Article Text

Abstract
Background: Endothelial injury is an important prognostic factor in acute respiratory distress syndrome (ARDS). Vascular endothelial growth factor (VEGF) plays a critical role in endothelial destruction and angiogenesis. Genetic variations of the VEGF gene have been associated with VEGF production. A study was undertaken to investigate the impact of VEGF gene polymorphisms on the clinical outcomes of ARDS.
Methods: Three VEGF polymorphisms (−460C/T, +405C/G and +936C/T) were determined in 1253 patients in an intensive care unit with risk factors for ARDS, 394 of whom developed ARDS. Patients were followed for assessment of 60 day survival. Plasma VEGF levels were measured in 71 patients with ARDS.
Results: The +936TT (OR 4.29, 95% CI 1.12 to 16.40, p = 0.03) and +936CT+TT (OR 1.98, 95% CI 1.14 to 3.42, p = 0.01) genotypes were significantly associated with increased mortality from ARDS. Plasma VEGF levels in patients with ARDS with the +936CT+TT genotype were significantly lower than in subjects with the +936CC genotype (median 49 (IQR 16–98) pg/ml vs 112 (IQR 47–162) pg/ml, p = 0.02). At the haplotype level, haplotype TCT (−460T+405C+936T) was significantly associated with a higher rate of mortality (OR 2.89, 95% CI 1.30 to 6.43, p = 0.009) and haplotype CGT (−460C+405G+936T) was associated less strongly with increased mortality (OR 1.90, 95% CI 0.94 to 3.83, p = 0.07) in patients with ARDS. Lower plasma VEGF levels were correlated with the probability of haplotype CGT (coefficient = −0.26, p<0.05), but the same trend of correlation was not significant to haplotype TCT.
Conclusions:VEGF polymorphisms may contribute to the prognosis and inter-individual variations in circulating VEGF levels in patients with ARDS.
- ARDS, acute respiratory distress syndrome
- SNP, single nucleotide polymorphism
- VEGF, vascular endothelial growth factor
Statistics from Altmetric.com
- ARDS, acute respiratory distress syndrome
- SNP, single nucleotide polymorphism
- VEGF, vascular endothelial growth factor
Acute respiratory distress syndrome (ARDS) is lung injury characterised by alveolar injury and increased pulmonary vascular permeability.1,2 The pathogenetic basis of ARDS is incompletely understood; however, emerging evidence has suggested that the severity and outcome of ARDS depend significantly on the balance between alveolar epithelial and/or vascular endothelial injuries and their repair mechanisms.2–6
Vascular endothelial growth factor (VEGF) is an endothelial cell-specific mitogen that promotes angiogenesis and mediates vascular permeability.6,7 Overexpression of VEGF in the lungs induces increased pulmonary vascular permeability resulting in pulmonary oedema.8 However, VEGF expression in human lung epithelial cells can also increase neovascularisation, thereby contributing to the repair of endothelial injuries.6,9 In human lungs, low levels of VEGF were associated with the severity of ARDS while raised VEGF levels were associated with recovery from ARDS, indicating a role for VEGF in the repair process of lung injury.10–13
The VEGF gene is located on chromosome 6p31.3. Several functional single nucleotide polymorphisms (SNPs) in this gene have been described in the literature. The +936C/T polymorphism (rs3025039) has been related to lower levels of plasma VEGF,14,15 whereas the −460C/T (rs833061) and +405C/G (rs2010963) polymorphisms have been shown to significantly increase VEGF production.16 Recent studies have indicated that these three SNPs are implicated in the risk of several disorders in which vascular injury and acceleration of inflammation are critical in disease development.17,18 However, the combined effect of these polymorphisms on the prognosis of ARDS has not been evaluated. Based on the biological function of these three VEGF polymorphisms on VEGF production and the pathological significance of VEGF in ARDS, we hypothesised that VEGF polymorphisms may contribute to the poor outcomes in ARDS, and correlate with circulating VEGF levels in patients with ARDS.
METHODS
Study subjects
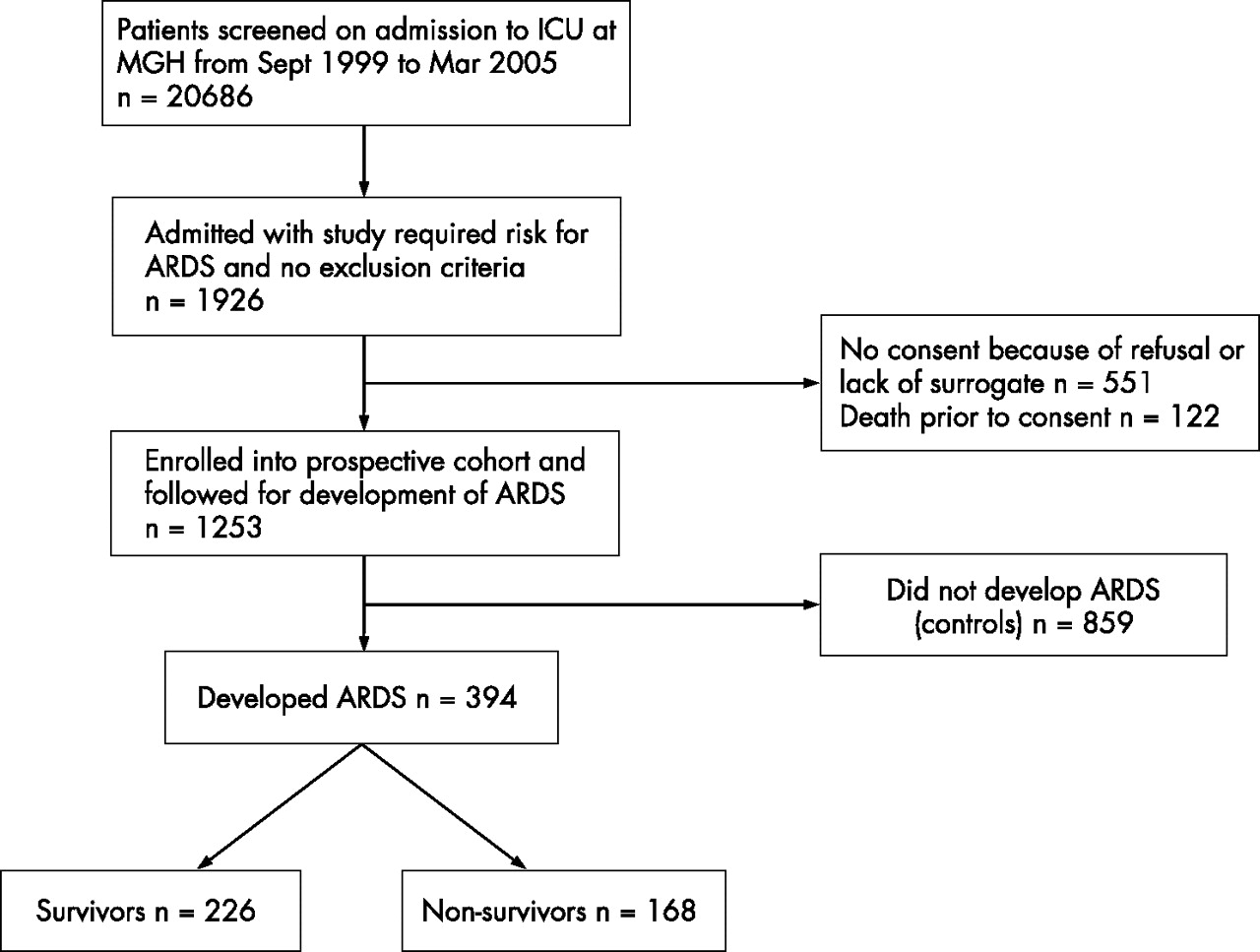
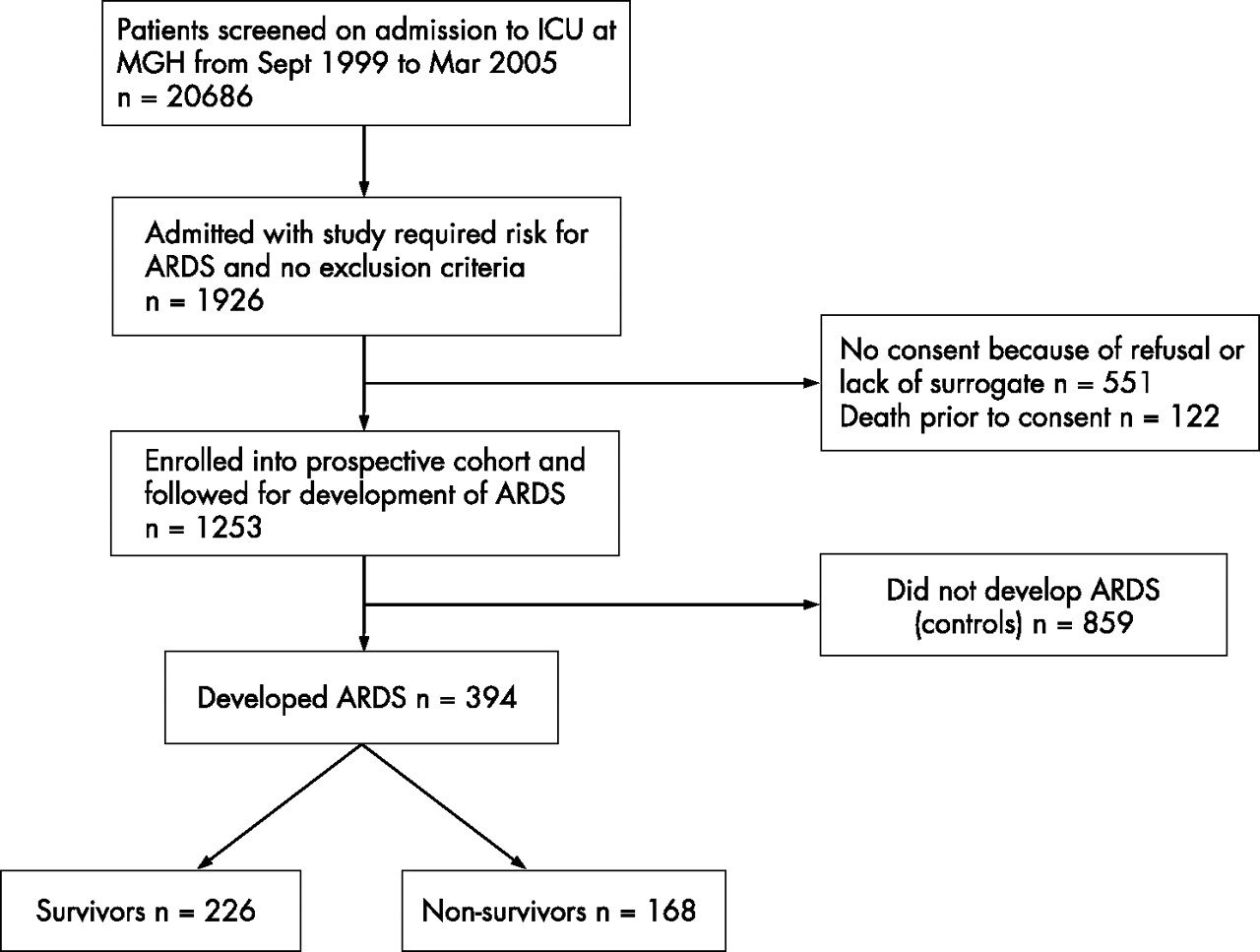
The present study was part of an ongoing research investigating the effects of multiple genetic variants on the risks or prognosis of ARDS. Recruitment of subjects was started in September 1999 and will continue until 2010. Details of the study have been described previously.19,20 Briefly, all admissions to the intensive care unit (ICU) at Massachusetts General Hospital were screened daily for study-defined clinical risk factors for ARDS such as sepsis, trauma, aspiration or massive transfusions and were followed prospectively during their stay in the ICU for the development of ARDS (fig 1). Subjects were classified as having ARDS if they were intubated on positive ventilation and met the American European Consensus Committee (AECC) criteria for ARDS: (1) arterial oxygen tension/fraction of inspired oxygen ratio of ⩽200 mm Hg; (2) bilateral infiltrates on chest radiographs; and (3) pulmonary arterial occlusion pressure ⩽18 mm Hg or no clinical evidence of left atrial hypertension. All cases of ARDS were followed for all-cause 60 day mortality. The study was approved by the Human Subjects Committees of Massachusetts General Hospital and the Harvard School of Public Health, Boston, and informed written consent was obtained from all subjects or their appropriate surrogates.
{kind=link}
Flow diagram of study design and patient selection for the case-control study. ICU, intensive care unit; MGH, Massachusetts General Hospital, Boston, Massachusetts, USA. Patients who had a previous history of acute respiratory distress syndrome (ARDS) and those who had previously been admitted to the ICU were excluded from being controls. The subjects were all Caucasians. Non-Caucasians were also enrolled but they were excluded from the analysis because they accounted for only 4% of all enrolment.
DNA isolation and genotyping assays
Genome DNA was extracted from peripheral blood samples using the Puregene DNA Isolation Kit (Gentra Systems, Minneapolis, Minnesota, USA) following the manufacturer’s protocol. The allelic discrimination of the VEGF gene was assessed with the ABI PRISM 7900 Sequence Detection System (Applied Biosystems, Foster City, California, USA) using the fluorogenic 5′ nuclease assay with Taqman Minor Groove Binder (MGB) probes. The wide-type Taqman MGB probes were FAM-labelled and the mutant probes were VIC-labelled. The primers and probes for the −460C/T, +405C/G and the +936C/T polymorphism assays were ordered from Applied Biosystems. Genotyping was performed by laboratory personnel blinded to subject status, and a random 10% of the samples were repeated to validate genotyping procedures. Two authors reviewed independently all genotyping results.
Analysis of VEGF levels in plasma
Plasma samples from day 2 after development of ARDS were available from 71 patients for the measurement of circulating VEGF levels. Blood samples were collected in 10 ml vacuum tubes and centrifuged for 10 min. Plasma samples were stored at −80°C until analysis. Plasma VEGF levels were quantified in duplicate according to the manufacturer’s recommendations with a commercially available ELISA kit (R&D Systems, Minnesota, USA). No statistically significant differences were observed between patients with plasma samples and those without plasma samples in terms of age, sex, APACHE III and risk factors for ARDS.
Statistical analysis
The demographic variables between different groups were compared by χ2 tests for categorical variables and by the Student t test and/or non-parametric test for continuous variables. The Hardy-Weinberg equilibrium was evaluated using the χ2 test. A logistic regression model was used to assess the effect of VEGF polymorphisms on the mortality of patients with ARDS, with adjustments for potential confounding factors such as age, sex, APACHE III score, diabetes, history of steroid use, number of units of red cells transfused and chronic liver disease. Linkage disequilibrium between the SNPs, haplotypes and their frequencies was estimated using the expectation maximisation algorithm. Association between haplotypes and the risk of ARDS was assessed using an “expectation substitution” approach to account for unknown phase.21 Haplotypes were coded as an additive fashion. Mortality from ARDS was regressed on haplotype counts by logistic regression, using the most common haplotype as the reference haplotype. The multiple Cox regression model was applied to test the effect of the VEGF polymorphisms on overall survival, adjusting for confounding factors such as age, sex, APACHE III score, diabetes, history of steroid use and chronic liver disease. The correlations between haplotype probabilities and plasma VEGF levels were estimated by the Spearman correlation test. All statistical analyses were performed using the SAS statistical software package Version 9.1 (SAS Inc, Cary, North Carolina, USA).
RESULTS
Patient population
Between September 1999 and March 2005, 1253 Caucasian patients with risk factors of ARDS were enrolled into the prospective cohort. In this study population, 394 (31.4%) were diagnosed as having ARDS and 859 did not develop ARDS (fig 1).
Clinical risk factors for ARDS and baseline characteristics between subjects with and without ARDS are shown in tables 1 and 2 in the online data supplement (available at http://thorax.bmj.com/supplemental). Among the 394 patients with ARDS studied, the 60 day mortality was 42.6% (168/394). Logistic analysis showed that older age, APACHE III, steroid use, haematological failure and liver disease were the major prognostic factors for survival (table 1).
Characteristics of survivors and non-survivors among patients with ARDS
Associations of VEGF genotypes and mortality from ARDS in all patients (n = 394)
VEGF genotypes in relation to ARDS mortality
Genotyping of the −460C/T, +405 C/G and +936 C/T polymorphisms was successfully achieved for all subjects and followed the Hardy-Weinberg equilibrium. The genotype frequencies of these three polymorphisms in the current study were broadly similar to those reported by others in Caucasian populations.22–28 When overall cases of ARDS were compared with patients without ARDS, no significant difference was found in the distribution of genotypes for any polymorphisms studied (p>0.05).
We tested for an association between mortality from ARDS and any of the three SNPs among the 394 patients with ARDS (table 2). No significant association was found between the −460C/T or +405C/G polymorphisms and the risk of mortality in patients with ARDS (p>0.05), but the +936TT genotype was significantly associated with a higher mortality from ARDS than the +936CC genotype (adjusted OR 4.29, 95% CI 1.12 to 16.40, p = 0.01). A similar association was also observed for the +936CT genotype, but this association was not statistically significant (adjusted OR 1.60, 95% CI 0.90 to 2.80, p = 0.10). When the mutant +936TT and +936CT were combined to form a united genotype, this combined +936CT+TT genotype was significantly associated with increased mortality compared with the +936CC genotype (adjusted OR 1.98, 95% CI 1.14 to 3.42, p = 0.01). No significant interactions between any genotypes and age, sex or types of injury were detected.
Association between VEGF haplotypes and ARDS mortality
Haplotype analyses were conducted to evaluate the combined effect of the three polymorphisms on survival in patients with ARDS. Consistent with observations from early studies,29VEGF −460C/T and +405C/G polymorphisms in our study were in strong linkage disequilibrium (correlation coefficient (R) = 0.68, Lewontin’s D′ (D′) = 0.99), whereas their linkage with the +936C/T polymorphism was much weaker (R = 0.04, D′ = 0.1 and R = 0.1, D′ = 0.20, respectively). Six haplotypes with frequencies >1% were estimated of the eight possible haplotypes (table 3). Interestingly, the −460T+405C+936T (TCT) haplotype was significantly associated with an increased risk of mortality from ARDS (adjusted OR 2.89, 95% CI 1.30 to 6.43, p = 0.009), and the −460C/+405G/+936T (CGT) haplotype was marginally significantly associated with a higher risk of mortality from ARDS (adjusted OR 1.90, 95% CI 0.94 to 3.87, p = 0.07). No associations were found between other haplotypes and mortality from ARDS in this study population.
Associations between VEGF haplotypes and ARDS mortality
Relationship between VEGF polymorphisms and plasma VEGF levels
To investigate the relationship between VEGF polymorphisms and circulating VEGF levels, plasma VEGF levels were categorised according to VEGF polymorphisms. Since the plasma levels of VEGF were not normally distributed (Kolmogorov-Smirnov test, p = 0.01), a non-parametric median two-sample test was used to compare the VEGF levels between different genotype carriers. The median (interquartile range) plasma VEGF level in individuals carrying the +936CT+TT genotype was significantly lower than that in individuals with the VEGF+936CC genotype (49 (16–98) pg/ml vs 112 (47–162) pg/ml, p = 0.02). Based on the sample sizes and median plasma VEGF levels between the +936CT+TT and the VEGF+936CC carriers, the power to detect a difference at α = 0.05 level was calculated to be 99%. At haplotype levels, the plasma VEGF levels were inversely correlated with haplotype CGT probability (Spearman coefficient −0.26, p<0.05). A similar correlation was also observed between plasma VEGF levels and the haplotype TCT probability, but this correlation did not reach statistical significance (coefficient −0.14, p = 0.26). Thus, haplotypes containing the 936T allele tended to correlate with lower plasma VEGF levels. There was no significant difference between survivors and non-survivors in plasma levels of VEGF (p>0.05).
Association between VEGF polymorphisms and ARDS survival
The Cox proportional hazard model was used to analyse the associations between VEGF polymorphisms and survival in patients with ARDS. After adjusting for other predictors of survival (age, sex, APACHE III score, diabetes, history of steroid use, haematological failure and chronic liver disease), both the +936CT+TT genotype (hazard ratio (HR) 1.71, 95% CI 1.09 to 2.72, p = 0.02) and haplotype TCT (HR 2.11, 95% CI 1.32 to 3.37, p<0.01) were significantly associated with lower survival probability, consistent with the results assessed by logistic regression models.
DISCUSSION
Our data have shown that the +936TT and +936CT+TT genotypes of the VEGF gene are significantly associated with an increased risk of mortality from ARDS. At the haplotype level, the TCT haplotype was significantly associated with a higher mortality from ARDS. In addition, we showed that VEGF polymorphisms contributing to increased mortality in patients with ARDS were correlated with lower plasma levels of VEGF.
This study has a number of strengths. First, the prospective determination of ARDS using the AECC definition minimised phenotype misclassification since there is no diagnostic gold standard for ARDS. Second, the VEGF polymorphisms and the circulating VEGF levels were determined in a parallel manner. Thus, the functional effect of VEGF polymorphisms can be assessed. Third, restricting analyses to Caucasian patients reduced the possibility of altered genotype frequencies in different ethnicities.
Among the three functional SNPs studied, none of the –460C/T and +405C/G polymorphisms was found to have a significant effect on mortality from ARDS. However, the +936TT and the combined+936CT+TT genotypes were significantly associated with ARDS mortality, suggesting that +936 polymorphisms may have a stronger role than either the –460C/T or +405C/G polymorphisms in VEGF gene functions. Recently, a small case-control study found that the frequency of the combined +936CT+TT genotype in patients with ARDS was significantly higher than in controls. This study also found that the +936CT and TT genotypes were associated with the APACHE III score in patients with ARDS, but the association between the +936 CT/TT genotype and increased mortality from ARDS did not reach statistical significance (OR >1.80, p>0.05).26 In the present larger study, a significant association between the +936CT+TT genotype and mortality was found in patients with ARDS. At the haplotype level, the haplotype containing the +936T allele was also associated with mortality from ARDS, further supporting the effects of +936C/T variants on outcomes in patients with ARDS.
Our data showed that the +936CT/TT genotype was significantly correlated with lower plasma levels of VEGF, consistent with the functions of this polymorphism reported in other studies.14,15 Although the plasma VEGF levels were measured at only one time point and may not therefore fully reflect the temporal response of VEGF over the course of the disease, our results suggest that VEGF may be a protective factor in the severity of ARDS. Decreased levels of VEGF in the lungs have been correlated with a higher lung injury score and lower survival rates in patients with ARDS,10,11,30 whereas increased VEGF production in the lungs resulted in less lung injury.31 In animal models, administration of VEGF prevented lung injury-induced death.30,32 In alveolar epithelial cells, VEGF mRNA expression increased during recovery from oxygen injury.33 In neonatal rats exposed to high oxygen levels, intraocular injection of VEGF at the onset of experimental hyperoxia prevented apoptotic death of endothelial cells and rescued the retinal vasculature.34 Taken together, these findings indicate that VEGF may function as a protective factor in ARDS.
Although the haplotypes predicted in the present study were identical to those previously reported, the overall distribution of haplotype frequencies in the present study was different from that in Chinese and Korean populations.29,35 Different haplotype frequencies in different populations may be due to different ethnic backgrounds or different disease states. Interestingly, the frequencies of TCT (5.3%) and CGT (7.4%) haplotypes in the present study were similar to those reported in the Chinese population (6.0% and 6.4%, respectively).29 In Asian populations, both the TCT and CGT haplotypes were significantly implicated in a reduced risk of lung cancer, and the CGT haplotype was associated with decreased survival in patients with breast cancer.29 These observations suggested that TCT and CGT haplotypes may play an important role in disease processes. However, since these previous studies did not measure circulating VEGF levels, the mechanisms connecting the VEGF haplotypes with development or severity of the disease are unclear. Our study not only indicated that the TCT haplotype was associated with mortality from ARDS, but also showed that the CGT and TCT haplotypes correlated with lower circulating levels of VEGF protein, which suggests that these functional haplotypes may contribute to mortality from ARDS by affecting VEGF production.
We acknowledge some potential limitations to this study. First, the sample size was relatively small. Additional studies with larger populations are required to confirm the associations between the VEGF haplotypes and mortality in patients with ARDS. Second, the VEGF gene is a polymorphic gene, and the present study only investigated three SNPs. Further studies on other functional VEGF SNPs are needed to define the role of the VEGF polymorphisms in prognosis in ARDS. Third, measurement of plasma VEGF levels was done at one time point so the role of the plasma VEGF level in the natural history of ARDS remains to be defined. Finally, since genetic polymorphisms often vary between ethnic groups, further studies are necessary to clarify the association between the VEGF polymorphisms and the outcome in patients with ARDS in diverse ethnic populations.
In summary, the findings of this study suggest that the +936TT and +936CT+TT genotypes and the TCT haplotype of the VEGF gene contribute to increased mortality and to inter-individual variations in plasma VEGF levels in patients with ARDS. The associations found in this study are biologically plausible and may have significant implications for the treatment of ARDS.
Acknowledgments
The authors thank Weiling Zhang, Kelly McCoy, Thomas McCabe, Marcia Chertok and Julia Shin for patient recruitment; Andrea Shafer and Lia Shimada for research support; Ian James for laboratory expertise; and Janna Frelich and Lucille Pothier for data management.
REFERENCES
Supplementary materials
Files in this Data Supplement:
Footnotes
-
Published Online First 8 February 2007
-
This work was supported by grants from National Institute of Health (HL60710, ES00002, and K23 HL67197).
-
Competing interests: Dr Christiani is a paid scientific advisor to Gentra Corporation.
Linked Articles
- Airwaves