Article Text

Statistics from Altmetric.com
Clinical presentation
A 20-year-old man was referred for intermittent high fever, night sweat and loss of body weight for 6 months associated with progressive exertional dyspnoea which developed 4 weeks before admission. The patient was unresponsive to antibiotics and 14 day pre-emptive antituberculous chemotherapy with rifampicin, isoniazid, ethambutol and pyrazinamide. His temperature was 39.8°C, heart rate 96 beats/min, blood pressure 110/70 mm Hg, breath rate 22/min with decreased breath sounds in the left upper thorax without cyanosis, clubbing and hepatosplenomegaly.
Laboratory examinations showed mild microcytic hypochromic anaemia, erythrocyte sedimentation rate 46 mm/h, severe restrictive airflow limitation with impairment of transfer factor. Blood biochemistry including angiotensin converting enzyme (ACE), electrolytes including calcium, immunological profiles including antinucleic antibody, extractable nuclear antigens, antineutrophil cytoplasmic antibody, and HIV antibody, tuberculin skin test, Ziehl-Neelson stain, repeated blood culture, abdomen ultrasonography and fibrobronchoscopy were unremarkable.
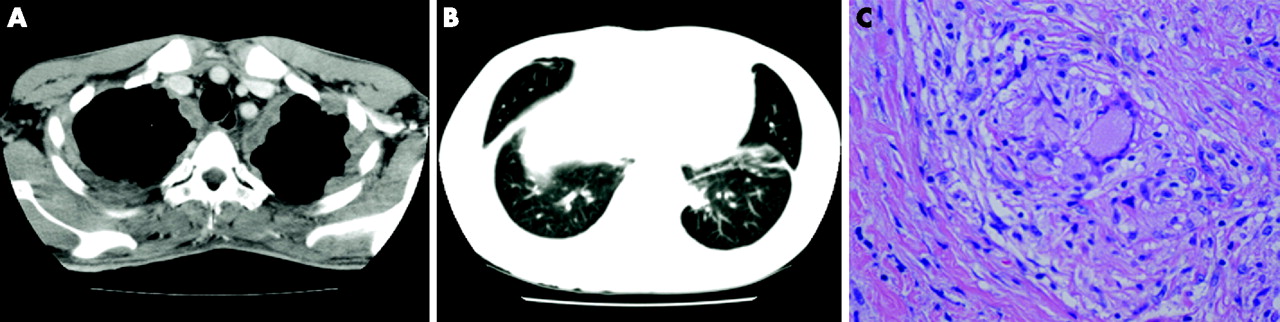
Plain chest radiography showed bilateral pleural thickening without parenchymal abnormality. A high resolution CT (HRCT) scan of the chest displayed thickening of the mediastinal, lateral and interlobar pleura (some >1 cm in thickness), multilobar subpleural pulmonary micronodules and thickening of bronchovascular bundles without intrathoracic adenopathy (fig 1A, B).
{kind=link}
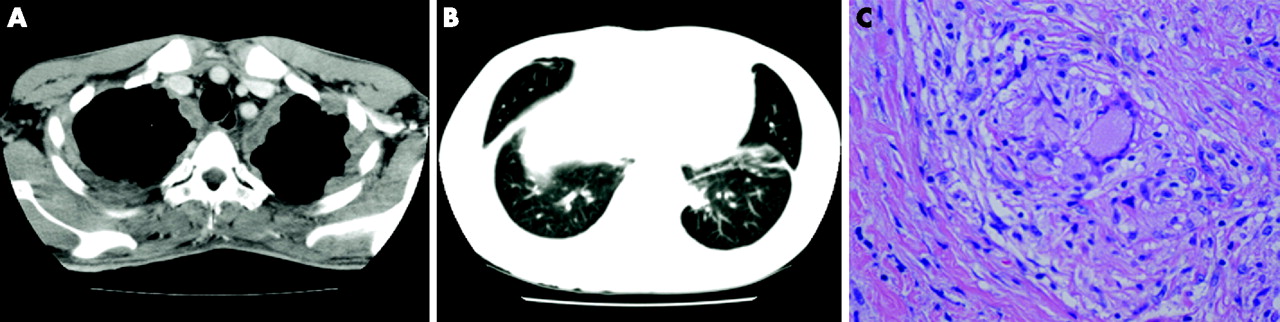
(A) High resolution CT (HRCT) scan showing diffuse thickening of lateral and mediastinal pleura with pleural nodularity, some >1 cm in thickness. (B) HRCT scan showing diffuse subpleural micronodules, thickening of bronchovascular bundles and thickening of interlobar septa. (C) Histological examination showing non-caseating epithelioid granuloma with focal central necrosis in biopsied pleura (H&E; ×400).
Question
What is the likely diagnosis and how should it be confirmed?
See page 637
This case was submitted by:
Linked Articles
- Miscellaneous