symptoms (mainly if they were sleepy), physical characteristics, whether they were deemed appropriate to proceed to sleep study or not, and actual (limited channel, Visilab or Embletta) sleep study results. We divided patients according to referral source. We used χ2 and non-paired t tests (as it was directly observed data and n>100).
Results: After being assessed in clinic, 586 from 589 (99%) patients referred from primary care were sent for limited channel sleep studies. 185 from 188 (98%) patients referred from secondary care were sent for limited channel sleep studies (p>0.90). The table compares the 308 patients with full sleep study results available.
Conclusions: Virtually all patients were sent for sleep studies from a SDB clinic irrespective of referral source. This does not reflect inappropriate screening at SDB clinic (for example, often staffed by SHOs) because a higher than expected proportion of referrals (with sleep study data available) did have the sleep apnoea hypopnoea syndrome (more than 80%). Referrals seem appropriate from primary and secondary care and the numbers represent the large burden of disease rather than poor screening by local doctors. In the random sample of patients with full sleep data available, there were no statistically significant differences in baseline demographics, self-reported tendency to fall asleep (Epworth) or severity of sleep disturbed breathing, according to referral source. Those from primary care had higher mean diastolic blood pressure and a tendency to higher mean systolic blood pressure but this is probably due to those who are referred from secondary care having more opportunity for screening; the difference in blood pressure cannot be explained by differences in severity of RDI or BMI. It is unlikely that education aimed at either primary or secondary care (or both) will improve our clinic’s efficiency; it may help doctors prioritise but is likely to increase waiting lists.
COMPLIANCE WITH CONTINUOUS POSITIVE AIRWAY PRESSURE THERAPY IN TYPE 2 LICENCE HOLDERS WITH MODERATE TO SEVERE SLEEP APNOEA
S. C. Madathil, D. Banerjee, L. Irish. Birmingham Heartlands Hospital, UK
Introduction: It is known that continuous positive airway pressure (CPAP) therapy reduces accidents and improves alertness in drivers with obstructive sleep apnoea hypopnoea syndrome.
Aims: 1. To look at CPAP compliance data in Type 2 driving license holders with moderate to severe sleep apnoea who were prescribed CPAP therapy. 2. To check how many of these drivers had informed the Driver and Vehicle Licensing Agency (DVLA) as advised to them when the diagnosis of sleep apnoea was confirmed.
Methods: Of all patients seen at the Sleep clinic of Birmingham Heartlands Hospital between August 2005 and June 2007, Type 2 license holders with an oxygen desaturation index (ODI) or apnoea hypopnoea index (AHI) of 15 or more on diagnosis, who had completed at least 12 months since the start of CPAP therapy were analysed. Usage data were downloaded using the software provided by the different CPAP machine manufacturers. DVLA reporting data was collected form the correspondence of DVLA to the sleep consultant.
Results: There were 48 Type 2 license holders, of which 40 were heavy goods vehicle (HGV) and 8 passenger carrying vehicle (PCV). All were male. There was wide variation in the hours of CPAP use with a range of 1.5 h/month to 308.85 h/month (corresponding to 0.05 h/night to 10.3 h/night). The median usage was 140.96 h/month (Corresponding to 4.69 h/night) with an SD of 86.27. 68.75% (n = 33) informed the DVLA, 31.25% did not (n = 15). There was no correlation between the hours of usage and informing the DVLA. The correlation between hours of usage and BMI, Epworth Sleepiness score (ESS), and ODI/AHI will be presented and discussed.
SHOULD WE SELECT PATIENTS FOR CONTINUOUS POSITIVE AIRWAY PRESSURE TRIALS BY OVERNIGHT OXIMETRY OR EPWORTH SCORE?
D. Neagu, N. Bell, R. Gibson, A. Harper, A. Kendrick, J. Catterall, A. T. Whittle. Respiratory Department, Bristol Royal Infirmary
Introduction: Patients under consideration for continuous positive airway pressure (CPAP) treatment for obstructive sleep apnoea (OSA) in our service have a one-month CPAP trial before deciding on long-term treatment. The decision to offer a trial is based on the patient’s symptoms and willingness to try CPAP, the Epworth score (ESS) and the findings on two nights’ overnight oximetry. Patients with “normal” oximetry or ESS may be offered a trial if their symptoms suggest significant OSA and they are keen to try CPAP. We reviewed 224 consecutive trials to see whether CPAP compliance and the symptomatic response to CPAP can be predicted from the pre-trial oximetry or ESS.
Method: We grouped the patients by pre-trial oximetry results (frequency of 4% dips below baseline, highest of two nights’ recording), and by pre-trial ESS. Outcome measures were CPAP usage during the one-month trial (mean hours/night) and the patients’ opinion of the benefit of CPAP (yes or unsure/no). Where data were available (n = 152) we calculated effect sizes (Cohen’s method) for the change between pre- and post-trial ESS (except when patients were categorised by ESS), Multiple Fatigue Inventory General Fatigue score (fatigue), and SF-36 Vitality index (vitality). Effect size <0.2 is insignificant, 0.2–0.5 is small, 0.5–0.8 is moderate and >0.8 is large.
Results: See tables 1 and 2. Twelve patients underwent a CPAP trial despite having 4% dip rate <10/h and ESS <10. Median usage in this group was 4.24 h/night (range 2.1–6.8); 6/12 patients (50%) felt the treatment was beneficial.
Discussion: Patients with all levels of oximetry dip rate or ESS showed similar (and satisfactory) average usage of CPAP during a one-month trial. In all groups, the majority of patients found the treatment beneficial, and the effect sizes for improvements in psychometric tests were moderate or large. Oximetry dip rate and ESS were not sufficient (separately or combined) to distinguish between patients who complied with and benefited from a trial of CPAP and those who did not. This was not an unselected population. Patients were offered CPAP trials following consultation with an experienced clinician, including an assessment of symptom severity and impact, and discussion of management options. A previous audit showed that, of the patients with 4% dip rate <5/h seen in our clinic, 27% were offered a CPAP trial, compared to 100% of those with dip rate >30/h. Our data do not support a policy of a trial of CPAP for every patient referred to a sleep clinic, but they do suggest that clinical consultation can identify significant numbers of patients who may benefit from CPAP, who would not be identified by oximetry or ESS alone.
CAN PATIENTS SELF-ADMINISTER THE EPWORTH SLEEPINESS SCALE?
R. Ghiassi1, A. Cummin2, L. Slingsby2, H. Wolfenden2, L. Bailey2, S. Ma De Los Santos2, K. Murphy2, M. R. Partridge1. 1Imperial College London, NHLI division, Charing Cross Hospital; 2Charing Cross Hospital, West London Sleep Centre, UK
Background: A cardinal feature of obstructive sleep apnoea syndrome (OSAS) is sleepiness which is often quantified by means of the Epworth Sleepiness Scale (ESS). This has been translated into several languages but numeracy and literacy skills amongst patients cannot be assumed and are often overestimated. We have studied the proportion of our patients who can self complete and the proportion who need assistance to complete the ESS.
Methods: 150 consecutive patients attending the West London Sleep Centre with suspected or proven OSAS were asked to complete an ESS and were observed doing so. A check list was utilised to record accuracy of responses and need for assistance.
Results: 10/30 (33.3%) of ESS naive new referrals made errors or were unable to complete the form without assistance from staff. The commonest error made was to give an answer between scores, for example, “1–2” or “2.5”, this was followed by errors (equally weighted) marking the answer with a “tick” or a “cross”, leaving questions blank or not understanding the different chances of dozing. A small number annotated answers, volunteered that they could not read or write or had language difficulties using the ESS and asked a family member or friend to fill in the form for them. Comparable data in follow-up patients who had previously completed an ESS show that 22/120 (18.3%) made errors or were unable to complete it. The types of errors which occurred in this group were similar to the new patients although fewer people asked a friend or family member to help them.
Conclusion: The ESS may not be suitable for all patients and in a group of patients attending a Sleep Centre in West London one third of ESS naive, and 18.6% of ESS non-naive patients needed help to accurately complete the form. We conclude that either assistance with completion of the ESS or alternative methods such as pictorial representations of sleepiness might improve the accuracy of recording self assessments of sleepiness.
BASELINE BLOOD PRESSURE AND HYPERSOMNOLENCE PREDICT BP FALL WITH CPAP TREATMENT OF OSA
G. V. Robinson, B. A. Langford, D. M. Smith, J. R. Stradling1. Oxford Centre for Respiratory Medicine; 1Oxford Radcliffe Hospitals NHS Trust, UK
Introduction: Obstructive sleep apnoea (OSA) is associated with high cardiovascular morbidity and mortality. Randomised controlled trials have shown that continuous positive airway pressure (CPAP) treatment of symptomatic OSA reduces 24-h blood pressure (BP), with the greatest BP falls in those patients with the most severe disease, as measured by symptoms and sleep study. No other predictors of BP fall have been identified, however recent data suggest that prior hypersomnolence is important for the BP lowering effect of CPAP. We have studied predictors of BP change with continuous positive airways pressure (CPAP) treatment of symptomatic OSA. Predictors of BP fall might influence clinicians when making decisions to treat hypertensive OSA patients, and might provide insight into the aetiology of the hypertension of OSA.
Methods: A prospective study of 86 patients with sleep study proven OSA and sufficient daytime symptoms to warrant treatment with CPAP was carried out. A particular >4% SaO2 dip rate and Epworth Sleepiness Score (ESS) were not trial entry criteria, thus providing a spread of disease severity. Mean 24-h BP, subjective sleepiness and fasting blood samples were measured at baseline and after 6 months CPAP treatment.
Results: Subjects had moderately severe OSA at baseline, with a median >4% SaO2 dip rate of 32.7 (IQR 18.3 to 49.8), and median ESS of 16.0 (IQR 12.0 to 18.0). The fall in mean 24-h BP at 6 months was 4.92 (SD 9.87) mmHg, with a mean fall in ESS of 9.7 (SD 5.3). This fall with treatment in mean 24-h BP correlated with baseline ESS (r = −0.24, p = 0.04), the fall in ESS (r = 0.39, p<0.001), obesity indices (eg, BMI, r = −0.38, p<0.001), and baseline mean 24-h BP (r = −0.60, p<0.0001). These variables were the only ones independently correlated on multiple linear regression. Using a post-hoc analysis of patients above and below the median value for baseline BP (100 mmHg) showed that subjects with a baseline ⩾100 mmHg had a 6 month BP fall of 9.2 (SD 9.5) mmHg, compared to a fall of 0.7 (SD 8.3) mmHg in those with a baseline BP <100 mmHg, mean difference 8.54 mmHg (95% CI 4.4 to 12.7), p<0.0001. There was also a correlation with the fall in pulse rate with treatment (r = 0.44, p<0.0001). There were no other independent predictors of blood pressure fall, such as baseline OSA severity, overnight hypoxia, caffeine intake, being on anti-hypertensive drugs or measures of insulin sensitivity.
Conclusion: Daytime hypersomnolence (and its improvement following OSA treatment), baseline mean 24-h BP and measures of obesity are the best predictors of the fall in mean 24-h BP following CPAP therapy. Sleep study measures of OSA severity did not predict blood pressure fall in this study. This suggests that sleep fragmentation may be more important than hypoxia in the pathogenesis of the hypertension of OSA. The presence or absence of hypersomnolence and the pre-treatment BP may influence decision making as to which patients with OSA are most likely to experience a fall in BP with CPAP.
ENDOTHELIAL PROGENITOR CELL NUMBER: A NOVEL CONCEPT IN PATHOGENESIS OF INCREASED CARDIOVASCULAR RISKS IN OBSTRUCTIVE SLEEP APNOEA SYNDROME
M. Uzbeck1, A. Liew3, J. Mcdermott3, D. Gallagher2, I. Saleem2, G. Avalos4, J. J. Gilmartin1, T. O’Brien2. 1Merlin Park university Hospital; 2University College Hospital; 3Regenerative Medicine Institute; 4National University of Ireland
Introduction: Patients with obstructive sleep apnoea syndrome (OSAS) are at increased risk of cardiovascular diseases. Endothelial progenitor cell (EPC) has been implicated in postnatal vasculogenesis and used as a surrogate marker of endothelial function. However, the effect of continuous positive airway pressure (CPAP) therapy in patients with OSAS on EPC number is currently unknown. We hypothesised that CPAP treatment may be associated with increase EPC number, therefore, improving their endothelial function and reducing their cardiovascular risk.
Aim: We investigated whether CPAP therapy in patients with OSAS could increase EPC number.
Methods: Patients with newly diagnosed OSAS (n = 9) were treated with CPAP therapy for one month. The number of EPCs in peripheral blood samples was assessed before and after CPAP therapy.
Results: CPAP therapy was associated with an increase in EPC number (mean (SEM); 127.0 (21.0) vs 65.6 (4.0); p = 0.047, n = 9). The increase in EPC number was more marked with exclusion of ex-smokers (137.4 (24.1) vs 60.6 (1.6); p = 0.026, n = 5).
Conclusion: Our study demonstrated that CPAP therapy in patients with OSAS is associated with an increase in EPCs number, elucidating a novel mechanism of improved endothelial function and reduced cardiovascular risk in these patients.
CHANGES IN CEREBRAL BLOOD FLOW DURING OF AROUSAL FROM SLEEP IN HEALTHY HUMANS
N. Bailey1, F. Kotajima2, D. M. O’Driscoll1, D. R. Corfield3, M. J. Morrell1, M. J. Morrell4. 1Imperial College; 2Jikei University School of Medicine; 3Keele University; 4Royal Brompton Hospital, UK
Aim: Obstructive apnoeas are associated with complex changes in cerebral blood flow (CBF) that may be induced by the changes in blood gases, and arousal from sleep at the termination of the apneoa (Balfors and Franklin. Am J Resp Crit Care Med 1994). In healthy individuals, induced arousals increase mean arterial blood pressure (MABP) and decrease cardiac R-R interval (RR). The aim of this study was to test the hypothesis that arousals induced during sleep would induce changes in CBF, and that the magnitude of the change in CBF would be related to the intensity of the arousal.
Method: Middle cerebral artery velocity (MCAV) was measured using transcranial Doppler ultrasound, as an index of CBF in 11 healthy subjects (mean (SD) age 27 (5.6) years). Sleep was monitored overnight. Arousals were induced using an auditory tone following >2 min of stable stage 2 sleep. The intensity of the arousals was scored from standard electroencephalograms (EEG) by a researcher blinded to the physiological data. Arousals were graded as: Category 1 an abrupt shift EEG frequency >3 s and <10 s; Category 2 an abrupt shift in EEG frequency >10 s. MCAV, cardiovascular and respiratory variables were analysed for 20 s or 5 breaths, pre- and post-arousal.
Results: Category 2 arousals were obtained in 9 subjects; (median (range) 3 (1–5) arousals/subject. Category 1 in 8 subjects; 4 (1–6) arousals/subject. Following Category 2 arousals the peak increase in tidal volume was 25.5% (ANOVA, p<0.01), the partial pressure of endtidal CO2 decreased by 2.9% (p<0.01) MABP increased by 25.6% (p<0.01) and RR interval decreased by 20.2% (p<0.01). MCAV increased initially by 7.8% (p<0.01) but then decreased significantly below baseline levels (fig). Category 1 arousals produced statistically significant post arousal responses for MCVA, cardiovascular and respiratory variables, which were no different from the Category 2 arousals.

Conclusion: Arousal from sleep produces an immediate increase in MCAV, associated with a corresponding cardiovascular activation. We speculate that the increase cerebral vascular tone is a neurally-mediated response that is triggered once a threshold is reached, independent of the magnitude of the arousal.
PREDICTING CONTINUOUS POSITIVE AIRWAY PRESSURE STARTING PRESSURES IN PATIENTS WITH OBSTRUCTIVE SLEEP APNOEA
S. Mandal, S. Turner, S. Lloyd-Owen. London Chest Hospital, UK
Introduction: We investigated whether or not clinical values, such as BMI and RDI actually correlated with continuous positive airway pressure (CPAP) pressures identified from AutoCPAP studies. We used the pressures derived from AutoCPAP measurements as the minimum pressure patients should be on to abolish their apnoeas 95% of the time. Patients were started on CPAP prior to the AutoCPAP studies. The starting pressure was based on the Clinician’s experience and reflected the severity of the obstructive sleep apnoea (OSA) as well as BMI. These starting pressures were compared to the results from the Autostudies.
Methods: Data were collected from records kept in the physiotherapy department in a Sleep and Ventilation unit from April 2006 to April 2007. All these patients had undergone AutoCPAP studies. The AutoCPAP equipment used was the ResMed Spirit and patients underwent autostudies for three nights. The RDI was derived from the number of apnoea/hypopnoea events occurring per hour from the patients sleep study (an Embletta).
Results: Ninety five patients had AutoCPAP studies. The mean BMI was 44.7 (SD 24.6) and the mean RDI 40.2 (SD 10.1). The mean AutoCPAP pressure was 11.9 cm H20 (SD 2.0) compared to a mean starting pressure of 9.3 cm H20 (that is, the pressure the patient was empirically started on before the AutoCPAP study was carried out, standard deviation 1.8). There was no significant correlation between AutoCPAP pressures and RDI or between AutoCPAP pressures and BMI. A significant correlation (p = 0.01) between starting pressures and RDI was found, this is not unexpected since there is a tendency for clinicians to start at higher pressures if the severity (that is, RDI) is deemed to be greater. A paired t test was then used to determine a correlation between AutoCPAP pressures and starting pressures. There was a significant difference between the two pressures (t = 9.8, p<0.001) suggesting that the clinical estimation of CPAP pressures was inaccurate.
Discussion: These results suggest that we should not be using the patients BMI and RDI to guide the pressure on which patients are started. The results also suggest that all patients should have AutoCPAP studies.
Basic mechanisms of lung disease
CORRELATION OF ALVEOLAR MORPHOLOGY AND PULMONARY FUNCTION IN THE DEXAMETHASONE-TREATED MOUSE MODEL OF EMPHYSEMA
S. V. Stinchcombe, M. Maden. King’s College London, UK
Rationale: Retinoic acid (RA) induces alveolar regeneration in several rodent models of emphysema, based on changes in alveolar histology. It is unknown whether regenerated alveolar tissue improves lung physiology in vivo. Whole body plethysmography (WBP) provides a non-invasive, non-sedated real-time measurement of pulmonary function. In this preliminary study we have assessed the differences in WBP between emphysematous and normal mice using the Dexamethasone (Dex)-treated mouse model. In addition, treatment with RA in post-natal rodents reduces alveolar size and increases alveolar number and surface area (SA). We have assessed the effects of exogenous RA on normal adult mouse lung.
Methods: TO outbred mice were Dex treated (0.3 mg/kg Dex in PBS, daily s.c.) from postnatal day 4–15 (P4–P15). Controls received PBS. From P46–57 half of the control animals received RA (2 mg/kg in DMSO/oil, daily i.p.). On P80 WBP was performed on all animals, awake and breathing spontaneously. Mice were then killed and lung morphology analysed (mean alveolar chord length (Lm), alveolar surface area (SA), lung volume (LV)).
Results: Dex-treated mice showed typical experimental emphysema, with increased Lm and reduced SA compared to controls. Plethysmography of Dex-treated mice revealed increased tidal volume (TV), inspiratory time (tI), expiratory time (tE), peak inspiratory flow (PIf), peak expiratory flow (PEf) and minute volume (MV) and reduced respiratory rate (f) compared with controls (p<0.05 for all comparisons). RA-treated animals showed no change in parameters of lung morphology or WBP compared with controls. Using values from all treatment groups, good correlation was seen between Lm and TV (Pearson’s correlation coefficient 0.73), tI (0.62), tE (0.72), PEf (0.68), f (−0.71) and MV (0.55). SA/100 g body weight showed significant inverse correlation with TV (−0.58), PIf (−0.54), PEf (−0.58) and MV (−0.55).
Conclusions: Spontaneous ventilation is increased in emphysematous Dex-treated mice, reflecting the reduction in gas exchanging SA. Changes in WBP parameters correlate well with alveolar morphology. Further work will use WBP to assess lung function in RA-induced alveolar regeneration. Exogenous RA does not cause morphological or functional change in normal adult mouse lung, suggesting that alveolar SA is physiologically controlled and not permitted to exceed the animal’s maximal metabolic requirements.
ROLE OF THE EPITHELIAL GROWTH FACTOR RECEPTOR IN MEDIATING PROINFLAMMATORY RESPONSES TO RESIDUAL OIL FLY ASH
S. Parnia, L. Hamilton, S. Holgate, D. D. Davies. University of Southampton, Southampton, UK
Background: Residual oil fly ash (ROFA) is a major contributor to fine respirable particulate matter (PM) pollution. Epidemiologic studies have demonstrated an association between PM pollution with increases in cardiovascular and respiratory mortality and morbidity. Acute exposure to ROFA leads to increased IL-8 expression and airway neutrophilia, however the mechanism of this response is unknown.
Objectives: As cigarette smoke and diesel exhaust particle-induced IL-8 expression by epithelial cells involves transactivation of the EGF receptor (EGFR), we studied the effects of ROFA on IL-8 release and the role of the EGFR.
Methods: Primary bronchial epithelial cells (PBEC) were exposed to ROFA. IL-8 and EGFR ligand expression (transforming growth factor α (TGF-α), heparin-binding EGF-like growth factor, and amphiregulin (AR)) were assessed by quantitative RT-PCR and ELISA. The effects of oxidant mediated IL-8 release as well as the effects of downsteam activation of the EGFR were assessed by quantitative RT-PCR.
Results: Exposure of PBECs to ROFA, stimulated transcription and release of IL-8 and EGFR ligands. IL-8 release was blocked by an EGFR neutralising antibody. Administration of an EGFR-selective tyrosine kinase inhibitor as well as inhibitors of MAP kinase pathway inhibited IL-8 gene expression at 6 h further confirming the role of EGFR activation. At 18 h dexamethasone inhibited IL-8 gene expression. By contrast the use of antioxidants did not alter IL-8 release at 6 or 18 h.
Conclusion: These data indicate that expression of IL-8 in response to ROFA is dependent on EGFR activation as well as MAP kinase and NFkB activation and may help to explain the recruitment of neutrophils into the airways of people exposed to particulate air pollution. Treatment strategies may thus allow the possibility of suppressing the epithelial inflammatory responses to particulate air pollution by blocking the EGFR pathway.
ABERRANT LOCAL STEROID METABOLISM AND ITS MODULATION BY INTRAVENOUS SALBUTAMOL IN PATIENTS WITH ACUTE RESPIRATORY DISTRESS SYNDROME
G. Perkins, K. Pettigrew2, S. Rathinam3, P. Rajesh3, F.Gao1, S. Hughes2, C. Bassford2, P. M. Stewart2, D. Thickett2. 1University of Warwick; 2University of Birmingham; 3Heartlands Hospital, UK
Introduction: Exogenous glucocorticoids have been extensively studied as a therapy for patients with acute respiratory distress syndrome (ARDS), but the effects have been disappointing. Surprisingly, there has been little attention paid to local steroid metabolism within the alveolar compartment. Tissue levels of cortisol are regulated by hydroxysteroid dehydrogenase (HSD)-1 and HSD-2. HSD-2 which inactivates cortisol, is elevated in alveolar macrophages (AM) and type II pneumocytes (ATII) in postmortem tissue suggesting that cortisol degradation may be increased in ARDS. We aimed to ascertain if cortisol levels in the lungs of patients with ARDS support a role for aberrant steroid metabolism.
Methods: Cortisol levels were evaluated by ELISA in the bronchoalveolar lavage fluid (BALF) and plasma of patients enrolled into the BALTI-1 study and compared to at risk and normal controls. As expected (BALF) cortisol levels were increased at day 0 and day 4 of ARDS compared to normal and at risk controls. Surprisingly there was no relation between the plasma and lung compartment cortisol levels. There was a negative relation between the severity of lung injury and day 4 BALF cortisol, suggesting local regulation of steroid metabolism may be important in determining cortisol levels. These data are supported by the finding that plasma levels of cortisol did not differ between at risk patients and the ARDS patients in contrast to the alveolar compartment.


Results: In the BALTI-1 study we gave intravenous salbutamol, achieving stable plasma concentrations of 10−6M. Interestingly BALF cortisol at day 4 in these patients was significantly elevated compared to untreated patients, an effect that was not observed in the plasma. This suggests that alterations of local lung steroid concentration might be induced by salbutamol increasing HSD-1 activity. We have detected both HSD-1 and HSD-2 mRNA expression in normal ATII and AMs by PCR.

Conclusions: Local enzymatic regulation of cortisol may be aberrant in patients with ARDS and this process appears modulated by intravenous salbutamol. Since steroids exert powerful biological effects upon inflammation, and lung repair, we believe that the regulation of cortisol levels and its modulation by beta agonists within the lung has significant potential importance.
LIPOPOLYSACCHARIDE-INDUCED UPREGULATION OF TUMOUR NECROSIS FACTOR-ALPHA CONVERTING ENZYME ACTIVITY ON PRIMARY HUMAN MONOCYTES
A. Scott, K. P. O’Dea, J. F. Smythe, J. Handy, M. Takata. Imperial College, London, UK
Introduction: Tumour necrosis factor-alpha (TNF-α) has been implicated in the pathophysiology of numerous disease states encountered in critical care medicine, including sepsis and acute lung injury. TNF-α converting enzyme (TACE) is responsible for cleaving membrane-bound TNF and both TNF receptors to release their soluble forms. Previous research into the regulation of TACE enzymatic activity has been based almost solely on monocyte cell lines. However, cell lines differ from primary human monocytes in terms of TACE post-translational processing. Using a novel, cell-based TACE catalytic activity assay we characterised the effects of lipopolysaccharide (LPS) stimulation on TACE activity in primary human monocytes and examined the underlying mechanisms.
Method: Human peripheral blood monocytes were purified from whole blood by density gradient centrifugation followed by negative immunomagnetic bead selection. Monocytes were incubated with LPS and a variety of pharmacological inhibitors. TACE expression was assessed by flow cytometry and enzymatic activity measured using a fluorescence resonance energy transfer peptide with a TACE specific sequence which fluoresces upon cleavage.
Results: LPS-stimulation produced a rapid (30 min, p<0.05) dose-dependent increase in TACE activity, but had no effect on TACE expression. Up-regulation of TACE activity was attenuated by co-incubation with N-acetyl-L-cysteine (NALC), a broad spectrum reactive oxygen species (ROS) scavenger (fig A, p<0.01), or by pre-incubation with diphenyleneiodonium (DPI), an NADPH oxidase inhibitor (fig B, p<0.01). The superoxide scavengers, superoxide dismutase and its cell permeable mimic MnPyP, failed to produce the same effect. These data indicated that H2O2/. OH- may be responsible for mediating the stimulatory effect of LPS; indeed, exogenous H2O2 mirrored LPS-induced TACE up-regulation (p<0.05).

Conclusion: The rapid increase in TACE activity on LPS-stimulated primary monocytes suggests that the underlying mechanism involves post-translational modification of the enzyme. We have demonstrated that H2O2/. OH-, produced in the respiratory burst by NADPH oxidase, may be the mediator responsible. This has implications for inflammatory diseases such as sepsis, where ROS are overproduced.
Acknowledgement: Supported in part by Westminster Medical School Research Trust.
SUBVERSION OF NEUTROPHIL APOPTOSIS BY STAPHYLOCOCCUS AUREUS
S. Anwar1, L. R. Prince1, I. Sabroe1, S. J. Foster2, M. K. Whyte1. 1Academic Department of Respiratory Medicine, University of Sheffield School of Medicine; 2Department of Molecular Biology and Biotechnology, University of Sheffield, UK
Introduction: Staphylococcus aureus (S aureus) is a major pathogen responsible for severe, invasive infections. Rising antibiotic resistance highlights the need to develop new therapies. Neutrophils kill phagocytosed bacteria and then undergo apoptosis (programmed cell death) which prevents host-derived injury and aids bacterial clearance. Neutrophil necrosis is pro-inflammatory and results in tissue injury. S aureus avoids clearance by neutrophils and intracellular survival is increasingly recognised. Recent work suggests it escapes the phagolysosome and resists killing by subverting autophagy. We propose that S aureus subverts neutrophilic responses with specific effects upon neutrophil survival.
Methods: Human neutrophils were isolated by plasma-Percoll gradient centrifugation of venous blood. Wild type and GFP modified S aureus SH1000 were cultured in RPMI and 10% FCS to exponential or plateau growth phase and co-cultured with neutrophils over a range of MOI (multiplicities of infection). In selected experiments neutrophils were pre treated with 3-methyl adenine, an autophagy inhibitor. Neutrophil apoptosis and necrosis were determined morphologically and by flow cytometry (Annexin V/To Pro 3 staining). Absolute neutrophil counts were determined using flow cytometry count beads.
Results: S aureus alters both neutrophil lifespan and mode of death. Cell counts demonstrate that exponential phase bacteria induce significant loss of neutrophils in a ratio dependent manner (neutrophil numbers at 2 h 39.87 (9.448)% of control at MOI = 1, p<0.001). Annexin V/ToPro3 staining revealed live S aureus induce rapid neutrophil necrosis (control 2.21 (0.97)% vs infected 41.77 (2.95)% at 3 h), without evidence of apoptosis. Exponential phase bacteria (E) cause greater necrosis than plateau phase (P) (E 48.13 (3.48)% vs P 30.48 (4.67)%, MOI = 1). Necrosis was observed in both infected and non infected neutrophils, suggesting induction by a soluble factor. Pre-treatment of neutrophils with 3-methyl adenine attenuated neutrophil necrosis. Heat killed bacteria suppressed neutrophil apoptosis but did not induce necrosis.
Conclusions: S aureus subverts the innate immune response by altering neutrophil death pathways. Apoptosis is suppressed and necrosis is induced. This effect is both bacterial dose and growth phase dependent, with effects extending to non-infected neutrophils. An inhibitor of autophagy attenuates neutrophil necrosis, implicating impaired phagolysosomal maturation in Staphylococcal pathogenesis. A better understanding of these molecular mechanisms may enable therapeutic manipulation in future.
A FAMILY WITH A NOVEL CHROMOSOMAL REARRANGEMENT: A RESOURCE TO IDENTIFY A FURTHER GENE FOR PULMONARY ARTERIOVENOUS MALFORMATIONS AND HEREDITARY HAEMORRHAGIC TELANGIECTASIA
C. L. Shovlin, N. Prigoda, F. S. Govani. Imperial College, London, UK
Background: Pulmonary arteriovenous malformations most commonly occur in the presence of hereditary haemorrhagic telangiectasia (HHT). HHT is caused by mutations in endoglin (HHT1), ALK-1 (HHT2), HHT3 on chromosome 5, HHT4 on chromosome 7, or MADH4 (JPHT). The known genes, and BMPR2, the gene mutated in primary pulmonary hypertension, encode proteins involved in transforming growth factor (TGF)-ݠsuperfamily signalling.
Methods: In the Hammersmith Hospital PAVM/HHT clinic, structured assessments identify individuals in whom associated clinical features suggest the possibility of a novel HHT gene. In ethically-approved studies, DNA is extracted and sent for sequencing of the known HHT genes, with the sequencing laboratory blinded to the lower clinical suspicion of disease gene identification. If mutations are not identified, further studies are commenced to assess if the family would be large enough for disease gene localisation by classical linkage studies, as we have recently performed for HHT3, or whether more innovative approaches are required.
Results: Clinical assessment of an individual referred to the clinic with HHT and PAVMs suggested a low likelihood of HHT1/HHT2/HHT3/HHT4 or JPHT. DNA was sent for mutational screening with other routine samples. No mutations were identified in endoglin, ALK1, or exons 8–11 of MADH4, mutated in JPHT. The lab remained blinded to the sample significance for more than three months. In family assessment, HHT-affected members were identified in three generations. The family was too small for conventional linkage analyses. Cytogenetic analyses identified a chromosomal rearrangement. Short tandem repeat polymorphisms spanning the rearrangement have been used to identify the extent of the rearranged region which co-segregates with HHT. The region does not include any of the five HHT gene loci.
Conclusions: We have identified an HHT/PAVM family with no identified mutations in the known HHT genes. The presence of a novel chromosomal rearrangement that does not include any of the HHT gene loci suggests this family may be an important resource to identify a novel HHT gene, in turn potentially identifying a novel component or regulator of TGF-ݠsuperfamily signalling.
THE ALK3/BMPR-II RECEPTOR COMPLEX MEDIATES BMP-DEPENDENT SMAD1/5 PHOSPHORYLATION IN HUMAN PULMONARY ARTERY SMOOTH MUSCLE CELLS
P. D. Upton1, R. C. Trembath2, N. W. Morrell1. 1University of Cambridge; 2King’s College London, UK
Background: Mutations in the gene encoding the bone morphogenetic protein type II receptor (BMPR-II) are associated with the development of familial pulmonary arterial hypertension (FPAH). Bone morphogenetic proteins (BMP) signal via the type I receptors, ALK3 and ALK6, in combination with BMPR-II, although activin receptors may also mediate BMP signalling. Growth differentiation factor-5 (GDF5) is reported to be a specific ligand for ALK6. We sought to define which receptors mediate phosphorylation of the BMP-specific Smad1/5 signalling proteins in human pulmonary artery smooth muscle cells (HPASMCs).
Method: DNase-digested total RNA was extracted from HPASMCs and expression of BMP receptors was determined using quantitative RT-PCR. To examine Smad1/5 phosphorylation, HPASMCs were incubated in 0.1% FBS overnight and then treated for 60 min with 0.1% FBS alone, or containing BMPs or GDF5, followed by lysis and western blotting. To examine the roles of BMP receptors, cells were transfected with specific siRNA pools (4 duplexes for each) for ALK3, ALK6 or BMPR-II, or a nontargeting siControl pool. After 36 h, cells were then treated with BMPs or GDF5 and lysed for western blotting.
Results: HPASMCs expressed mRNA for ALK2, ALK3 and BMPR-II at high levels, whereas ALK6, ActR-II and ActR-IIB expression levels were low. BMP2, BMP4 and GDF5 all stimulated Smad1/5 phosphorylation, although BMP4 alone was effective at 1 ng/ml. GDF5 was a weaker agonist than BMP2 or BMP4. ALK3 and BMPR-II siRNA transfection both potently abrogated Smad1/5 phosphorylation in response to BMP2, BMP4 or GDF5. In contrast, ALK6 siRNA did not alter Smad1/5 phosphorylation in response to any of these ligands, suggesting the functional Smad1/5 response to GDF5 in HPASMCs does not involve ALK6.
Conclusion: These data show that ALK3 and BMPR-II comprise the main functional receptor complex mediating Smad1/5 responses to BMPs in HPASMCs. Contrary to expectation, GDF5 also induces Smad1/5 phosphorylation via ALK3 and BMPRII, not ALK6. These data provide important insights into the functional roles of endogenous BMP receptors in HPASMCs that are essential if we are to understand the mechanisms of dysfunctional BMP responses in FPAH.
EPIGENETIC MECHANISMS SILENCE ADAM33 EXPRESSION IN BRONCHIAL EPITHELIAL CELLS
H. M. Haitchi, Y. Yang, J. Cakebread, D. Sammut, A. Harvey, J. W. Holloway, P. Howarth, S. T. Holgate, D. E. Davies. Roger Brooke Laboratory, Division of Infection Inflammation & Repair, University of Southampton, UK
Background: ADAM33 polymorphism is strongly associated with asthma and bronchial hyperresponsiveness (Van Eerdewegh P et al, Nature 2002). Although considered to be a mesenchymal cell–specific gene, recent reports have suggested epithelial expression of ADAM33 in severe asthma (Foley SC et al. JACI 2007).
Objectives: As dysregulated expression of ADAM33 may contribute to disease pathogenesis, we characterized the mechanism(s) that control its transcription and investigated ADAM33 expression in bronchial biopsies and brushings from normal and asthmatic subjects.
Methods: The ADAM33 promoter and CpG island methylation were analysed using bioinformatics, luciferase reporters and bisulfite sequencing of genomic DNA. Epithelial-mesenchymal transition was induced using TGF1. ADAM33 mRNA was scrutinised in bronchial biopsies and brushings using RT-qPCR, melt curve analysis and direct sequencing.
Results: The predicted ADAM33 promoter (−550 to +87) had promoter transcriptional activity. Bisulfite sequencing showed that the predicted promoter CpG island (−362 to +80) was hypermethylated in epithelial cells, but hypomethylated in ADAM33 expressing fibroblasts. Treatment of epithelial cells with 5-aza-deoxycytosine caused demethylation of the CpG island and induced ADAM33 expression. In contrast, phenotypic transformation of epithelial cells via a TGFݭinduced epithelial-mesenchymal transition was insufficient to induce ADAM33 expression. ADAM33 mRNA was confirmed in bronchial biopsies, but no validated signal was detected in bronchial brushings from normal or asthmatic subjects.
Conclusion: The ADAM33 gene contains a regulatory CpG island within its promoter whose methylation status tightly controls its expression in a cell type specific manner. ADAM33 repression is a stable feature of airway epithelial cells, irrespective of disease.
Funding: AAIR Charity, The Rayne Foundation & Roger Brooke Charitable Trust (UK).
A POLYMORPHISM IN THE MATRIX METALLOPROTEINASE 9 GENE MAY INFLUENCE EMPHYSEMA DISTRIBUTION IN ALPHA 1 ANTI-TRYPSIN DEFICIENCY
A. M. Wood, G. L. Mcnab, R. A. Stockley. University of Birmingham, Birmingham, UK
Introduction: Polymorphisms in several genes have been associated with upper zone dominant emphysema in chronic obstructive pulmonary disease (COPD). However, patients with alpha 1 antitrypsin deficiency (AATD), the only widely accepted genetic risk factor for COPD, usually exhibit lower zone dominant emphysema. This suggests an important role for genetic variation in determining emphysema distribution. We hypothesised that genes influencing emphysema distribution in usual COPD might also influence patients with AATD. Since upper zone dominant emphysema is uncommon in AATD, occurring in 10.4% of the UK patient registry, those with this phenotype represent a highly selected population in whom genetic influences on phenotype should be readily detectable.
Methods: Patients with the PiZZ genotype of AATD and a stored blood sample suitable for DNA extraction were selected from the UK national registry. Upper zone dominant emphysema (UZDE) was diagnosed using appearance and density mask analysis of patients’ baseline high resolution computed tomography (HRCT) scan of the chest. The proportion of voxels below a threshold level of −910 Hounsfield units (voxel index, VI) was recorded at the level of the aortic arch and inferior pulmonary veins, representing upper and lower zones respectively. Those with a radiological appearance of emphysema and upper zone VI >lower zone VI were deemed to have UZDE, thus giving 36 patients suitable for the study. 50 subjects with lower zone dominant emphysema (LZDE) were randomly selected for comparison. DNA was extracted from blood using a spin column method (DNEasy, Qiagen) and quantifed using the Nanodrop spectrophotometer. Genotyping was carried out for the matrix metalloproteinase 9 (MMP9) C-1562T polymorphism using the amplification refractory mutation system (ARMS), which uses allele specific primers. Their specificity was confirmed by sequencing the PCR product for a control subject. Control DNA from 200 racially matched subjects was genotyped in the same way.
Statistical analyses: Power calculations were carried out using the Genetic Power Calculator. These revealed >80% power to detect a relative risk (RR) of 3 of developing UZDE in our cohort when genotyping 5 times the number of controls (n = 180) for the MMP9 C-1562T polymorphism. We would have had insufficent power to detect a difference conferred by variations in other genes previously associated with UZDE (GSTP1, EPHX1 and MMP1), hence these were not examined. Comparisons of genotype and allele frequency between the UZDE group and controls were carried out using ÷ and Fisher’s exact tests. Comparisons between the UZDE and LZDE group were carried out using logistic regression. Quantitative analyses of genotype against densitometric CT data were not possible, as their non-normal distribution violated the assumptions of ANCOVA.
Results: The SNP was in Hardy Weinberg equilibrium in both patient and control groups. Genotype results were obtained for 34 UZDE subjects, 44 LZDE subjects and 190 controls. There was no significant difference in genotype between the three groups. There was a trend towards association of the T allele with UZDE (p = 0.076), but not with LZDE (p = 0.5), when compared to controls (fig). Subjects with LZDE had smoked more than those with UZDE (Mann-Whitney test, p<0.001), thus to compare the two groups for influences of genotype on outcome smoke exposure was controlled for using a regression model. This showed no significant influence of C-1562T genotype on emphysema distribution (p = 0.545–0.848), though smoke exposure remained a good predictor of LZDE (p = 0.003).

Discussion: Our results suggest the T allele may influence development of UZDE, but did not reach statistical significance, suggesting that it confers an RR of less than 3. A larger study using multinational AATD registries with adequate control matching might be able to confirm/consolidate our findings.
LUNG AND BLOOD T CELL DIFFERENTIATION IN UNTREATED TUBERCULOSIS
A. Dunleavy, R. Breen, M. Lipman. The Royal Free and University College London Medical School, UK
Background: The host T cell response plays a critical role in controlling Mycobacterium tuberculosis infection. Rational and effective immunisation strategies require an understanding of what contributes to protective immunity. Previous work has focussed on detectable changes in peripheral blood T cells, though this may not reflect what occurs at tissue sites.
Methods: Here we have investigated T cell differentiation markers in blood and lung, using cells obtained by induced sputum, from 11 subjects with active TB and 3 healthy controls. TB was pulmonary in 7 cases, lymph node in 2 and abdominal and renal in 1 each. One of 11 subjects was HIV co-infected. Fresh samples were stained with 4 panels of monoclonal antibodies for surface markers which could distinguish naive and memory cell phenotypes. These included CCCR7, CD45RA, CD62L, CD27, CD28 & CD57. Samples were analysed using four-colour flow cytometry.
Results: More pronounced differences were found between induced sputum and blood than in TB compared to control populations within the same body compartments (the table shows representative data). In general, effector memory cells were demonstrated at much higher frequencies in lung than blood. This was consistent across all differentiation marker panels.
Conclusion: The use of non-invasive induced sputum techniques has enabled us to demonstrate important differences between blood and local tissue cell phenotypes. The simplicity of our methodology will allow us to repeatedly investigate subjects over time and within different TB disease states. The information derived from the lung will be of critical importance to models of human TB pathogenesis.
USING TRANSGENIC ZEBRAFISH MODELS TO HELP UNDERSTAND INFLAMMATORY LUNG DISEASE
C. A. Loynes1,2, D. M. I. Trushell1, P. W. Ingham2, M. K. B. Whyte1,2, S. A. Renshaw1. 1Academic Unit of Respiratory Medicine, School of Medicine and Biomedical Science; 2MRC Centre for Developmental and Biomedical Genetics, University of Sheffield, Sheffield, UK
The removal of neutrophil granulocytes from inflamed sites is an essential step in the resolution of inflammatory disease in any organ, including the lung. Neutrophil apoptosis is believed to be critical for this process to occur. However, the molecular events required are poorly understood, at least in part due to the genetic intractability of the neutrophil, and the inability of current models to permit visualisation of inflammation resolution in vivo.
Zebrafish are the ideal model to study in vivo the behaviour of inflammatory neutrophils, and their response to genetic and pharmacological perturbations. The larvae are a simple model of the inflammatory environment, containing all the important cellular and molecular components of the innate immune system, which closely parallels that of humans. Zebrafish have three main advantages over current models for the study of neutrophils. Firstly they are transparent, which allows visualisation of inflammation in vivo. Secondly, they are genetically tractable, and as such they permit ready manipulation of genetic events controlling inflammation resolution, as well as enabling the generation of transgenic lines with labelled neutrophils. Finally they are permeable to small molecules, making them amenable to use in programmes of drug discovery.
We have established a model of spontaneously resolving neutrophilic inflammation in a transgenic line, which labels neutrophils with green fluorescent protein (GFP). We have observed for the first time the morphological and biochemical changes of neutrophil apoptosis during inflammation resolution in vivo. In addition, we have manipulated the process of neutrophil apoptosis using caspase inhibitors, bacterial products and cAMP analogues, and shown that these delay inflammation resolution, strengthening experimentally the link between neutrophil apoptosis and resolution of inflammation in vivo. We have therefore demonstrated the utility of such a line in understanding the biology of a fundamentally important cell in inflammatory disease. We are beginning to use this model to screen for new drugs which we hope will be useful in identifying new compounds for the treatment of inflammatory disease.
Acute exacerbations of chronic obstructive pulmonary disease
FATIGUE AT EXACERBATION OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE
R. Baghai-Ravary, J. K. Quint, J. J. P. Goldring, J. R. Hurst, G. C. Donaldson, J. A. Wedzicha. University College London, UK
Background: Fatigue is a common symptom in chronic obstructive pulmonary disease (COPD) and is related to quality of life (Breslin et al 1998). We have shown that exacerbation frequency is an important determinant of quality of life (Seemungal et al 1998). We therefore examined for the first time whether exacerbations affect fatigue.
Method: Thirty two COPD patients (18 male), mean age 65.9 (SD 9.2) years, FEV1 1.3 l (0.6), FEV1 51.5% (20.7) were assessed when stable and at exacerbation; 18 patients were also examined six weeks post-exacerbation onset. At each clinic visit, questionnaires were completed by the patients on fatigue (Functional Assessment of Chronic Illness Therapy-Fatigue Scale, FACIT-Fatigue) and depression (CES-D) and lung function was measured with a spirometer (Vitalograph). Patients recorded daily increase in respiratory symptoms on diary cards and exacerbations were identified by our usual criteria of two consecutive days of two symptoms (with at least one major symptom), or if in the opinion of the attending clinician the patient was exacerbating.
Results: Patients were seen 4.3 (2.9) days from the onset of exacerbation symptoms. Compared to stable values, at exacerbation there was a significant decrease in FACIT-Fatigue (increased fatigue) of 8.3 (5.9) p<0.001, increase in depression (CES-D) of 6.9 (10.1) p = 0.003 and reduction in FEV1 0.13 l (0.28), p = 0.006. Change in FACIT-Fatigue was related to increase in CES-D (r = −0.46, p = 0.008) and reduction in FEV1 (r = 0.36, p = 0.04). In 18 patients, who attended clinic six weeks post-exacerbation and were without an intervening exacerbation, fatigue had recovered to stable levels (p = 0.48).
Conclusion: Increased fatigue was commonly seen at COPD exacerbation; related to change in FEV1 at exacerbation and increase in depressive symptoms. Fatigue recovered by six weeks from exacerbation onset. Fatigue contributes to the morbidity of COPD exacerbations and needs to be recognised and addressed.
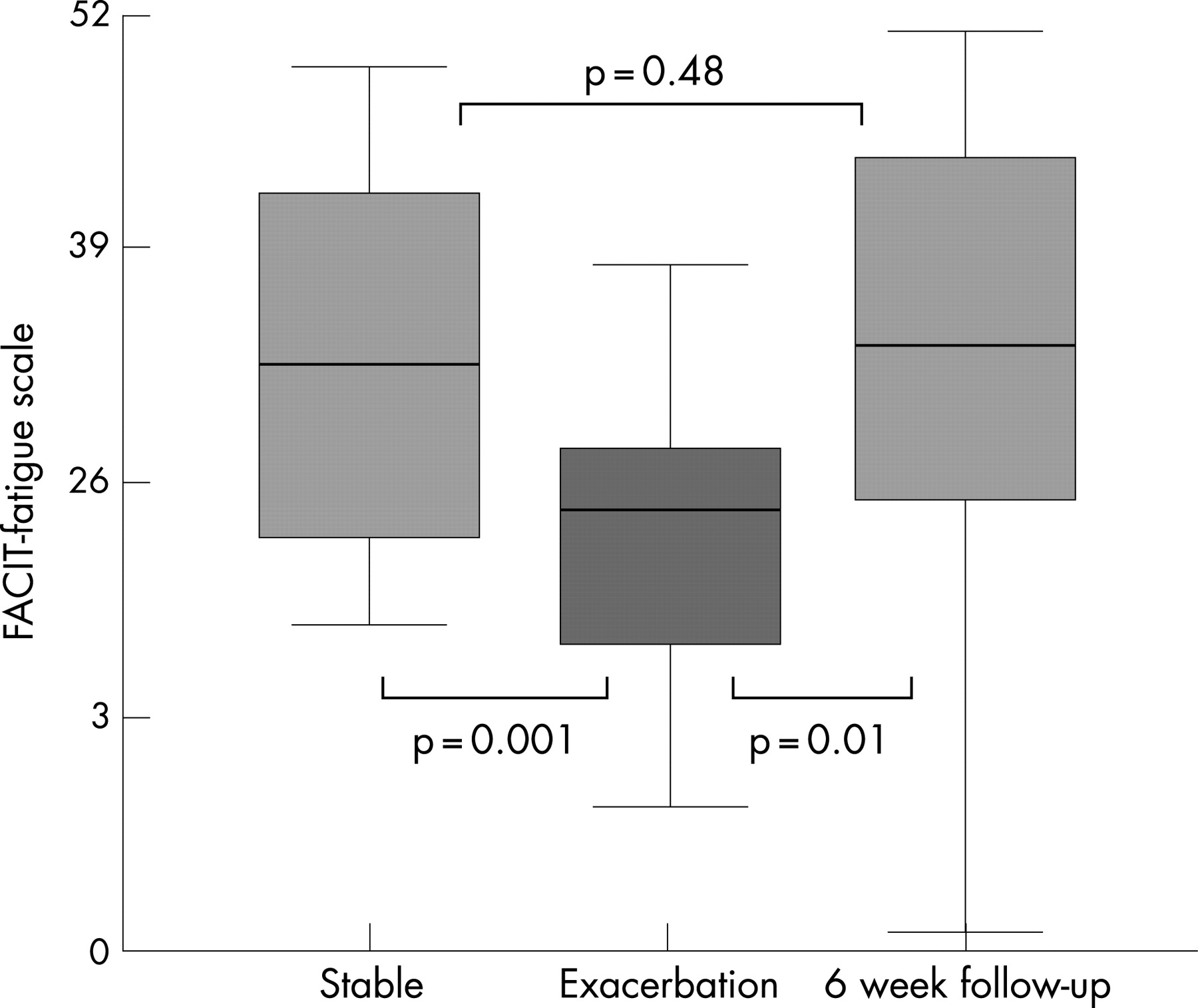
CHARACTERISTICS OF PATIENTS WHO HAVE A FIRST ADMISSION WITH AN ACUTE EXACERBATION OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE
R. Ahmed, A. Dinham, L. Starling, A. Bastin, N. Hill, M. Stern, L. Restrick. Whittington Hospital, UK
Introduction: One aim of early diagnosis of chronic obstructive pulmonary disease (COPD) is to delay time to first admission by appropriate interventions—for example, support to stop smoking, pulmonary rehabilitation (PR), early oral corticosteroids for exacerbations and inhaled corticosteroids (ICS). The aim of this study was to determine in what proportion of patients admitted with acute exacerbation of COPD (AECOPD) to a London inner city hospital the diagnosis of COPD was already known and what interventions had been offered.
Methods: Case records of patients coded as a first admission with AECOPD over one year (May 2005–April 2006) were retrospectively reviewed. Those who were incorrectly coded were excluded. Parameters documented included: age >40, >20 pack-year smoking history, progressive breathlessness, no alternative diagnosis, obstructive spirometry and chest x ray compatible with COPD. In addition we documented how the diagnosis of COPD was made, markers of severity of disease other than spirometry (MRC breathlessness score, acidosis during admission, length of stay (LOS) and in-hospital mortality), smoking status, oral corticosteroid prescription before admission, ICS use, respiratory team input, consideration for PR and in-patient support to stop smoking.
Results: 112 case notes of 123 patients coded as a first admission with AECOPD were reviewed; 11 case notes were incomplete or missing. 62 of 112 were incorrectly coded; 27 had previous admissions with COPD, 30 did not have COPD and 5 were discharged from A&E. 50 patients fulfilled our criteria for COPD and a genuine first admission; 45/50 (90%) had spirometry recorded at some time; mean (SD) FEV1 1.06 (0.40) l and FVC 2.00 (0.68) l; obstructive ratio in 39/45 (87%) and FEV1<1 l in 23/45 (51%) patients. In 11 patients clinical diagnosis was accepted; 6 non-obstructive spirometry, 5 no spirometry. Mean age was 70 (range 47–86) years; 25 male and 25 female. Diagnosis of COPD was not made before admission in 19/50 (38%) patients. Of the 31/50 (62%) where diagnosis was already known, pre-admission spirometry was done in 21/31 (68%; all 13 diagnosed in chest clinic, 8/14 (57%) diagnosed by GP and 0/4 where unclear who diagnosed COPD. In-patient spirometry was performed in 28/50 (56%) patients. MRC breathlessness score was ⩾4 in 22/40, 10/47 (21%) were acidotic during admission, in-hospital mortality was 2/50 (4%) and mean (range) LOS was 10.3 (1–51) days. Interventions in those with COPD diagnosis before admission included: 5/31 (16%) known to have started oral corticosteroids before admission, 14/31 (45%) ever had oral corticosteroids for AECOPD, 21/31 (68%) on ICS on admission, 2/31 (6%) had done PR before the admission and 17/31 (55%) remained current smokers. Documented interventions during admission included smoking cessation advice in 16/25 (64%) smokers, PR considered for 6/28 (21%) appropriate patients, respiratory team input in 32/50 (64%) patients and 33/45 (73%) discharged on ICS.
Discussion: Although this was a first admission with COPD, one in three patients had not been diagnosed before admission despite severe, symptomatic disease. Half had an FEV1<1 l, mode MRC breathlessness score was 4, 20% were acidotic during admission and mortality was 4%. Of the patients diagnosed before admission very few had done PR, only one in six had started oral corticosteroids before admission and only half had ever had oral corticosteroids. Of concern half were current smokers. There were also gaps in in-patient care; only two thirds of patients had respiratory team input, only half had spirometry performed and patients were not offered PR despite an established service. More needs to be done to educate health professionals to make an earlier diagnosis of COPD in at-risk patients, and to offer, and educate patients to ask for, appropriate interventions at diagnosis, in particular support to stop smoking, PR and early use of oral corticosteroids to treat AECOPD.
RISK FACTORS FOR PROLONGED ADMISSION AND EARLY READMISSION IN COPD: A PILOT STUDY USING PARR SCORE
A. Hare, D. Mukherjee, V. Hegade, J. Samuel, B. Yung. Basildon University Hospital, UK
Introduction: Hospital admissions for acute exacerbations of chronic obstructive pulmonary disease (AECOPD) are a major economic burden to health services. Admissions may be prolonged and readmissions frequent. The Patient At Risk of Re-hospitalisation (PARR) score uses hospital discharge data to identify patients at high risk of re-hospitalisation in the 12 months following a “reference” hospitalisation. “Risk scores” are based on a range of patient data derived from current and previous hospitalisation, area of residence and hospital of current admission.
Methods: We performed a pilot audit looking at risk factors for prolonged stay and readmission in patients admitted with AECOPD to our District General Hospital between August 2005 and January 2006. We used the PARR scoring system and examined patient factors easily assessed at admission.
Results: Fifty one patients were identified. Mean age 73 years, 41% male. Mean FEV1 45% predicted. 76% had at least one other significant comorbidity. 29% current smokers. There were no deaths during the reference admission. 12% required NIV during admission. Mean duration of inpatient stay 12 days. 16% were readmitted during the subsequent three-month period. Admission was prolonged (>12 days) in males, patients living alone, requiring NIV during admission, or needing assessment by occupational therapy or physiotherapy. Use of LTOT, home nebulisers, antidepressants or inhaled corticosteroids were not associated with prolonged admission. Patients under respiratory physicians and those who had previously undergone pulmonary rehabilitation (PR) had shorter than average lengths of stay. A PARR score of >50 was associated with a higher than average duration of stay (15 days). A score of <50 was associated with an average duration of stay. Patients admitted for longer than 12 days had an increased rate of readmission in the 3 months following the reference admission.
Conclusions: This pilot study suggests that male patients living alone with high PARR scores may benefit from early intervention by the multidisciplinary team to reduce duration of admission and delay readmission. Patients may benefit from being under the care of a respiratory team, and should be considered for PR (if appropriate). Further large prospective studies are needed to see if early interventions in these patient groups have clinical and cost benefits.
IS EXACERBATION FREQUENCY RELATED TO SOCIAL FACTORS?
J. K. Quint, R. Baghai-Ravary, J. J. P. Goldring, G. C. Donaldson, J. A. Wedzicha. University College London, UK
Background: Viruses are thought to be important causes of exacerbations. A high exacerbation frequency has been shown to be associated with increased frequency of acquiring the common cold. Studies have also shown that viral outbreaks are related to children returning to school. Therefore the spread of respiratory viruses may be associated with contact with young children. We investigated whether social isolation or contact with young children had an effect on a patient’s exacerbation frequency.
Methods: All patients had been recruited in our London cohort for >1 year. We calculated the number of exacerbations recorded on diary cards in a 12-month period and classified patients as frequent or infrequent exacerbators (frequent exacerbators ⩾3 exacerbations/year; infrequent <3). Exacerbations were defined as one major symptom and one major or one minor symptom for more than two days, or the presence of one symptom and treatment with steroid or antibiotic. We studied 78 patients; mean age 71.1 (SD 9.0) years, FEV1 1.1(0.5) l (0.5), FEV1 % predicted 43.6% (18.7) smoking history 43.5 pack years (28.1). Data were collected on various social factors; how many people lived with the patient, how often they had contact with children and their ages.
Results: Fifty two patients were male (66.6%), 29 lived alone (37.1%) and 43 (55.1%) lived with a spouse. 18 patients (23.1%) had daily contact with children under the age of 16, 7 (9.0%) had contact more than twice per week, 10 (12.8%) had contact 1–2 times/week, and 1 (1.3%) less than once a week. 42 patients (53.4%) had no contact with children under the age of 16. The mean age of the youngest child patients had contact with was 5.7 (SD 3.8) years. Exacerbation frequency was not related to living alone, living with a spouse or multiple co-habitants, contact with children or the age of the child (all p>0.05).
Conclusion: It appears that exacerbation frequency is independent of social contacts. It may be that although a large proportion of patients have regular contact with young children, they keep away when they are ill as they are aware of the consequences of exacerbations.
Funding: NIH RO1 HL082578-01.
SEVERITY CLASSIFICATION OF EXACERBATIONS BASED ON QUANTIFICATION FROM DIARY CARD SYMPTOM LENGTHS AND SCORES
K. Vijayasaratha, R. A. Stockley. University Hospital Birmingham NHS Trust, UK
Rationale: Symptom defined exacerbations of COPD are often “unreported” (untreated). Classification of the severity of these episodes is currently based on the level of healthcare use and thus unreported episodes cannot be classified. We explored these details using a scoring system from a symptom-based diary card.
Methods: Symptom diary cards from 23 patients with alpha-1 antitrypsin deficiency (AATD), who were taking part in a trial of AAT replacement therapy (blinded to date) over two years, were studied. Daily scores were recorded for the severity of dyspnoea (5–20), sputum colour (1–5), sputum volume (1–4) and well-being (5–20). Higher scores implied worse symptoms and scores for each symptom were added to give a total daily score. An exacerbation was defined from the first day of an increase in baseline symptoms for two consecutive days and resolved on the first day returning to stable state for at least two consecutive days. Episodes were grouped according to the treatment.
Results: A total of 263 episodes were identified of which 155 (81 treated, 74 untreated) were complete enough to be analysed in detail. The length of the episodes related to health care utilisation, as did the total score and the increase in score seen on the first day of the episode.
Conclusions: The more severe the episode (based on healthcare use), the longer the duration (p<0.001), higher the total score (p<0.001) and greater the increase in score on the first day (p<0.05). The data confirms that symptomatology even as early as the first day and the length of exacerbation relate to healthcare use. The data provide a tool sensitive to patients’ healthcare needs.
DO FREQUENT EXACERBATORS WITH COPD PERCEIVE THEIR EXACERBATION FREQUENCY MORE ACCURATELY THAN INFREQUENT EXACERBATORS?
J. K. Quint, R. Baghai-Ravary, J. J. P. Goldring, G. C. Donaldson, J. A. Wedzicha. University College London, UK
Background: Exacerbations of chronic obstructive pulmonary disease (COPD) are important therapeutic outcomes. Knowledge of exacerbation frequency is important for stratification on clinical trials. We investigated whether perception of exacerbation frequency differs between frequent and infrequent exacerbators.
Methods: We asked COPD patients to recall the number of exacerbations they had in the last year and compared this to the number of exacerbations recorded on diary cards in the 12 months preceding the date of questioning. All patients had been recruited in our London cohort >1 year. Exacerbations were defined as one major symptom and one major or one minor symptom for more than two days, or the presence of one symptom and treatment with steroid or antibiotic. Frequent exacerbators were defined as having ⩾3 exacerbations per year, and infrequent <3. We studied 78 patients; mean age 71.1 (SD 9.0) years, FEV1 1.1 (0.5) l (0.5), FEV1 % predicted 43.6% (18.7) smoking history 43.5 pack years (28.1).
Results: Infrequent exacerbators, on direct questioning perceived a mean of 1.33 exacerbations/year (SD 1.4), but by diary card monitoring had a mean of 1.05 (0.8) exacerbations/year. They overestimated the number of exacerbations in a year by 0.29 (27% of the true value). Frequent exacerbators perceived a mean of 4.14 (1.8) exacerbations/year, but actually experienced 4.75 (1.8) exacerbations in a year. They underestimated the number of exacerbations in a year by 0.61 (12.8%). There was a difference between perceived and actual exacerbation frequency in the frequent and infrequent exacerbator groups (χ2 p = 0.01). 36 out of 42 patients correctly perceived themselves to be infrequent exacerbators (85.7%) and 31 out of 36 patients correctly perceived themselves to be frequent exacerbators (86.1%). 11 patients, (14%) were poor perceivers of their exacerbation frequency. There were no predictive factors to identify these patients; St George’s Respiratory Questionnaire, age, sex, comorbidities, or social factors (all p>0.05).
Conclusions: Frequent and infrequent exacerbators perceive their exacerbation frequency differently. Perception is less accurate at the extremes of numbers of exacerbations; the majority of patients, who have between 1 and 3 exacerbations per year, are the most accurate.
Funding: NIH RO1 HL082578-01.
REPORTED AND UNREPORTED EXACERBATIONS OF COPD-ANALYSIS BY DIARY CARDS
K. Vijayasaratha, R. A. Stockley. University Hospital Birmingham NHS Trust, University of Birmingham, UK
Rationale: Approximately half of symptom defined exacerbations are not reported to medical staff or prompt the patient to change their therapy. We characterised the episodes in detail to determine any difference between reported and unreported episodes.
Methods: Symptom diary cards from 23 patients with alpha-1 antitrypsin deficiency (AATD), who were taking part in a trial of AAT replacement therapy (blinded to date) over two years, were studied. Daily scores were recorded for the severity of dyspnoea (5–20), sputum colour (1–5), sputum volume (1–4) and well-being (5–20) with higher scores indicating worse symptoms. Scores were added to give a total daily score. Mean daily stable state score (DS), total additive score for all days in an exacerbation (TE), and total change in score from baseline during an exacerbation [(?E = TE-(DS × length of exacerbation in days)] were calculated. An exacerbation was defined as an increase in baseline symptoms for two consecutive days and resolution was defined as the first of at least two consecutive days of symptoms returning to baseline.
Results: In total 81 exacerbations that were reported (treatment increased) and 74 unreported (no treatment change) were analysed. Untreated exacerbations had significantly shorter exacerbation length, duration of dyspnoea, sputum colour change, sputum volume change and worse well-being. Further the untreated episodes had lower TE and ?E scores signifying that these episodes are symptomatically milder (see table). In particular the deterioration of “well-being” persisted for less than two days on average for unreported episodes.
Conclusions: The most important determinants of whether a patient seeks medical help or a change in therapy in symptom defined exacerbations are the degree of change and number of symptoms but especially how long the patient feels “less well” than usual.
MANAGEMENT OF COPD EXACERBATIONS IN THE WEEK BEFORE HOSPITAL ADMISSION
S. J. Olive, P. J. Browne, S. N. Ampikaipakan, C. Parfitt, S. W. Watkin. Norfolk and Norwich University Hospital, UK
Fifty one consecutive patients with AECOPD were assessed by proforma for medical and nursing interventions in the week before admission. Patients too unwell for interview were excluded. Details were collected as part of routine assessment of eligibility for supported discharge. Data included: contact with primary care, changes in drug treatment, possession of a self-management plan and whether investigations such as chest examination, pulse oximetry and chest radiograph.
63% did not contact their GP despite worsening COPD. 50% were aware that their chest symptoms were worsening for 3 or more days. 75% of patients had no physical examination by a doctor and 2/3 (n = 13) of those who did see their doctor did not have oxygen saturations checked. One patient had a chest x ray (an open access GP x ray service is available). No patients (or GPs) contacted the hospital respiratory service for advice regarding admission avoidance. There was considerable variation in the management of patients with no evidence of adherence to the BTS/NICE guidelines (BTS 1997, NICE 2004). Less than a third (n = 15) of patients had any change in treatment (increased bronchodilator therapy, oral corticosteroids, antibiotics). 25 of the 51 patients initiated their own admission by dialling 999, 17 contacted their GP (of whom 2 were told to dial 999), 8 contacted the out of hours service (of whom 6 were told to dial 999) and 1 contacted the practice nurse. Although 9 patients in the study had self-management plans, only 2 of these contacted their doctor and none stepped up their treatment.
An opportunity exists for intervention before admission with AECOPD and a randomised study will test whether a helpline to the supported discharge service team +/− early home visit improves exacerbation management.
QUALITY INDICATORS FOR NON-INVASIVE VENTILATION SERVICES: A SURVEY OF 100 UK NHS HOSPITALS
C. M. Roberts, R. Stone, R. Buckingham, N. Pursey, D. Lowe. Royal College of Physicians, UK
Several randomised controlled trials (RCTs) have demonstrated the efficacy of non-invasive ventilation (NIV) in the management of COPD patients admitted to hospital with type II respiratory failure. This treatment is now widely if not universally available in UK hospitals and applied to many admissions. The 2003 UK national audit of acute hospital COPD care demonstrated that observed outcomes for patients treated with NIV were far worse than those expected from the RCTs. One reason for this may be that the standards of implementation of NIV in clinical practice are less rigorous than those of RCT conditions. In addition we have previously reported that patients are unaware of this important medical intervention and recommended that information be provided to patients at risk of admission whilst in a stable clinical state. As part of the National COPD Outcomes and Resources Project (NCROP) we collected baseline quality data on a number of service areas including NIV provision. We examined this data against 12 service quality recommendations from the BTS and NICE and consensus standards derived from a panel of multidisciplinary clinicians, managers and patients that form the NCROP steering group.
One hundred NHS Trusts recruited for NCROP were surveyed. Lead clinicians were asked if their service met indicators “in full”, “partially”, or not at all. Further information was sought to the reasons if not or only partially met. At the time of abstract submission 98 of 100 Hospitals had provided baseline data. 76/95 (80%) provided NIV for all eligible persistently hypercapnic COPD patients admitted, 18 (19%) partially met this criterion whilst 1 unit did not provide this service. 71/94 (76%) provided NIV in an area where staff were fully trained to deal with this treatment. Where not fully met this was because of inadequate specialist bed provision or trained nursing staff. 74/96 (77%) had a designated consultant lead for the service. 53/94 (56%) hospitals had a multidisciplinary training programme for all staff whereas 7 (7%) units had no programme at all. When asked if staff outside of specialist respiratory wards knew how to manage COPD and the indications for NIV 37/95 (39%) responded met in full whilst 9 (9%) not met at all. 83/95 (87%) had written management protocols for NIV but only 55/96 (57%) provided protocols in all areas where NIV was administered and only 37/95 (39%) fully met the provision of individualised written instructions for patients including escalation beyond or cessation of NIV. A full range of masks and pillows was available in 52/96 (54%) hospitals whereas 9 units had only a standard mask provision. 30/95 (32%) of units carry out a comprehensive annual audit of NIV use whilst 27 (28%) perform no audit at all.
Regarding provision of patient information only 17/94 (18%) hospitals fully met the provision of written information on NIV for patients whilst 67 (71%) did not meet this criterion at all. When asked if the unit had a policy for providing information on NIV to patients when in a stable clinical state e.g. outpatients or pulmonary rehabilitation only 6/95 (6%) of units fully met this whilst 67 (71%) did not meet this at all. Further explanation provided by hospitals did suggest that many units were aware of the need to provide information and many were actively looking to provide information packages and were formulating policies.
We conclude that there is great variability in the quality of service provided between NHS Trusts and that these often do not meet the recommended standards and those used in the RCTs upon which the recommendation to implement NIV services are based. It is of concern that there remains a deficiency in the provision of information to patients regarding this significant medical intervention. It is possible that the poor survival of COPD patients given NIV observed in the 2003 UK national audit may in part or whole be accounted for by the variable quality of service provision. It is encouraging that many of the units engaged in NCROP are aware of their weaknesses and are actively addressing these. NCROP aims to define minimum standards and improve the quality of services offered to COPD patients across the UK and will be re-surveying all the participants in 2008. NCROP provides summaries of its findings to the National Service Framework working party.
SURVEY OF THE USE OF NON-INVASIVE VENTILATION IN THE CLINICAL MANAGEMENT OF ACUTE COPD IN 233 UK HOSPITALS
S. Kaul, I. Coutts, D. Lowe, M. Roberts, M. Pearson. Royal College of Physicians, UK
Background: Non-invasive ventilation (NIV) is a clinically proven, cost-effective intervention for acidotic exacerbations of chronic obstructive pulmonary disease. This survey examined the extent to which recommendations are being followed in the UK and assesses whether results from randomised controlled trials (RCTs) are reproduced in practice.
Method: Between August and October 2003 a national audit of COPD exacerbations was conducted by the Royal College of Physicians and the British Thoracic Society. 233 UK hospitals each prospectively identified 40 consecutive acute COPD admissions, documenting process of care and outcomes from a retrospective case note audit. Units also completed a resources and organisation of care proforma.
Results: Patient and organisational audit data were available for 233/247 (94%) of UK hospital units. Nineteen hospitals (8%) did not offer NIV. There was no access to NIV in 92 (39%) ICUs, in 88 (36%) HDUs and on the general wards of 85 (34%) hospitals. In 74 (30%) hospital units it was available on all three sites. A low pH (<7.35) was noted at some time during admission for 26% (1714/6544) of patients and NIV was administered to 31% of them. Of the 1714 with acidosis, patients receiving NIV were more likely to: be under, or to be seen by, a respiratory specialist, have more severe disease (higher PCO2 (median 9.8 vs 7.8 kPa), lower oxygen tension (median 8.8 vs 9.8 kPa), higher incidence of peripheral oedema (48% vs 39% ), have radiological pneumonia (27% vs 16%) and have longer hospital stays (median 9 days vs 7 days) than those who did not receive NIV. But there was a higher mortality rate (in-hospital (26% vs 14%) and at 90 days (37% vs 24%)) which was present for each level of acidosis when NIV was used. Confining analysis only to those would have qualified for the plant trial reduced but did not abolish this negative outcome. Furthermore those hospitals who gave NIV not at all or rarely, had similar mortality and case-mix to those who used NIV most. Those hospitals least likely to offer NIV, or who did not offer the treatment at all, did not have higher mortality rates than those who did.
Conclusions: NIV is not uniformly available. Patient access depends as much on hospital organisation and resources as on clinical need. The observed results in routine practice do not match the results achieved in RCTs. Potential explanations of this challenging outcome include that important case-mix variables were not collected, inappropriate selection of patients by hospitals, or even a challenge to the RCT conclusions. Translating RCT evidence into the reality of everyday NHS practice is not straightforward.
DOES MANAGEMENT OF ACUTE EXACERBATION OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE IN THE COMMUNITY IMPROVE THE OUTCOMES? A PROSPECTIVE OBSERVATION STUDY
K. Patel, R. Olayan, R. Kedia. Mid Cheshire Hospitals NHS Trust, Leighton Hospital, UK
Background: Acute exacerbation of chronic obstructive pulmonary disease (COPD) is a common medical emergency, which can account up to 10% of acute medical admissions. The latest NICE guidelines (2004) for management of COPD, recommend that selected cases of acute exacerbation of COPD can be easily managed in the community, thus obviating need for hospital admission and saving hospital bed days.
Aim: In a prospective observational study, we compared the difference in outcome of COPD exacerbation in patients who did or did not receive treatment in community prior to hospitalisation.
Method: We recruited 32 patients with acute exacerbation of moderate to severe COPD (as per NICE criteria) admitted to medical admission unit between May to June 2007 were. Data on patients’ demography, characteristics including duration of stay, length of treatment and mortality were recorded.
Results: See table.
Conclusion: This study highlights that prior treatment of COPD exacerbation in community does not seem to reduce the duration of symptoms, length of treatment and hospital stay in patients with moderate to severe COPD. We recommend developing a model of care to assess patients with moderate to severe COPD with acute exacerbation in community for assessment, treatment and early hospital admission by Supported Early Discharge or Rapid Response Team to improve care and reduce the duration of exacerbation.
A PILOT STUDY OF INTENSIVE PHYSIOTHERAPY AND RESPIRATORY NURSING INPUT FOR PATIENTS WITH AECOPD ADMITTED TO GENERAL MEDICAL WARDS
P. Vaughn1, K. Ross1, L. Bryceland1, I. Bryce1, B. Sloan2, C. Bray3, C. E. Bucknall1. 1Stobhill Hospital; 2Department of Public Health, University of Glasgow; 1Greater Glasgow & Clyde NHS Board, UK
Background: Hospitalisation with an acute exacerbation of COPD (AECOPD) is associated with impaired quality of life, reduced exercise capacity and increased risk of readmission (Garcia-Aymerich, Thorax 2003). Spruit (Chest, 2003) showed that such in-patients showed a 5% decline in quads muscle strength from day 3 to day 8. A subsequent cohort study confirmed this finding and showed that the time spent walking and standing while in hospital correlated with quads muscle strength (Pitta, Thorax 2006).
Aim: To provide intensive physiotherapy input to promote early mobilisation and sputum clearance to these patients and respiratory specialist nurse review within the existing service framework.
Method: Daily physiotherapy for patients admitted to these wards; respiratory nurse specialist review before discharge; pulmonary rehabilitation referral at discharge and contact by telephone one month after discharge to assess mobility, level of breathlessness and further healthcare use.
Results: Seventy seven patients admitted to nine medical wards were assessed (average age 72.3 years; range 46–87 years). 52 (67%) patients were able to undertake regular exercise and 50 patients were contacted by telephone at one month; 27 patients were not able to participate and were not followed up, usually because of significant comorbidity and/or because they were awaiting long-term care; this subgroup was no different from those able to undertake early mobilisation in terms of age, lung function or BMI. Significant improvements in leg extensions, arm raises, sitting to standing and marching exercises were achieved (all p<0.001). Average (paced) step test duration at assessment was 91.1 seconds and at discharge 121.9 seconds; mean difference = 20.68, 95% CI (0.65 to 40.70), p = 0.043. Telephone follow-up of 50 patients showed: breathlessness level returned to baseline: average MRC breathlessness score = 3.2 (SD 1.1), n = 49 compared with pre-exacerbation score average = 3.35 (SD 1.16), n = 77; 10 readmissions for 9 patients (18%); further antibiotics 15 (30%) and prednisolone 14 (28%); continued use of exercise reported by 43/50; eight new referrals for pulmonary rehabilitation.

Conclusions: 67% of patients admitted to general medical wards with an AECOPD were able to undertake activities of leg extensions, arm raising, sit to stand and marching on the spot at an early stage of their admission, with the additional physiotherapy input provided. This subgroup were similar to the whole cohort in terms of age, lung function and BMI. Significantly increased activity, as judged by observed exercise levels at assessment and discharge, was observed, with a significant improvement in step test time (p = 0.043) on objective assessment of mobility. This additional input was successfully integrated into the existing hospital service. A formal RCT is required to confirm these observations and formally test the impact on readmissions and quality of life.
Funding: An educational grant from Boehringer Ingelheim and Greater Glasgow NHSB.
CAUSE OF DEATH IN PATIENTS HOSPITALISED WITH ACUTE EXACERBATIONS OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE
C. L. Pearce, P. W. Jones, E. H. Jones. St George’s Medical School, University of London, UK
Background: The TORCH study (Calverley et al. N Engl J Med 2007;356 :775–89) showed that only 35% of stable out-patients with moderate to severe chronic obstructive pulmonary disease (COPD) died of pulmonary causes. Other causes of death were cardiovascular disease (27%) and cancer (21%). The contribution of non-respiratory disease to mortality of patients hospitalised with COPD exacerbations is not known and has potential implications for treatment. We therefore determined the reported cause of death in patients hospitalised with acute exacerbations of COPD (AECOPD).
Methods: Patients admitted with AECOPD over two years (2005–6) who died in hospital were identified using ICD-10 codes for obstructive lung disease. The hospital death certificate database was searched to establish reported cause of death (part Ia); comorbidities contributing to death (parts Ib, Ic and II); and to ensure all people with COPD recorded on their death certificate were included.
Results: 160 patients died: 90 in 2005; 70 in 2006 (23% and 13% of annual COPD admissions). Patients who died were 56–96 years (range), 87 male, 73 female and stayed in hospital for 0–57 days before death. 128 (80%) of patients died from a respiratory cause, 6% from cardiovascular disease, 2% from cancer and 13% from other causes. Cause of death was not affected by age or gender. In 63 (49%) patients with a respiratory cause of death, non-respiratory co-morbidities were considered to have contributed to mortality (34 (54%) cardiovascular, 4 (6%) cancer, 5 (8%) both CVD and cancer and 20 (32%) other causes). Patients dying of cardiac and respiratory causes had a slightly, but not significantly (p = 0.093) shorter median time from admission to death than patients dying of cancer or other causes.

Conclusions: Most patients with AECOPD die of a respiratory cause, although comorbidities, particularly cardiovascular disease contribute to death in nearly half. The emphasis of treatment for patients with AECOPD should remain on their respiratory problems, but comorbidities should be investigated and managed.
Investigations and outcomes in pulmonary fibrosis
SURVEY OF A MULTIDISCIPLINARY MEETING FOR THE DIAGNOSIS OF INTERSTITIAL LUNG DISEASE
R. A. Heinink, B. Holloway, S. Trotter, J. Reynolds, P. S. Burge. Birmingham Heartlands Hospital, UK
Background: Accurate diagnosis is critical to the management of interstitial lung disease. The American Thoracic Society (ATS) and European Respiratory Society (ERS) have previously highlighted the importance of a dynamic diagnostic process involving physician, radiologist and pathologist (all with a specialist interest in lung disease). We present data from a 2 year cohort of the Interstitial Lung Disease Multi-Disciplinary Meeting (ILD-MDM) at our hospital.
Method: 137 patients were discussed a total of 168 times between November 2004 and October 2006. The ILD board recommendations were compared with the medical records to identify discordances with subsequent practice, and to identify their reasons.
Results: First presentation included results of bronchoalveolar lavage differential cell count (BAL) in 56, transbronchial biopsy (TBB) in 27 and surgical biopsy in 15. Table 1 shows the number of investigations which were suggested by the multidisciplinary board, whether they were carried out, and why not if they weren’t. Table 2 shows the diagnostic conclusions reached by the ILD-MDM board. No conclusion was made in 42 patients for a variety of reasons, including 4 who were awaiting investigation. Not including these 4 patients, 71.4% (95/133) of the patients discussed were given a diagnosis by the ILD-MDM board at the first or subsequent presentation.
Conclusion: The ILD board reached a diagnosis in 71% of patients presented. The ratio of cases of idiopathic interstitial pneumonias diagnosed without open biopsy concords with guidelines. There remains a reluctance of physicians to recommend somewhat unpleasant investigations recommended by the board in some patients despite the consequences of giving inappropriate treatment without a diagnosis.
COHORT MORTALITY STUDY OF CRYPTOGENIC FIBROSING ALVEOLITIS
J. M. Harris1, R. M. Rudd2, I. D. A. Johnston3. 1Imperial College (NHLI); 2London Chest Hospital; 3University Hospital, London, UK
Background: Many studies have addressed the issue of increased lung cancer risk among patients with cryptogenic fibrosing alveolitis (CFA); recently the study by Hubbard et al (Am J Respir Crit Care Med 2000) reported an excess relative risk of 7.31. Two independent co-mortality studies of US data (Wells and Mannino, South Med J 1996) and UK data (Harris et al, J Epidemiol Community Health 1998) have failed to confirm these findings.
Methods: We now report vital status of members of the BTS CFA cohort study (588 patients). With the help of the Office for National Statistics, vital status to 31 December 2001 was determined for all but three subjects.
Results: In total, 487 (83.2%) individuals had died; 46 (9.4%) had lung cancer (ICD9 162) recorded on their death certificates. The observed frequencies were compared against numbers expected from age- and sex-specific rates 1990–2001 for England and Wales, and Scotland, with results summarised in the table as standardised mortality ratios (SMR) with 95% confidence intervals (95% CI). Stratified analyses demonstrated increased risk of lung cancer mortality among younger subjects (those aged <69 years; 285 subjects, 28 lung cancer deaths; SMR 10.59). Similar results were found when analyses were stratified by sex and by smoking habits; higher risks were observed for males (363 subjects, 40 lung cancer deaths; SMR 8.09) and for past or current smokers (441 subjects, 44 lung cancer deaths; SMR 8.31).
Conclusion: It appears that these patients with CFA experienced an increased risk of lung cancer. Non-small cell lung cancers probably start to grow from the first malignant cell approximately 10 years before clinical manifestation while for small cell cancers the interval is approximately three years (Geddes, Br J Dis Chest 1979). Given that the carcinogenic process began some time before diagnosis, both diseases, CFA and lung cancer, are so closely linked in time that it remains uncertain which started first.
THE PROGNOSTIC VALUE OF HIGH RESOLUTION CT SCORES IN PATIENTS WITH CRYPTOGENIC FIBROSING ALVEOLITIS SYNDROME AND A CLINICO-RADIOLOGICAL DIAGNOSIS OF IDIOPATHIC PULMONARY FIBROSIS/FIBROTIC NON-SPECIFIC INTERSTITIAL PNEUMONIA
Z. H. Hoo1, N. Hirani1, P. A. Mcfarlane1, A. J. Simpson1, J. M. Murchison2. 1University of Edinburgh; 2New Royal Infirmary, UK
Introduction: Idiopathic pulmonary fibrosis (IPF) has a highly characteristic appearance on high resolution CT (HRCT) scan, but about 50% of patients have a “non-diagnostic” HRCT appearance. A significant proportion of these patients have a bibasal and peripheral pattern of disease without honeycombing dominance and only surgical lung biopsy can thus distinguish IPF from fibrotic non-specific interstitial pneumonia (NSIP). In the UK, biopsy is performed relatively infrequently, hence the importance of stratifying patients based on HRCT appearance.
Aims: To determine the components of a detailed baseline HRCT score that best predicted 2-year mortality in patients with cryptogenic fibrosing alveolitis (CFA) syndrome and predominantly basal and peripheral disease, ie, a clinico-radiological diagnosis of IPF/fibrotic NSIP.
Methods: This retrospective study involved 41 patients presenting from 2000–2006. A radiologist blinded to the patients’ clinical details scored the baseline HRCT scans for the extent of “ground-glass” and detailed “reticular/fibrosis” patterns (0–100% to nearest 5%). Severity of “bronchiolectasis and bronchiectasis” were scored 0–3. The log-rank test was performed for each HRCT parameter dichotomised into “high” (>sample median) and “low” (>sample median) scores. Baseline characteristics (sex, age, smoking status, baseline FVC and presence of emphysema) were similarly analysed. The prognostic value of baseline HRCT scan was compared to the current “gold standard” prognostic indicator in IPF; >10% FVC decline at 6 months.
Results: The baseline HRCT scores (mean (SD)) that predicted reduced 2 year cumulative survival were: (a) “High” “bronchiolectasis and bronchiectasis” score (>0.167): 57.9 (11.3)% vs 90.5 (6.4)%, p = 0.015; (b) “High” “reticular score” (>12.5): 60.0 (11.0)% vs 90.2 (6.6)%, p = 0.030. The HRCT parameters were not influenced by baseline characteristics. Ground-glass score and baseline characteristics had no prognostic value. Patients with relative FVC decline of >10% 6 months post-baseline HRCT scan had a 2-year cumulative survival of 29.2 (17.3)% (vs 84.8 (6.2)% for those without such decline, p = 0.000095).
Conclusion: In patients with CFA syndrome and a clinico-radiological diagnosis of IPF/fibrotic NSIP, the baseline HRCT and in particular the “bronchiolectasis and bronchiectasis” score is a potentially useful prognostic tool. Although not as specific as >10% decline in FVC at 6 months, the baseline HRCT score has important implications for patients at presentation and for those patients who maintain FVC.
RELATIONSHIP BETWEEN RIGHT HEART CATHETERISATION AND NON-INVASIVE MEASURES OF PULMONARY HYPERTENSION IN PATIENTS WITH FIBROSING LUNG DISEASE
T. J. Corte, M. Gatzoulis, S. J. Wort, A. U. Wells. Royal Brompton Hospital, London, UK
Introduction: Pulmonary hypertension (PH) is common in interstitial lung disease (ILD) and associated with a poor prognosis. As the gold standard test, right heart catheterisation (RHC) is invasive and resource-limited, reliable non-invasive measures of PH are needed.
Methods: All ILD patients referred for RHC during 1997–2007 were included (n = 95; 54 male; age 56.5±12 years). All patients had concurrent echocardiography and pulmonary function. The relationship of RHC mean pulmonary artery pressure (mPAP) and pulmonary vascular resistance index (PVRi) to echocardiographic variables, pulmonary function, exercise capacity, as measured by 6 minute walk testing (6MWT, n = 58) and brain natriuretic peptide (BNP, n = 36), was examined.
Results: 64 of 95 patients had PH on RHC (mean (SD) mPAP 32.2 (12.7) mm Hg, pulmonary vascular resistance (PVR) 5.7 (4.3) WU, cardiac output 4.3 (1.2) litres/min) and echocardiography (mean RVSP 57 (19) mm Hg (n = 70), pulmonary acceleration time (PAT) 97.6 (27.6) ms (n = 65)). Diagnoses included idiopathic pulmonary fibrosis (n = 21), non-specific interstitial pneumonia (n = 28), sarcoidosis (n = 20), hypersensitivity pneumonitis (n = 11), other ILD (n = 15). There was major functional impairment (DLco 31.6 (18.2)%, Pao2 8.5 (2.5) kPa, desaturation <89% on 6MWT in 81%). BNP levels were 19 pmol/l (1.4–342). mPAP correlated with echocardiographic parameters (RVSP (r = 0.53, p<0.0001), peak tricuspid velocity (r = 0.46, p<0.01), degree of tricuspid regurgitation (r = 0.33, p<0.01), PAT (r = −0.35, p<0.01), resting pulmonary function (DLco/VA (r = −0.22, p = 0.03), Pa o2 (r = −0.35, p<0.001)) and BNP (r = 0.4, p = 0.02). No correlation was found with 6MWT variables. On stepwise linear regression, RVSP (p<0.0005) and Pa o2 (p<0.01) were independent determinants of mPAP (equation r2 = 0.33). Similarly, PVRi correlated with echocardiographic parameters (RVSP (r = 0.45, p<0.001), tricuspid gradient (r = 0.4, p<0.01), PAT (r = −0.34, p = 0.02)) as well as DLco/VA (r = −0.34, p<0.01), Pa o2 (−0.28, p = 0.03) and BNP (r = 0.49, p = 0.01). On stepwise linear regression, RVSP (p<0.001) and Pa o2 (p<0.05) were independent determinants of mPAP (equation r2 = 0.29).
Conclusion: PH has important prognostic and potential therapeutic implications in patients with fibrotic lung disease. mPAP and PVRi, as measured by the gold standard RHC, correlate with echocardiographic measures of PH (particularly RVSP, and PAT), as well as DLco/VA, Pa o2 and BNP. These results, especially the combination of RVSP and Pa o2, have the potential to guide physicians in the selection of patients referred for RHC.
ESTIMATION OF ASBESTOS FIBRE CONCENTRATION IN INDUSTRIES CONSISTENT WITH RISK OF ASBESTOS-RELATED DISEASE
N. Jarad, R. Mason, S. Spencer-Jones. Bristol Royal Infirmary, UK
Background: Estimating the intensity of asbestos exposure is important for the attribution of lung pathology to previous asbestos exposure. It also has implications for both medical and medico-legal reasons. There has previously been no comprehensive comparative review of the concentration of occupational asbestos exposure in the atmosphere.
Methods: This is a descriptive paper. Articles were identified using several research methods. Data were collected for 189 different activities within a range of professions involving asbestos exposure. 66 citations were reviewed; research papers (and their associated references), textbooks, official health and safety documents and relevant websites. The data reviewed ranges from 1975–2002. For exposure intensity, we took the average daily concentration of fibres for each occupation as reported in the relevant literature. Occupations were divided into five categories according to average fibre/ml (f/ml) exposure concentration: (1) very heavy exposure (>25 f/ml); (2) heavy exposure (15–24 f/ml); (3) moderate exposure (5–14 f/ml); (4) light exposure (1–4 f/ml); and (5) very light exposure <1 f/ml.
Results: The mean (range) of f/ml asbestos concentration for the five groups according to the order of classification was as follows: 148.7 (35.5–500), 21.25 (18.5–24), 7.9(6–11), 2.9(1.1–4.9) and 0.37(0.13–0.87). The concentration of fibres for most occupations has declined over time, following the instigation of safety methods. The most effective methods of reducing dust intensity were (in descending order): dust extraction by vacuuming, wetting the equipment and the dust, and improved ventilation.
Conclusion: We describe the average estimated intensity of asbestos exposure for people who worked in occupations that used asbestos fibres. The concentration of airborne asbestos fibres has reduced over the years according to the literature. However, the risk of malignant mesothelioma continues to be present if appropriate protection for asbestos fibre inhalation does not take place.
LUNG TRANSPLANT REFERRALS FOR IDIOPATHIC PULMONARY FIBROSIS IN NOTTINGHAM
G. Jenkins. University of Nottingham, UK
Background: Idiopathic pulmonary fibrosis (IPF) is a progressive, ultimately fatal, condition for which lung transplant is indicated. There is low window of opportunity for transplant in this group of patients due to their age and the rate of progression of disease that makes timing of referral for transplant critical. However, the guidelines for transplant referral produced by British Thoracic Society (BTS) and the International Heart and Lung Transplant Consensus Group (IHLT) are inconsistent.
Objective: The aim of this study was to estimate the proportion of eligible patients referred for transplant and whether current referral guidelines for patients with IPF appear appropriate.
Sample: Notes of all patients diagnosed with IPF at Nottingham University Hospitals by high resolution CT scanning between Jan 2002 and Jan 2004 were reviewed. Patients with at least 2 documented gas transfer measurements were included in the audit.
Main outcome measures: Change in gas transfer, transplant referral, and the proportion of who had died by July 2007 were documented.
Results: Mean (SD) age of patients at diagnosis was 66.58 (1.19) years and the mean (SD) DLco at diagnosis was 44.9 (2.8)% predicted. The proportion of patients who subsequently died was 57% and only 1 patient was referred for transplant. On the basis of age alone (<65 years) 37% were eligible for transplant at diagnosis. Using BTS and IHLT guidelines the proportion eligible for transplant at diagnosis was 35% were 18%, respectively. The proportion of these patients who subsequently died was 50% and 22%, respectively. IHLT guidelines recommend referral following a 15% drop in DLco over 6 months, whereas the BTS guidelines do not precisely specify a rate of change in lung function. None of our patients were eligible for transplant based on these criteria. However, in patients under 65 years an average drop in DLco of 2% or greater over 3 months was associated with 62.5% mortality.
Conclusion: Our data suggest the number of patients referred for lung transplant is low and that rate of change of DLco might be a more important indicator for transplant referral in eligible patients (<65 years) than absolute values of DLco.
IS HIGH RESOLUTION CT USEFUL FOR PREDICTING LUNG FUNCTION DECLINE IN PULMONARY SARCOIDOSIS? A RETROSPECTIVE STUDY OF 21 CASES
T. K. Loke, A. Devaraj, J. Van Der Leer, S. Grubnic, D. S. Mcgrath. St George’s Healthcare NHS Trust, London, UK
Rationale: High resolution CT (HRCT) is highly sensitive for detecting early parenchymal changes in pulmonary sarcoidosis (PS). Although the HRCT features of PS are well described, it is unclear whether these features provide prognostic information in patients with this condition. We conducted a retrospective study of patients with PS who had undergone HRCT at the time of diagnosis, and correlated pulmonary function tests (PFTs) performed at baseline and at 2 years, with features on their initial HRCT.
Methods: HRCT and PFTs were performed according to standard protocols. Two radiologists scored parenchymal abnormalities on HRCT independently and discrepancies were resolved by consensus. Data for FEV1, FVC and TLCO were expressed as means (SD). PFTs at baseline and at 2 years follow-up were compared using the paired t test; correlations between HRCT scores and changes in PFTs were analysed using Spearman’s rank correlation coefficient.
Results: 21 cases of PS (13 cases histologically confirmed) were available for this study. Mean FEV1 (2.39 (0.71) litres; 78.4 (17.6)% predicted) and FVC (3.25 (0.96) litres; 89.96 (18.60)% predicted) at 2 years did not change significantly compared to baseline. A small but significant decline in TLCO (mean change: −5.9 (17.3)%; p = 0.042) was seen at 2 years compared to baseline (mean % predicted: 75.8 (17.4)). HRCT scoring of traction bronchiectasis (r = −0.60, p = 0.04) and linear opacities ((r = −0.72, p = 0.01) correlated inversely with FEV1 decline at 2 years. The extent of nodularity, ground glass opacities, honeycombing, parenchymal bands or masses did not correlate with changes in FVC or TLCO during this period.
Conclusion: Traction bronchiectasis and linear opacities detectable on HRCT may be associated with progressive decline in pulmonary function. Longer-term studies are needed in order to clarify this.
FAMILIAL IDIOPATHIC PULMONARY FIBROSIS, WITH BONE MARROW HYPOPLASIA AND HEPATIC NODULAR REGENERATIVE HYPERPLASIA: A NEW SYNDROME?
A. Talbot-Smith1, W. Syn2, G. Macquillan3, D. Neil2, E. Elias2, P. Ryan1. 1Hereford County Hospital; 2University Hospital Birmingham; 3University of Western Australia
Background: Familial idiopathic pulmonary fibrosis (FIPF) accounts for between 0.5–2.2% of all cases of IPF. We report for the first time a family with features of IPF in association with bone marrow hypoplasia (BMH) and hepatic nodular regenerative hyperplasia (NRH) which we believe is a new familial syndrome.
Cases: Sibling 1—a 34-year-old male builder/carpenter presented with acute dyspnoea, with HRCT revealing IPF. He had abnormal liver function tests (LFTs), thrombocytopenia, lymphopenia and a hypocellular bone marrow. Despite corticosteroids he deteriorated and died 10 months after presentation. Post-mortem (PM) examination confirmed IPF and hepatic NRH with portal hypertension. The siblings’ father, a retired bricklayer aged 74, then presented with a four-month history of dyspnoea. Pulmonary fibrosis was confirmed on HRCT along with pleural thickening. He also had thrombocytopenia but normal LFTs. He failed to attend appointments and died suddenly 18 months later. A PM examination revealed usual interstitial pneumonitis (UIP), liver NRH with portal hypertension, and mild focal myocardial fibrosis. Sibling 2—a male bricklayer aged 46, also presented with dyspnoea. HRCT showed pulmonary fibrosis with UIP pattern and pleural thickening on video-assisted thoracoscopic surgery (VATS) lung biopsy. He had thrombocytopenia with lymphopenia, a hypocellular bone marrow and abnormal LFTs. He failed to respond to treatment with corticosteroids and azathioprine and died 6 months later awaiting lung transplantation assessment. A PM examination revealed florid UIP, asbestos pleural plaques and hepatic NRH with portal hypertension. Sibling 3—a carpenter/joiner aged 57, was asymptomatic when referred for assessment. However an HRCT was consistent with IPF. CT of his abdomen revealed varices and “radiological evidence” of cirrhosis. He also had thrombocytopenia with a hypocellular bone marrow. He failed to respond to corticosteroids and azathioprine, and developed abnormal liver function tests despite discontinuing azathioprine. He developed respiratory failure but was turned down for lung transplantation due to the haematological disorder and died 4 years after presentation. A PM examination showed features of NRH with portal hypertension. All four cases had no evidence of autoimmune disease. Pro-thrombotic states were excluded in siblings 1 and 3. Only sibling 2 was known to have had some asbestos exposure.
Discussion: Familial IPF is believed to be an autosomal dominant condition with variable penetrance and multiple aetiologies. Hepatic NRH is condition characterised by microvascular damage, and nodule formation without fibrosis. It is believed to be caused by obliteration of the portal venous microcirculation and results in non-cirrhotic portal hypertension. However, a percentage of patients eventually progress to liver failure. Liver function tests are often normal and a diagnosis of NRH can easily be overlooked. Liver biopsy and a high index of clinical suspicion are required. In NRH, microvascular injury leads to ischaemic damage with secondary regeneration of hepatic nodules while, in IPF, chronic inflammatory process triggers fibroblast activation and collagen deposition. The triad of BMH, NRH and pulmonary fibrosis may have arisen independently due to within organ effects of a single genetic defect, or may be causally interrelated. A possible unifying hypothesis we propose is that the thrombocytopenia which was a common presenting feature in the family may have been indicative of abnormalities in platelet function which caused obliteration of small portal vein radicals and subsequent “downstream” lung injury when the hepatic “filter” function failed. Alternatively, an as yet undefined bone marrow derived endothelial or thrombotic factor may cause secondary hepatic nodule formation, and up-regulation of pro-fibrogenic mediators such as connective tissue growth factor that leads to lung fibrosis. The association of NRH with haematological states such as polycythaemia rubra vera, primary macroglobulinaemia and myeloid metaplasia further support this hypothesis. It is also possible that lung inflammation is the primary event with activation of pro-inflammatory cytokines causing secondary damage, although this is not a common feature of other forms of pulmonary fibrosis.
Conclusion: We have described a new syndrome of idiopathic pulmonary fibrosis, bone marrow hypoplasia and hepatic nodular regenerative hyperplasia occurring in one family. Although the underlying pathological process remains undetermined, we have discussed possible hypotheses.
Management of pleural diseases
DIAGNOSTIC YIELD OF THE CLINICAL INVESTIGATIONS OF PLEURAL EFFUSION
E. Nour, M. Rudolf. Chelsea and Westminster Hospital, London, UK
Background: Pleural effusions, the result of accumulation of fluid in the pleural space, are common medical problems. The aim of the study was to assess the adequacy, complications and diagnostic yield of various clinical investigations and improve current practice by comparing what was done with the British Thoracic Society guidelines.
Methods: This was a retrospective study, conducted over 1 year period January–December 2005. All patients investigated for pleural effusion were identified from computerised records of the chemical pathology, cytology, and microbiology departments and case notes were examined.
Results: A total of 140 records of patients were reviewed. The most common diagnoses were: malignancies (27.1%), pneumonia (25%), congestive cardiac failure (20%) and tuberculosis (15.7%). Pleural aspiration was performed in 137 patients. 11 had pneumothorax; four of them required chest drain. Classification of exudative and transudative pleural effusion was not applicable in 33 patients because of lack of information of total serum protein, serum and pleural fluid LDH. 24 (57.1%). Pleural fluid specimens were positive for malignancy from 15 patients and 22 (47.9) were negative from 18 patients. Abrams’ needle pleural biopsy specimens were diagnostic in 10 patients and non-diagnostic in 10, true negative in 10 and inadequate samples in 2 patients. 167 pleural fluid samples were obtained for bacterial culture, 7 (4.2%) samples from 5 patients were true bacterial culture positive. 74 pleural fluid samples were obtained for TB culture, 11(14.9%) from 11 patients were TB culture positive. Bronchoscopy was performed in 25 patients, diagnostic in 8 patients with lung cancer and 4 out 7 patients with tuberculous effusions.
Conclusion: Total serum protein, serum and pleural fluid LDH should be measured to apply Light’s criteria in patients with pleural fluid less than 30 g/l. Microbiologic testing of pleural fluid specimens should be ordered more selectively as the positive yield of microbiologic smear and cultures on pleural fluid specimens is very low. Abrams’ needle biopsy still has a place in the diagnosis of malignant and tuberculous effusions. Bronchoscopy should be considered in the presence of a mass, haemoptysis or suspected tuberculous effusion with a negative pleural fluid, biopsy and sputum.
CLOSED PLEURAL BIOPSY IN DIAGNOSIS OF SUSPECTED PLEURAL MALIGNANCY: HOW USEFUL IS IT?
N. Surange, S. Das. Stockport NHS Foundation Trust, UK
Background: Blind percutaneous pleural biopsy has a low diagnostic yield in malignant pleural effusion. Video-assisted thoracoscopic surgery (VATS) has high diagnostic yield and negative predictive value. Stepping Hill Hospital does not have VATS available on site; but radiology services including staging CT scan and image-guided biopsy have improved recently. We audited the closed pleural biopsies aiming to review our diagnostic pathways for unilateral pleural effusion.
Methods: Retrospective analysis of patients (n = 54) who underwent pleural biopsy with Abrams needle between 1 January 2005 and 31 December 2006. We collected data from histology reports, radiology reports, clinical and lung cancer MDT records. We obtained clinical records of 51 cases.
Results: Adequate samples were obtained in 48/54 cases (89%). 17 biopsies diagnosed carcinoma. Final diagnoses in 51 patients included cancer in 30 (59%) and other diagnoses in 12 (23%). Definite diagnosis could not be established in 9 (17%) patients. Of the cancers, the diagnosis was Primary lung carcinoma in 9 (17%), mesothelioma in 5 (10%), metastatic breast carcinoma in 6 (11%), metastatic ovarian carcinoma in 5 (10%), metastases from other sites 4 (8%), non-Hodgkin’s lymphoma in 1 (<2%). Other diagnoses included CCF in 4 (8%) and parapneumonic effusion in 8 (16%). Of the 30 carcinomas, pleural biopsy diagnosed 17 (59%)—6 primary lung cancer, 1 mesothelioma, 9 metastatic carcinoma and 1 non-Hodgkin’s lymphoma. Simultaneous pleural fluid cytology was positive in 13/51 patients (43% of cancers). In the cytology negative cases, pleural biopsy was diagnostic in 4, VATS in 4 and radiologically guided biopsy from other site in 7 cases.
Conclusion: Our audit showed diagnostic rate of 59% on closed pleural biopsy, a slightly higher yield over pleural fluid cytology. In most patients CT scan identified an accessible lesion, diagnosed pneumonia and abdominal or pelvic malignancy. Radiologically guided biopsy was diagnostic in all cases. Our findings suggest that CT scan and image-guided biopsy are useful tools in the diagnosis of suspected malignant, cytology negative, pleural effusion where thoracoscopy services are not available.
SPECIALIST REGISTRAR LED CHEST ULTRASOUND SERVICE IN A LARGE TEACHING HOSPITAL
S. Baird, A. Ashish, M. Haris, J. Koch, C. N. Smyth, M. J. Walshaw. Royal Liverpool and Broadgreen University Hospital, UK
Introduction: BTS guidelines (2003) on pleural effusion management state that where infection or malignancy is suspected the effusion should be sampled, and a drain placed if pus is present. Unfortunately, where the effusion is small, loculated, or deeply situated, fluid sampling and drain insertion can be difficult and pleural ultrasound (USS) may help. However, this traditionally requires the assistance of the radiology department, with the inevitable management delays. Furthermore, many radiology departments merely mark appropriate chest wall sites which may have altered with posture when the patient returns to the ward. To speed up the diagnostic and treatment process for these patients, we investigated the utilisation of pleural USS by respiratory medical staff using a portable machine at the bedside.
Methods: We looked at 18 scans in 14 consecutive patients (mean age 65 years (range 39 to 82), 11 male) over 3 months. All were carried out by a respiratory SpR (SB) following a short pleural USS training course.
Results: Eleven patients (79%) had a pleural USS as part of their initial procedure: suspected empyema/loculated effusion on radiography (9, 50%), failed pleural tap (2, 11%), small effusions (3, 17%), and fluid volume estimation in non-functioning drains (4, 22% (3 repeat)). At 6 procedures (43%) empyema was diagnosed and immediate USS-guided chest drains inserted. The remaining 8 were exudative effusions: 5 parapneumonic (needle drainage), 2 lung cancer (1 USS-guided drain, 1 USS-guided pleural biopsy), and 1 volume estimation for a non-functioning drain. All were carried out <24 hours of the request with no complications. In 14 cases where fluid sampling was the objective, this was successful in 13 (93%): the remaining case had an insignificant amount of fluid.
Conclusion: If the required skills and equipment exist within the chest department, a pleural ultrasound service performed the respiratory wards can be effective and timely, improving the quality of the patient journey. Although it is not included in the core skills essential for the training of respiratory SpRs, it is a useful technique which is easy to learn and consideration should be given to including it in the respiratory SpR curriculum.
AN AUDIT OF PERCUTANEOUS PLEURAL BIOPSY IN THE INVESTIGATION OF PLEURAL EFFUSION IN A DISTRICT GENERAL HOSPITAL
M. Masoli, J. Goldman. Torbay Hospital, UK
Introduction: Blind pleural biopsy has traditionally been used in the investigation of exudative pleural effusions. This study aims to examine the efficacy of pleural biopsy in the investigation of pleural effusion in a district general hospital.
Method: Patients undergoing pleural biopsy between June 2004 and June 2005 were identified from Torbay Hospital pathology database. Case notes and pathology reports of these patients were analysed retrospectively. All patients had presented to respiratory teams with a pleural effusion requiring further investigation.
Results: 46 patients were identified, 36 had blind Abrams biopsies, 10 had CT guided biopsies.
12/36 (34%) of Abrams biopsies were insufficient for assessment and in only 17/36 was pleura identified. No difference was noted in yield between SpRs and SHOs/HOs under SpR supervision. 28 had a final diagnosis of malignancy. Abrams biopsy had a diagnostic yield of 21% (6/28). With CT guided biopsy pleural tissue was identified in 100% of cases. 6/10 were positive for malignancy with 8 having a final diagnosis of malignancy, yield 75% (6/8). 22/36 of patients required further investigation after a blind pleural biopsy (11 VATS, 6 CT guided biopsies). Pleural fluid cytology correctly diagnosed malignancy in 36% of cases. No fatalities were reported and no patients had any significant complications.
Conclusion: Blind pleural biopsy and pleural cytology were diagnostic of malignancy in only 21% and 36% of cases, respectively. This falls below the expected yield of 57% for malignancy stated in BTS guidelines. The relatively low yield for blind pleural biopsies may be due to several factors including operator inexperience, which is likely to increasingly become an issue with changes to specialty training. In contrast, CT guided biopsies demonstrated a high yield for malignancy (75%). This study would confirm the relatively low yield of blind pleural biopsies in the investigation of malignant pleural disease in a DGH setting and support the use of CT guided pleural biopsies.
THE USE OF BEDSIDE THORACIC ULTRASONOGRAPHY IN A DISTRICT GENERAL HOSPITAL
P. Cadden, M. Najib, R. Sundar. Royal Albert Edward Infirmary, UK
Background: Transthoracic ultrasonography (TUS) is being used more frequently by respiratory physicians and therefore has escaped the domain of radiology. Ultrasound machines have multiple uses, eg, guiding the placement of central lines and assessing the abdomens of trauma patients. The widespread use of these machines in respiratory medicine will allow faster assessment of respiratory patients suffering with pleural disease. We have access to an ultrasound machine that is shared with the emergency and acute medicine departments. We report our initial experience with bedside TUS in a district general hospital including indications, outcomes and safety of use.
Methods: Over a 2 month period a record was maintained of patient details and indications for procedure as well as subsequent procedures.
Results: A total number of 28 bedside ultrasound scans were performed under consultant supervision by 3 trainee respiratory physicians. Patients ranged from 16 to 87 years old (mean 76; median 68). The indications included pleural effusion (n = 14), empyema (n = 5) and query complete drainage of fluid on previous occasion (n = 7). A small or larger effusion was found in 12 patients. Loculated effusions were identified in 3 patients. 60% had a subsequent procedure, ie, diagnostic aspiration, pleural biopsy, drain insertion or removal after their bedside ultrasound. We calculate that 35% had a change in their management as a result of the ultrasound appearances, ie, definitive drain management, further imaging ordered, surgical referral etc.
Conclusion: We found that procedures were easy for trainees to perform under the supervision of a competent consultant respiratory physician in the same way as all trainees learn the art of flexible bronchoscopy. Bedside availability provided immediate access to images which guided and altered patient management in a large proportion of patients and has resulted in decreased workload for our radiology department. We believe that this imaging modality should be taken up more widely by respiratory physicians and taught to all respiratory trainees in the country to provide better patient care for patients suffering from pleural disease. We estimate that in a 12 month period approximately 100–120 ultrasounds would be performed and justify the cost of obtaining the necessary equipment.
PROPHYLACTIC ANTIBIOTICS FOR MEDICAL THORACOSCOPY: IS THERE A NEED FOR IT?
H. Lockman, M. F. Bone. South Tyneside District Hospital, UK
Introduction: Medical thoracoscopy is being used more and more by respiratory physicians for diagnosing and managing pleural diseases. The use of prophylactic antibiotic for the procedure is unclear. We have performed medical thoracoscopy using standard bronchoscopes (Olympus) via a thoracoport without prophylactic antibiotics. We note that in some centres prescribing prophylactic antibiotics for patients undergoing the procedure is standard practice.
Method: All patients who had medical thoracoscopy between the period of May 2005–April 2007 were included. The patient details were tracked via the endoscopy records. Medical case notes were retrieved, and results of biochemistry, pathology and radiology were reviewed electronically.
Results: 53 procedures were performed on 52 patients. Only 50 medical case notes were retrieved. 3 more patients were excluded (procedure were abandoned in 2 patients, and 1 patient had 2 thoracoscopies in 6 months) (n = 47). Average age for the procedure was 66.8 (19–89 years old). 4 had the procedure for unresolving pneumothorax, 12 malignant effusion, 1 empyema, and 30 for investigation of pleural effusion. 33 (70%) had CT chest, 38 (80%) pleural fluid analysis (35 were exudates) and 20 (43%) chest drains prior to thoracoscopy. Antibiotics: 11 (23%) were on antibiotics up to 8 weeks before the procedure, 5 (11%) were on antibiotics when they had thoracoscopy, and 18 were on antibiotics up to 8 weeks after the procedure. Samples from the procedure: 1 was positive for acid fast bacilli, 1 had MRSA (sputum and carriage sites were previously positive, had a chest drain before thoracoscopy), 1 was positive for Pseudomonas 6 days after the procedure (pus swab previous drain site), 1 for Moraxella catarrhalis (blood cultures 1 month later), and 1 had sputum positive for MRSA and Pseudomonas aeruginosa. All of these 3 patients also had chest drains respectively prior to the thoracoscopy.
Conclusion: The rate of infection is low for medical thoracoscopy. The infections that we see are iatrogenic from previous chest drains (4 patients, 9%). It is safe to perform medical thoracoscopy on patients without the need for prophylactic antibiotics.
COMPLIANCE WITH BRITISH THORACIC SOCIETY GUIDELINES FOR THE MANAGEMENT OF SPONTANEOUS PNEUMOTHORAX IN 2 UK TEACHING HOSPITALS
P. T. Tzoulis, J. S. H. Hogg, S. B. P. Pearson. Leeds Teaching Hospitals NHS Trust, UK
Introduction: British Thoracic Society (BTS) updated guidelines for the treatment of spontaneous pneumothorax in 2003 in an effort to standardise treatment and improve clinical practice. Previous studies suggested that compliance with 1993 BTS guidelines was only 20–40% among non-respiratory staff. One of the purposes of the 2003 BTS guidelines was to reduce length of hospitalisation and pain for many patients. It was estimated that adherence to these guidelines would prevent approximately 7000 unnecessary chest drain insertions per year in the UK. There is still concern about the variability in the management of pneumothorax. We used the audit criteria suggested in 2003 BTS guidelines.
Aims: To compare management of pneumothorax in two teaching hospitals against BTS guidelines. To collect data about timing of suction, referral rates to thoracic surgeons and its timing and number of chest drains clamped.
Methods: Retrospective medical notes audit of 49 patients presenting with spontaneous pneumothorax to Leeds General Infirmary and St James’s University Hospital over a 1-year period between 1 February 2006 and 1 February 2007.
Results: Of 49 cases reviewed (mean age 45.9 years, 37 males, 12 females), 12 (24.5%) were lifelong non-smokers, 16 (32.6%) were ex smokers, 21 (42.8%) were current smokers.15 patients (30.6%) had an episode of pneumothorax in the past (8 ipsilateral, 8 contralateral). Traumatic and iatrogenic pneumothoraces were excluded. 31 episodes of primary pneumothorax were studied. There were 3 tension pneumothoraces which were treated as recommended. Observation was decided for 1 small, asymptomatic pneumothorax and one patient denied any interventions. Only 50% (13 of 26) of primary, non-tension pneumothoraces were treated initially with aspiration which is recommended as first line treatment for all primary pneumothoraces requiring intervention and 50% were treated with chest drainage. Only 2 out of 13 simple aspirations were successful. In 1 case tension pneumothorax was developed 6 hours post aspiration. After initial unsuccessful aspiration, repeated aspiration was performed only in 3 cases (should be considered in 9 cases according to guidelines) and it was successful in 1 case. Overall, 26 of 31 primary pneumothoraces were treated with intercostal tube insertion. Chest drainage was successful in 92% (24 of 26 patients). Recurrence rate, at 3 months, after simple aspiration was 33.3% (1 of 3) and recurrence rate after tube drainage was found 11.5% (3 of 26 patients).All patients managed successfully with aspiration did not require admission, while median length of stay after chest drainage was 4 days. 18 episodes of secondary pneumothorax were studied. Underlying lung diseases were COPD (8 patients), asthma (5), fibrosing alveolitis (5), lung cancer (5), lung metastases (1). In all cases chest drain was the initial management apart from a patient with small pneumothorax who was managed initially with aspiration and subsequently with drainage. In 16 out of 18 patients (88.8%) drainage was successful. Median length of stay was 10 days and recurrence rate at 3 months was 11.1%. Of the 44 patients managed with intercostal tube drainage, 5 were complicated by surgical emphysema (not life threatening). No case of penetration of major organs or pleural infection was documented. Suction was applied to 73.9% (17 of 23) of patients with a persistent air leak (continued air bubbling through an intercostal tube 48 hours after insertion). In 41% (7 out of 17) of patients it was commenced less than 48 hours post drain insertion, but never directly after tube insertion. Mean time of application of suction was 3.5 days post drain insertion. 5 cases of persistent air leak were referred to thoracic surgeons requiring inpatient surgical intervention. Referral to thoracic surgeons is recommended after 3 days of persistent air leak for secondary and after 5 days for primary pneumothoraces. Mean time of referral was after 6.5 days of persistent air leak for secondary (2 referrals) and after 5 days for primary (3 referrals). 10 out of 39(25.6%) non-bubbling chest tubes were clamped for several hours before their removal to detect small air leaks. No case of detected air leak as well as no complication was documented. In 1 case pneumothorax recurred within 24 hours after tube removal without previous clamping requiring re-insertion of chest drain. Most cases (41 of 49) were managed initially by A+E. Respiratory staff managed initially 6 cases, medical 1 case and thoracic surgeons 1 case. All patients were managed after admission by respiratory physicians apart from 4 admissions (2 thoracic surgeons, 1 care of the elderly and 1 general medicine).
Conclusion: Compliance with guidelines is suboptimal, especially in the management of primary pneumothorax. Chest drain insertion is still used as first line treatment for primary pneumothoraces in many cases. Aspiration was found considerably less effective than chest drainage in primary pneumothoraces contrary to recent randomised controlled trials.
THE MANAGEMENT OF SPONTANEOUS PNEUMOTHORAX
S. Grundy, A. Sukuraman, M. Paracha. Blackpool Victoria Hospital, UK
Introduction: We were interested to know how closely the British Thoracic Society guidelines for the management of spontaneous pneumothorax were followed and how effective interventions such as applying suction to drains and replacing small intercostal drains with larger “surgical” drains are.
Methods: A sample of 51 cases of spontaneous pneumothorax, who presented between January 2005 and May 2007, were reviewed retrospectively. This included 33 primary pneumothoraces and 18 secondary pneumothoraces. Average age of patients with primary and secondary pneumothoraces was 38 and 70 years, respectively. 65% were male. The underlying diagnoses in cases of secondary pneumothorax were COPD (12), interstitial lung disease (3), asthma (2) and lung cancer (1). The table shows the initial management strategy for cases in each group of patients according to BTS guidelines. The recommended interventions are highlighted in bold italics.
Results: All patients who had no intervention had radiological follow up confirming complete resolution. Aspiration was performed on 14 occasions. It was successful in 5/10 (50%) primary pneumothoraces and 3/4 (75%) secondary pneumothoraces. Aspiration was only attempted twice in 1 case. All other failed aspirations proceeded to intercostal drain insertion. Of 29 drains inserted as first line therapy, 17 were Seldinger drains and 12 large bore surgical drains. There was no difference in efficacy between the different types of drain. 9 Seldinger (Portex Ltd, Hythe, UK) drains were replaced with large drains (28–32 French). 3/9 (33%) were effective. 6/9 (66%) were unsuccessful and required further intervention. Low-pressure, high-flow suction was applied to 20 drains. 15/20 (75%) required surgical intervention despite suction. 4/20 (20%) resolved following placement of a larger drain and only 1 resolved with suction alone. However, in this case suction was applied immediately after insertion of drain. Overall compliance with BTS guidelines was met in only 51% of cases. The bulk of cases when guidelines are not followed involve placement of a drain when aspiration should be attempted first. This occurred in 18/30 (60%) cases when aspiration is recommended. When a drain was the recommended therapy there was 77% compliance.
Conclusion: This audit suggests that suction is not an effective intervention and results in prolongation of presence of a drain. It may be reasonable to replace a Seldinger drain with a larger “surgical” drain if pneumothorax does not resolve. Large bore surgical drains are still being inserted inappropriately as first line therapy in a substantial number of patients with primary pneumothorax with associated pain and risk of complications. We believe further education is required to promote the BTS guidelines and would welcome a large randomised controlled study evaluating the efficacy of applying suction to intercostal drains.
ARE WE CONFORMING TO CURRENT BTS GUIDELINES ON THE MANAGEMENT OF PRIMARY SPONTANEOUS PNEUMOTHORAX?
F. Guarasci, J. Gelder, K. A. Rodger. York Hospital, UK
Introduction: The current British Thoracic Society (BTS) guidelines for the management of primary spontaneous pneumothorax (PSP) suggest simple aspiration as the first intervention in those who are breathless or have a rim of air >2 cm on chest radiograph (CXR). Those patients without either of these features are either discharged or observed.
Aims: To assess whether our institution is currently conforming to these guidelines.
Methods: Data were collected retrospectively from case notes of patients admitted with a diagnosis of PSP between 1 April 2003 and 1 June 2007. Initial and subsequent management was reviewed including the administration of oxygen and the use of suction. Measurements of pneumothorax size were taken using a calibrated Medview v5.0.0 diagnostic workstation.
Results: 57 episodes of PSP occurred in 47 patients between the study dates. Mean age was 27.5 years (range 16–48 years). 40 (85%) were male and 21 (45%) were smokers. 36 of the 57 episodes (63%) were defined as large by BTS criteria, the other 21 were all non-uniform in appearance and of these 9 (16%) were defined as small and received no intervention. 37 episodes were treated by aspiration in the first instance. Only 14 (38%) of these were felt to be successful enough to merit discharge. 3 episodes were treated with a second aspiration and all of these proceeded to intercostal chest drain (ICD). 23 episodes were treated with ICD after failed aspiration and 11 episodes were treated by ICD initially. In this combined group none were given oxygen in accordance with BTS guidelines and 11(32%) required suction. All patients requiring ICD had a Seldinger tube inserted in accordance with BTS guidelines (size range 12–18 French). In the 11 episodes where ICD was the first intervention only 1 patient had evidence of tension pneumothorax on CXR. A total of 46 (81%) of these episodes were treated according to BTS guidelines in there initial intervention.
Conclusion: The majority of patients admitted to our institution with PSP were treated in accordance with current BTS guidelines.
IS SURGICAL ACCESS OR PROCEDURE PERFORMED THE PRINCIPAL DETERMINANT OF OUTCOME FOR SURGERY TO PREVENT RECURRENT PNEUMOTHORACES?
E. Lim1, E. Maratos2, A. Barker2, L. Edmonds2. 1Royal Brompton Hospital, London; 1Papworth Hospital, Cambridge, UK
Background: We have highlighted the importance of surgical access in a systematic review reporting a 4-fold increase in pneumothoraces with video-assisted thoracoscopic surgery (VATS) compared to open surgery aimed to prevent recurrent pneumothoraces. To further our work, we aimed to evaluate the influence of the type of pleurodesis (pleurectomy versus pleural abrasion) whilst adjusting for surgical access (VATS versus open).

Methods: A systematic literature search undertaken for studies on pneumothorax surgery in Medline, Embase, Cochrane Library, Internet trial registers and conference abstracts identified 29 studies (4 randomised and 25 non-randomised) eligible for inclusion. A fixed effects meta-analysis was performed to pool within study recurrence rates between two different forms of access (VATS versus open surgery) where the same pleurodesis procedure was performed in both groups and meta-regression used to determine the between study influence of type of pleurodesis (pleurectomy versus pleural abrasion).
Results: In the 19 studies that performed the same pleurodesis through two different forms of access, the overall relative risk of recurrence for VATS was 4.731 (95% CI 2.699 to 8.291; p<0.001) compared to open surgery. Of the 19 studies, 3 used a combination of pleurectomy and abrasion, and 1 study performed blebectomy alone. Of the 15 studies that performed exclusively pleurectomy or pleural abrasion (9 pleurectomy, 6 pleural abrasion) in both access arms. Meta-regression suggested no statistically significant difference in the impact of procedure on recurrence rates (p = 0.220).
Conclusion: Current evidence suggests a four fold increase in recurrence of pneumothoraces when a similar pleurodesis procedure is performed using VATS compared to an open approach. After adjusting for access, the type of procedure did not influence the outcome to prevent recurrent pneumothoraces.
Asthma: airways inflammation
CASE SERIES OF ATYPICAL PRESENTATION OF ALLERGIC BRONCHOPULMONARY ASPERGILLOSIS
A. Shah, A. Proudfoot, S. Khan, R. Vancheeswaran, D. Creer. Barnet General Hospital, UK
Allergic bronchopulmonary aspergillosis (ABPA) is a complex hypersensitivity inflammatory reaction within airways in response to inhalation of Aspergillus spores in an aspergillus-sensitive patient. ABPA occurs primarily in patients with asthma (1–2%) or with cystic fibrosis (CF) (1–15%).
While there are 19 isolated reports of cases where patients did not have clinical asthma, only two series describing patients diagnosed with ABPA without asthma masquerading as malignancy have been reported and none in recent years. We report a series of 6 patients diagnosed with ABPA between 2004 and 2006 at Barnet General Hospital with an atypical presentation.
Methods and results: We performed a retrospective survey of respiratory patients from Barnet General Hospital between the period January 2004 to December 2006. During this period there were 6 new cases of ABPA with no background history of asthma or CF. Standard diagnostic criteria were used to confirm diagnosis. Average age of patients was 66 years old, five were male and three were ex-smokers. Four of the patients had obstructive spirometry but none showed evidence of bronchodilator reversibility.
Conclusion: Asthma is the first criterion for a diagnosis of ABPA in all reported series. This case series highlights the importance of considering serological testing and investigation for ABPA in those patients with any combination of pulmonary infiltrates and eosinophilia irrespective of age and history of asthma or atopy. Moreover, it demonstrates that the associated “mucoid impaction syndrome” which has been described in 14–54% of ABPA patients can masquerade as bronchial carcinoma, particularly in the elderly population where clinical suspicion of malignancy is often high and suspicion of ABPA low.
1. Berkin KE. Lung collapse caused by allergic bronchopulmonary aspergillosis in non-asthmatic patients. BMJ 1982;285 :552–3.
2. Sanchez-Alarcos J. ABPA mimicking bronchogenic cancer. Allergy 2001;56: 80–1.
RELATIONSHIP BETWEEN ASTHMA SYMPTOMS, SPIROMETRY, DISEASE SEVERITY AND EXHALED NITRIC OXIDE WITH EXACERBATION RATE IN PATIENTS ATTENDING ROUTINE PRIMARY CARE NURSE-LED CLINICS
D. Menzies1, C. Jackson2, C. Mistry1, B. Lipworth1. 1University of Dundee; 2Tayside Centre for General Practice, UK
Background: International asthma guidelines recommend proactive disease monitoring and treatment adjustment based on spirometry and symptoms. Airway inflammation may also be related to disease severity. Few data from primary care exist on whether any of these measures accurately reflect exacerbation rate.
Methods: Practice nurses prospectively gathered data from routine asthma clinics in 5 general practice surgeries on patient symptoms (Royal College of Physician’s (RCP) “Three Questions”), reliever use, spirometry, current maintenance pharmacotherapy, disease severity (British Thoracic Society (BTS) treatment step) and exhaled nitric oxide (FENO). Asthma exacerbation data (unscheduled health care contact and rescue oral corticosteroid therapy) for the 12 months prior and 3 months subsequent to the clinic visit were then obtained.
Results: 267 adult asthmatics (mean (SEM) age 51.6 (1.1); FEV1 86.3% (1.2) predicted) participated. Exacerbation rate for the 12 months prior to the clinic visit was positively correlated with dose of inhaled corticosteroid (ICS) (p<0.001), BTS guideline step (p<0.001), reliever use (p = 0.002) and RCP symptom score (p<0.001), but negatively correlated with FENO (p = 0.039). Patients on maintenance therapy at BTS treatment steps 2–5 had a significantly (p<0.05) lower FEV1 but also FENO than patients at step 1, whereas there was no difference for reliever use. Patients who exacerbated in the 3 months subsequent to their visit had no difference in reliever use, ICS dose, FENO, or FEV1 compared to those without an exacerbation. 7/60 patients who reported 2 or 3 RCP symptoms experienced a disease exacerbation in the subsequent 3 months compared with 6/207 who reported 0 or 1 symptom (p = 0.005). Subsequent logistic regression revealed that none of the recorded variables were significant predictors of impending asthma exacerbation after the clinic visit.
Conclusion: Although there are correlations between asthma exacerbation rate and maintenance ICS dose, reliever use, BTS treatment step and FENO, we found no variable that predicts subsequent exacerbation following a scheduled nurse review appointment in primary care.
THE CORRELATION BETWEEN EXHALED NITRIC OXIDE AND SPUTUM EOSINOPHIL COUNTS IN PATIENTS WITH AIRWAYS DISEASE
P. Haldar, D. Shaw, R. Siva, M. Berry, C. Brightling, R. Green, A. Wardlaw, I. Pavord. Institute for Lung Health, Glenfield Hospital, Leicester, UK
Background: Eosinophilic inflammation is predictive of steroid responsiveness in airways disease. The fractional exhaled nitric oxide (FeNO) correlates significantly with induced sputum eosinophil counts in asthma and may be a useful surrogate marker of eosinophilic airway inflammation in this population. Here we explore the strength of this correlation across different disease categories associated with eosinophilic inflammation: a group with mild to moderate asthma managed in primary care (PCA, n = 114); a group with refractory asthma managed in secondary care (RA, n = 84); a group with chronic obstructive pulmonary disease (COPD, n = 62) and a group with eosinophilic bronchitis (EB, n = 25).
Methods: Paired sputum eosinophil counts and FeNO at 50 ml/sec measured at the same time point was log transformed for each subject. The Pearson correlation coefficient (r) between log transformed variables was calculated independently in each disease group after controlling for atopic and current smoking status.
Results: Significant and comparable linear correlation was observed in the asthma subgroups (PCA: r = 0.41, p<0.001; RA: r = 0.40, p<0.001) but the correlation was absent in the other disease groups (EB: r = 0.31, p = 0.125; COPD: r = 0.096, p = 0.453). In COPD the correlation was significant in current smokers ((n = 20) r = 0.49, p = 0.042). We examined whether fixed airflow obstruction in RA identified a pathological process analogous to COPD that may lead to the observed dissociation between FeNO and eosinophils seen with COPD. Patients with RA and a post bronchodilator FEV1 <60% predicted (n = 30) shared the same correlation between FeNO and sputum eosinophils as other asthma patients (r = 0.42, p = 0.021).
Conclusion: The correlation between FeNO and eosinophilic inflammation varies in different diagnostic groups of airways disease. The reasons for this are not clear but suggest that disease specific pathological factors are important and support the consideration of current diagnostic labels in the clinical interpretation of FeNO.
A STUDY OF AIRWAY INFLAMMATION AND VIRAL INFECTION IN ACUTE SEVERE ASTHMA
A. V. Kamath1, W. R. Monteiro2, S. Mildenhall1, C. F. Ramsay1, O. P. Twentyman1, A. M. Wilson1, I. D. Pavord2, S. L. Johnston3, B. D. W. Harrison1.1Norfolk and Norwich University Hospital; 2Institute for Lung Health, Glenfield Hospital; 3National Heart and Lung Institute, Imperial College London, UK
Introduction: Virus infection is a common trigger for acute exacerbations of asthma. It is generally considered that this type of infection results in neutrophilic rather than eosinophilic airway inflammation. Sputum cell count has been used as a measure of airway inflammation in asthma. We set out to characterise the airway inflammation in patients with acute severe asthma and correlate the four patterns1 of inflammation with the presence of viral infections.
Methods: All patients admitted to a large acute general hospital between October 2004 and February 2006 with acute severe asthma were invited to participate. Patient demographics, history including recent symptoms of a “flu-like illness” and characteristics suggestive of poor treatment compliance2 were recorded. Sputum samples (spontaneous or induced) and nasopharyngeal aspirates obtained within 24 hours of admission were analysed for 9 viruses including human rhinovirus, respiratory syncytial virus and influenza, using RT- PCR. Sputum cell counts were performed and, based on cell counts, patients were classified as eosinophilic (≥1.9%), neutrophilic (>61%), eosinophilic and neutrophilic (≥1.9% and >61%) or paucigranulocytic (<1.9% and <61%). The characteristics between the various subgroups were compared using ANOVA and χ2 tests with p<0.05 being considered to be statistically significant.
Results: 92 patients consented to the study and the 69 patients who were able to provide sputum samples were recruited.
Conclusion: (1) Viral infection is not associated with any particular pattern of airway inflammation in patients with acute sever asthma. (2) Patients with eosinophilic airway inflammation are younger in comparison to the other subgroups but this was not statistically significant. (3) Patients with neutrophilic airway inflammation tend to be better compliant with treatment though this was not statistically significant.
1. Haldar P , Pavord ID. JACI 2007;119 :1043–52.
2. Smith J , et al. J Asthma 2005;42 :437–45.
EXHALED NO (FENO) CORRELATES TO SPUTUM EOSINOPHIL COUNT IN ACUTE SEVERE ASTHMA
A. V. Kamath1, W. R. Monteiro2, S. Mildenhall1, C. F. Ramsay1, O. P. Twentyman1, A. M. Wilson1, I. D. Pavord2, B. D. W. Harrison1. 1Norfolk and Norwich University Hospital; 2Institute for Lung Health, Glenfield Hospital, UK
Introduction: It has been suggested that exhaled nitric oxide (FENO) be used to guide treatment in asthma. It has been shown to correlate with sputum eosinophil counts in patients with stable asthma. In a preliminary study in patients with acute severe asthma we investigated the relationship between FENO and sputum eosinophil and neutrophil counts.
Methods: Twenty-one patients admitted to a large acute general hospital with acute severe asthma between March 2005 and February 2006 were included in the study. Sputum samples (spontaneous or induced) and FENO were obtained within 24 hours of admission. Sputum was processed for differential cell counts and FENO was measured at a flow rate of 50 ml/s (NIOX, Aerocrine, Sweden). The Spearman rank test was used to find correlations between (1) FENO and sputum eosinophils (2) FENO and sputum neutrophils.
Results: A total of 21 patients (F = 14) produced sputum and performed acceptable FENO measurements. The mean age of patients was 43.7 years (SD 14.4), the median steroid dose was 200 μg BDP (range 0–4000 μg), and 5 were current smokers. The median sputum eosinophil and neutrophil counts were 3% (0–58)) and 60% (30–97), respectively. There was a significant correlation between FENO and sputum eosinophils (r = 0.667, p = 0.001) but not between FENO and sputum neutrophils (r = −0.209, p = 0.362).
Conclusion: This is the first study assessing the correlation of FENO with sputum inflammatory cells in acute severe asthma. Although the numbers are small the results are consistent with those in chronic stable asthma. These results suggest FENO may be used as a marker of eosinophilic airway inflammation in acute asthma exacerbations.
ATOPY AND SARCOIDOSIS: A PILOT STUDY SHOWING CORRELATION WITH DISEASE STAGE
A. K. Khan1, A. W. O'Regan1, J. S. Berman2, D. A. Serlin2. 1University College Hospital, Galway, ROI; 2Boston University School of Medicine, USA
Background: The pathogenesis of chronic lung fibrosis in sarcoidosis is poorly understood and there are no reliable markers of progressive disease. There is evidence that airway epithelium regulates the pathogenesis of lung fibrosis in other diseases. Airways disease has been associated with chronic pulmonary sarcoidosis and we have previously reported a significant increase in rhinitis and airway obstruction in sarcoid patients with chronic lung disease. We hypothesised that atopy may be associated with nasal symptoms and chronic disease in sarcoidosis.
Methods: In an Irish and American cohort of patients with sarcoidosis we determined the prevalence of nasal allergic symptoms, signs, and atopy using a disease specific questionnaire, physical exam, and both skin and RAST testing. The study was IRB approved.
Results: 50 patients were studied. 25% were African American; 75% Caucasian and 45% were male. Disease stage was stage 0–1: 54%; stage 2–3: 30%; stage 4: 16%. Nasal symptoms were present in 35% and atopy in 38%. There was a good correlation between nasal symptoms and atopic phenotype. Atopy was significantly associated with the American cohort, African American race and stage 4 (fibrotic) lung disease (atopy was present in 30% stage 0–1; 40% stage 2–3, and 63% stage 4).
Conclusion: Contrary to the Th1-Th2 paradigm, these studies show that atopy, a Th2-mediated immune response, can exist in the Th1-mediated disease of sarcoidosis. The data suggest that there may be an association between atopy and progressive or fibrotic lung disease, particularly in the African American cohort. Further studies are required to better define this association.
TNF-ALPHA ANTAGONISM USING ETANERCEPT REDUCES SYSTEMIC INFLAMMATION AND SPUTUM MACROPHAGES IN SEVERE ASTHMA
J. B. Morjaria1, A. J. Chauhan2, K. S. Babu1, P. Vijayanand1, D. Bagmane1, R. Djukanovic1, D. E. Davies1, S. T. Holgate1. 1University of Southampton; 2Queen Alexandra Hospital, UK
Rationale: TNF-α has been implicated as playing a pivotal role in the inflammatory process in corticosteroid-refractory asthma. Recent studies have reported that antagonising TNF-α using a soluble TNF-α receptor, etanercept, in severe asthmatics, GINA stage IV, resulted in a significant improvements in asthma control and quality of life as well as bronchial hyperresponsiveness. To investigate if there were any systemic responses to TNF-α blockade, we assessed serum albumin, C reactive protein (CRP) and cytokines in 36 subjects (18 in group) before and after 12 weeks of treatment with etanercept or placebo in a randomised-controlled trial. We also assessed sputum inflammatory cells and supernatant cytokines in 14 subjects.
Methods: CRP and albumin was measured in the Southampton General Hospital Laboratories. Sputum was processed using a standardised protocol and differential cell counts were performed after staining with Diff quick. Serum and sputum supernatants were analysed for TNF-α using ELISA, and IL-6 and IL-1ݠusing a cytokine bead array with flow cytometry.
Results: There was a significant reduction in the sputum macrophages following treatment with etanercept (p = 0.046); however, this was not observed in the neutrophil and eosinophil counts. We observed a significant reduction in serum CRP (p = 0.029) and a significant increase in serum albumin (p = 0.022) as a result of treatment with etanercept as opposed to placebo, demonstrating reduction in systemic inflammation. As observed in other studies using etanercept, levels of TNF-α in serum in the etanercept group showed a marked increase compared to placebo (p<0.0001). Of note, in both treatments groups, sputum IL-6 and IL-1ݠwere elevated and decreased with etanercept but not significantly.
Conclusion: The significant reduction in systemic inflammation as measured by a significant reduction in serum CRP and improvement in serum albumin confirms the view that there is a systemic inflammatory component to asthma. Furthermore, TNF-α, a pleotropic regulatory cytokine, may have critical role in corticosteroid-refractory asthma and antagonising it may be novel treatment in this subgroup of patients in whom there is an unmet clinical need.
THE PAPER RECYCLING INDUSTRY, HYDROXYLAMINE AND OCCUPATIONAL ASTHMA: TWO CASE REPORTS
S. Tran1, J. Hoyle2, R. M. Niven1, H. C. Francis1. 1South Manchester University Hospital; 2North Manchester General Hospital, UK
Introduction: Occupational disease linked to the paper recycling industry has not as of yet been well documented. No previously confirmed formal diagnosis of occupational asthma caused by hydroxylamine has been made.
Methods and results: We have assessed and performed occupational assessment of 8 workers involved in this industry. Two of these original 8 assessed workers were later diagnosed with occupational asthma (OA). Both workers developed their respiratory symptoms within 2 years of the first use of the chemical hydroxylamine as part of the “de-inking” process (it was used as a substitute for glutaraldehyde on risk grounds although no prior cases of OA had been found, while glutaraldehyde was used for this process). The 2 positive cases had worked at the same plant for 11 and 20 years, respectively. Both gave histories of work related wheeze, shortness of breath and cough. Both cases performed OASYS peak flow records over a three week period and had OASYS II index of 2.85 and 2.67 respectively. Both cases were redeployed on site to non-exposed areas and subsequently demonstrated improvement in bronchial reactivity. Case 1: diagnosis PC20 = 1.25 μg/ml; 12 months post cessation of exposure 4.5 μg/ml; Case 2: diagnosis PC20 6 μg/ml; 6 months post cessation of exposure >8.0 μg/ml). Case 2 subsequently consented to and underwent a blinded, placebo controlled occupational challenge using hydroxylamine by first painting on to a board, then by aerosol exposure within the challenge room (see fig) demonstrates the late asthmatic reaction occurring on the high exposure hydroxylamine challenge (aerosolised). Since the first 2 cases were found 1 of 2 further referrals from the same industry site has also been provisionally diagnosed with OA.
Conclusion: We believe these are the first 2 confirmed cases of OA caused by hydroxylamine in the paper recycling industry.

THE OUTCOME OF OCCUPATIONAL ASTHMA WITH CONTINUING EXPOSURE: A SYSTEMATIC REVIEW
M. Munshi, J. Szram, S. Macneill, P. Cullinan. NHLI Imperial and Royal Brompton Hospital, London, UK
Background: We recently published a systematic review of the outcome of occupational asthma (OA) following cessation of exposure to the causative agent. Here we report a similar review of studies of patients whose exposure continued after diagnosis.
Aims and methods: Original papers documenting symptomatic and physiological outcomes in patients with OA were identified through electronic searches of Medline and Embase (n = 17 studies, 699 patients). 16 studies recruited their patients from specialist clinics. 16 reported symptomatic outcomes, while 11 and nine respectively reported changes in FEV1 and NSBHR.
Results: Only one of 699 patients reported complete symptomatic recovery. Improvement in symptoms was reported by between 0% and 63% of patients with a pooled estimate of 18.4% (95% CI 9.5 to 32.6). No change in symptoms was reported by 0% to 100% of patients with a pooled estimate of 22.1% (95% CI 5.8 to 56.4). Deterioration in symptoms over the period of follow up was reported by 0% to 100% with a pooled estimate of 58.3% (95% CI 27.3 to 83.9). In 92% (n = 412) of patients there was a decline in FEV1 over the period of study; and in 77% an increase in NSBHR. There were too few studies for a detailed examination of the predictors of outcome but patients with persistent exposure to diisocyanates and those with a longer duration of exposure appeared to fare worse.
Conclusion: Systematic reviews of observational studies need to be interpreted with care, but these findings tend to confirm that patients with OA whose exposure to the causative agent persists have a worse prognosis than those in whom further exposure is avoided. The issue of outcomes with reduced, rather than abolished, exposure remains both important and contentious.
THE EFFECT OF WELDING ON LUNG FUNCTION DECLINE AND RESPIRATORY SYMPTOMS: A SYSTEMATIC REVIEW
S. J. Upchurch1, J. Szram1, M. Cosgrove2, P. Cullinan1. 1Imperial College School of Medicine (NHLI); 2The Welding Institute, UK
Background: There remains controversy over the relationship between welding fume exposure and airflow obstruction. Cross-sectional surveys of employees in the welding industry may be subject to important survival biases and medical advisors would benefit from accurate information regarding likely decline in lung function attributable to their work.
Methods: We undertook a systematic review of published literature describing longitudinal changes in lung function and/or symptoms among welders. Through a full search of electronic and bibliographic sources we identified original cohort studies documenting changes in lung function (7 studies, 1695 subjects) or respiratory symptom (3 studies, 391 subjects). We undertook meta-analysis using random effects methods.
Results: The median duration of follow up was 4.5 years for studies of lung function and 2 years for studies of respiratory symptoms. Reported annual decline in FEV1 for welders varied from −272 ml to −0.1 ml with a pooled estimate of −29.1 ml/year (95% CI −57.8 to −0.4); the equivalent figure for non-welders in the same studies was −11.1 ml (95% CI −24.5 to 2.3) Among welders the overall estimate of FEV1 decline was greater in smokers (−31.7 ml/year (95% CI −61.8 to −1.6)) than in non-smokers (−10.7 ml/year (95% CI −29.1 to 7.7)). The findings for incident respiratory symptoms were inconsistent; it was not possible to calculate a pooled estimate of change. In between-study comparisons we found no clear patterns of improvement relating to total duration of exposure or follow-up.
Conclusion: The interpretation of systematic reviews of observational studies is often difficult; and the longitudinal evidence-base for this topic is sparse. These findings, however, suggest that any increase in FEV1 decline among welders is confined to those who smoke. Clinicians and epidemiologists with an interest in welding should consider embarking on a collaborative and carefully standardised study of the respiratory health effects of this common occupational exposure.
ECONOMIC EVALUATION OF A NEW AIRWAY INFLAMMATION MONITOR IN THE DIAGNOSIS AND MANAGEMENT OF ASTHMA IN THE UK
J. Berg, P. Lindgren. i3 Innovus, Stockholm, Sweden
Objectives: Fractional exhaled nitric oxide (FENO) is a measure for the airway inflammation underlying asthma, which can be used for both diagnosis and monitoring the effect of anti-inflammatory treatment. The objective of this study was to assess the cost-effectiveness of NIOX MINO® Airway Inflammation Monitor, a portable non-invasive device for measuring the level of FENO, in asthma diagnosis and management.
Methods: Two decision trees were constructed that capture the different alternatives and consequences in asthma diagnosis and management. Reflecting available clinical data on diagnostic precision, FENO measurement was compared against standard diagnostics, including spirometry, reversibility testing, bronchoprovocation and sputum eosinophil count. The impact of asthma management with FENO measurement on inhaled steroid use, exacerbations and hospitalisations was compared against standard guidelines (spirometry) over a 1 year timeframe. A UK payer perspective was chosen, focusing on direct medical costs taken from published sources in 2006. Effectiveness was measured in quality-adjusted life-years (QALYs).
Results: Asthma diagnosis based on FENO measurement using NIOX MINO results in a cost of £29 per patient, including the cost of false diagnoses, compared to £39 for standard diagnostics. If FENO measurement is conducted in addition to standard tests, the incremental cost would be £16 per patient. Asthma management with FENO measurement instead of standard guidelines is a dominant strategy. In mild to severe patients, it results in cost-savings of £96 per patient and year and 0.06 QALYs gained. In a more severe population, management with NIOX MINO would save costs of £313 per patient and lead to 0.004 QALYs gained.
Conclusion: Asthma diagnosis based on FENO measurement with NIOX MINO alone is less costly and more accurate than standard diagnostic methods, while the addition of FENO measurement to spirometry increases costs marginally. The use of FENO measurement in treatment decisions is less costly than asthma management based on standard guidelines, while providing the same health benefits.
SPUTUM GRANULOCYTE CELL TYPE DOES NOT PREDICT RATE OF RECOVERY OF PEAK EXPIRATORY FLOW IN ACUTE SEVERE ASTHMA
A. V. Kamath1, W. R. Monteiro2, S. Mildenhall1, C. F. Ramsay1, O. P. Twentyman1, A. M. Wilson1, I. D. Pavord2, B. D. W. Harrison1. 1Norfolk and Norwich University Hospital; 2Institute for Lung Health, Glenfield Hospital, UK
Introduction: Acute severe asthma is usually characterised by airway inflammation and associated with a drop in peak expiratory flow (PEF). Sputum cell counts and PEF have been used to guide treatment response in patients with chronic asthma. The aim of this study, in acute severe asthma, was to determine whether speed of recovery, assessed by increase in PEF during the first 24 hours of admission was associated with any particular pattern of granulocytic inflammation.
Methods: Forty-three patients admitted to a large acute general hospital between October 2004 and February 2006 with acute severe asthma were included. Patient demographics, history and PEF on admission and after 24 hours were recorded. Admission sputum cell counts were analysed and patients were classified based on the cut points recommended by Haldar et al: eosinophilic (⩾1.9%), neutrophilic (>61%), eosinophilic and neutrophilic (⩾1.9% and >61%), and paucigranulocytic (<1.9% and <61%). PEF measured on admission and 24 hours post admission was expressed as a percentage of the patients’ best or predicted. The 4 subgroups were compared using ANOVA and p<0.05 was considered to be statistically significant.
Results: See table.
Conclusion: Although patients with eosinophilic inflammation had lower PEF on admission this was not statistically significant. The speed of improvement of PEF in the first 24 hours of acute severe asthma is the same irrespective of the inflammatory cell pattern.
1. Haldar P , Pavord ID. J Allergy Clin Immunology 2007;119 :1043–52.
Lung cancer: investigation and management
ANTHRACOFIBROSIS: A MIMIC OF LUNG CANCER. IS IT THE PMF OF THE AIRWAYS?
G. Wynn, P. M. Turkington, B. R. O’Driscoll. Hope Hospital, Salford, UK
Introduction: Anthracosis is black pigmentation of the bronchial mucosa, commonly found in former coal miners. Athracofibrosis describes inflammatory bronchial stenosis with anthracotic mucosa, usually in Asian patients with previous tuberculosis. Anthracofibrosis has not been previously reported in European subjects.
Methods: Seven patients (5 male) were found to have anthracofibrosis at bronchoscopy in Salford between 1993 and 2006.
Results: Five patients were UK Caucasians, one was Yemeni and one Pakistani. Mean age was 72.4 years (range 66–81). One Asian female patient had previous spinal tuberculosis. The other female had calcified lymph nodes shown on CT. None were current smokers, three (43%) had previously smoked cigarettes. Five patients give a history of asthma and/or had an obstructive pattern of respiratory function tests. One patient had restrictive lung disease. Three had worked as tilers or in tile making factories and three had worked as coal miners. Two patients had persistent symptoms after episodes of pneumonia, all of the others had breathlessness and most had cough. All patients had findings on the chest x-ray and/or CT scan suggestive of lung cancer usually segmental collapse or hilar opacity. Bronchoscopy revealed dark, pigmented areas forming hard raised plaques or bronchial stenosis. Biopsy or cytology showed dust-laden macrophages in five patients. Dense acellular collagenous fibrotic material was also seen. In all but one patient the pigmented lesions were associated with stenosis and/or occlusion of the affected airways. Six of seven patients remained clinically and radiologically stable throughout their follow up period (one to thirteen years).
Conclusion: Our study in one district would indicate an incidence of about 120 cases per annum in the UK but there have been no previous UK case reports. Previous (Asian) case series suggested a link to tuberculosis but six of our seven patients had an occupational history of coal or other dust exposure suggesting that anthracofibrosis in European subjects may be an extreme manifestation of the “coal tattoos” or bronchial anthracosis, common among coal miners. Anthracofibrosis may be a previously unrecognised complication of anthracotic lung diseases.
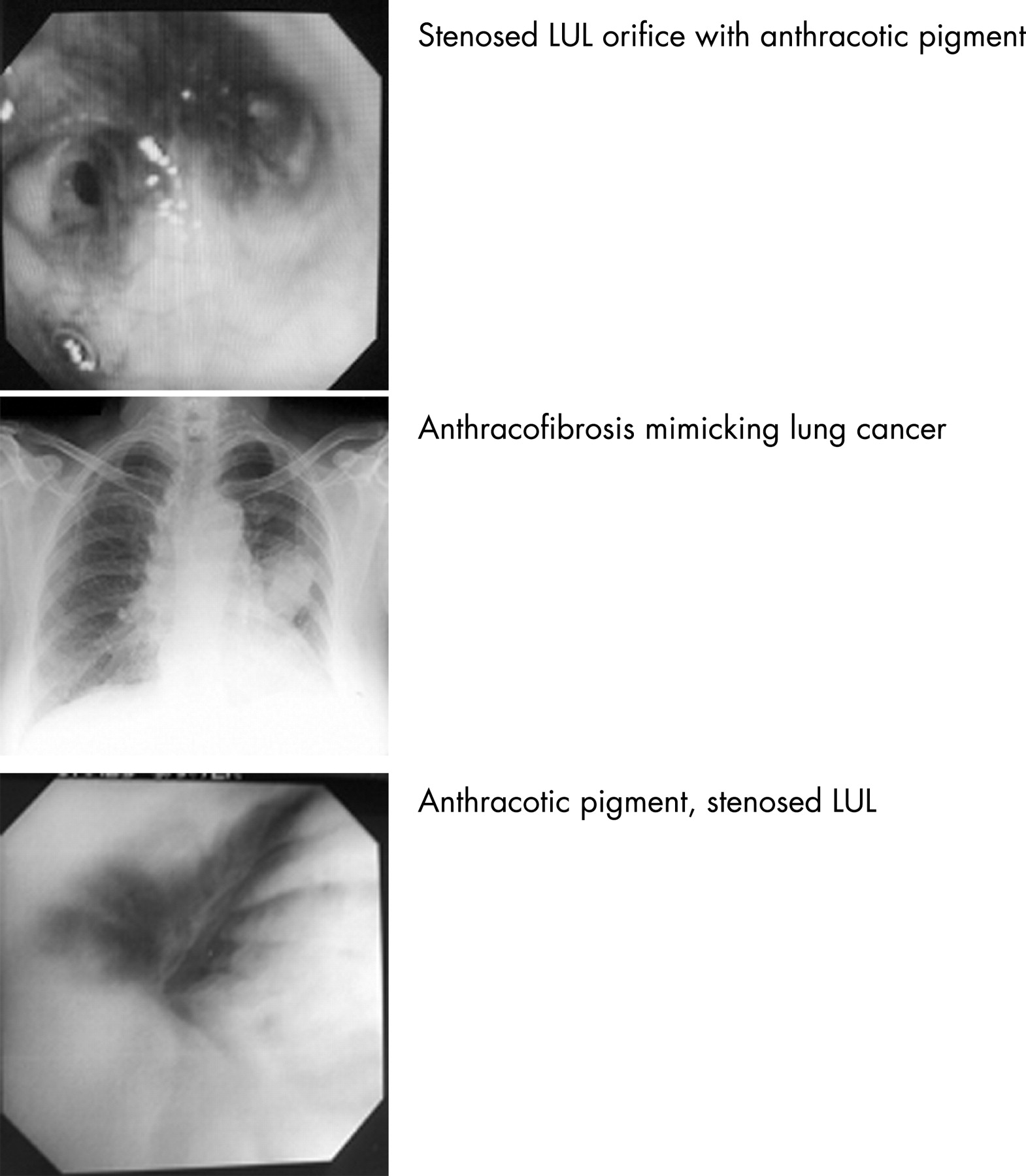
OUTCOME FOR PATIENTS WITH NEGATIVE FDG-PET SCANS
N. Sinnott, M. Asim, S. Durairaj, M. J. Walshaw, M. J. Ledson. The Cardiothoracic Centre-Liverpool, UK
Introduction: FDG-PET scanning is a relatively new technique, where moderate or high tracer uptake can indicate primary lung tumours and metastases. However, in some patients with solitary nodules the scan may be negative, and the subsequent diagnostic pathway and ultimate outcome is unclear. To explore this, we followed the clinical course of a group of such patients.
Methods: We obtained the clinical records of all 33 patients (mean age 68 years (range 45–89), mean PS = 1 (0–3), mean smoking history 35 pack years (0–120), mean FEV1 1.60 litres (0.54–3.82)) with suspected lung cancer (chest radiology lesion size mean 2.3 cm (0.7–4.0)) between March 2005 and July 2006 at our large lung cancer unit, where the FDG-PET scan was classed as “negative” (SUV <2.5 or “low/no probability of malignancy” on the radiologist’s report) (29% of the total). Only 3 cases had mediastinal lymphadenopathy (2 borderline). Bronchoscopy was unhelpful in all cases.
Results: Six underwent thoracotomy based on the MDT’s suspicion of lung cancer: of these 3 had adenocarcinoma, 1 squamous cell carcinoma, 1 sarcoidosis, and 1 folded lung. A further 3 underwent percutaneous CT-guided lung biopsy (1 adenocarcinoma). Of the 26 patients (79%) still undiagnosed, 2 DNA’d from follow-up (at 3 and 12 months), 16 remain under follow-up (mean time 20.3 months (range 12 to 34)) and 8 have been discharged (mean time to discharge 7.8 months (range 1 to 18)): of these 3 had “old” nodules on previous radiological review, 1 had a lesion which cleared, 1 had an azygous vein on vascular screening, and 3 were deemed to have “benign” lesions. To date, none of the patients still under follow-up have developed cancerous change in their lesions, although the clinical teams are still suspicious of malignancy.
Conclusion: In the small proportion of patients presenting to our lung cancer unit with suspected malignancy where FDG-PET scans were “negative”, 15% had an underlying lung cancer. However, in every case the cancer was diagnosed while the patient was still in the initial diagnostic pathway. From our data, it appears that in the remaining patients, ongoing surveillance may give only a low yield of cancer.
PROGNOSTIC FACTORS FOR LONG-TERM SURVIVAL AFTER PULMONARY METASTASECTOMY IN SARCOMA PATIENTS: A 12 YEAR EXPERIENCE
S. Letafat1, E. Belcher2, S. Sathianandan1, S. Jordan2, P. Goldstraw2. 1Imperial College; 2Royal Brompton Hospital, London, UK
Background: In sarcoma patients pulmonary metastases are common and the lung is the most frequent site of relapse after curative treatment of the primary tumour. Although prolonged survival after pulmonary metastasectomy for sarcoma is well documented, the prognostic factors which influence survival are not known.
Objective: The aims of the study were to evaluate the long-term survival in sarcoma patients undergoing pulmonary metastasectomy and to identify factors predicting outcome.
Methods: This retrospective study assessed 157 metastasectomy procedures performed on 105 consecutive patients from 1995 to 2007. Of these patients, 30 underwent more than one metastasectomy. We examined the impact of age, gender, sarcoma type, disease-free interval (DFI), number and distribution of metastases, prior metastasectomy and the presence of a pleural effusion on survival in these patients. Kaplan–Meier log-rank test and the Cox regression model were used to compare survival in the different subgroups.
Results: Perioperative mortality was 0%. Overall survival was 51.7% at 5 years (95% CI 40.8% to 61.6%) and 46.7% at 10 years (95% CI: 34.8% to 57.7%). DFI greater than 12 months (HR = 0.447, 95% CI 0.247 to 0.809; p = 0.01) and repeated metastasectomy (HR = 0.18, 95% CI 0.07 to 0.44; p<0.001) were statistically significant predictors of survival. There was no significant survival difference between patients with solitary versus multiple metastases (p = 0.40). Furthermore, the presence of bilateral pulmonary metastases or pleural effusion, whether haemorrhagic or not, did not affect survival.
Conclusion: Surgical resection of sarcomatous pulmonary metastases confers good long term survival with a low operative mortality. Patients with a DFI of 12 months or longer have a significantly better prognosis. Improved prognosis in patients who underwent repeated metastasectomy may be related to a selection bias. This, however, highlights the importance of postoperative surveillance and repeated pulmonary metastasectomy in selected patients to achieve long-term survival. The presence of a pleural effusion, especially when haemorrhagic, causes concern as to the possibility of pleural dissemination. Our study has for the first time shown that this is not a negative prognostic factor and should not be considered a contraindication for pulmonary metastasectomy. Moreover, multiple or bilateral pulmonary metastases do not negatively impact on survival and, therefore, should not preclude surgery.
PROGNOSTIC IMPLICATIONS OF IMPROVED CT DETECTION OF PULMONARY METASTASES IN PATIENTS UNDERGOING PULMONARY METASTASECTOMY
S. Sathianandan1, E. Belcher2, S. Letafat1, E. Lim2, S. Jordan2, P. Goldstraw2. 1Imperial College; 2Royal Brompton Hospital, London, UK
Background: Pulmonary metastasectomy is an established treatment modality for selected patients with pulmonary metastases. Computed Tomography (CT) remains the mainstay for preoperative assessment and surgical planning while intraoperative palpation is the gold standard for achieving complete resection.
Aims: The aims of this study are to document the incidence of unexpected pulmonary nodules (those undetected on CT but detected during intraoperative palpation) in patients undergoing pulmonary metastasectomy over a 12 year period and through 2 different CT scanners (continuous and spiral), to compare CT with intraoperative palpation and determine the impact of unexpected nodules on survival.
Methods: This was a retrospective study using medical records of patients undergoing thoracic surgery. The mean proportion of CT nodules against number palpated was documented over 2 time frames of CT technology. Agreement was compared using Bland and Altman plots with regression. Cox proportional hazards regression was used to estimate the impact of finding unexpected nodules on survival.
Results: Between 1 January 1995 and 31 March 2007, 331 pulmonary metastasectomies were carried out on 239 patients. The overall 1 and 5 year survival was 84% (95% CI 79% to 89%) and 56% (95% CI 49% to 64%), respectively. The mean proportion of nodules predicted by CT versus found on intraoperative palpation was 81% versus 88% (p = 0.05) for continuous and spiral CT, respectively. CT was in perfect agreement with operative findings in 56%, underestimated number of nodules in 39% and overestimated in 5%. On average, intraoperative palpation detected 1.15 nodules more than CT. The disparity increased with the number of nodules predicted preoperatively by CT (regression for slope parameter of Bland and Altman plot was 0.42 (95% CI 0.37 to 0.49; p<0.001). The survival of patients with unexpected nodules was poorer with a hazard ratio of 1.34 (95% CI 0.85 to 2.13), however this did not achieve statistical significance (p = 0.21).
Conclusion: Our study suggests that unexpected metastases are common, the proportion of nodules detected (CT over intraoperative palpation) increased with improvements in CT. Discrepancy between the numbers found and predicted did not affect survival after complete resection suggesting that the imprecision of CT can be overcome by careful intraoperative palpation, this becoming increasingly relevant as number of nodules predicted increases.
FOLLOW-UP OF ISOLATED PULMONARY NODULES DISCOVERED BY CT SCAN
J. F. Greenwood1, Z. H. Hoo2, R. M. Angus1. 1University Hospital Aintree; 2University of Edinburgh Medical School, UK
Introduction: The follow-up of pulmonary nodules (PN) found incidentally at computed tomography (CT) scanning creates a major workload for the multidisciplinary team. The Fleischner Society for Chest Diagnosis advocate serial interval CT imaging dependent on initial nodule size, and have issued guidelines for such follow-up (Radiology 2005;237 :395–400). Previously published series have shown an eventual cancer rate of 1–3% for all PN, but less than 1% when the initial PN size was smaller than 5 mm. We report the results of our PN follow-up over a 3 year period.
Method and results: We retrospectively examined all CT chest reports containing the word “nodule” for 3 years from July 2003. From a total of 1304 patient records, and following exclusion of patients with known metastatic disease, new PN were found incidentally in 217 patients. All were assumed to be high-risk for subsequent development of malignancy. 177 patients (81%) underwent follow-up CT scanning, with an interval range of 6 weeks to 27 months from the index scan. The need for interval imaging was stated in 174 reports, and a suggested time to next scan was given in 129. Initial follow-up was actually carried out according to Fleischner Society guidelines in only 16%, the majority of variances being scanning earlier than recommended (63%). A total of 600 CT scans (mean 2.7 per patient) were performed. CT follow-up was deemed complete after 2 years, or if the report stated “no further follow-up required”. A further CT scan was not performed for the reasons shown in table 1.
The outcome is known in 211 patients (97%). The nodule discovered at initial CT scan was subsequently found to be malignant in 15 patients (7%); in these cases the initial PN was 5 mm or less in size in 5 patients, 2.3% of the total cohort. Table 2 shows ultimate diagnosis.
Conclusion: Our lung cancer diagnosis rate from follow-up of isolated PN was 3.7%. This is slightly higher than previously reported figures, and is reflective of our high regional incidence of bronchial carcinoma. The diagnosis rate of other metastatic malignancies is also significant, and these all occurred some time following definitive treatment of the distant primary tumour. Although compliance with the Fleischner Society guidelines within the audit period was low, clinical and radiological measures were effective enough to ensure that only 2 patients did not get follow-up of some sort. Both of these patients are now being recalled. However, application of the guidelines would reduce the number of unnecessarily early scans. While the follow-up of patients with incidentally discovered pulmonary nodules may seem onerous at times, our data confirm that the diagnostic yield for malignancy is significant and important in the high-risk population.
PREOPERATIVE FEV <2 L DOES NOT ACCURATELY PREDICT THE DEVELOPMENT OF COMPLICATIONS FOLLOWING A PNEUMONECTOMY
D. M. Cook1, A. Pearce2, F. Gao1. 1Birmingham Heartlands Hospital; 2Guys Hospital, London, UK
Introduction: The UK Pneumonectomy Outcome Study is the largest ever prospective study into the risk factors that predict poor outcomes following a pneumonectomy.
Methods: Data from 315 pneumonectomies was submitted from 23 thoracic surgical centres across the UK during the calendar year 2005. All adult patients (>18 years of age) undergoing a pneumonectomy for lung cancer during 2005 were eligible for the study.
Results: A major complication was defined as: death, unplanned ICU admission, inotrope requirement, requirement for further surgery, dialysis or a clinically significant arrhythmia. The major complication rate was 32.1% (n = 315). The mean FEV1 was 2.25 (0.56) litres in the patients having a major complication (n = 100) and 2.11 (0.64) litres in the patients without a major complication (n = 212). An FEV1 <2 litres was not associated with a significantly increased rate of major complications (OR = 1.38, CI 0.85 to 2.24; p = 0.2). A predicted postoperative FEV1 <40% was also not associated with a significantly increased rate of major complications (OR = 1.32, CI 0.8 to 2.2; p = 0.3). The mean predicted TLCO was not significantly different in the group having a major complication 68.8% (16.4) compared to the group not having a major complication 72.5% (17.8). A preoperative FEV1 <60% predicted was associated with an increased rate of major complications (OR = 2.0, CI 1.007 to 3.96; p = 0.06).
Conclusion: A preoperative FEV1 <2 litres or predicted postoperative FEV1 <40% did not predict major complications following a pneumonectomy. The best predictors of major complications were a preoperative FEV1 <60% and a predicted postoperative FEV1 ⩽30%. The BTS guidelines on spirometric data do not predict accurately the development of complications following a pneumonectomy.
DOES THE USE OF BRONCHOSCOPY IN THE INVESTIGATION OF HAEMOPTYSIS IMPROVE THE DIAGNOSIS OF EARLY LUNG CANCER?
E. K. Sage, R. A. M. Breen. St Thomas' Hospital, London, UK
Introduction: Haemoptysis is a non-specific symptom that is often seen in clinical practice. Although it may be indicative of underlying pathology, in up to 50% of cases no cause can be found. Detection of early lung cancers is a priority and haemoptysis is often highlighted as a key symptom. Its presence is a criterion for referral under the 2-week wait policy even in the presence of a normal or non-specifically abnormal chest radiograph. Often such cases are investigated by bronchoscopy, despite previous work suggesting a low incidence of lung cancer (5–6%). We wondered whether the introduction of the 2-week wait policy had increased the proportion of early tumours observed and so had improved the utility of bronchoscopy in this area.
Methods: Patients being investigated for haemoptysis at a London teaching hospital between 2003 and July 2007 were identified from bronchoscopy records. Chest radiographs for each patient were reviewed and those where an obvious cause for haemoptysis had been observed were excluded. Computerised hospital records were used to identify pathological diagnoses at time of bronchoscopy and subsequent presentations.
Results: During the study period 1618 bronchoscopies were performed of which 113 (7%) were for haemoptysis with no abnormality on chest radiograph (77/113 (68%)) or with non-specific abnormalities (36/113 (32%)). The median age of this group was 55 years (range: 21–87). Malignancy was diagnosed in 0/113 (0%) and no diagnoses of malignancy have been made during median follow-up of 29 months (range: 1–60). Possible non-malignant diagnoses were made in 17/113 (15%). These were bacterial infection in 11/113 (10%); TB in 2/113 (2%); MAI in 1/113 (1%); fungal infection in 3/113 (3%).
Conclusion: Our findings suggest that the diagnostic yield of bronchoscopy in investigating patients with haemoptysis but normal or non-specifically abnormal chest radiographs remains low in the era of the 2 week wait referral policy. These data do not support haemoptysis alone being an indication for urgent referral.
LUNG CANCER BRONCHOSCOPY WITH NO VISIBLE TUMOUR: IMPACT OF TRANSBRONCHIAL NEEDLE ASPIRATION
C. M. R. Thomas, M. Bafadhel, M. Slade. Churchill Hospital
Transbronchial needle aspiration (TBNA) is increasingly used in flexible bronchoscopy (FB), in particular for its value in lung cancer staging. Current literature shows diagnostic yields of TBNA in non-visible tumour to be in the range of 38% (BTS guidelines) up to 87% (data on peribronchial disease, Chest 2005). In our centre, TBNA was first introduced as a diagnostic and staging technique in 2002, with its use becoming routine in early 2003.
Methods: Continuous, prospective audit of bronchoscopy data has been in place since 2001, with data from 2000 available from retrospective case note review. We reviewed bronchoscopy data for suspected cancer, dividing it for analysis into 2000–2002 (pre-routine TBNA use), 2003–2004 and 2005–2006. Two post-2002 periods were studied because previous analysis of TBNA performance had demonstrated an increasing diagnostic yield over the period 2003–2006.
Results: There was no significant impact upon diagnostic yield from the addition of TBNA to standard diagnostic modalities (washings, brushings, biopsies) where tumour was visible endobronchially (p(χ2) = 0.35). In contrast, in non-visible tumour, TBNA had a significant impact (p(χ2) = 5×10−8). The table shows the non-visible tumour data on both the overall diagnostic yield across the time period studied, and specifically, the impact of TBNA on the diagnostic yield of the bronchoscopies.
Conclusion: The technique of TBNA is known to have a learning curve and this is reflected in the data above. There is clear evidence of improved diagnostic yield in non-visible tumour bronchoscopies between 2002 and 2006 which is not explained by changes in the availability of CT scans pre-bronchoscopy. The TBNA data shows a steady increase in positive yield correlating with overall increase in diagnostic yield. In particular, it can be seen in 2005–2006, a positive TBNA result accounted for the diagnosis in over half of all FB performed. TBNA is well recognised as an important modality for the staging of lung cancer, but our data also shows its importance as a diagnostic modality, in particular in cases with non-visible tumour.
COMPARATIVE YIELD OF TRANSBRONCHIAL NEEDLE ASPIRATION (CONVENTIONAL AND ENDOBRONCHIAL ULTRASOUND GUIDED) AND PET-CT IN THE EVALUATION OF MEDIASTINAL MALIGNANCY
W. L. Williams, R. Naseer, J. Mills, J. Edwards, J. Howells, M. Munavvar. Lancashire Teaching NHS Foundation Trust, UK
Introduction: Mediastinal staging of lung cancer is of importance because it helps determine prognosis and guide treatment options for both operable and inoperable lung cancers. Conventional transbronchial needle aspiration (cTBNA) has been used as an adjunct to imaging such as CT and PET for many years to determine mediastinal staging. The diagnostic yield of cTBNA can vary between 20–89% (Herth F et al. Chest 2004;125 :322–5). Over the last 10 years endobronchial ultrasound (EBUS) has been developed and is being used to obtain EBUS guided TBNAs. This study looks at whether cTBNA versus EBUS guided TBNA concurs with other investigations (CT and PET, bronchial washings ± brushings).
Methods: We performed a retrospective analysis of 48 patients in the respiratory department of a teaching hospital. Patients had undergone either cTBNA and/or EBUS guided TBNA between March 2006 and June 2007 in the endoscopy suite, performed by a single operator (MM). 42 of the patients had also undergone bronchial washings and/or brushings. All 48 had some form of imaging modality (PET-CT, PET or both). The cytology results were analysed for all patients by the same histopathologist (JE). All patients were discussed at the lung MDT meeting and a definitive diagnosis was taken to be the outcome of the meeting. All other results obtained were compared with the definitive diagnosis. A further analysis was performed, looking at diagnostic yield. A positive diagnostic yield was taken as a correlation between the MDT outcome and the cytology diagnoses (bronchial washings and/or brushings; cTBNA; EBUS guided TBNA).
Results: 42 people had bronchial washings and/or brushings (mean age 66 years; 27 men and 15 women); 27 had cTBNA (mean age 65 years; 18 men and 9 women) and 40 people had EBUS guided TBNA (mean age 65 years; 27 men and 13 women).
Conclusion: EBUS guided TBNA targets smaller lymph nodes in more difficult to reach locations than cTBNA is capable of. Smaller lymph nodes are more difficult to identify and in the early stages of malignancy may contain few malignant cells, making sampling and cytological diagnosis difficult (Herth F et al. Eur Respir J 2006;28 :910–4). Fifteen EBUS-TBNA specimens received a pathology report of non-malignant but based upon the results of other investigations, were concluded to be malignant. Therefore, no technique should be used in isolation as these malignant cases were reported as such by bronchial washings and/or brushings and one was confirmed further by cTBNA. Diagnostic yield of cTBNA varies greatly (from 20–89%) which may be owing to operator experience, tumour size and location (Herth F et al. Chest 2004;125 :322–5). This study has demonstrated a high diagnostic yield from both cTBNA and EBUS guided TBNA. The excellent results obtained by both techniques have reduced the need for more invasive procedures in order to gain a diagnosis, which has in turn, reduced the risk to patients, and overall, helped reduce costs.
INTERVENTIONAL FLEXIBLE BRONCHOSCOPY: WHAT TO EXPECT FROM A NEW SERVICE
M. G. Slade. Churchill Hospital, Oxford, UK
Introduction: In August 2003, after appropriate training, we initiated an interventional bronchoscopy (IB) service in our cancer centre. There has been continuous, prospective data collection on all procedures performed since that date. There are few published data from the UK on IB practice. We hypothesised that our data would be of interest to colleagues planning to develop an IB service.
Methods: Data were extracted on all procedures between August 2003 and July 2007. These included indications, diagnosis, technique, outcomes (survival, FEV1, performance status, breathlessness) and complications.
Results: 116 procedures were performed, (75 as first IB procedure, 41 subsequent procedures), all for the relief of malignant central airway obstruction. There were 17, 24, 31 and 44 procedures per year, respectively. For first procedures (n = 75), median survival was 146 days, median improvement in FEV1 was 24%, and in performance status 1 point. In 17 patients (23%) the FEV1 improved by 50% or more. 29 patients (25%) had an FEV1 <1.0 litre pre-procedure and had similar outcomes to the group as a whole. A qualitative improvement in reported breathlessness occurred in 72%. 7 patients (9%) survived less than 30 days: 3 died from rapid tumour progression, 1 massive haemoptysis, 1 pneumonia, 2 respiratory failure. Across all procedures, an ablative technique (cryotherapy, electrocautery, argon plasma coagulation) was used in 87 (75%) and airway stenting in 29 (25%). Non-fatal complications occurred in 9 patients (8%).
Conclusion: Steady procedure growth can be expected in new IB practice. Clinically significant improvements in FEV1, performance status and breathlessness can be achieved with acceptable morbidity and mortality, even in patients with low FEV1 pre-procedure.
A PROSPECTIVE AUDIT EXAMINING THE IMPACT OF INTEGRATED PET-CT SCANNING ON LUNG CANCER MULTIDISCIPLINARY TEAM DECISION MAKING
C. Hooper, I. Lyburn, A. Penketh. Cheltenham General Hospital, UK
Introduction: Studies have demonstrated that PET scan results change treatment in 19–30% of patients with non-small cell lung cancer. Integrated PET-CT has been demonstrated to have a greater diagnostic accuracy than visual correlation of PET and CT, but the additional impact on patient management is less clear. The decision to scan and response to scan results should be conducted within the gold standard decision making environment of the multidisciplinary team (MDT).
Aims: To examine the impact of integrated PET-CT scanning on lung cancer MDT decision making in a district general hospital setting. Also to confirm the effect of PET-CT on TMN staging and compare PET-CT staging with surgical staging.
Methods: All patients who were discussed by the lung cancer MDT before receiving a PET-CT scan for suspected or confirmed lung cancer between June 2006 and March 2007 were included. The MDT was asked to commit to a collective pre PET-CT management plan for each patient and this was compared to the post PET-CT plan. Data were collected prospectively at each fortnightly lung cancer MDT meeting and later verified using MDT record sheets.
Results: The lung cancer MDT requested that 21 patients undergo a PET-CT in 10 months. Their CT staging complied with NICE guidance for PET indications. There was a single solitary pulmonary nodule. PET-CT confirmed CT staging in 9/20 (45%) patients, up-staged 9/20 (45%) and down-staged 2/20 (10%). The pulmonary nodule had a borderline SUV. PET-CT altered the MDT management plan in at total of 7/21 (33%) patients. Surgical staging was available for 10 patients, confirming PET-CT staging for 5/10 (50%) and being greater than that established by PET-CT for 5/10 (50%).
Conclusion: A systematic approach in compliance with NICE guidelines was taken in requesting PET-CT scans in this group of patients. The formal MDT plan was changed in 33% of cases. This represented avoidance of potential morbidity associated with delivering CHART to an unencompassable field in 3 cases and provided useful additional preoperative information for at least 4 patients. There was no avoidance of inappropriate planned surgery. It is perhaps surprising that the use of integrated PET-CT did not produce greater concordance between radiological and surgical staging. This may represent true disease progression in the time period between staging procedures.
PULMONARY MALIGNANCY IN PATIENTS WITH A PREVIOUS DIAGNOSIS OF BREAST CANCER
N. Sinnott, H. Burhan, M. Asim, S. Durairaj, O. Khan, T. Zahoor, M. J.Walshaw. The Cardiothoracic Centre-Liverpool, UK
Introduction: A significant proportion of malignant pulmonary shadows are secondary deposits, yet diagnosis still falls to the lung cancer unit. Breast cancer is common: increasing survival means that more may present with lung metastases. To explore this further, we looked at presenters to our lung cancer unit with a histological diagnosis of chest malignancy who had a history of breast cancer.
Methods: We cross checked our lung shadow database (2000–2006), with the local breast cancer registry for patients with a breast cancer history. We interrogated the records of all 127 such cases for smoking history, duration of breast cancer, pulmonary lesion appearance, and lung tumour histology.
Results: Three primary breast cancers and 12 non-malignant cases were excluded. Of the remaining 112 patients (mean age 72 (range 40–94), mean PS = 1 (0–4), mean smoking history 31 pack years (0–126), mean FEV1 1.48 l (0.33–3.36)), 37 (33%) had primary lung cancer, 67 (60%) metastatic breast cancer, 5 (5%) metastatic disease (unknown primary) and 2 (2%) other cancers (plasmacytoma and lymphoma). There was no difference in smoker numbers between breast cancer deposits and the remainder (χ2 = 2.30, p = NS) nor in lung lesions type/distribution (data available in 90 cases, χ2 = 1.07, p = NS). There was a trend (p = 0.08) towards breast cancer patients having smoked less. In 78 cases where data were available, breast metastases were the more likely cause of the malignancy if the primary was diagnosed ⩽15 years (see table). Average time from diagnosis was 7 years (0–28).
Conclusion: In the majority of breast cancer patients referred to a lung cancer unit the pulmonary disease will be due to breast cancer metastases: this is true up to 15 years after diagnosis, more so for those who have smoked less. With the rising incidence of breast cancer and its improving survival, pulmonary clinicians will need to be increasingly aware of the likelihood of breast cancer metastases in this patient group.
PRESENTING SYMPTOMS, CHEST RADIOGRAPH ABNORMALITIES AND FEV1 IN GP REFERRALS FOR SUSPECTED LUNG CANCER: HOW WELL DO THEY DISCRIMINATE?
H. J. Steer, E. Bowie, V. Masani. Royal United Hospital, Bath, UK
Background: The Department of Health introduced guidelines in 2000 for suspected lung cancer referrals, which recommended an urgent chest x ray (CXR) for patients with haemoptysis, or persistent symptoms of cough, chest pain, dyspnoea or weight loss. Urgent respiratory referral was recommended for those with persistent haemoptysis, a CXR suggestive of cancer or if a high clinical suspicion of lung cancer existed. We reviewed all new patients seen in our suspected lung cancer clinic in 2005 to determine whether presenting symptoms, an abnormal CXR, a smoking history and FEV1 could help discriminate between patients with lung cancer and those with benign conditions.
Methods: The initial referral letter and subsequent clinic letters of all new referrals to the urgent suspected lung cancer clinic in 2005 were reviewed. The CXR findings were defined either as (1) consistent with malignancy (mass, lymphadenopathy, collapse, consolidation, effusion) or (2) normal/not consistent with malignancy. Smoking history was defined as being over 10 pack years.
Results: A total of 359 referrals were made, 63 of which were excluded—40 due to lack of information and 23 because of other cancers including mesothelioma, lymphoma and pulmonary metastasis. Of the remaining 296 patients 108 (37%) had primary lung cancer, of which 71% were NSCLC, 7% were SCLC and 21% were histologically unproven. Comparing presenting symptoms in the group with lung cancer (C) to the group with benign diagnoses (B), we found that persistent cough (C 66.7% vs B 51.6%; p = 0.015 by Fishers exact test), weight loss (C 43.0% vs B 26.1%; p = 0.004), smoking history (C 91.5% vs B 57.1%; p<0.001), CXR findings (C 95.3% vs B 70.4%; p<0.001), dyspnoea (C 58.3% vs B 45.7%; p = 0.04), and chest pain (C 34.3% vs B 21.3%; p = 0.019) were more common in lung cancer. Haemoptysis was more common in benign diagnoses (C 23.1% vs B 25.5%), although this was not significant. Mean percentage predicted FEV1 was lower in those with lung cancer (C 71.5 vs B 79.3, mean difference 7.8 (95% CI 1.2 to 14.4); p = 0.02 by independent samples t test).
Conclusion: Most of the symptoms listed in the Department of Health guidelines occurred more frequently in lung cancer than in benign diagnoses. Interestingly haemoptysis was not discriminatory. This is likely to reflect the relatively high numbers seen with haemoptysis due to benign causes. Some of these patients may not need referral providing there are no other concerning features and it is not persistent.
Assessment of comorbidity in COPD
MEASUREMENT OF OPEN CAPACITY IN STABLE COPD PATIENTS
Background: The open capacity (OC), ie, the difference between total lung capacity and closing capacity (OC = TLC – CC), denotes the volume range where peripheral airway closure is absent. This index has been proposed instead of CC, because the measurement is easier to perform and there is no need to determine RV.
Methods: In 50 stable chronic obstructive pulmonary disease (COPD) patients stratified according to GOLD, we measured spirometry, dyspnoea (VAS), OC and slope of phase IV (single-breath N2 test), and arterial Pao2, after administration of 2.5 mg inhaled salbutamol via a nebuliser. Tidal expiratory flow limitation (FL) during resting breathing was also measured with the negative expiratory pressure (NEP) technique.
Results: See table. The VAS was increased in stages III and IV concurrent with a decrease in IC, reflecting hyperinflation. The OC decreased in stage II and could not be assessed in stages III and IV because the slope of phase III was continuously rising, indicating marked ventilation distribution abnormality. The Δ(IC-OC) decreased in stage II. In both stages I and II, IC>OC (reflecting tidal airway closure) was present in one patient (each). The slope of phase IV increased progressively from stage O to stage IV, the Pao2 correlating significantly with ΔN2/L (%pred) (p<0.05). In group O, 4/10 patients had abnormal ΔN2/L. Tidal FL was present in one stage II patient, and in about one-half of stage III or IV patients.
Conclusion: The open capacity is as useful as the closing capacity, but it is easier for the COPD patients to perform and requires less equipment. Using single-breath N2 test, abnormalities can already be found in GOLD zero patients.
AN OBSERVATIONAL STUDY OF THE PREVALENCE OF ANAEMIA IN MODERATE TO SEVERE COPD
M. Masoli, T. Howell, P. Hughes. Derriford Hospital, UK
Introduction: Anaemia and haematocrit in chronic obstructive pulmonary disease (COPD) have been identified as independent risk factors for reduced functional capacity and mortality respectively. COPD is known to have a systemic inflammatory component characterised by raised levels of inflammatory markers that may affect haematopoiesis. This study aimed to examine the prevalence of anaemia in a population of COPD patients under chest clinic follow up.
Methods: A retrospective analysis of patients currently under follow up with Derriford Hospital COPD outreach service was undertaken using the most recent blood test data available. Anaemia was defined as a haemoglobin <13 g/dl for both men and women since the issue of Hb threshold in post-menopausal women remains controversial. The main focus of the study was those patients with an Hb <12 g/dl, as this level is considered more clinically significant and is the defined cut-off point for treatment in anaemia in chronic heart failure. The notes of all anaemic patients were examined and patients with haematological disorders, malignancy, gastrointestinal bleeding or recent acute coronary syndrome were excluded.
Results: 210 patients were included in the analysis, 86 men, 124 women; mean (SD) age for the anaemic and non-anaemic groups was 77 (8.3) years and 73 (9.6) years, respectively. The majority of patients had severe COPD with a mean FEV1 0.87 (0.37). Anaemia (<13 g/dl) was present in 47% and polycythaemia in 8%. Mean Hb levels for anaemic and non-anaemic patients were 11.6 (1.0) g/dl and 14.5 (1.2) g/dl, respectively. 25% of patients were found to have an Hb <12 g/dl (mean Hb 10.9 (0.78) g/dl). Haematocrit was significantly reduced in this group (mean HCT 0.35). There was no difference in mean Hb between patients receiving supplemental oxygen and those who did not receive it; however, more patients in the anaemic group were receiving supplemental O2 (42% vs 35%).
Conclusion: This study suggests that anaemia in COPD may be more prevalent than previously thought, particularly in patients with more severe COPD. Further studies are required to assess the clinical and physiological impact of anaemia in COPD and determine whether correcting anaemia may have any place in the management of this disease.
ULTRASOUND MEASUREMENT OF RECTUS FEMORIS MUSCLE CROSS-SECTIONAL AREA AND THE RELATIONSHIP WITH WHOLE BODY FAT FREE MASS AND QUADRICEPS STRENGTH IN COPD
J. M. Seymour1, C. Ward1, C. Jolley1, J. Steier1, G. Rafferty1, P. Sidhu2, M. Polkey3, J. Moxham1. 1King's College London; 2King's College Hospital; 3Royal Brompton Hospital, London, UK
Introduction: Quadriceps muscle strength (QMS) is on average 30% lower in chronic obstructive pulmonary disease (COPD) than in healthy age matched individuals, whereas upper limb and diaphragm strength are relatively preserved. Interestingly, reduced quadriceps maximum voluntary contraction strength (QMVC) provides greater prognostic information than body mass index (BMI) or whole body fat-free mass (FFM) but demands patient cooperation and effort. Ultrasound measurements are effort independent, radiation free and can be performed by non-expert personnel. We hypothesised that a reproducible index of specific lower limb muscle mass could be obtained using ultrasonography and that this would better predict QMS in COPD than FFM measurement.

Methods: Healthy volunteers and patients with COPD were recruited. Spirometry, FFM (electrical bioimpedance), right leg QMS and rectus femoris cross sectional area (RFCSA) were measured. RFCSA was determined by ultrasound (planimetric technique) at two-thirds of the distance between the anterior superior iliac spine and patellar border (see fig) and recorded as the mean of three measurements within 5% of each other. QMS was assessed by QMVC and twitch quadriceps contraction following magnetic femoral nerve stimulation (TwQ). Inter-occasion and inter-observer variability of RFCSA measurement was assessed using Bland Altman analysis. Unpaired t tests were used to examine between group differences.
Results: 20 healthy volunteers with normal spirometry (mean (SD) age 54 (15) years, 9 males) and 22 patients with COPD (68 (10) years, 11 males, 47 (23) %predicted FEV1) were recruited. Although BMI was similar, FFM was greater among healthy volunteers than in COPD (50 (10.9) kg vs 45.7 (5.9) kg, p<0.01), as was RFCSA (508 (182) mm2 vs 314 (89) mm2, p<0.01) and QMS (QMVC: 39.8 (16.5) kg vs 23.0 (6.7) kg, p<0.01; TwQ: 8.5 (3.3) kg vs 5.9 (1.2) kg, p<0.01). Twitch interpolation (an estimate of voluntary activation during a QMVC effort) was similar in both groups (0.85 (0.08) vs 0.87 (0.08)). In all subjects, reduced QMS correlated with reduced RFCSA, FFM, %predicted FEV1 and increased age. A significant correlation of QMS with BFFM was not seen in the COPD subjects (see table 1). Multiple linear regression analysis was used to assess the possible interaction of age, %predicted FEV1, FFM and RFCSA in determining QMS. RFCSA was the only variable to independently predict QMVC among all subjects (p<0.01, adjusted R2 0.66). TwQ was independently predicted by both FFM and RFCSA in healthy subjects (p<0.01, combined adjusted R2 0.62) but only by RFCSA in patients with COPD (p = 0.02, adjusted R2 0.24). Inter-occasion and inter-observer variability are presented in table 2.
Conclusion: A reduced correlation between whole body fat free mass and quadriceps strength in COPD would be consistent with preferential lower limb muscle loss in this condition, perhaps as a consequence of inactivity. A simple index of lower limb muscle mass (the RFCSA) can predict quadriceps strength as assessed by either QMVC or TwQ. Similar to TwQ, ultrasound RFCSA measurement is independent of patient effort, but is quicker and easier to perform. The 95% limits of agreement between RFCSA measurements are comparable to those previously reported for QMVC or TwQ and may be due in part to injudicious selection of measurement location, given narrower inter-observer limits seen when scans are taken from the same marked point.
MUSCLE RING FINGER PROTEIN 1 (MURF-1), ATROGIN-1 AND MUSCLE WASTING IN COPD
S. A. Sathyapala1, G. S. Marsh1, N. S. Hopkinson1, J. Moxham2, P. Kemp3, M. I. Polkey1. 1Royal Brompton Hospital; 2King's College Hospital, London, UK; 3Imperial College, London, UK
Introduction: Thigh muscle wasting is a poor prognostic factor in COPD. Animal models implicate increased MuRF-1 and atrogin-1 expression in muscle wasting and elevated quadriceps MuRF-1 and atrogin-1 have been described in COPD patients compared to controls.
Aim: To investigate the relationship between quadriceps MuRF-1 and atrogin-1 mRNA and clinical parameters of muscle wasting in COPD patients versus controls.
Methods: 19 GOLD Grade II-IV COPD patients and 12 healthy controls underwent lung function, arterialised capillary ear lobe blood gas analysis, fat-free mass measurement by bioelectrical impedance and needle biopsy of the vastus lateralis. Muscle MuRF-1 and atrogin-1 mRNAs were quantified (normalised to β2-microglobulin (β2M) or acidic ribosomal phosphoprotein PO, RPLPO) using real-time PCR. Mid-thigh cross-sectional area (MTCSA) was assessed by CT in 10 patients and 7 controls. Analysis of group differences was performed using the unpaired Student’s t test and Mann–Whitney U test according to data distribution and correlations by simple regression analysis.

Results: In the COPD group (but not controls) there were significant negative correlations between MuRF-1 (normalised to β2M or RPLPO) and MTCSA (r = −0.74 p = 0.01, r = −0.75 p = 0.01) and FFMI (r = −0.54 p = 0.02, r = −0.51 p = 0.03), but not between atrogin-1 and MTCSA or FFMI (see table and fig).
Conclusion: Quadriceps MuRF-1 mRNA negatively correlates with parameters of thigh and global muscle bulk in COPD patients and MuRF-1 may therefore be an important contributor to muscle wasting in these patients. The absence of a correlation in controls suggests a balance between protein synthesis and degradation in healthy subjects.
THE EFFECT OF MUSCLE WASTING ON EXERCISE CAPACITY AND DEPRESSION IN PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
K. Al-Shair1, B. Mallia-Milanes1, R. Dockry2, U. Kolsum2, T. Southworth2, K. Roy2, D. Singh1, J. Vestbo1. 1North West Lung Research Centre, The University of Manchester; 2Medicines Evaluation Unit, Wythenshawe Hospital, Manchester, UK
Introduction: In recent years, there has been an increasing interest in studying extrapulmonary manifestations of chronic obstructive pulmonary disease (COPD) such as loss of weight, muscle wasting, osteoporosis and depression. Muscle wasting in COPD may be related to systemic inflammation, dietary status, and reduction in lung function. Changes in fat-free mass may impact on both exercise capacity and mood in COPD. We aimed to study the association between fat-free mass and exercise capacity and depression in patients with COPD.
Methods: To date 74 stable COPD patients have been enrolled in our cross-sectional study, (our aim is 100 patients). All subjects underwent measurement of body composition using bioelectrical impedance analysis, Dutch criteria for muscle-wasting were used (FFM index <16 kg/m2 for men, <15 kg/m2 for women). We used 6 minute walk test (6MWT) to measure exercise capacity, and we measured spirometry and capillary arterial earlobe blood for blood gases analysis. The presence of depression was investigated using the Centre for Epidemiologic Studies Depression Scale (CES-D) and the Brief Assessment Schedule Depression Cards (BASDEC). Dyspnoea was assessed using the MRC score. Data management and analysis were performed using SPSS 13.
Results: We found no differences in FEV1, MRC dyspnoea score, or Pao2, but BMI was lower (p = .001) in wasted than in non-wasted patients. MRC dyspnoea score was positively correlated with BASDEC score (0.27, p = 0.02) and negatively correlated with total distance in 6MWT (−0.45, p = 0.001). Among the whole sample 17.1% suffered from depression disorder (total of 7 or more in the BASDEC scoring system), and the prevalence of depression among wasted patients was 26.7% and 14.5% among not wasted patients. Moreover, 83.3% of depressed and 34.6% of not depressed patients walked less than 350 metres in the 6MWT. The BASDEC and CES-D depression scales were predictors of total distance in 6MWT after correction for FEV1%, gender, age and pack/years (p = 0.01 and 0.018, respectively). We also found that 53.3% of depleted patients and 43.4% of not depleted walked less than 350 metres in the 6MWT. A multiple linear regression analysis showed insignificant positive correlation between FFM index and total distance in 6MWT before and after adjustment to FEV1, age and BMI (p = 0.19 and 0.35, respectively).
Conclusion: Both dyspnoea and depression were predictors of exercise capacity in patients with COPD. Fat-free mass index was less strongly associated with exercise capacity, underlining the importance of perception and mood in COPD.
ELEVATED C REACTIVE PROTEIN LEVELS ARE ASSOCIATED WITH AN ACCELERATED DECLINE IN LUNG FUNCTION IN AN AGEING POPULATION
N. Ward1, N. E. Rice2, D. Melzer2, B. D. Patel1. 1Department of Respiratory Medicine, Royal Devon and Exeter NHS Foundation Trust; 2Epidemiology and Public Health Group, Peninsula Medical School, UK
Introduction: Although cross sectional studies have reported an inverse association between C reactive protein (CRP) level and forced expiratory volume in 1 second (FEV1), results relating to decline in FEV1 from longitudinal studies have been conflicting. Using data from the English Longitudinal Study of Ageing (ELSA) we assessed the association between CRP and decline in FEV1.
Methods: Measurements of FEV1 were obtained in 2001 and 2004. Predicted values for FEV1 were calculated using regression coefficients for age and height derived independently from men and women life-long non-smokers without respiratory disease. Blood CRP levels were obtained at the 2004 survey. Where necessary, appropriate methods were used to normalise variables before inclusion in correlation or regression analyses.
Results: Measurements of CRP and decline in FEV1 were available for 1263 people (45.8% men), mean (SD) age 61.9 (8.8) years. There was a significant inverse relationship between ln CRP and FEV1 percent predicted at the 2004 survey (r = −0.23, p <0.0001). In regression analysis this remained significant after adjustment for age, sex, smoking status and pack years smoked (β = −0.12, p<0.001). There was a significant inverse association between ln CRP measured in 2004 and decline in FEV1 as percent of baseline (r = −0.11, p⩽0.0001). In regression analysis this remained highly significant after adjustment for age, sex, smoking status and pack years smoked (β = −0.87, 95% CI −1.41 to −0.32, p = 0.002). The rate of decline in individuals in the bottom decile of CRP was −5.78% (±8.07) compared with −9.37% (±12.70) in the top decile (p = 0.002). The trend across deciles remained highly significant after adjustment for age, sex, smoking status and pack years smoked (p⩽0.002).
Conclusion: These results support an inverse association between CRP and FEV1. In this cohort we also show an association between CRP levels and decline in FEV1 in the preceding 3 years. These associations were independent of potential confounding exposures. This suggests that either systemic or airway inflammation, reflected by an elevation in CRP, is associated with a more rapid decline in FEV1.
TEN YEAR LONGITUDINAL CHANGE IN LUNG FUNCTION AND C REACTIVE PROTEIN IN MIDDLE-AGED MEN IN NORTHERN IRELAND
K. M. Mcclean1, C. R. Cardwell1, F. Kee2, I. S. Young2, J. S. Elborn3. 1Queens University; 2Royal Victoria Hospital; 3Belfast City Hospital, UK
Background: Systemic inflammation may be related to reduced pulmonary function. We tested the hypothesis that longitudinal changes in high sensitivity C reactive protein (hsCRP) would be related to decline in lung function over 10 years in apparently healthy middle-aged men in Northern Ireland.
Methods: From 1991 to 1994, 2745 healthy men aged 50 to 59 years were recruited into the Belfast arm of the Prospective Epidemiological Study of Myocardial Infarction (PRIME). 2010 of these men were rescreened at 10 years. In this study we describe cross-sectional and longitudinal analysis of the 722 men who had a valid spirometry trace (ERS/ATS criteria) and plasma sample at both time points.
Results: The men had a mean age of 54.4 years at baseline and 36.4% had never smoked. In cross-sectional analyses of baseline and 10 year follow-up data, there was a negative relationship between hsCRP and forced expiratory volume in 1 second (FEV1). After adjustment for smoking, BMI, age and height, the difference in FEV1 was reduced by 5.4 ml (95% CI −10.6 to −0.24, p = 0.04) and 18 ml (95% CI −26.1 to −10.5, p<0.0001) for each mg/l increment in serum hsCRP in baseline and 10 year follow-up samples, respectively. Mean decline in FEV1 over the 10 year period was 454 ml. There was no significant association between baseline serum hsCRP levels and decline in FEV1 (p = 0.25) or forced vital capacity (p = 0.31) over 10 years. There was also no significant association between the mean of the two hsCRP measurements and 10 year decline in lung function (p = 0.75). There was, however, an association between the change in hsCRP over 10 years with change in FEV1 when assessed as a continuous measure (−3.4 ml/mg/l change in hsCRP, 95% CI −6.3 to −0.55, p = 0.019). After adjustment for confounders this association remained (p = 0.03).
Conclusion: This analysis provides further evidence that serum hsCRP levels are inversely associated with lung function in cross-sectional studies. In this population, an increase in hsCRP over 10 years is associated with a decline in lung function over the same time period. This association suggests a link between systemic inflammation and decline in lung function.
STABILITY OF AIRWAY AND SYSTEMIC INFLAMMATORY BIOMARKERS IN MODERATE COPD PATIENTS OVER 1 YEAR
U. Kolsum, K. Roy, C. Starkey, Z. Borrill, B. Mallia-Milanes, J. Vestbo, D. Singh. University of Manchester, UK
Background: Chronic obstructive pulmonary disease (COPD) involves airway and systemic inflammation. Induced sputum and blood biomarkers can be used to assess inflammation. However, there is limited information on the change in airway and systemic inflammatory biomarkers over time, or their relation to each other.
Aims: To investigate the stability of airway and systemic inflammatory biomarkers over 1 year and the relationships between airway and systemic inflammatory biomarkers.
Methods: 58 COPD patients were recruited for the baseline visit (FEV1 mean (SD) 57.2 (13.7)% predicted). Airway and systemic inflammation measurements were performed at the baseline visit and repeated 1 year later. Induced sputum differential cell counts (neutrophil %, macrophage % and eosinophil %) and sputum supernatant interleukin-8 (IL-8) were measured. Systemic inflammation was measured by serum interleukin-6 (IL-6), plasma tumour necrosis factor-α (TNF-α) and C reactive protein (CRP). Paired t test or Wilcoxon matched pairs test determined the mean differences between visits. Reproducibility was expressed as an intraclass correlation coefficient (Ri). Pearson or Spearman correlations determined the relationships between the airway and systemic markers. The table shows the values measured at baseline and year 1.
Results: There was no significant change in the group mean (or median) values for all airway and systemic biomarkers between both visits (p>0.05 for all). Ri analysis showed significant agreement between the two visits for macrophage %, IL-8, CRP, TNF-α and IL-6, but not for % neutrophils and % eosinophils (p>0.05). At the baseline visit, neutrophil % was correlated with CRP (r = 0.4, p = 0.02). At the year 1 visit, neutrophil % and IL-8 were associated with TNF-α (r = 0.5, p = 0.002 for both). CRP was associated with IL-6 at both visits (r = 0.5, p = 0.0001, r = 0.5, p = 0.0002 respectively).
Conclusion: In our moderate COPD patients the overall group means (or medians) of airway and systemic inflammatory biomarkers do not change over a year. Taking into account individual patient variability, eosinophil and neutrophil % have the most variability. Induced sputum measurements appear to be more variable than systemic biomarkers. Links between neutrophilic airway inflammation and systemic inflammation was found to exist at both visits. A robust link between CRP and IL-6 is present at both visits but was not linked to TNF-α.
CT ASSESSMENT OF COPD PHENOTYPE IN A COHORT OF 133 PATIENTS
G. Mair1, D. Mcallister1, J. Maclay1, M. Connell2, J. Murchison2, W. Macnee1. 1Edinburgh University; 2Lothian Health NHS Trust, UK
Introduction: Emphysema can be quantified as CT lung density and has been validated against pathology, pulmonary function, health status and exercise tests. In order to better define COPD into separate phenotypes of disease, we have examined relationships between emphysema distribution and clinical parameters.

Methods: Patients were recruited as part of a cross-sectional study on COPD. Demographic data, spirometry, 6 minute walking distance, MRC and SGRQ scores were collected. Patients underwent low dose CT scanning and the scans were analysed using software developed in house. Assessment was made using two pixel indices (PI) of low density (PI-910 and PI-950). Distribution was divided into upper or lower and core or rind predominance (volumes were divided equally). In addition, hole size analysis (number of clustered areas of low density plotted against their size, slope indicates severity) was performed.
Results: In comparing upper to lower zone predominant disease, only one clinical parameter was significantly different; greater SGRQ score with upper zone predominance (p = 0.01). Core predominance was associated with lower FEV1 %predicted (p<0.001), FEV1/FVC ratio (p<0.001), and BMI (p = 0.012), but higher BODE index (p<0.001), and MRC dyspnoea score (p = 0.011). When divided into four groups depending on core/rind and upper/lower distribution, all of these associations remained significant except BMI. In all cases, those patients with a predominance of lower zone rind disease were less severe. Hole size analysis revealed that patients with predominantly upper zone, core disease had the most severe emphysema (correlation with extent of emphysema; upper zone r = 0.33, p<0.001, core r = 0.68, p<0.001).
Conclusion: Our results show that CT density can be used to define emphysema distribution. Differentiating core from rind predominance relates better to clinical parameters than differentiating upper from lower predominance. Clinically, patients with upper zone, core predominance have most severe disease.
WHEN SHOULD WE START MONITORING ALPHA-1 ANTITRYPSIN DEFICIENT SUBJECTS?
J. Holme1, J. Stockley1, R. A. Stockley2. 1University Hospital Birmingham NHS Foundation Trust; 2University of Birmingham, UK
Introduction: Several physiological and radiological parameters have been shown to be useful for the diagnosis and monitoring of progression in COPD related to alpha-1 antitrypsin deficiency (AATD). However, the age at which these parameters become abnormal, and the chronological order in which this occurs, is not known. We aimed to assess the age at which physiological and radiological measurements become abnormal in PiZ subjects with AATD in order to determine the age at which screening for early disease should be commenced using 2 different methods. We studied 63 subjects with the PiZ phenotype from the UK AATD registry who had never smoked and 221 ex or current smokers. We also studied 204 subjects who had been diagnosed with AATD due to lung disease (lung index) and 42 who were identified by family screening alone (non-index) in order to reduce the selection bias associated with registry data. The latter are also the subjects in whom screening for disease is applicable.
Methods: FEV1 % predicted, FEV1:FVC and KCO % predicted were measured. Density mask analysis was performed on CT scan slices from the upper (aortic arch level) and lower (inferior pulmonary vein level) zones, to determine the proportion of voxels less than −910 HU (voxel index), with a higher number indicating more extensive emphysema. Correlations and regression equations were calculated to examine the relationships between age and each of the variables. The average normal value for each parameter was inserted into the regression equation for all variables with a significant correlation with age, in order to predict the age at which the average patient exceeded the average population value. Finally, we calculated the proportion of subjects in each 5 year age cohort who had a test result that was worse than the average for the general population, and recorded the age group at which more than 50% of subjects (a greater number than expected in the general population) achieved this threshold.
Results: There was reasonable agreement between the two methods used. Physiological and densitometry parameters were abnormal in the majority of ex and current smokers and lung index cases prior to their baseline visit, even if they were in their 20s. Test results, especially physiology, became abnormal in these subjects at a much younger age than in never smokers and non-index cases respectively. The table shows the calculated age at which test parameters become abnormal for never smokers and non-index subjects using the two methods described above. In never smokers, CT densitometry tended to become abnormal in the 20s, shortly followed by gas transfer measurements. Abnormal spirometry only became apparent later in the late 30s to 40s. For non-index subjects, CT densitometry and gas transfer became abnormal in the 20s, with spirometry only deviating from normal some 15–20 years later.
Conclusion: The data suggest that monitoring subjects with AATD should begin in early adult life and that CT densitometry and gas transfer measurement will be more sensitive than spirometry to detect early disease.
USE OF THE OESOPHAGEAL DIAPHRAGM ELECTROMYOGRAM TO DETERMINE NEURAL RESPIRATORY DRIVE IN HEALTHY SUBJECTS AND IN COPD
C. J. Jolley1, J. S. Steier1, J. Seymour1, K. Ward1, G. Rafferty1, A. Lunt1, M. I. Polkey2, Y. M. Luo3, J. Moxham1. 1King's College London School of Medicine, King's College Hospital; 2Royal Brompton Hospital, London, UK; 3Guangzhou Institute of Respiratory Diseases, China
Introduction: Levels of neural respiratory drive (NRD) are high in chronic obstructive pulmonary disease (COPD). NRD can be accurately measured using a multipair oesophageal electrode to record the diaphragm electromyogram (EMGdi), but normal data are limited. This study aimed to establish ranges of EMGdi in healthy subjects and to investigate the use of EMGdi as a biomarker of COPD severity.
Methods: EMGdi was recorded during resting breathing in 100 healthy subjects (mean (SD) age 41.4 (17.9), 57.3% male), and 25 patients with COPD (age 66.8 (8.35), 76.0% male, FEV1 35.3 (14.8)%pred, VC 86.6 (21.5)%pred). EMGdi was normalised to EMGdipeak recorded during maximal inspiratory manoeuvres (“EMGdi%max”). EMGdipeak was also compared to the amplitude of the compound muscle action potential recorded following bilateral magnetic phrenic nerve stimulation (CMAPdi).
Results: EMGdi%max was 9.25 (3.35) (mean (SD)) in healthy subjects. EMGdi%max was higher in subjects aged 51–80 years (28.4% of the total) than 18–50 year-olds (11.5 (3.35) vs 8.38 (2.99), p = 0.001). There were no significant male/female differences, and no correlations between EMGdi%max and age, height, weight or body mass index. EMGdi%max was higher in COPD patients than in age- and sex-matched controls (mean 27.7 (10.3)% vs 11.4 (3.36)% p<0.01), correlating with FEV1%pred (r = −0.63, p = 0.001), VC%pred (r = −0.69, p<0.001), and inspiratory capacity (IC) (r = −0.61, p = 0.02). There was a positive correlation between CMAPdi amplitude (2.41 (0.84) mV) and EMGdipeak (243.5 (72.3) uV, r = 0.61, p<0.01).
Conclusion: This is the first large-scale study of normal levels of EMGdi. EMGdi is increased in COPD and the relationships with VC%pred and IC suggest hyperinflation as a determinant. CMAPdi amplitude could provide a method of assessing EMGdi%max when volitional inspiratory manoeuvres are not possible.
MEASURING HAT:HDAC ACTIVITY RATIO IN SPUTUM MACROPHAGES: A NON-INVASIVE METHOD FOR DETECTING INFLAMMATORY STATUS IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE
A. Mulgirigama, K. Ito, S. Kharitonov, P. J. Barnes. National Heart & Lung Institute, London, UK
Background: Recent concepts of the molecular mechanisms involved in inflammation demonstrated that histone acetylation plays a critical role in regulating gene expression. Histone is acetylated by histone acetyltransferases (HAT), facilitating inflammatory gene transcription. Histone deacetylases (HDAC) reverse this process. We have already reported a reduction in HDAC activity and slight increase in HAT activity in peripheral human lung tissue and alveolar macrophages obtained by bronchoalveolar lavage from patients with COPD, compared with healthy controls. This imbalance between HAT and HDAC is a potential molecular mechanism of the persistent inflammation seen in COPD. The aim of this study was to analyse the balance between HAT and HDAC activity, in sputum macrophages from COPD patients and to compare this to healthy non-smokers. The HAT:HDAC activity ratio in sputum macrophages was also assessed as a non-invasive marker of inflammation in COPD.
Methods: Patients with moderate and severe COPD (GOLD criteria) (n = 12) and healthy non-smokers (n = 8) were recruited. FEV1 and FVC measurements were obtained by spirometry. Induced sputum was collected and the supernatant was analysed for interleukin 8 (IL-8), and growth related oncogene-α (GRO-α), by ELISA. Sputum macrophages were isolated and nuclear extraction was performed, from which HAT and HDAC activity were measured.
Results: Median (range) IL-8 and GROα levels in sputum supernatants were significantly higher in the COPD group, compared with controls (IL-8: 4794 (2807–8183) vs 190.7 (136.6–481.7) pg/ml, p<0.0001; GROα: 5433 (3760–6010) vs 422.2 (229.9–1323) pg/ml, p = 0.0002). Levels of IL-8 and GROα positively correlated with the HAT:HDAC activity ratio measured in sputum macrophages (IL-8: r = 0.5985, p = 0.0053; GROα: r = 0.5942, p = 0.0057). Median (range) HAT activity was significantly higher in COPD patients compared with controls (42.90 µg/µl (28.45–72.40) vs 16.05 µg/µl (6.000–23.05), p = 0.0034). No difference in HDAC activity was found between the two groups. Median (range) HAT:HDAC activity ratios were elevated in patients with COPD, compared to controls (848.7 (471.3–2246) vs 77.51 (37.87–230.5), p = 0.001). The HAT:HDAC activity ratio was found to be negatively correlated with FEV1 (r = −0.5489, p = 0.0122) and FEV1/FVC (r = −0.4722, p = 0.0355).
Conclusion: Our data show that the HAT:HDAC activity ratio in sputum macrophages from COPD patients is higher compared with healthy non-smokers. This HAT:HDAC imbalance is positively associated with IL-8 & GROα and negatively associated with FEV1 and FEV1/FVC. This suggests an underlying link between these molecular mechanisms and the decline in FEV1 seen in COPD. The ability to measure the ratio of HAT and HDAC activity in sputum has potential as a novel, non-invasive marker for detecting inflammatory status in COPD.
AORTIC CALCIFICATION IS DIRECTLY RELATED TO ARTERIAL STIFFNESS AND INVERSELY RELATED TO BONE MINERAL DENSITY IN PATIENTS WITH COPD
C. E. Bolton1, C. M. Mceniery2, R. Sabit1, M. Munnery3, B. Mcdonnell3, A. Dixon2, M. D. Stone4, I. B. Wilkinson2, J. R. Cockcroft3, D. J. Shale1. 1Respiratory Medicine, Cardiff University; 2Cambridge University; 3WHRI, Cardiff University; 4Bone Research Unit, Cardiff University, UK
Background: Aortic calcification and osteoporosis are associated with ageing. Calcification of the aortic wall reduces elasticity altering pressure buffering properties. We reported increased arterial stiffness (AS), a predictor of cardiovascular risk, in COPD, particularly in patients with osteoporosis, which has a greater prevalence in patients compared to older healthy controls. Hence, we expected aortic calcification to be associated with both AS and a low BMD in patients with COPD.

Methods: Patients with confirmed COPD were studied when clinically stable. Those receiving bisphosphonates, long term oral corticosteroids or with known IHD were excluded. Peripheral blood pressure was determined by sphygmomanometry and AS as aortic (carotid–femoral) pulse wave velocity (PWV) (Sphygmocor, Atcor) and augmentation index (AIx). CT scanning was performed from aortic arch to iliac bifurcation and the calcium volume in the lower 5 cm of the abdominal aorta was quantified by a volume scoring method. A representative subgroup (n = 27) had a DXA scan to determine total lumbar, total hip, femoral neck, trochanter and intertrochanteric bone mineral density (BMD).
Results: Of the 45 (27 male) patients, the mean (range) age was 66 (50–83) years. The mean (SD) FEV1 was 1.5 (0.7) litres, smoking pack years 44 with 13 patients current smokers. Peripheral MAP was 109 (11.7) mm Hg and peripheral pulse pressure 65 (16) mm Hg. The aortic PWV was 11.6 (2.6) m/s and AIx of 28.4 (9.8)%. BMD total hip was 0.94 (0.16) g/cm and total lumbar spine was 1.04 (0.19) g/cm. Aortic calcium volume (cm3-logged) was related to total hip BMD (r = −0.439, p = 0.02) and to three separate hip sites, (see fig), but not to lumbar spine. Aortic calcification was related to aortic PWV (r = 0.34, p = 0.02) but not AIx.
Conclusion: Calcium deposition in the wall of the aorta is likely to be a factor in the increased AS in patients with COPD and may be relevant to their excess cardiovascular risk. The lack of association of aortic calcification to lumbar BMD may be due to aortic calcification overlying the lumbar DXA image. Aortic PWV is preferential to AIx in this age group. The inverse relationship between aortic calcium deposition and loss of hip BMD suggests links between two degenerative processes, which may indicate premature ageing in COPD.
Supported by GlaxoSmithKline Global
ARTERIAL STIFFNESS IS REDUCED BY COMBINATION INHALED CORTICOSTEROID/LONG ACTING BETA-2 AGONIST THERAPY IN PATIENTS WITH COPD
R. Sabit1, C. E. Bolton1, C. Allanby1, J. R. Cockcroft2, D. J. Shale1. 1Respiratory Medicine, Cardiff University; 2Department of Cardiology, Cardiff University, UK
Background: Cardiovascular events are more common in patients with COPD, even when confounding risk factors are accounted for. Arterial stiffness, an independent risk factor for cardiovascular disease, is increased in patients with COPD. Inhaled corticosteroids may influence cardiovascular outcomes by reducing systemic inflammation. We hypothesised that combination inhaled corticosteroid/long acting beta-2 agonist therapy would be associated with a reduction in arterial stiffness in an open label observational study in patients with COPD.
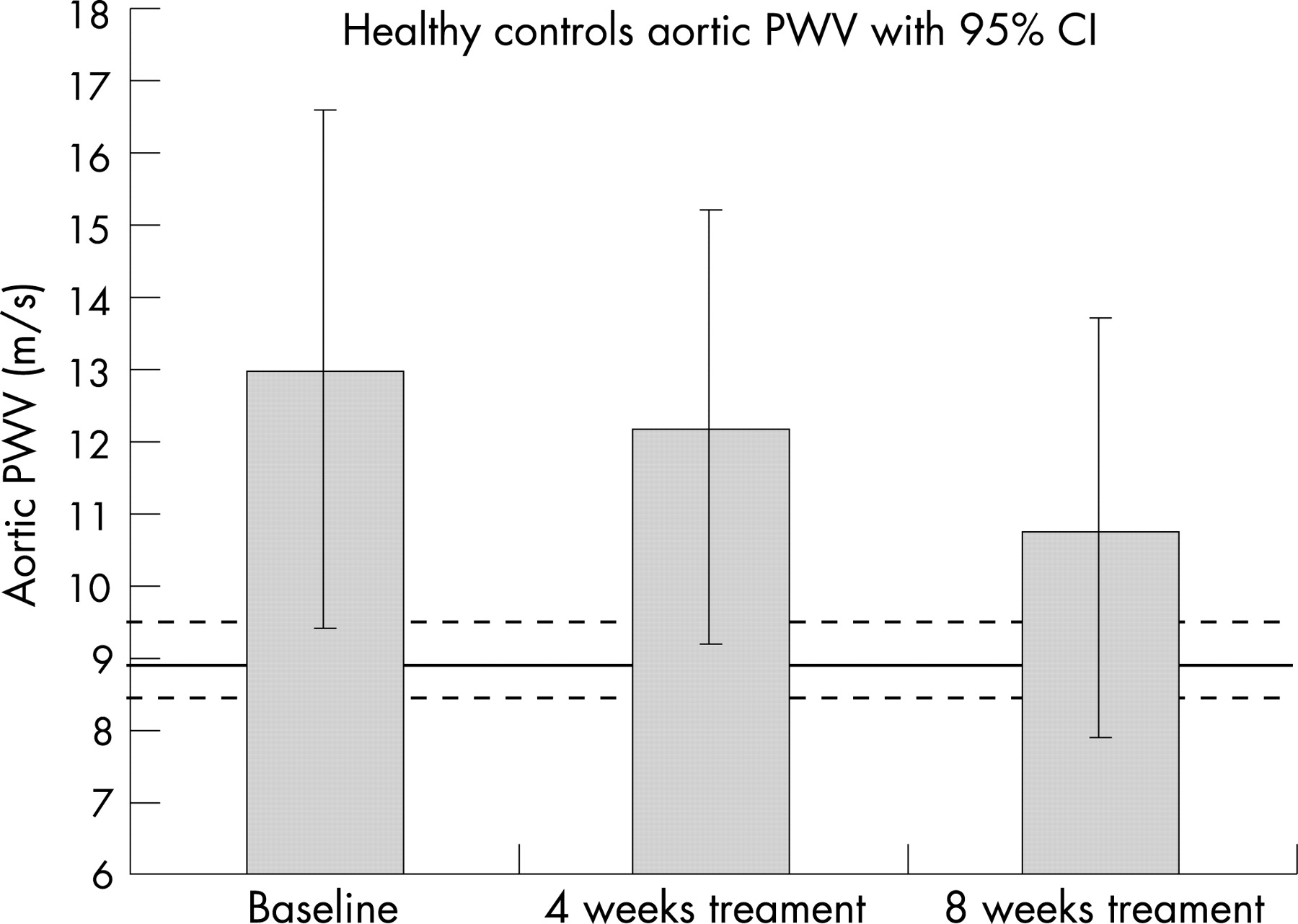
Methods: Fourteen patients with confirmed COPD, all free of overt cardiovascular disease, who met the criteria for combination inhaled therapy, were studied. Arterial stiffness was assessed by measuring augmentation index (AIx) and aortic pulse wave velocity (PWV) (SphygmoCor(AtcCor)). AIx and aortic PWV were measured on two separate occasions before commencement of treatment to assess inter-observer variability (their average formed “baseline”). All patients were independently prescribed inhaled fluticasone/salmeterol 500 μg bd by their practitioner. After 4 and 8 weeks of treatment, arterial stiffness was repeated. Spirometry was performed at baseline and after 8 weeks of treatment.
Results: Patients, mean (SD) age of 65.7 (7.7) years, had a mean (SD) FEV1 of 1.01(0.29) litres. Mean AIx and aortic PWV measurements taken before commencement of treatment were similar (both p = 0.1). Mean (SD) FEV1 increased from 1.10 (0.29) litres at baseline to 1.17 (0.34) litres after 8 weeks of treatment (p<0.01). Peripheral mean arterial pressure was higher at baseline (109 (11) mm Hg) than after 8 weeks (102 (14) mm Hg) of treatment (p<0.01). Mean AIx and heart rate did not change throughout the study. Mean (SD) aortic PWV was greater at baseline (13.0 (4.0) m/s) than after 8 weeks of treatment (10.8 (2.9) m/s) (p<0.01), but similar to aortic PWV after 4 weeks of treatment (12.2 (3.2) m/s). Mean aortic PWV was lower in patients after 8 weeks treatment than after 4 weeks treatment (p<0.01).
Conclusion: In patients with moderate-severe COPD, the inhaled fluticasone/salmeterol combination is associated with a decrease in arterial stiffness after 8 weeks of treatment. The improvement in aortic stiffness is associated with a reduction in mean arterial pressure and an increase in FEV1.
Supported by GlaxoSmithKline.
Pulmonary embolism
SURVEY OF THE PRESCRIPTION OF VENOUS THROMBOPROPHYLAXIS PRESCRIPTION IN MEDICAL INPATIENTS
R. A. Heinink, S. Saraf, K. Barnett, R. Harris, C. Mcneill, R. Lodwick. New Cross Hospital, Wolverhampton, UK
Background: It has been estimated that there are over 500,000 deaths in the EU annually from pulmonary embolism. Surveys and registries show that the risk of venous thromboembolism (VTE) in medical patients remains under-recognised and that its management is suboptimal, despite extensive clinical evidence on the benefits of thromboprophylaxis. In reaction to this, the British government established an independent experts working group in 2005, which has recently published its conclusions.
Aim: To survey medical VTE prophylaxis in our hospital, which serves approximately 250,000 patients.
Methods: We performed a survey of each individual medical inpatient bed once during a 4 month period at our hospital. Data on indications and contraindications to pharmacological VTE prophylaxis, demographics and anticoagulation prescription were collected. Data were compared to the following guidelines: ACCP-2004, SIGN-2002, ICS (International Consensus Statement)-2006, Opinion at VTE experts meeting-2006, and VTE prophylaxis guidelines recently instituted at several local hospitals. Patients were excluded if anticoagulants were contraindicated or prescribed for another reason.
Results: Data from 148 patients were included in the analysis. The number of patients in which VTE prophylaxis was indicated varied between 36% using ACCP guidelines and 93% using guidelines recently initiated at several local hospitals. The percentage of patients who received prophylaxis out of those in which it was indicated was 28% for the ACCP guidelines, and between 21% and 23% for the other four guidelines and opinions.
Conclusion: Our data support previously published data that VTE prophylaxis in medical patients is suboptimal. It also demonstrates the inconsistency of different guidelines and opinions, and supports the government’s request for a unifying national guideline.
CLINICAL SETTINGS AND PATIENT FACTORS SIGNIFICANTLY INFLUENCE DIAGNOSTIC UTILITY OF D-DIMER IN VENOUS THROMBOEMBOLISM
A. Qasim, A. Keegan, D. Byrne, M. Duggan, N. O'Connell, A. O'Driscoll. Naas General Hospital, Kildare, ROI
Background: D-dimer remain important in diagnostic algorithms for venous thromboembolism (VTE). The aim of our study was to identify factors influencing utility of D-dimers in diagnosing VTE.
Methods: Consecutive symptomatic medical patients, who presented to our emergency department during the study period from 1 November 2006 to 31 December 2006, had D-dimer assessed by using automated quantitative immunoturbidometric technique. The impact of factors including patient’s age, renal function and abnormal chest radiology on D-dimer was analysed. Final diagnosis of VTE was established by venous compression ultrasonography and computed tomographic pulmonary angiography. All VTE negative patients were followed for 2 months to detect any future occurrence of thromboembolism.
Results: Of the 4026 patients who attended our emergency department, a total of 525 patients had D-dimer assessed. Final diagnosis of VTE was established in 25 patients. Median D-dimer levels for VTE negative patients <60 years, with normal renal function, and normal chest radiology were 0.38 μgFEU/ml (range 0.19–2.3), 0.39 μgFEU/ml (range 0.17–3.5), and 0.39 μgFEU/ml (range 0.1–4.3), respectively. Similar figures for those ⩾60 years, with renal impairment and abnormal chest radiology were 0.75 μgFEU/ml (range 0.22–4.3), 0.52 μgFEU/ml (range 0.17–4.4), and 0.92 μgFEU/ml (range 0.26–5.6), respectively. Individual factors including patient age, renal function and chest radiology had significant influence on D-dimer levels (p<0.01). A combination of patient age ⩾60 years, presence of renal impairment (MDRD stage 2–5) and abnormal chest radiology resulted in a false positive D-dimer in 96% of VTE negative patients (n = 72). Overall, negative predictive value of D-dimer in VTE was above 99% for all patient groups.
Conclusion: D-dimer has high negative predictive value in thromboembolism; however, its diagnostic role is significantly influenced in patients with a triad of advanced age, renal impairment and abnormal chest radiology.
CLINICAL PROBABILITY ASSESSMENT AND D-DIMER ASSAY USE IN PATIENTS UNDERGOING CT PULMONARY ANGIOGRAM FOR SUSPECTED ACUTE PULMONARY EMBOLISM
C. Rossiter, T. Peel, M. Weatherhead. Wansbeck General Hospital, UK
Introduction: Current British Thoracic Society guidelines on the management of acute pulmonary embolism suggest all patients with possible acute pulmonary embolism should have clinical probability assessed and documented. Blood D-dimer assay should then only be considered following assessment of clinical probability. There is a perception that clinical probability is poorly assessed and that D-dimer assays are often carried out inappropriately.
Methods and results: This study looked at 101 consecutive patients undergoing CT pulmonary angiogram (CTPA) and retrospectively reviewed the notes assessing clinical probability and the use of D-dimer assays according to the BTS guidelines. Age range was 28 to 98 years (mean 69.6 years). Only 5 of the 101 case notes contained a written assessment of the clinical probability. In the remaining 96 cases this was assessed retrospectively. There were 20 patients identified as low probability. In this group 19 patients had their D-dimer measured, with 14 positive results and 5 negative results. Only 1 pulmonary embolus was identified on CTPA in a patient with a positive D-dimer. 47 patients were identified as intermediate probability. 40 of the 47 patients had a D-dimer measured (33 positive, 7 negative). There were 12 pulmonary emboli identified on CTPA within the intermediate probability group (9 with a positive D-dimer, 1 with a negative D-dimer and 2 with no D-dimer assay obtained). 1 scan was inconclusive in a patient with a positive D-dimer. 34 patients were identified as high probability. 32 of the 34 patients had a D-dimer assay measured (29 positive, 3 negative). There were 19 pulmonary emboli identified on CTPA (17 patients with a positive D-dimer, 2 patients with no D-dimer obtained). All 3 patients with a negative D-dimer had negative CTPAs for pulmonary embolus.
Conclusion: This study confirms that clinical probability is poorly assessed and documented. D-dimer assays are often carried out inappropriately especially in patients with a high probability of pulmonary embolus. Patients with low or intermediate probability with a negative D-dimer often still undergo investigation with CTPA. Only one pulmonary embolus was identified in the low probability group and highlights the need for considering and seeking out alternative diagnoses in this group.
USE OF CT PULMONARY ANGIOGRAPHY AS THE FIRST LINE IMAGING MODALITY FOR PULMONARY EMBOLISM IN A MEDIUM-SIZED DISTRICT HOSPITAL
A. Youzguin, J. Longfield, A. Allan, P. Hughes, A. Brown, M. Maciver. Southport and Ormskirk Hospitals NHS Trust, UK
Introduction: The BTS recommends CTPA as the test of choice in suspected pulmonary embolism (PE) after the pre-test probability (PTP) was assessed, and D-dimer (Dd) assayed in appropriate cases. In our hospital (325 beds) we have used CTPA as the only “in-hours” imaging mode for PE since November 2004. We were interested to find how CT pulmonary angiography (CTPA) was utilised in the first 12 months.
Methods: We analysed the radiological database from November 2004 to October 2005. Of 220 patients who underwent CTPA, we randomly sampled 100 cases: 3 did not have sufficient data, thus 97 entered the final analysis. Where PTP was not assessed, we calculated it retrospectively, using Wells criteria.
Results: PE was diagnosed in 18 patients (19%); in the remainder abnormalities other than PE were found on 29 scans (37%). CTPA was performed within 24 hours in 68%, most of delays being due to weekends. PTP had only been assessed prospectively in 7 patients (7%), but a retrospective application of Wells criteria showed that 56 (58%) had a low, 38 (39%) intermediate, and 3 (3%) high probability for PE. PE was diagnosed in 9% of patients with low, 32% with intermediate, and 33% with high PTP. Dd assay was performed in 40 patients (41%) and 14 of these were inappropriate. Conversely, there was no assay performed in 33 patients (34% of all) where it was appropriate.
Conclusion: Although the rate of PE diagnosis by CTPA was similar to major studies (PIOPED II – 18%) which may reflect the good diagnostic acumen of admitting physicians, there was poor adherence to the BTS recommended diagnostic pathway. Had these guidelines been applied, up to a third of scans could have been avoided. Further education of admitting physicians may improve this aspect of patient care.
CT SCAN RADIATION CAN EQUAL ATOMIC BOMB EXPOSURE: AN AUDIT TO INVESTIGATE THE APPROPRIATE USE OF CT PULMONARY ANGIOGRAPHY IN INVESTIGATION OF SUSPECTED PULMONARY EMBOLISM
J. E. Evans, D. Ip, E. Sawicka. Princess Royal University Hospital, UK
Introduction: British Thoracic Society guidelines recommend CT pulmonary angiography (CTPA) as initial investigation in suspected pulmonary embolism (PE). Stratification of probability of PE prior to scanning is also recommended. Within the respiratory department we noticed an increase in the number of CTPAs performed. There is no evidence suggesting an increased incidence of PE. Over recent years there has been media attention relating to the increased risk of malignancy following exposure to ionising radiation. Newspapers published reports comparing radiation dose from CT scanning to that received by survivors of atomic bombs. As clinicians we must therefore prevent unnecessary exposure to radiation in order to avoid potential future litigation. In view of this we performed an audit to investigate this matter further.
Methods: 639 CTPA reports were reviewed during the period February 2004–August 2006. We also recorded request form data. We assessed 88% of presenting chest x rays (CXR). 33% of clinical notes we reviewed in order to ascertain the symptoms, signs and probability of suspected diagnosis which had prompted this line of investigation in order assess whether it was appropriate.
Results: The number of scans performed in each consecutive 6 month period increased; 98, 104, 114, 140, 183. Indications for CTPA include shortness of breath (70%), hypoxia (64%), chest pain (58%), abnormal echo/pulmonary hypertension (28%), haemoptysis (7%) and pleural rub (20%). The following pathology was demonstrated on CTPA; pulmonary emboli (19%), pneumonia (28%), moderate/large pleural effusion (40%), COPD (25%), malignancy (25%), bronchiectasis (14%). 14% of scans were normal. Respiratory physicians, general physicians and other specialities requested 24%, 58% and 18%, respectively. Respiratory physician requests were 5 times more likely to return a positive CTPA than their general medical colleagues. 20% of presenting CXRs were normal, 61% suggested cause other than PE, and 19% demonstrated changes possibly consistent with PE. 69% of reviewed clinical histories/examinations were suggestive of cause other than PE and only 2 (1.3%) of these individuals had PE on CTPA. In only 13% was a formal assessment of probability of PE documented.
Conclusion: In this trust unnecessary radiation exposure could have been avoided in up to 440 individuals and this would have missed only 2 PEs. Clinicians seem concerned about missing pulmonary emboli. There appears to be less concern regarding the risk of unnecessary radiation exposure and potential litigation from individuals who develop malignant disease in the future. The result is inappropriate imaging, unnecessary radiation exposure and undue pressure on busy radiology departments. General clinicians do not fully utilise tools aimed at preventing this while respiratory physicians do this more accurately. This audit demonstrates the importance of thorough review of all available information, the need for better education and respiratory physician input in patients prior to CT scanning.
AN AUDIT OF CT PULMONARY ANGIOGRAM REFERRALS IN THE DIAGNOSIS OF ACUTE PULMONARY EMBOLISM: IS THERE ADHERENCE TO NATIONAL GUIDELINES?
R. J. Moon, L. Adamson, N. Bowry, R. Pandey, I. W. Brown, J. E. M. Wilkinson. Southampton University Hospitals NHS Trust, UK
Introduction: CT pulmonary angiogram (CTPA) is the gold standard investigation for pulmonary embolism (PE). However, this is an expensive and limited resource with significant radiation exposure. The British Thoracic Society guidelines (2003) suggest a hierarchical pathway of investigations: D-dimer, isotope lung (V/Q) scanning and CTPA to diagnose PE, based on a clinical probability prediction. We performed a retrospective audit of patients undergoing CT-PA to determine if there is adherence to these guidelines in a hospital with nuclear medicine and CT scanning facilities.
Methods: We identified 154 patients who underwent CTPA. 99 records were analysed for documentation of symptoms of PE, assessment of clinical probability, and documented investigations before CTPA. We assessed the clinical probability to determine the appropriateness of these investigations.
Results: Probability of PE was assessed by the audit team as high in 22 cases, intermediate in 38 cases and low in 39 cases. The medical team had assessed probability correctly in 5 out of 8 cases. 58% of the patients were not investigated appropriately before CTPA. 30 (39%) low and intermediate probability patients did not have a D-dimer assay. D-dimer had been unnecessarily requested in 9 (41%) high probability patients. A V/Q scan could have been performed in 29 patients with a normal chest x ray. 51 patients had a raised D-dimer, in whom PE was diagnosed in 18 (35%). No patient with a negative D-dimer assay had evidence of a PE on CTPA (1 low, 1 intermediate and 1 high probability). PE was diagnosed in 28 patients (6 (15%) low probability, 10 (26%) intermediate probability, 12 (54%) high probability), of whom 16 had been appropriately investigated. Of the remaining 12 patients, one did not require CT-PA as there was a high clinical probability and a high probability V/Q scan. Two intermediate probability patients had not had a D-dimer assay performed, and 9 had not undergone a V/Q scan despite an apparently normal chest radiograph. Overall, CTPA could potentially have been avoided in 48% of cases.
Conclusion: We found inadequate adherence to BTS guidelines in our trust. Promoting the use of probability assessment could guide more appropriate investigations and avoid unnecessary CTPAs.
HIGH PREVALENCE OF MULTIPLE RISK FACTORS FOR VENOUS THROMBOEMBOLISM AMONG HOSPITALISED MEDICAL PATIENTS: A CASE FOR MANDATORY FRONT-OF-HOUSE PRIMARY THROMBOPROPHYLAXIS FOR ALL MEDICAL ADMISSIONS
A. R. Guhan, H. M. Khor, J. Anderson. The James Cook University Hospital, Middlesbrough, UK
Introduction: 75% of inpatient mortality from venous thromboembolism (VTE) occurs in medical patients (MP), even though post-surgical VTE receives higher profile. The incidence of VTE among MP is estimated to be 15–20%, reducing by 50% with primary thromboprophylaxis (pTP). Increasing age of our patient population and their increasing likelihood of multiple comorbidities carries with it increasing risk of developing VTE during or shortly after their hospital stay. The annual cost of managing VTE is estimated to be £1 billion and pTP has been shown to be cost effective in terms of incremental cost per VTE avoided. Despite this knowledge, the current practice of pTP in medical inpatients is less than optimal, perhaps because pTP prescription is left to case-by-case evaluation-of-need by the treating physician. A recent audit of our practice of pTP across our Division of Medicine (289 patients in 11 wards) showed that 83% of patients should have received pTP as per the SIGN guidelines (www.sign.ac.uk/guidelines) (SG); our compliance was 17%. In this study we re-analysed data from our audit to ascertain the mean age of our medical patient population and classify the prevalence of VTE risk factors among them by age group.
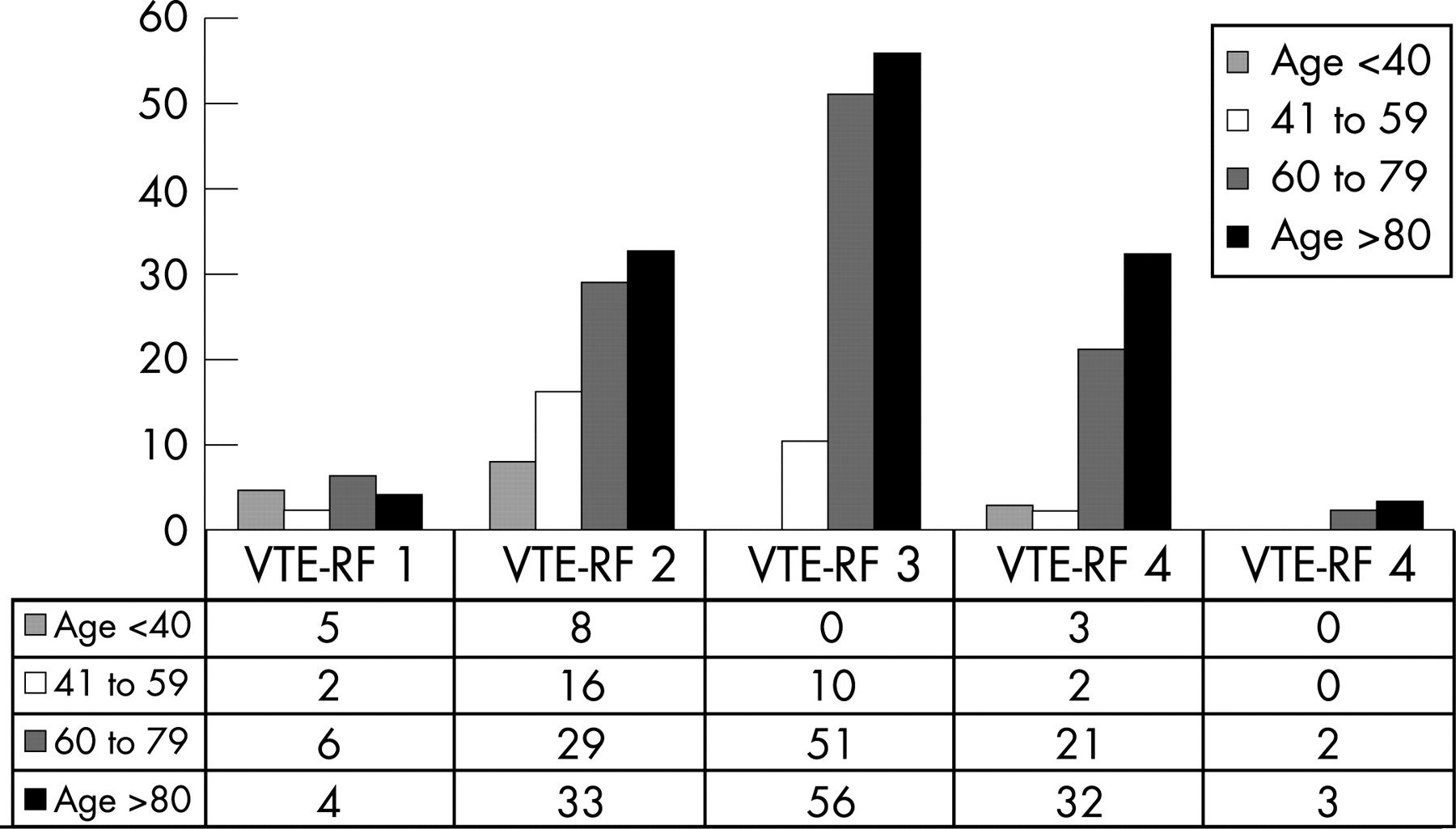
Methods: Patient demographics, primary diagnosis, secondary diagnoses and length of stay up to point of data collection (May 2006) from our audit data were analysed to ascertain the number of VTE risk factors (VTE-RF) in each patient as per the SG. Patients were grouped according to the number of VTE-RF and tabulated against their age group (<40 years, 41–59, 60–79 & >80 years).
Results: Complete data are available from 283 of 289 patients. The length of stay up to the point of data collection ranged from zero days to 209 days (mean: 13.6 days; median: 8 days). Our patients’ ages ranged from 17–110 years (mean 74; median 78 years). 237 (83.7%) were over 60 years old. Most number of patients had 3 VTE-RF (n = 117; this included age>40 and length of stay >4 days). 86, 58, 17 and 5 patients had 2, 4, 1 and 5 VTE-RF, respectively. 266 (94%) patients had 2 or more VTE-RF. Patients over the age of 60 years were significantly more likely to have 2 or more VTE-RF (n = 227 (96% of the over-60s)) as compared to those <59 years old (n = 39 (85% of the under-60s), as shown in the fig. 165 (69.6%) of the over 60s have 3 or more VTE-RF. None of the patients had less than one VTE-RF.
Conclusion: The vast majority (83.7%) of our medical patients were over 60 years old with 96% and 69.6% of them having 2 or more and 3 or more VTE-RF, respectively. Since compliance with our current system of case-by-case evaluation-of-need for pTP (as per SG) is less than optimal, a policy of front-of-house mandatory pTP prescription for all medical patients over the age of 60 years unless specifically contraindicated could be a possible solution that needs consideration.
A REVIEW OF PATIENTS ADMITTED WITH PULMONARY EMBOLISM TO DETERMINE HOW MANY CAN BE MANAGED SAFELY AS OUTPATIENTS
A. M. R. Selman, Z. Mangera, B. Yung, D. K. Mukherjee, J. T. Samuel. Basildon and Thurrock University Hospital Trust, UK
Background: Pulmonary embolism (PE) is a common differential diagnosis in medical admissions units (MAU) when patients present with breathlessness and positive D-dimer tests. Scoring systems have been developed to identify patients who may be managed as outpatients. We reviewed patients admitted with PE to our MAU to stratify the risk of significant mortality or morbidity and to determine the proportion who could be managed as outpatients using available criteria.
Methods: Patients with a confirmed discharge diagnosis of PE over a 1 year period (March 2005 to February 2006) were reviewed. Patients were stratified using the prediction score as high risk according to age (>70 years), comorbidities (cancer, heart failure, chronic lung or renal disease and cerebrovascular disease) and clinical abnormalities (pulse>110 bpm, systolic blood pressure <100 mm Hg, oxygen saturation <90% or altered mental state).
Results: Of 69 patients identified, 19 were excluded due to incomplete documentation. Of the remaining 50 patients, 14% had low clinical probability, 50% intermediate probability and 36% high probability of having PE at admission as per British Thoracic Society guidelines. 66% had CT pulmonary angiogram, 30% had ventilation perfusion scans and 12% had leg ultrasonography to confirm diagnosis. 25 (50%) were >70 years of age. 6 of the remainder had comorbidities and a further 10 patients had clinical abnormalities. 9 patients (18% overall) did not have any risk factors and would have been suitable for outpatient treatment.
Conclusion: We found that nearly one in five patients could have been safely managed as outpatients despite only including those who had a definite diagnosis of PE. If all patients with a differential diagnosis of PE were included, a significantly larger number may have been managed safely as outpatients. Treating this low risk group of patients in the outpatient setting may result in better resource allocation within hospitals, more cost effective treatment provision and a more favourable patient experience. We plan to prospectively look at all patients admitted with an admission diagnosis of PE with a view to managing appropriate patients as outpatients.
COPD: community to hospital and back again
PULMONARY REHABILITATION IN NORTHERN IRELAND: A REGIONAL SURVEY
B. O'Neill2, S. Elborn1, 3, MacMahon. J1, J. Bradley1. 1Regional Respiratory Centre, Belfast Trust, Belfast City Hospital; 2Health and Rehabilitation Sciences Research Institute, University of Ulster; 3Department of Respiratory Medicine, Queen's University Belfast, UK
Introduction: In March 2006 the Strategic Framework for Respiratory Conditions in Northern Ireland (DoH, NI) recommended a clear pathway through pulmonary rehabilitation (PR) and follow on services.
Aim: The aim of this survey was to determine the location and structure of the different components of the patient pathway such as PR programmes, ongoing exercise facilities and support networks in NI.
Methods: Questionnaires to current providers of PR, local council leisure centres providing exercise programmes for patients with respiratory conditions and support groups in NI. Data were collected between July 2006 and January 2007.
Results: There are currently 23 PR programmes in NI and these are largely concentrated in the east of the province. PR programmes were in accordance with the BTS statement for structure, except for the frequency of supervised exercise; sessions were held once a week in 11/23 (48%) programmes and twice a week in 12/23 (52%) programmes. All programmes used at least one type of exercise test, breathlessness scale and a quality of life scale; however, there was a lack of consistency between PR programmes in the specific measurement tools. 55/84 (66%) council leisure centres provided one or more exercise programme(s) that included people with respiratory disease and information on 89 programmes was provided. The programmes accessed by respiratory patients most frequently included: “GP referral” (18/89, 20%), “Health Wise” schemes (16/89, 18%), “Senior Programmes” (14/89, 16%); aerobics (8/89, 9.0%); “Fit & Well” schemes (3/89, 3%) and aqua fit (6/89, 7%). The measurement tools used in these programmes were not the same as those used by PR programmes. 59/89 (66%) programmes suggested further training needs which could facilitate the provision of appropriate exercise, specifically education in respiratory disease (42/59, 71%). There are 13 support groups for patients with respiratory disease in NI. While their function is diverse, information specifically about respiratory disease was provided by 12/13 (92.3%) support groups.
Conclusion: PR is established in NI, though may not be accessible to all patients who could benefit. Facilities for ongoing exercise and support groups are less developed. A strategic coordinated approach will ensure implementation of the whole patient pathway in NI.
A SURVEY OF PULMONARY REHABILITATION SERVICES PROVIDED IN ENGLAND IN JUNE 2007 COMPARED TO 2002
B. Selvarajah, A. O. Dunscombe, T. S. Irani, R. Banka. King George Hospital, UK
Pulmonary rehabilitation has been shown to significantly improve quality of life in patients with chronic obstructive pulmonary disease (COPD). It has also been shown to reduce attendances to primary and secondary care facilities and hence has been validated as a cost effective treatment for this condition. A survey conducted in 2002 by the British Thoracic Society (BTS) showed that 77.2% of hospitals in the UK provide a pulmonary rehabilitation service. However, many did not have secure funding and often patient numbers were limited. We endeavoured to repeat this survey to ascertain whether funding and access to pulmonary rehabilitation has improved since 2002 and whether the BTS recommendations are being met.
Methods: In June 2007, a survey was carried out by email or telephone to all English hospitals with an adult respiratory medicine department. Consultants, respiratory nurses or physiotherapists were invited to answer a series of questions regarding the pulmonary rehabilitation facilities they offer. Our results were then compared to those obtained in 2002 by the BTS Pulmonary Rehabilitation Survey.
Results: A total of 214 hospitals in England were invited to participate in the survey. We received 185 responses, of which 23 were incomplete. 150 hospitals had access to pulmonary rehabilitation (81%). This is compared to 160 (77.2%) in the 2002 survey. Community based pulmonary rehabilitation has certainly expanded since 2002, from 14 centres (9%) to 39 (27%). The number of combined hospital and community programmes has also increased from 17 (11%) to 39 (27%). Most programmes run for 6–8 weeks (range 4–16) and this was similar between the two surveys. The proportion of services offering at least 2 sessions per week has improved from 64% in 2002 to 85% in 2007. The majority of courses were funded by the NHS (88% in 2002 and 79% in 2007) but often funding is not secure and there has only been a small improvement in this (57% in 2002 and 67% in 2007). Programmes with no extra funding have in fact risen from 10% in 2002 to 15% in the 2007. The number of patients attending individual programmes has increased over the past 5 years. 58 programmes (46%) now cater for >100 patients per year, compared to 23 programmes (15%) in 2002. The number of programmes providing a service to <50 patients per year has reduced from 64 (42%) to 25 (20%).
Conclusion: Pulmonary rehabilitation is a well researched, non-pharmacological treatment for COPD and has been validated as a cost effective treatment for this condition. However, it is still not universally available and there is large variability in services around the country. In this study, we show that the availability of pulmonary rehabilitation is improving in England, with programmes catering for larger numbers of patients than in 2002. However, there is still a shortfall of places on pulmonary rehabilitation programmes, when compared with the number of people diagnosed with COPD in the UK. Courses are more commonly being run in the community, which improves accessibility for patients. A larger proportion of programmes offer at least 2 supervised sessions per week, which the BTS recommends as a minimum for a programme to be effective. However, funding of these services remains a serious problem and there has only been a small improvement in the security and provision of funds by the NHS since 2002. The number of programmes with no extra funds has in fact risen since 2002 to 15% and hence the good will of staff is increasingly being relied upon to sustain these services. Our results show that despite some improvement in the provision of pulmonary rehabilitation in England, we still have some way to go before it is universally available to patients suffering with COPD. It is hoped that the National Service Framework due to be published for COPD will help to address this issue further.
THE IMPACT OF THE 2004 NICE GUIDELINE AND 2003 GENERAL MEDICAL SERVICES CONTRACT ON COPD IN PRIMARY CARE IN THE UK
R. Hubbard, C. Smith, K. Challen, J. Gribbin. University of Nottingham, UK
Introduction: The introduction of the NICE guideline on COPD and the inclusion of COPD in the new Quality and Outcomes Framework (QOF) were designed to improve the care of people with COPD in primary care in the UK. We have investigated whether these initiatives have had an impact on the recorded prevalence of COPD in general practice and the recording of spirometry data and the use of combined inhaled corticosteroid/long acting beta-agonist inhalers.
Methods: We analysed data from The Health Improvement Network (THIN) for the time period 1 year before and after the introduction of the NICE guideline. THIN is a computerised longitudinal general practice database which includes data collected as part of routine primary care.
Results: The prevalence of COPD in 2003 was 1.27%, and this increased by 14% to 1.45% in 2005. The risk of COPD was strongly related to age, male gender, socioeconomic disadvantage and living in the North of England, Scotland and Wales. People with COPD had an increased mortality compared to the general population (adjusted rate ratio for 2003 2.38, 95% CI 2.30 to 2.47). The presence of recorded spirometry data in people with COPD increased from 18% in 2003 to 62% in 2005, and FEV1 was consistently a strong predictor of survival. For example, the hazard ratio for people with COPD and an FEV1 <30% compared to general population in 2005 was 3.44 (95% CI 2.44 to 4.85). The use of combination inhalers in people with moderate to severe COPD also increased markedly during the study from 25% in 2003 to 44% in 2005.
Conclusion: Following the introduction of the NICE guideline for COPD and the new QOF there has been an increase in the prevalence of COPD in general practice and a large increase in spirometry data and prescriptions for combination inhalers. This represents significant progress for people with COPD.
GUIDELINE ADHERENCE WHEN TREATING COPD IN UK PRIMARY CARE
I. R. Small1, J. Clelland1, J. Roberts3, L. J. Small2. 1University of Aberdeen; 2Peterhead Health Centre; 3Salford Royal FT, UK
Introduction: Since the introduction of the Quality Outcome Framework (QOF; 2004), GPs and practice nurses keep COPD registers, including lung function. However, there is no requirement to categorise severity (lung function), dyspnoea or functional ability, or to record or monitor treatment. We hypothesised that the focused nature of QOF will make such clinical observations and actions less likely, even in practices with an interest in respiratory care.
Methods: We looked at routine data collected in 3 large, respiratory-interested practices. FEV1 % predicted, level of severity (by NICE/COPD Consortium Guidelines), MRC Dyspnoea Scale, and current pharmacotherapy data (ICS/LABA) were analysed using SPSS. Non-parametric tests were used given the categorical nature of the data.
Results: 730 patients were identified from a population of 46,028, a prevalence of 1.58%. 616 (84%) had had FEV1 measured as part of routine review. 349 (47.8%) had MRC Dyspnoea scale recorded. We found 56% mild, 33% moderate and 11% severe disease. 44% of patients had an MRC scale of 3 or above. In the moderate to severe group (268 patients), 217 (81%) were on ICS/LABA therapy, with 157 (72%) of that group at an appropriate/licensed dose. In patients with FEV1 50–60% predicted, we found 47% on ICS/LABA treatment at the dose licensed for more severe patients.
Conclusion: QOF has been successful in ensuring that lung function is assessed on diagnosis and review. Even respiratory interested practices do not routinely screen for dyspnoea. The primary care managed COPD population is skewed towards more significant disease. Adherence to guidelines in terms of ICS/LABA therapy is mixed, with significant levels of non-prescribing or prescribing at an unlicensed dose.
ARE INHALED CORTICOSTEROIDS BEING PRESCRIBED APPROPRIATELY IN COPD?
D. Ankers, C. Nesbitt, J. Hadcroft. Royal Liverpool University Hospital, UK
Introduction: There are clear guidelines for the prescription of inhaled corticosteroids (ICS) in COPD, namely FEV1 <50% predicted plus ⩾2 exacerbations per year (NICE 2004). The only ICS currently licensed for use in COPD are fluticasone (as Seretide 500 Accuhaler) and budesonide (as Symbicort Turbohaler). We wished to determine whether these guidelines are being adhered to or whether ICS are being prescribed inappropriately to those in whom there is no proven benefit from this treatment.
Methods: We performed a prospective case note audit of inpatients on the two respiratory wards of our city centre teaching hospital during a 2 month period. We included all those with a proven or proposed diagnosis of COPD and noted their spirometry, if available, as well as the number of exacerbations requiring steroids and/or antibiotics as recalled by the patient in the previous 12 months. We recorded the name, strength and device of ICS if prescribed and whether this prescription had been initiated in primary or secondary care.
Results: 43 patients were identified as having COPD during this period of whom 38 (88%) were prescribed ICS. 26/38 had FEV1 <50%, 20/38 had ⩾2 exacerbations per year but only 13/38 satisfied the NICE criteria for the prescription of ICS. 25/38 had been prescribed ICS inappropriately according to NICE. The level of inappropriate prescription of ICS was slightly higher in primary (11) than secondary care (7). 5/43 patients had not been prescribed ICS despite satisfying NICE criteria. Of the 13 patients who had been prescribed ICS appropriately, only 1 had been prescribed a licensed product. Of the 25 who had been prescribed ICS inappropriately, only 2 would have been receiving a licensed drug had the prescription been appropriate.
Conclusion: There are clear benefits of ICS in COPD, but these have been shown in frequent exacerbators with severe COPD. The inappropriate prescription of ICS carries implications for both the NHS and patients in terms of cost and drug side effects. Even among the group of patients with COPD in whom ICS prescription is appropriate, the choice of ICS is often not one approved by the Medicines and Healthcare Products Regulatory Agency.
DOCTORS’ ACTION AND ATTITUDE TO CURRENT SMOKERS LIMITED BY COPD OR ANGINA, COMPARED WITH PATIENTS LIMITED BY ALCOHOL OR DRUG ABUSE
L. Winstanley1, M. Daunt2, J. Macfarlane1. 1Nottingham City Hospital; 2Queen's Medical Centre, UK
Introduction: We surveyed 98 doctors (87 trainees, 12 consultants) regarding their personal views when managing patients with different health problems, who had previously all been offered relevant cessation services.
Methods: The four scenarios included: (a) current excess alcohol drinker limited by complications; (b) current cigarette smoker limited by angina; (c) current intravenous drug user limited by complications: (d) current cigarette smoker limited by chronic obstructive pulmonary disease (COPD). Each was scored on a 5 point scale from strongly disagree to strongly agree.
Results: The proportion of doctors who agreed/strongly agreed to the statement “Their current condition is largely their own fault” were: (a) 61%; (b) 60%; (c) 68%; (d) 77%. For the statement “Their future health is largely under their own control”, the results were (a) 70%; (b) 76%; (c) 72%; (d) 69%. When asked to rank the 4 groups of patients from “most to blame” to “least to blame” for their own ill health, 72% doctors ranked smokers with COPD more to blame than smokers with angina; 55% and 38% doctors ranked them more to blame than alcohol or drug abuse patients, respectively. In the last 2 weeks, 94% of doctors had managed patients who smoked, 75% had offered smoking cessation advice and 46% prescribed nicotine replacement therapy (NRT). Of the total 918 smokers seen by them, 298 (32%) had been offered cessation advice and 119 (13%) NRT.
Conclusion: Nearly 4 in 5 doctors judged the health of smokers with COPD to be largely their own fault, more so than smokers with angina and the other patients. By contrast, COPD patients who smoked were deemed least in control of their future health. Three quarters of doctors ranked COPD smokers more to blame than smokers with angina and over half more so than alcohol dependent patients. Most doctors said they offered cessation advice. However, of the near 1000 smokers they had managed recently, only a third were given cessation advice and 13% NRT; this is not surprising as only a small minority of doctors had received smoking cessation training. This study demonstrates worrying actions and attitudes towards smokers with COPD.
COMPARATIVE ASSESSMENT OF CONTINUOUS TREATMENT FOR DIAGNOSED COPD WITH TIOTROPIUM BROMIDE (TIOTROPIUM®), COMBINED IPRATROPIUM AND SALBUTAMOL (COMBIVENT®): A 12-MONTH FOLLOW-UP STUDY IN THE GENERAL PRACTICE RESEARCH DATABASE (GPRD)
J. Griffin1, S. Lee1, M. Caiado1, T. Williams3, S. Kesten1, D. Price2. 1Boehringer-Ingelheim; 2University of Aberdeen; 3GPRD, UK
Background: The National Institute of Clinical Excellence COPD guidelines consider long acting anticholinergics or short acting anticholinergics plus short acting beta-agonists as equivalent choices for bronchodilation in chronic obstructive pulmonary disease (COPD) in patients who remain symptomatic despite treatment with a single bronchodilator. A retrospective database study was undertaken to assess the comparative efficacy of continuous treatment with tiotropium bromide (Spiriva®) versus combined ipratropium and salbutamol (Combivent®) in decreasing the risk of infected exacerbation in patients diagnosed with COPD. Secondary objectives were to assess the relative risk reductions in COPD hospital referral rates, and use of salbutamol, oxygen and oral and inhaled steroid use.
Methods: The study was derived from the General Practice Research Database (GPRD) comprising 9 million UK based patients between 1987 and 2006. Logistics regression models were used to create a propensity score for each patient meeting the inclusion and exclusion criteria (diagnoses of COPD, aged 35 or over at the first prescription of study medication, treated for 12 months with either 18 μg tiotropium or 160 μg combined ipratropium and salbutamol (2 puffs four times a day), and with a minimum of 12 months of medical history in the database prior to the date of the first prescription of study medication (ie, the patient cohort entry date). Propensity score matching was used to balance prognostic covariates between the treatment groups by identifying patient with similar baseline characteristics. The following covariates were used to fit logistic regression models and to create a propensity score for each patient who met the inclusion and exclusion criteria: age, BMI, smoking status, comorbidity (asthma, cardiovascular disease, diabetes and osteoporosis), history of infected exacerbation and COPD-related referrals, COPD medication history prior to initiation of the study treatment, and exposure to concomitant COPD medication. Patients identified by the propensity score matching contributed to the cohort for the outcome evaluations. Incidence rate ratios and 95% confidence intervals for the 12 month follow-up period were derived for each study cohort. Infected exacerbations were defined as an inclusion code relating to lower respiratory tract infection treated with either oral steroid or antibiotics for no more than a 4 week duration.
Results: 3385 and 808 patients treated with tiotropium and combined ipratropium and salbutamol respectively met the inclusion and exclusion criteria. Tiotropium treated patients had significantly more comorbidities, more infected exacerbations, hospital referrals and higher usage of COPD medications in the 12 month prior to entering the study cohort than combined ipratropium and salbutamol treated patients. Propensity score matching successfully adjusted for the imbalances in the two cohorts with 1308 tiotropium treated patients and 654 combined ipratropium and salbutamol treated patients identified for inclusion in the final analysis (see table for statistically significant parameters).
Conclusion: Our findings indicate that the continuous use of tiotropium is associated with a decreased risk of infected exacerbation and COPD-related hospital referrals compared to the use of the combination of ipratropium and salbutamol for the treatment of COPD.
END OF LIFE PLANNING FOR SEVERE COPD: A PILOT STUDY
A. Matthews1, H. Broomfield2, C. Potter2, R. Kennedy2, A. Dinham2, L. Restrick2, M. Brennan1, M. Stern2. 1Haringey Palliative Care Team; 2Dept Respiratory Medicine, Whittington Hospital, London, UK
Introduction: Predicting survival for patients with severe COPD is extremely difficult and it is not clear whether severe but stable COPD patients should be offered formal palliative care input. Studies have suggested that ∼50% of COPD patients would like to discuss end of life issues and felt that they benefited if offered the opportunity (Knauft et al 2005, Jones et al 2004). The Whittington Chronic Respiratory Support (CRS) team cares for patients with severe COPD who have had >2 admissions per year (annual mortality 17%). As part of an existing collaboration with Haringey Community Palliative Care Team, CRS patients were offered the opportunity to have a home visit from a palliative medicine doctor and a member of the CRS team (respiratory nurse specialist or physiotherapist) for a patient-led discussion about end of life issues. This study was undertaken to pilot this service development.
Methods: Visits were offered (in person at home by a CRS team member) to all CRS patients without cognitive impairment. A leaflet outlining the purpose of the visit and examples of issues they may wish to discuss was given. Visits were arranged within 2 weeks for those accepting. All discussions were recorded by the palliative care doctor in a letter, summarising any advance-care plans. Once read and agreed by the patient, copies were held by the patient, GP and hospital notes. Uptake and outcomes of the offer was prospectively measured and a thematic analysis of the letters undertaken. A patient feedback questionnaire was administered by the CRS team member at the end of the study to ascertain patients’ experience of the intervention.
Results: Of 62 patients under CRS, 52 were invited to take up the offer (10 unsuitable: cognitive impairment or medical instability). 33 patients (63%) declined. Of 19 accepting, 4 subsequently cancelled (2 changed mind, 1 too unwell, 1 died). 15 visits took place. 3 recurrent themes emerged: cardiopulmonary resuscitation (CPR), non-invasive ventilation (NIV) and intensive care (IC). 12 patients (80%) discussed CPR; none had a clear understanding of what it involved. 3 believed a DNAR decision would preclude treatment in the A&E resuscitation room. 6 patients wanted CPR unless they were known to be dying, 4 would want if offered and 2 said they would not want it. 4 patients had NIV previously; all described it as distressing. 3 would accept it again but 1 was unsure. 6 patients had not had it but would want it if offered. 9 (60%) patients discussed IC although only 2 had direct experience; of these, 1 would definitely accept again but 1 was unsure. The other 7 would want IC care if offered. Other issues discussed included place of care: all patients wanted to be admitted to hospital if they deteriorated. 3 patients requested respite admissions to the hospice and 3 explored fears about dying. 14/15 (93%) of patients returned the feedback questionnaire. 13/14 found the experience valuable, providing the opportunity for asking questions, although 3/14 (21%) found the discussion upsetting. 6/14 made decisions as a result of the discussion, while 4/14 felt that something important changed in their life as a result.
Conclusion: Approximately 1/3 of CRS patients took up the opportunity to have a visit from a palliative care specialist. The visits provided a valuable insight into patients’ wishes, understanding and expectations, particularly of CPR, NIV and IC. The patients’ past experiences had a great bearing on their future choices. Resuscitation in particular was poorly understood. In contrast to other studies, the preferred place of care and of death for these COPD patients was hospital. Local guidelines for the ongoing provision of end-of-life planning for patients with severe COPD are being drafted as a result of this study.
DETERMINANTS OF FATIGUE IN STABLE CHRONIC OBSTRUCTIVE PULMONARY DISEASE
R. Baghai-Ravary, J. K. Quint, J. J. P. Goldring, J. R. Hurst, G. C. Donaldson, J. A. Wedzicha. University College London, UK
Background: Fatigue is a common symptom in COPD but determinants of fatigue are not well understood. We investigated the relationship between fatigue in stable COPD and markers of disease severity.
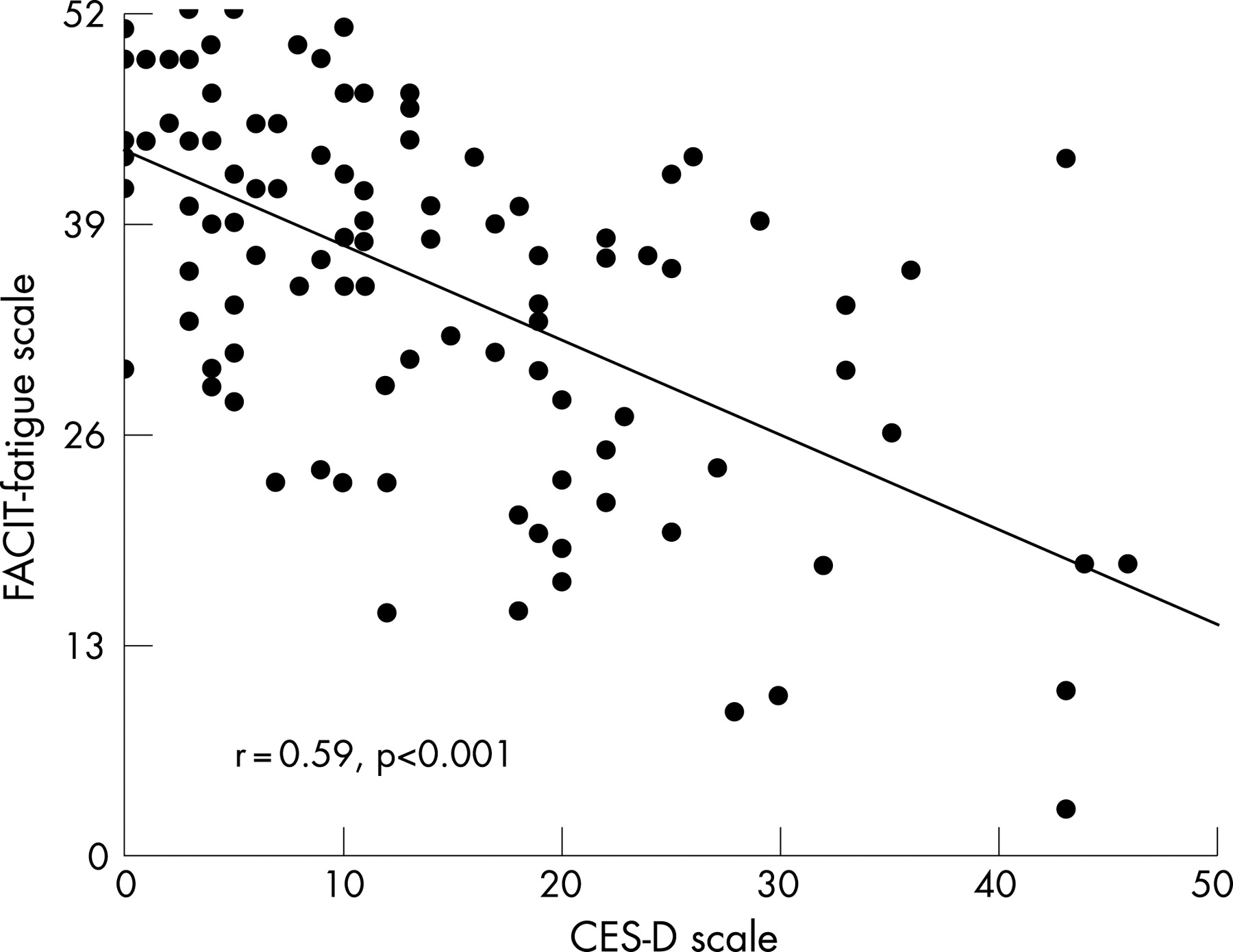
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
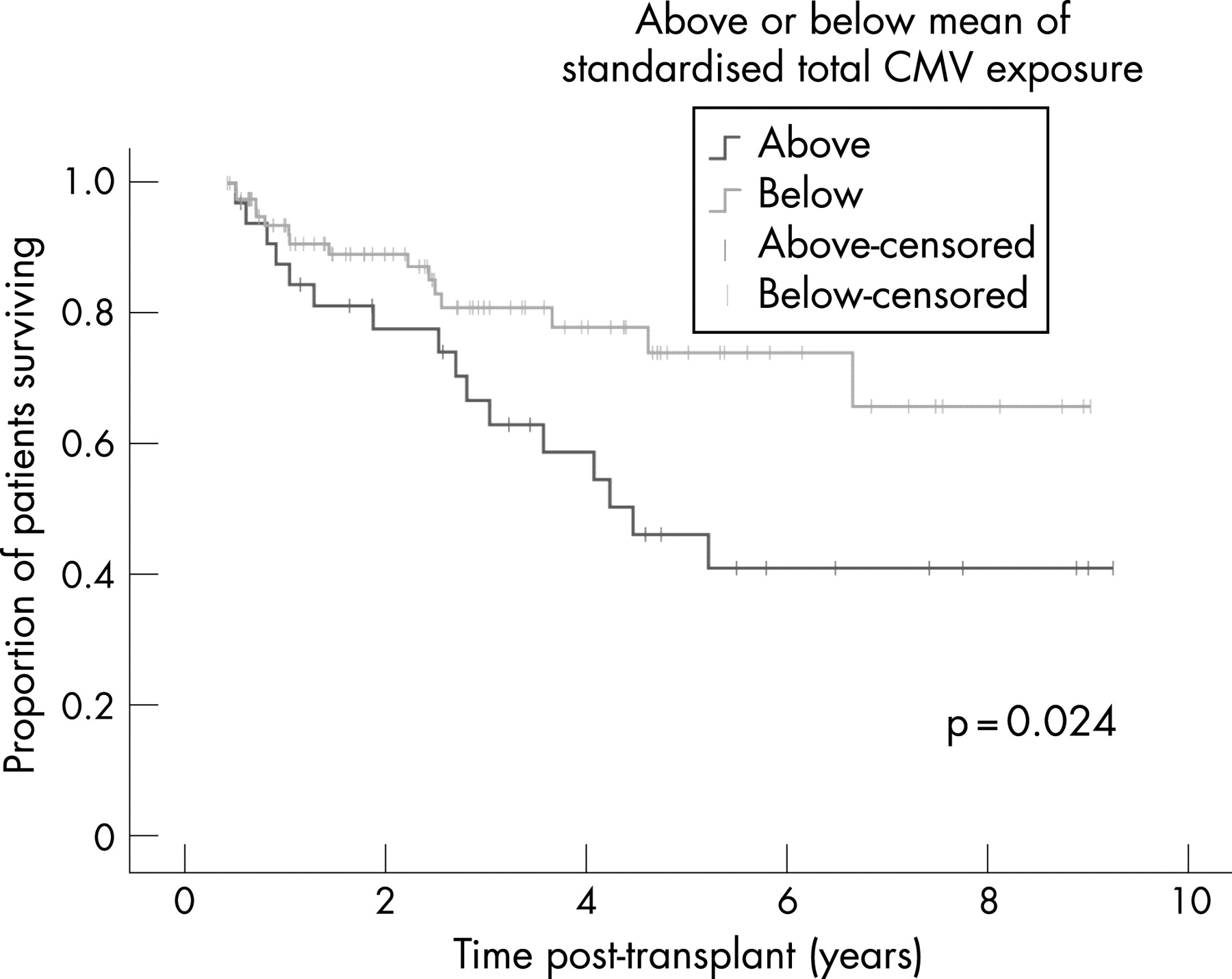{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
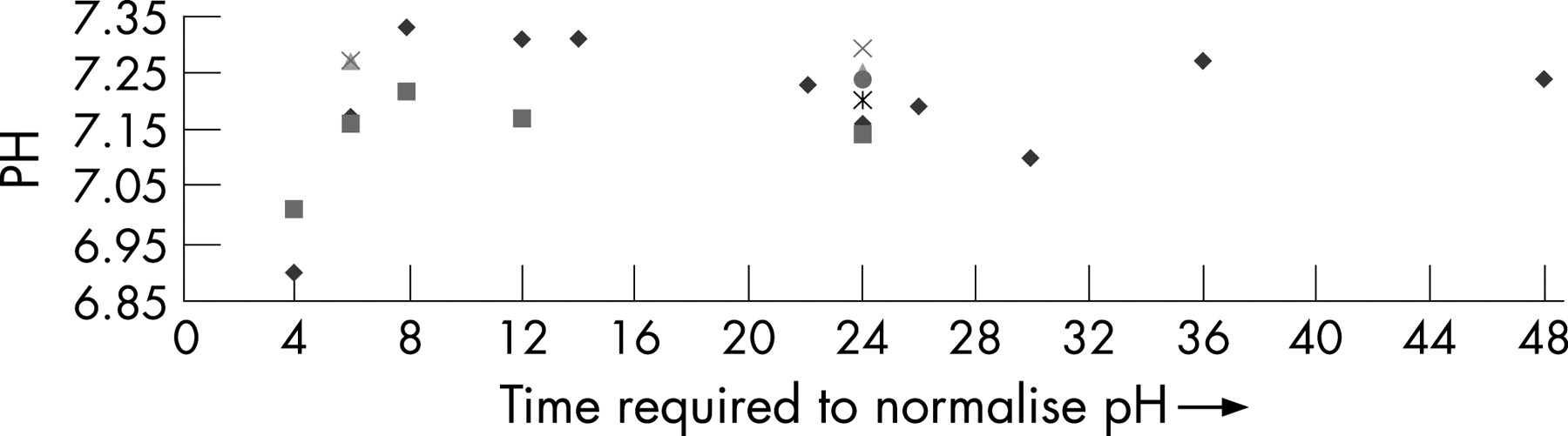{kind=link}
{kind=link}
{kind=link}
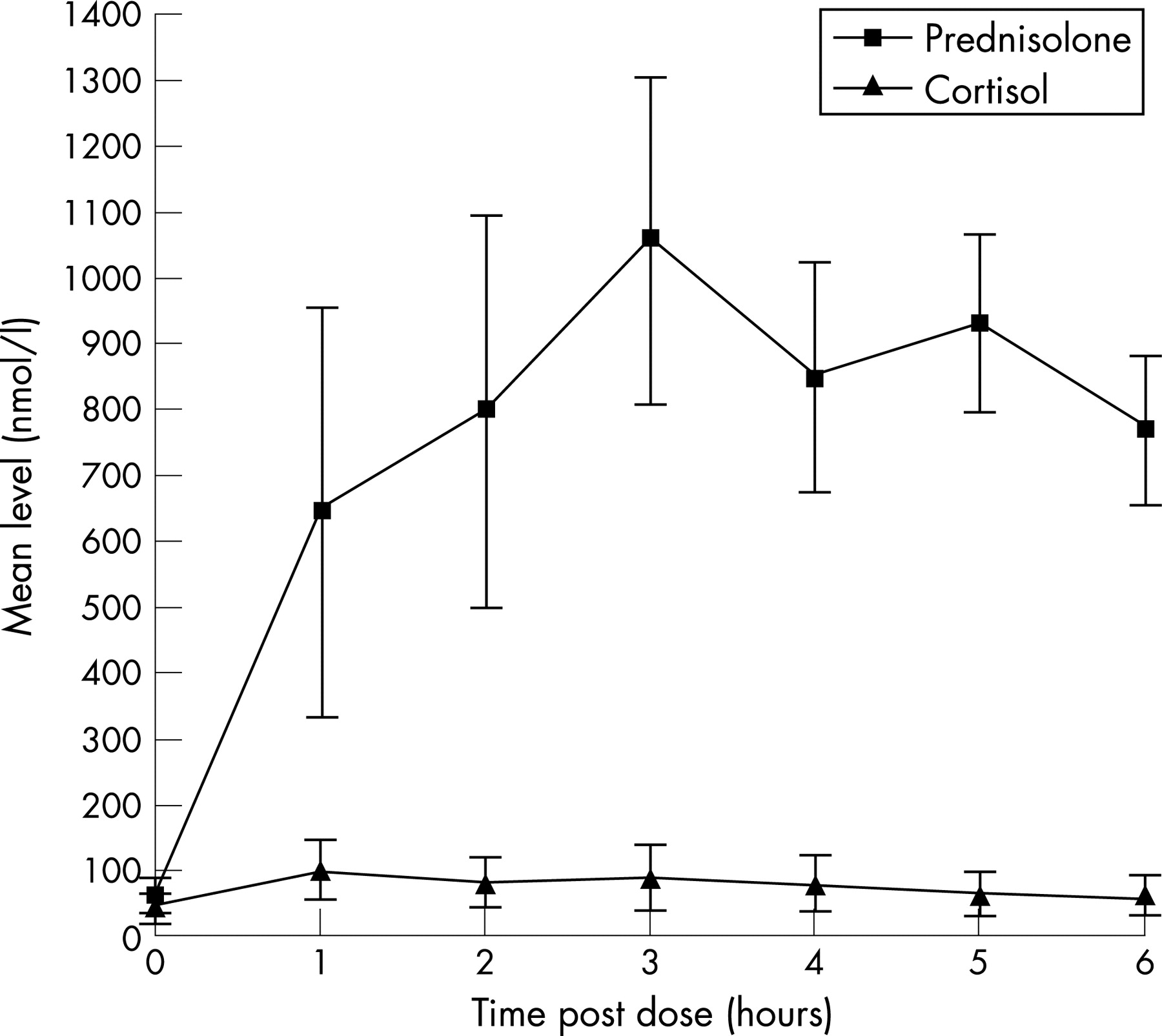{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
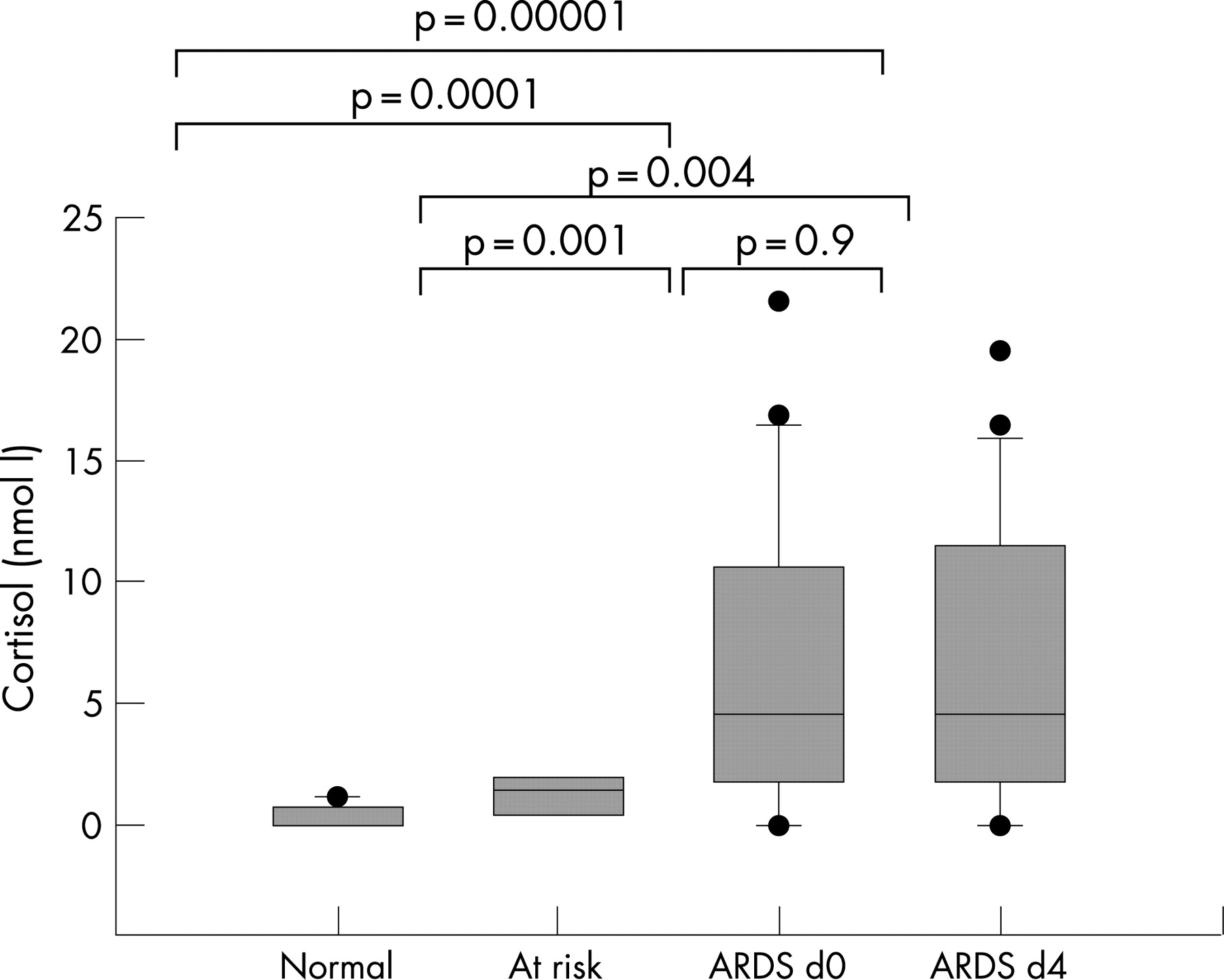{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
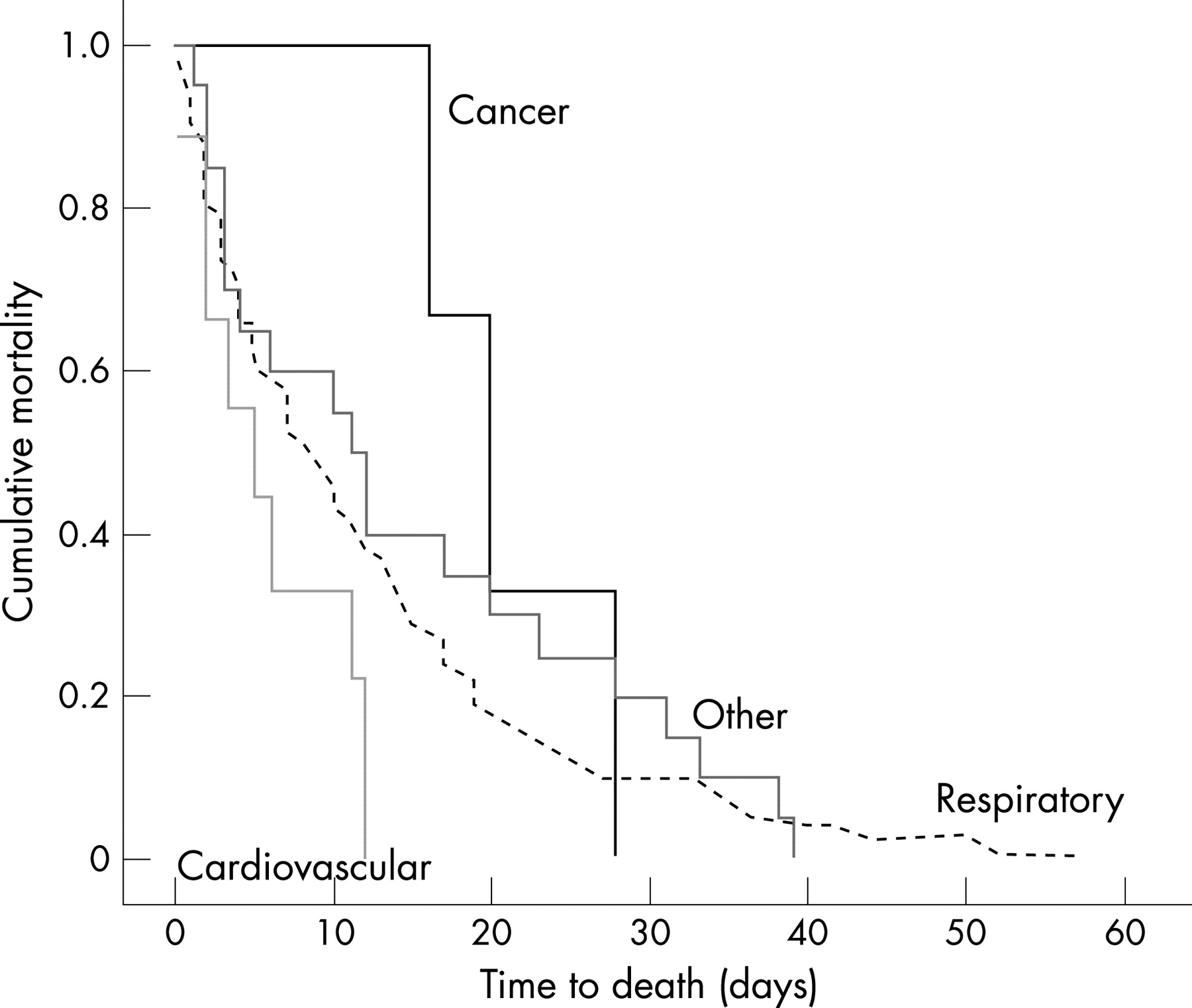{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
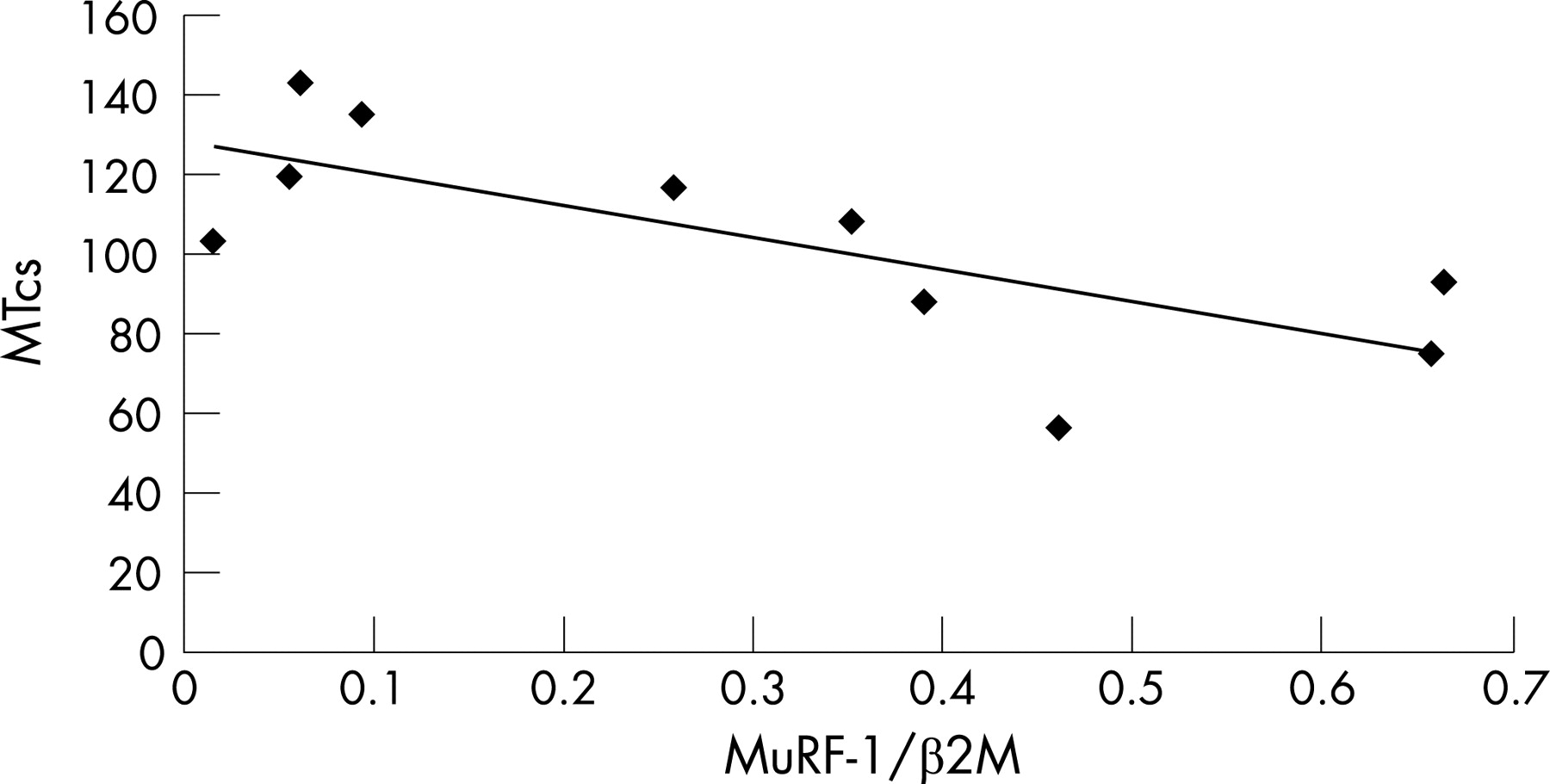{kind=link}
{kind=link}
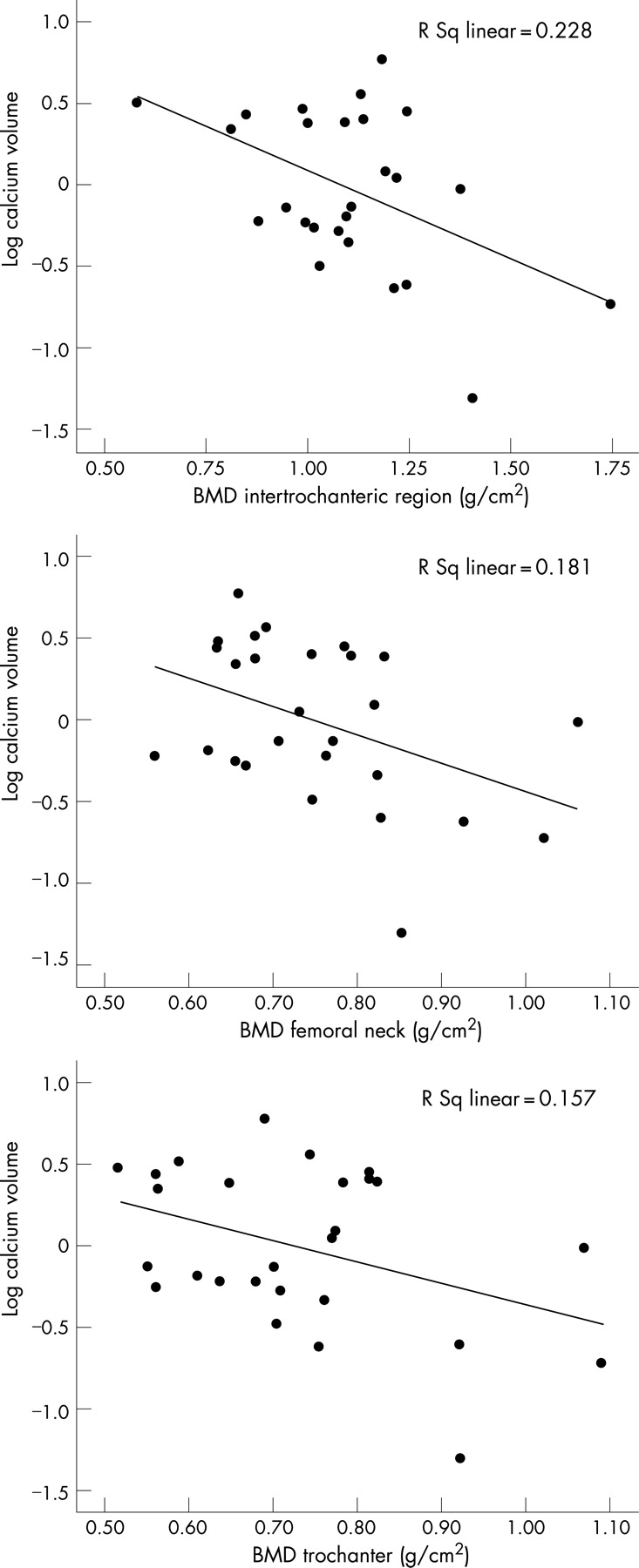{kind=link}
{kind=link}
{kind=link}
{kind=link}
Methods: 107 COPD patients (64 male) from the London cohort were examined when clinically stable, at least 4 weeks from the onset of an exacerbation. Fatigue was assessed with the validated Functional Assessment of Chronic Illness Therapy-Fatigue Scale (FACIT-Fatigue). History of comorbidity (ischaemic heart disease (IHD), hypertension, OA, RA, congestive heart failure) was noted. Exacerbations were diagnosed as one major plus another respiratory symptom on two consecutive days. Daily time outdoors recorded on diary cards was averaged over 3 days before and after assessment. Patients had an assessment of dyspnoea (MRC scale and 10 cm Visual Analogue Scale, VAS), depression (CES-D), quality of life (SGRQ). Spirometry, Sao2, and a 6 minute walk test were measured.
Results: Patients had a mean (SD) age of 69.3 (8.2) years, FEV1 1.3 l (0.6), FEV1 53.1 (21.1)%, BMI 25.7 (5.4) kg/m2, VAS 4.4 (2.3) cm, FACIT-Fatigue 35.3 (11), CES-D 14 (11.2), total SGRQ 49.2 (11), daily time outdoors 4.3 (2.8) hours and a 6 minute walking distance of 306.2 (86.7) m. Median resting Sao2 was 95% (IQR 94–96). Increased fatigue (lower FACIT-Fatigue) was significantly related to increased perception of dyspnoea by MRC (ANOVA p<0.001) and VAS (r = −0.34; p<0.001), reduced time outdoors (r = 0.41, p = 0.004), reduced quality of life (r = −0.61, p<0.001) and higher depressive symptoms score (r = −0.59, p<0.001). A CES-D score consistent with clinical depression (CES-D⩾16) was related to more fatigue 27.6 (10.7) compared with 40.0 (8.4) (p<0.001). Patients with a history of IHD were more fatigued 30.0 (13.5) compared with 36.2 (10.4) (p = 0.04). Frequent exacerbators (⩾3 per year) had a lower FACIT-Fatigue 32.6 (11.7) compared to 36.8 (10.5) (p = 0.06). No association was seen with other comorbidities, spirometry, Sao2, or 6 minute walking distance (p>0.05).
Conclusion: Fatigue is associated with a number of parameters in COPD, and monitoring fatigue could be important.
CLINICAL FEATURES USED BY HOSPITAL PHYSICIANS TO DIAGNOSE COPD AND CONCORDANCE WITH ACCEPTED DIAGNOSTIC CRITERIA
I. White, S. Murphy, V. Dudzevicius, V. Dudzevicius, N. Krishnaraj. James Cook University Hospital, Middlesbrough, UK
Background: Most patients admitted to hospital with exacerbation of COPD are treated by non-respiratory physicians. The purpose of this study was to ascertain clinical features accepted by physicians as diagnostic of COPD.
Methods: Physicians (all grades) in a university hospital with approximately 1000 admissions/year for COPD were asked to complete a questionnaire on COPD diagnosis.
Results: 54.5% (18/33) consultants and 58% (43/74) junior doctors completed questionnaire. The following were considered diagnostic of COPD: (A) Symptoms of dyspnoea/productive cough and wheeze in a current/ex-smoker (47.5%); (B) Cough productive of sputum most days for 3 months in 2 consecutive years (68.8%); (C) Symptoms of chronic bronchitis with hyperinflation on CXR (64%); (D) Previous documentation of COPD (38%); (E) Irreversible airflow obstruction on spirometry in smoker/ex-smoker (90%). Opinion varied between respiratory and non-respiratory physicians (see table).
Conclusion: Non-respiratory physicians are more likely than respiratory physicians to diagnose COPD without spirometric evidence of airflow obstruction.
AN INTEGRATED RESPIRATORY TEAM SPANNING PRIMARY AND SECONDARY CARE CAN REDUCE HOSPITAL ADMISSIONS AND GP CONSULTATIONS FOR COPD
S. J. Perrott1, N. J. Pott2, R. Mahadeva1. 1Cambridge University Hospitals NHS Trust; 2Cambridgeshire PCT, UK
Introduction: Chronic obstructive pulmonary disease (COPD) is a major source of morbidity, mortality and health resource usage in primary and secondary care. COPD affects 4–6% of adults in Europe and accounts for 10% of medical admissions in the UK, accounting for over 90,000 admissions to hospital annually. Mortality related to exacerbations of COPD is high. Early identification and treatment of exacerbating patients, thus avoiding some hospital admissions, can be seen to be essential to the health of patients and the NHS due to high financial cost implications.
Methods: In order to deal with increasing demand on secondary care services an Integrated Specialist Respiratory Service has been developed between Cambridgeshire PCT and Cambridge University Hospitals NHS Trust. Cambridge City and South Cambs area has a population of 250,000 and is served by one acute Trust. The Integrated Respiratory Team of specialist nurses and physiotherapists have a hospital based respiratory consultant lead clinician and provide early supported discharge and admission avoidance for COPD patients. The aim of the new service is to increasingly centre care within the community. Furthermore, by linking closely with secondary care utilising an intensive case management approach in complex, severe COPD patients, early detection of deterioration and timely appropriate management is possible.
Results: Data collected between November 2006–April 2007 demonstrated 122 potential admissions or GP consultations avoided by successful management of the exacerbation or crisis within the community. Feedback from patients was extremely positive. It is difficult to know the exact proportion of patients that would have been admitted to hospital without our new service, but a conservative estimate based on 50% admission avoidance would equate to potential cost savings of over £85,000 to the PCT over 6 months.
Conclusion: Hospital admissions and GP consultations can be avoided in COPD patients if specialist teams are placed within the community supported by close links with secondary care respiratory clinicians, hospital based respiratory nurses, general practitioners and locality teams (district nurses, occupational therapists, social workers). Service redesign using this type of model has the potential to provide the patient with the appropriate care, by the appropriate person, in the appropriate place at the appropriate time.
REMOTE DAILY REAL TIME MONITORING OF SYMPTOMS IN PATIENTS WITH COPD: MOBILE TECHNOLOGY AND EXACERBATIONS (MOTEX) STUDY
Z. M. Garland1, T. Powell1, E. Larsen2, N. O'Brian2, N. A. Jarad1. 1Bristol Royal Infirmary; 2t+ Medical, UK
Background: A paper diary has been used previously in managing COPD patients. In this method, exacerbations not presented by patients are diagnosed after the events. We examine the use of a real time remote electronic diary as a means of early identification and management of COPD exacerbations.
Methods: Eighteen patients completed the study. The mean age was 66.1 years and mean FEV1 was 1.05 litres (range 0.4–1.82). Basic demographic data, respiratory symptom score and spirometry were collected at the start and end of the study. Patients were provided with an Xda II (O2 Telecommunications) attachable to a hand held spirometer (Vitalograph). The software on the Xda II was written by e-san Limited (Oxford) with specifications identified by us. Patients were asked to score their respiratory symptoms (sputum colour/volume, breathlessness and fatigue) once daily. Patients then answered whether they underwent GP/hospital consultations or changed any medication that day (yes or no). Finally, an FEV1 and PEF measurement was recorded. The data were then electronically sent to a secure server where it was viewed daily on real time over 6 months. Baseline symptoms and FEV1 were identified at a 2 week exacerbation-free run in period. The system detected exacerbations when there was an increase in 2 or more symptoms with or without a 10% decline in FEV1 or only a 10% decline in FEV1, all over 2 successive days.
Results: A total of 90 exacerbations were recorded whereby 48 (53%) were detected by the system and by patients, 28 (31%) by patients but not the system, and 14 (16%) by the system but not the patients. From the start to the end of the study mean (SD) FEV1 increased from 1.05 (0.09) to 1.12 (0.09) litres (p = 0.022). Similar results were obtained for FVC. Symptom score improved or remained unchanged in 11/18 (61%) patients. Patients expressed satisfaction with using the device as a method of monitoring their symptoms.
Conclusion: Patients with severe COPD are able to electronically record their symptoms daily and are happy to do so. Exacerbations detected were probably excessive but FEV1 and FVC improved. This study confirms that remote daily monitoring of symptoms and basic spirometry in severe COPD patients is possible.
DEPRESSION AND COPD
H. Bakere, A. Jeyabalan, S. Iles. Royal Cornwall Hospital, UK
Introduction: Around 20% of patients with chronic obstructive airways disease suffer from anxiety and depression. COPD is a heterogeneous disease; within secondary care the population seen in different settings may have different characteristics. We compared the incidence of anxiety and depression in inpatients and outpatients at a district general hospital, and those attending a community based pulmonary rehabilitation programme, using the hospital anxiety and depression score and the prime MD (PHQ-9) depression score.
Methods: During the period August 2006–August 2007 participants in each setting completed the questionnaires. Social and clinical characteristics were also recorded. Standard scoring values for the questionnaires were used.
Results: 79 participants were studied: 36 inpatients, 26 outpatients and 17 pulmonary rehabilitation attendees. Using the HAD score, 10 participants (12%) had a score suggestive of an anxiety disorder and 14 (17%) had a score suggestive of a depressive disorder. 26 (32%) participants had at least moderate depression using the Prime MD score. The characteristics of the participant groups and the levels of depression and anxiety are show in the table.
Discussion: There is a high prevalence of anxiety and depression in those with COPD, which is probably under identified as suggested by the low numbers receiving treatment. Of 26 patients identified by the prime MD score as having at least moderate depression, only 5 were on treatment for depression. There are important differences between patient groups. Inpatients tend to be older with more advanced disease and have a higher prevalence of depression. The pulmonary rehabilitation group and outpatient group were similar but depression is less common in those attending pulmonary rehabilitation. We postulate that pulmonary rehabilitation has a positive effect on the declared symptoms of anxiety and depression as assessed by the scoring methods used.
Conclusion: This study confirms that depression and anxiety are a problem for those with COPD in this typical district hospital. Inpatients are the most at risk and both inpatients and outpatients are probably under treated. Pulmonary rehabilitation may be protective. When we think of COPD as a systemic disease we should not forget the mental health impact.