Article Text

Abstract
Background: Extensive biochemical and biophysical changes of the pulmonary surfactant system occur in the acute respiratory distress syndrome (ARDS).
Methods: The effect of intrabronchial administration of a recombinant surfactant protein C-based surfactant preparation (Venticute) on gas exchange, surfactant composition and function was investigated in 31 patients with ARDS in a randomised controlled phase I/II clinical pilot trial. Bronchoalveolar lavage fluids for surfactant analysis were obtained 3 h before and 48 and 120 h after the first surfactant application. Potentially deleterious effects of surfactant neutral lipids in patients with ARDS were also identified.
Results: Before treatment all patients had marked abnormalities in the surfactant phospholipid and protein composition. In response to surfactant treatment, gas exchange improved and surfactant phospholipid and protein content were almost normalised. Alveolar surface activity was dramatically impaired before treatment and only partially improved after surfactant administration. Further analysis of the bronchoalveolar lavage fluids revealed a twofold increase in neutral lipid content and altered neutral lipid profile in patients with ARDS compared with healthy controls. These differences persisted even after administration of large amounts of Venticute. Supplementation of Venticute or natural surfactant with a synthetic neutral lipid preparation, mimicking the profile in ARDS, caused a dose-dependent deterioration of surface activity in vitro.
Conclusion: Intrabronchial surfactant treatment improves gas exchange in ARDS, but the efficacy may be limited by increased concentration and altered neutral lipid profile in surfactant under these conditions.
- ARDS, acute respiratory distress syndrome
- BAL, bronchoalveolar lavage
- Fio2, fractional inspired oxygen
- γads, surface tension after 12 s of film adsorption
- γmin, surface tension values after 5 min of film oscillation at minimum bubble radius
- HPTLC, high-performance thin-layer chromatography
- LA, large surfactant aggregate
- Pao2, arterial oxygen tension
- SP, surfactant protein
Statistics from Altmetric.com
- ARDS, acute respiratory distress syndrome
- BAL, bronchoalveolar lavage
- Fio2, fractional inspired oxygen
- γads, surface tension after 12 s of film adsorption
- γmin, surface tension values after 5 min of film oscillation at minimum bubble radius
- HPTLC, high-performance thin-layer chromatography
- LA, large surfactant aggregate
- Pao2, arterial oxygen tension
- SP, surfactant protein
Pulmonary surfactant is a lipoprotein complex consisting of lipids (90%) and proteins (10%). Surfactant reduces the alveolar surface tension to near 0 mN/m, preventing alveolar collapse, and enables gas exchange and alveolar ventilation at physiological transpulmonary pressure gradients.1 Approximately 80–90% of the lipids are phospholipids. Four surfactant proteins (SP) have been identified (SP-A, SP-B, SP-C and SP-D).2 Surfactant obtained by bronchoalveolar lavage (BAL) can be separated into different subfractions by buoyant density gradient or differential centrifugation. The large surfactant aggregate (LA) fraction, consisting of lamellar bodies, tubular myelin and large multilamellar vesicles, displays excellent biophysical activity in vitro and in vivo and represents the precursor fraction of the interfacial surface film.3–5 In patients with the acute respiratory distress syndrome (ARDS), extensive alterations of biochemical and biophysical surfactant properties have been described.6–8 In addition, intrabronchial surfactant administration was shown to be beneficial in different ARDS models.9 Impaired surfactant function may therefore play a role in the development of gas exchange abnormalities in clinical ARDS. Accordingly, in some recent phase II and phase III clinical trials, administration of surfactant in subjects with ARDS significantly improved arterial oxygenation10–12 and surfactant composition.13,14
In the present study we investigated surfactant abnormalities in the BAL fluids of patients with ARDS participating in a randomised controlled phase I/II study in Europe/South Africa addressing the safety and efficacy of a recombinant SP-C-based surfactant (Venticute). Before randomisation, profound surfactant abnormalities were encountered, with a marked loss of surface tension-lowering properties and severe alterations in phospholipid, fatty acid and surfactant protein composition. In response to surfactant treatment, gas exchange was improved and phospholipid, fatty acid profiles and SP-C content were nearly normalised, but surface activity was only partially restored. To investigate the underlying mechanism for this partial restoration, we further analysed the LA fraction from the BAL fluids. Interestingly, we observed a twofold increase in the relative amount of neutral lipids in the LA fraction of patients with ARDS. Physiologically, neutral lipids represent 10–20% of the BAL fluid lipids and about 5% of the LA lipids. Within the LA fraction, the neutral lipids consist of cholesterol (30–40% of total neutral lipids), free fatty acids (25–30%), cholesterol ester (∼12%), monoglycerides (10–15%), diglycerides (∼14%) and triglycerides (∼8%).6,15 The increased concentration of neutral lipids in the LA fraction of subjects with ARDS was still present even after administration of large amounts of Venticute. Moreover, the composition of the neutral lipid fraction was markedly different between subjects with ARDS and healthy controls. Reconstitution of Venticute or a natural surfactant preparation with a neutral lipid preparation, mimicking the profile in subjects with ARDS, provoked a dose-dependent inhibition of surfactant function in vitro. This effect was already evident at a relatively neutral lipid dose found in patients with ARDS.
Changes in quantity and composition of the surfactant neutral lipids may thus contribute to the impairment of surface activity and gas exchange abnormalities in ARDS.
METHODS
Study design
Thirty-one patients with ARDS as defined by the American-European Consensus criteria16 for a maximum of 120 h since diagnosis (early ARDS) were investigated. All patients with ARDS participated in a randomised multicentre controlled phase I/II pilot study investigating the safety and efficacy of an intrabronchial administration of a recombinant SP-C-based surfactant (Venticute). Efficacy was assessed by calculating (1) the excess area under the arterial oxygen tension/fractional inspired oxygen (Pao2/Fio2) curve during the 24 h after administration of the first drug dose and (2) the number of days with unassisted breathing within the 28 day observation period and comparing these variables among groups. Another objective of the study was to assess BAL fluid recovered from the patients for surfactant components and function.
During a 6 h baseline period, clinical and respiratory parameters were recorded and the first BAL fluid sample (−3 h) for surfactant analyses was obtained. Baseline demographic and physiological data for each of the patient groups are shown in table 1. No significant differences were detected between groups. Values for the modified Acute Physiology and Chronic Health Evaluation (APACHE) II score and for baseline positive end-expiratory pressure and Pao2/Fio2 values indicate a similar severity of illness among the groups.
Baseline demographic and physiological data
Immediately after the conclusion of the baseline period, patients were prospectively randomised to receive either standard care (ARDS-standard care, n = 17) or standard care + 1 ml recombinant SP-C surfactant (containing 1 mg recombinant SP-C + 50 mg phospholipid)/kg lean body weight given up to four times in 24 h (ARDS-surfactant; n = 14).
BAL fluid was obtained from previously unlavaged lung segments at 48 and 120 h after the first treatment. Patients were subsequently observed for up to 28 days or until discharge from hospital. Additional information on study methods is provided in the online data supplement available at http://thorax.bmj.com/supplemental.
As a control group, 11 healthy volunteers without any history of cardiac or lung disease and with normal pulmonary function were studied. To investigate the effect of ventilation on the neutral lipid content in the BAL fluid, the relative neutral lipid content in the BAL fluid was also determined in four mechanically ventilated patients suffering from cardiogenic pulmonary oedema in the absence of ARDS and lung infection. A comparable disturbance in gas exchange was observed in patients with ARDS and in those with cardiogenic pulmonary oedema (Pao2/Fio2 ratio 126 mm Hg vs 152 mm Hg).
In vitro experiments with neutral lipids and surfactant preparations
Preparation of a rabbit BAL fluid pool
Healthy rabbits of either sex were killed by intravenous application of a lethal dose of pentobarbital/ketanest. A catheter was placed into the trachea and the lungs were lavaged three times with 50 ml 0.9% NaCl. After filtration of the lavage fluid through sterile gauze and sedimentation of cells (200 g, 4°C, 10 min), supernatants originating from 20 rabbits were pooled and then centrifuged at 48 000 g (4°C, 1 h). The pellet represents the LA fraction and was resuspended in a small volume of 0.9% NaCl/3 mM CaCl2 and adjusted to a stock concentration of 2 mg/ml phospholipids.
Recombinant SP-C-based surfactant preparation
The recombinant SP-C-based surfactant preparation used for the in vitro experiments was identical to the study drug material and was donated by ALTANA Pharma AG, Konstanz, Germany. The recombinant SP-C-based surfactant preparation contains dipalmitoylphosphatidylcholine and phosphatidyl-glycerol (7:3 wt/wt), enriched with 5% (wt/wt) palmitic acid and 2% (wt/wt) recombinant human SP-C. A stock preparation containing 2 mg/ml phospholipids was used.
Neutral lipid preparation
The neutral lipid preparations used for the in vitro experiments were designed to mimic the neutral lipid profile in patients with ARDS and consisted either of 100% or 50% unsaturated fatty acids. Increasing amounts of a 1 mg/ml stock solution were dried under nitrogen and resuspended with the rabbit LA pool or the recombinant SP-C surfactant. Details are outlined in the online data supplement available at http://thorax.bmj.com/supplemental.
Surfactant analysis
Isolation of large surfactant aggregates (LA)
BAL fluid from patients with ARDS, those with cardiogenic pulmonary oedema or healthy volunteers was centrifuged at 48 000 g (4°C, 1 h). The resulting pellet containing the LA fraction was resuspended in a small volume of 0.9% NaCl/3 mM CaCl2 and adjusted to a phospholipid concentration of 2 mg/ml. In parallel experiments, the LA fraction from seven patients with ARDS was further purified by sucrose gradient centrifugation as described in detail previously.17
Phospholipid and fatty acid analysis
Lipids were extracted with chloroform/methanol according to method of Bligh and Dyer18 and the phospholipid content was determined by spectrophotometric measurement of phosphorus.19 For separation and analysis of phospholipid classes, high-performance thin-layer chromatography (HPTLC) was used as previously described.7 Similarly, the fatty acid profile of phosphatidylcholine was assessed by gas-liquid chromatography as outlined previously.20
Determination of neutral lipid content and profile
The amount and relative distribution of neutral lipids was measured by HPTLC and densitometric scanning as previously described,6 with the following modifications: plates were pre-run with chloroform before application of the lipid standards and samples and the staining procedure was performed by incubation of the plates for 30 min with a 0.1% (wt/v) aqueous solution of 8-anilino-1-naphthalenesulfonic acid (8-ANSA, Merck, Darmstadt, Germany).
Quantification of surfactant proteins
The content of the surfactant proteins in the BAL fluid was determined by recently described ELISA techniques.7,21–23
Determination of surface activity
Surface tension measurements were performed by means of a pulsating bubble surfactometer (Electronetics, New York, USA) at a phospholipid concentration of 2 mg/ml. Surface tension after 12 s of film adsorption (γads) and after 5 min of film oscillation at minimum bubble radius (γmin) were recorded.
Analysis of data
Data are given as median and interquartile range. The box and whisker plots indicate the median, 1st and 3rd quartiles; the whiskers are extended to the most extreme value inside the 1.5-fold interquartile range. Values outside (potential outliers) are indicated by circles. The statistical analyses were performed in R Version 2.3.1.24 Deviations from the normal distribution were tested using the Shapiro-Wilk test. The comparability of data sets to justify a combination was tested with the F-test or multiway ANOVA and Wilcoxon rank sum tests. Differences between two groups were tested with the Student’s t test and Wilcoxon rank sum test according to the distribution of the data. Before-after treatment comparisons were performed with paired t tests and Wilcoxon sign rank tests, respectively. The p values of multiple comparisons were corrected with the algorithm of Benjamini-Hochberg25 to control the false discovery rate. Categorical data were tested for independence in contingency tables employing Fisher’s exact test. The distribution of the outcomes between the groups (alive, weaned and alive) was tested using the χ2 goodness-of-fit test against the null hypothesis of a uniform distribution. All tests were performed with an undirected hypothesis (two-sided). The level of statistical significance was set at 5%.
RESULTS
Gas exchange, biochemical and biophysical surfactant properties on surfactant treatment
Patients with early ARDS were treated up to four times by intrabronchial administration of 1 ml recombinant SP-C surfactant (containing 1 mg recombinant SP-C + 50 mg phospholipid)/kg lean body weight. A significant improvement in Pao2/Fio2 ratios at 48 h (p = 0.008) and 120 h (p = 0.0005) after initial treatment was observed (table 2). The value for the excess area under the Pao2/Fio2 curve during the 24 h after administration of the first drug dose was also higher in the surfactant treatment group than in patients receiving standard care only (402 vs 220 mm Hg/h; see table S2 in the online data supplement available at http://thorax.bmj.com/supplemental); however, this difference did not reach statistical significance, probably due to small sample sizes. Further study results are summarised in table S2 in the online data supplement (http://thorax.bmj.com/supplemental). In addition to the improvements in gas exchange, surfactant treatment produced a far-reaching restoration of key biochemical surfactant properties (table 2). In detail, the concentration of phospholipids was markedly increased in total BAL fluid, and the relative amount of the LA fraction was nearly normalised. Moreover, the relative amount of phosphatidylglycerol and the degree of palmitoylation in phosphatidylcholine were both fully normalised upon surfactant application, and the concentration of SP-C in total BAL fluid was greatly increased (table 2). No significant differences in BAL fluid concentrations of SP-A, SP-B or SP-D were detected between the standard care group and the surfactant treatment group (data not shown).
Biochemical surfactant properties and gas exchange in healthy controls and patients with acute respiratory distress syndrome (ARDS) receiving either standard care or additional surfactant treatment
In contrast to the complete normalisation of the phospholipid and fatty acid profiles, surface tension values after 5 min of film oscillation (γmin, fig 1) and after 12 s of film adsorption (γads, data not shown) were significantly improved in the patients receiving surfactant treatment (p = 0.02 at 48 h, p = 0.04 at 120 h), although not to values observed for healthy subjects. This observation was made in LA obtained by either high speed centrifugation (as depicted in fig 1) or by sucrose gradient centrifugation (data not shown).

Influence of intrabronchial surfactant administration on biophysical surfactant properties in patients with acute respiratory distress syndrome (ARDS). The surface tension after 5 min of film oscillation at minimum bubble radius (γmin) of the large surface aggregate (LA) fraction obtained by high speed centrifugation in healthy controls and patients with ARDS at a phospholipid concentration of 2 mg/ml is displayed. Data are given for patients with ARDS before randomisation (−3 hours = baseline) and 48 h and 120 h after intrabronchial administration of 1 ml recombinant SP-C surfactant (containing 1 mg recombinant SP-C + 50 mg phospholipid)/kg lean body weight given up to four times (surfactant) and for patients receiving standard care only (standard). The box-and-whisker plots indicate the median, 1st and 3rd quartiles; the whiskers are extended to the most extreme value inside the 1.5-fold interquartile range. Values outside (potential outliers) are indicated by circles. The significance level is indicated by *p = 0.02 (at 48 h) and p = 0.04 (at 120 h; all versus baseline values).
Neutral lipid content and profile of the LA fraction
To investigate the underlying mechanism for the partial restoration of surface activity, we further analysed the LA fraction from the BAL fluids for neutral lipid levels and profiles. Compared with healthy controls, the relative amount of neutral lipids within the LA fraction was significantly increased in the initial BAL fluid samples of the patients with ARDS at baseline (p = 0.0005), and no major changes were noted over the subsequent 120 h observation period, regardless of whether the patients received standard care only (p<0.001 at 48 h) or standard care + Venticute (p = 0.013 at 48 h, p<0.001 at 120 h; fig 2). Taking into consideration the absolute amount of phospholipids in the BAL fluid and the relative LA content, the median concentration of LA-related neutral lipids was 11.1 μg/ml (interquartile range 2.1–19.2) 48 h after surfactant treatment and 2.7 μg/ml (interquartile range 1.4–6.5) 120 h after treatment, and thus several fold higher in the ARDS-surfactant group compared with the pre-treatment data (baseline) and the ARDS-standard care group. Analogous data were obtained when the LA fraction was analysed after isolation by sucrose gradient centrifugation (data not shown). In contrast, in mechanically ventilated patients with cardiogenic pulmonary oedema, the relative amount of neutral lipids within the LA fraction (% of phospholipids) was unaltered compared with healthy controls (median (interquartile range) 6.1% (5.4–7.6%) vs 5.9% (5.2–7.1%)).

Neutral lipid content of the large surfactant aggregate (LA) fraction of healthy controls and patients with acute respiratory distress syndrome (ARDS). The content of neutral lipids (% of phospholipids, wt/wt) in the LA fraction obtained by high speed centrifugation from healthy controls, patients with ARDS before (−3 h = baseline) and after intrabronchial administration of 1 ml recombinant SP-C surfactant (containing 1 mg recombinant SP-C + 50 mg phospholipid)/kg lean body weight given up to four times, and from patients with ARDS receiving standard care only is given. The box-and-whisker plots indicate the median, 1st and 3rd quartiles; the whiskers are extended to the most extreme value inside the 1.5-fold interquartile range. The significance level is indicated by *p = 0.013; ***p<0.001 (baseline) and p<0.001 (standard treatment at 48 h and surfactant treatment at 120 h; all versus healthy controls). NL, neutral lipids; PL, phospholipids.
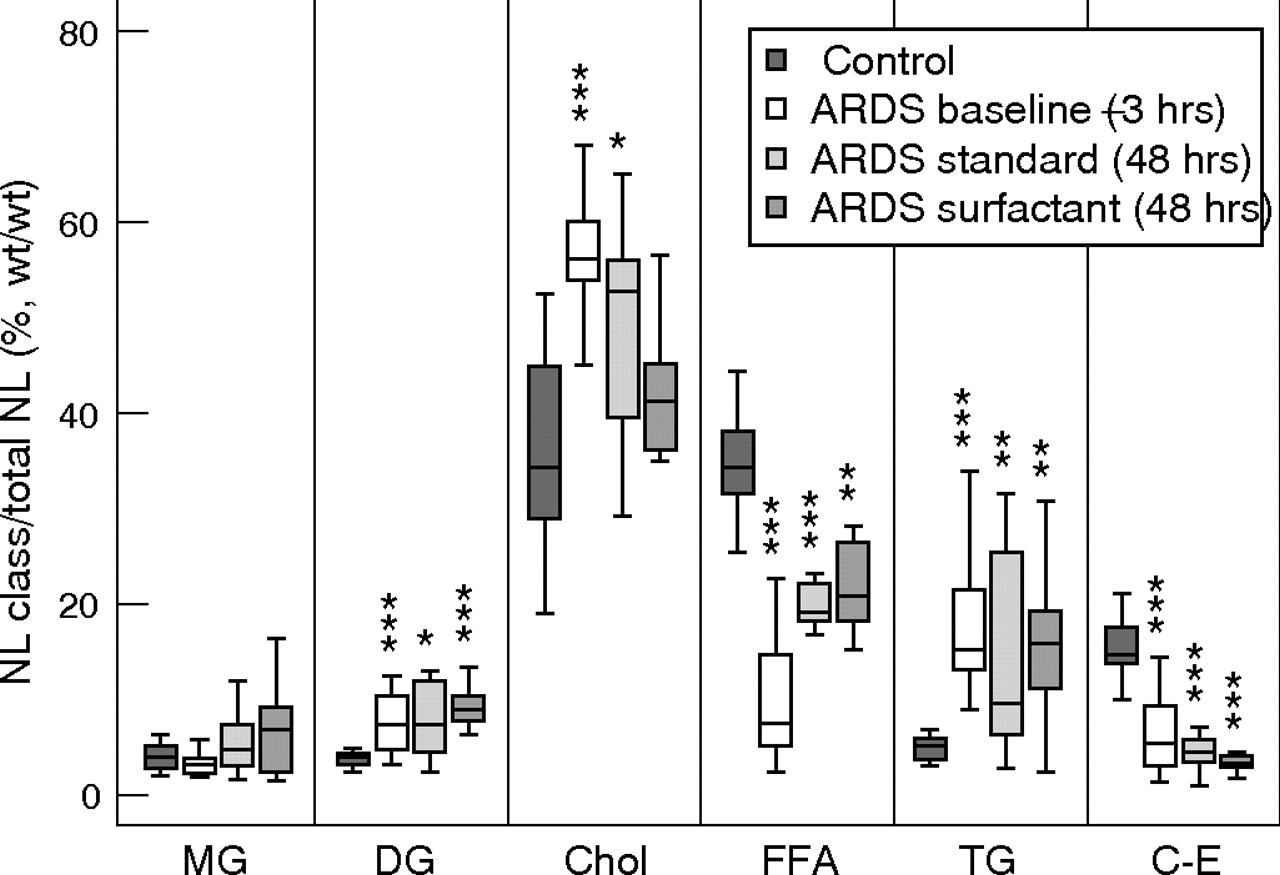
In addition to the increased levels of neutral lipids in patients with ARDS, changes were also observed in the neutral lipid profile. At baseline the relative contents of cholesterol, diglycerides and triglycerides were significantly increased (all p<0.001), whereas free fatty acids and cholesterol esters were decreased (all p<0.001; fig 3). Forty-eight hours after randomisation, the percentages of cholesterol and free fatty acids approached those in healthy controls whereas other neutral lipids remained at baseline concentrations (fig 3). There was no major difference in the neutral lipid composition between the ARDS-surfactant group and the ARDS-standard care group, with the exception of a slightly higher amount of free fatty acids (putatively based on the application of free palmitic acid contained in the recombinant SP-C surfactant) at the expense of the cholesterol fraction in the ARDS-surfactant group.

Neutral lipid profile of the large surfactant aggregate (LA) fraction of healthy controls and patients with acute respiratory distress syndrome (ARDS). The content of different neutral lipid classes (% of total neutral lipids, wt/wt) in the LA fraction obtained by high speed centrifugation from healthy controls, from patients with ARDS before treatment (−3 h = baseline) and from patients with ARDS receiving standard care or additional treatment with 1 ml recombinant SP-C surfactant (containing 1 mg recombinant SP-C + 50 mg phospholipid)/kg lean body weight given up to four times at 48 h after initial treatment is given. The box-and-whisker plots indicate the median, 1st and 3rd quartiles; the whiskers are extended to the most extreme value inside the 1.5-fold interquartile range. The significance level is indicated by *p<0.05; **p<0.01; ***p<0.001 (patients with ARDS pre or post standard or surfactant treatment vs healthy controls). MG, monoglycerides; DG, diglycerides; Chol, cholesterol; FFA, free fatty acids; TG, triglycerides; C-E, cholesterol ester; NL, neutral lipids.
Impact of neutral lipids on the surface activity of different surfactant preparations in vitro
The potential impact of neutral lipid mixtures—mimicking the neutral lipid profile in patients with ARDS—on the surface activity of different surfactant preparations was then investigated. Addition of increasing amounts of a completely unsaturated neutral lipid mixture to the recombinant SP-C surfactant or to a natural rabbit LA preparation resulted in a dose-dependent increase of γmin to almost 20 mN/m in both surfactant preparations (fig 4). γads values were only slightly increased in the presence of increasing amounts of neutral lipids (see fig S1 in online data supplement available at http://thorax.bmj.com/supplemental). A neutral lipid mixture consisting of 50% unsaturated fatty acids exhibited a similar inhibitory effect on the biophysical activity of the recombinant SP-C surfactant (fig 4 and fig S1 of the online data supplement available at http://thorax.bmj.com/supplemental).

Influence of neutral lipids on the surface activity of a recombinant surfactant protein (SP)-C-based surfactant preparation and of the large surfactant aggregate (LA) fraction of natural rabbit lung surfactant. A neutral lipid mixture containing 100% unsaturated neutral lipids and mimicking the neutral lipid profile in patients with acute respiratory distress syndrome (ARDS) was added in increasing amounts(0–25% of phospholipids, wt/wt) to 2 mg/ml recombinant SP-C surfactant (squares) and to 2 mg/ml of the LA fraction of natural rabbit lung surfactant (circles). A neutral lipid mixture containing 50% unsaturated neutral lipids was also added in increasing amounts to recombinant SP-C surfactant (triangles). The surface tension values after 5 min of film oscillation at minimum bubble radius (γmin) are given. Data are given as median values (n = 8 for each concentration). NL, neutral lipids; PL, phospholipids.
In order to define the putative surfactant inhibitory effect of each component of the neutral lipid mixtures more precisely, we investigated the influence of increasing amounts of single neutral lipids on the surface activity of the recombinant SP-C surfactant. Diglycerides and, to a lesser degree, free fatty acids showed a marked inhibitory effect on the γmin values (fig 5). Interestingly, two different neutral lipids—monoglycerides and cholesterol—were the most effective in inhibiting the γads values (fig S2 of the online data supplement available at http://thorax.bmj.com/supplemental).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Influence of single neutral lipids on the surface activity of a recombinant surfactant protein (SP)-C-based surfactant preparation. Single neutral lipids were added in increasing amounts (0–15% of phospholipids, wt/wt) to 2 mg/ml of the recombinant SP-C surfactant. The surface tension values after 5 min of film oscillation at minimum bubble radius (γmin) are given. Data are given as median values (n = 8 for each concentration). Monoglycerides (diamonds); diglycerides (upward triangles); cholesterol (circles); free fatty acids (downward triangles); triglycerides (stars); cholesterol ester (squares); NL, neutral lipids; PL, phospholipids.
DISCUSSION
In this study we have investigated the effect of intrabronchial administration of a recombinant SP-C-based surfactant (Venticute) on gas exchange, surfactant composition and function of 31 patients with ARDS. All patients participated in a randomised controlled multicentre phase I/II study in Europe/South Africa addressing the safety and efficacy of this surfactant preparation in ARDS. The study was performed in parallel to an almost identical trial in North America.13 In accordance with some former studies, a significant improvement was seen in gas exchange in the early period after surfactant administration. At baseline the BAL fluid concentrations of total phospholipids, phophatidylglycerol and SP-C, the relative amount of the LA fraction and the degree of palmitoylation in phophatidylcholine were all significantly decreased in patients with ARDS. Following administration of the recombinant SP-C surfactant all parameters were almost fully normalised, which paralleled the improvement in gas exchange. Surfactant treatment favourably decreased the raised minimum surface tension values of the LA fraction, although the values were still considerably higher than the ranges normally observed in healthy controls. As the applied material itself is known to possess excellent surface activity and, in addition, the far-reaching normalisation of biochemical parameters implies that the exogenous surfactant material successfully merged with the endogenous pool, there are only a few possible explanations for the limited improvement in surface activity in response to surfactant administration:
First, it could be argued that inhibitors of surfactant function (particularly plasma proteins such as fibrin(ogen)26) are largely responsible for the incomplete restoration of surface activity with surfactant treatment. However, we have used two different techniques—high speed centrifugation and sucrose gradient centrifugation—to isolate the LA fraction from BAL fluid, thereby separating the LA fraction from proteinaceous material and other inhibitors. Protein recovery in the LA fraction was 2.7% with centrifugation at 48 000 g and <0.5% with sucrose gradient centrifugation (data not shown).7 As the surface activity of the LA fraction obtained by the two methods deteriorated to the same extent and as there was no appreciable contamination of the lipid fraction with lysoPC, platelet-activating factor or proteins, we think that inhibitory pheno-mena are unlikely to explain the incomplete restoration of surface activity of the LA fraction. Nevertheless, we would anticipate that the “true” alveolar surface tension of patients with ARDS, both before and after surfactant treatment, is higher as a result of the presence of these inhibitors, as suggested in previous reports.7,14
Second, it might be argued that the lack of SP-B was responsible for the incomplete improvement in surface activity. However, numerous studies have shown that SP-C-based surfactants such as the recombinant SP-C surfactant achieve similar low surface tension values in vitro and similar efficacy in vivo to that of natural surfactant extracts containing both hydrophobic surfactant proteins.27–29 Nevertheless, this issue may be of some importance in the presence of inhibitors where SP-B-based surfactants have been shown to display better surface activity than SP-C-based surfactants.27,28 However, as discussed above, the isolated LA fractions were almost completely separated from potential inhibitors. We therefore think that this issue is not of major importance.
Third, direct damage to surfactant-specific proteins, probably by proteolysis, has previously been demonstrated in the lungs of patients with ARDS.30 We found a significant increase in SP-C levels in the BAL fluids of patients with ARDS following surfactant treatment (p = 0.003 at 48 h). However, it is possible that some of this exogenously administered protein is degraded by the action of activated polymorphonuclear neutrophils30 and this may contribute to the limited improvement in surface activity in response to surfactant treatment.
Fourth, there was a marked increase in neutral lipids in the LA fraction of subjects with ARDS, but no significant difference between the neutral lipid content in the BAL fluids of mechanically ventilated patients with cardiogenic pulmonary oedema and healthy controls. These findings indicate that mechanical ventilation itself is not responsible for the observed changes in the neutral lipid content of the lungs of patients with ARDS. The recombinant SP-C surfactant used in this study contains free palmitic acid at a relative concentration of 5%. Assuming that most of the material reached the distal lung after administration, one may anticipate a reduction in the neutral lipid content of the LA fraction to values close to 5%. Instead, the neutral lipid content remained raised after surfactant treatment. In addition, the neutral lipid profile (which was significantly altered at baseline) was only marginally affected by treatment with the recombinant SP-C surfactant. As such an increase in neutral lipids may have disadvantageous effects on surface tension, we analysed changes in surface activity of different surfactant preparations when supplemented with a synthetic neutral lipid mixture mimicking the neutral lipid profile of patients with ARDS. This resulted in a dose-dependent impairment of surface activity above a neutral lipid to phospholipid ratio of 0.05.
Neutral lipids have been known for a long time to be an integral component of the pulmonary surfactant system. They are actively secreted within the lamellar bodies from type II cells,1 but their precise role within the surfactant system is still unclear. In particular, data are scarce in view of the regulation and role of neutral lipids in acute respiratory failure. Alveolar cholesterol was found to be increased in some animal models of acute lung injury31 but neutral lipids have never been investigated in patients with ARDS. It has recently been shown that cholesterol plays a critical role in promoting the lateral organisation of bilayer membranes made of native pulmonary surfactant.32 Furthermore, neutral lipids such as cholesterol enhance adsorption at the air-water interface and also improve film respreading of dipalmitoylphosphatidylcholine or more complex phospholipid films, thus improving surface activity.33–35 However, neutral lipids were much less effective in enhancing adsorption than the hydrophobic surfactant proteins SP-B and SP-C.33 In oscillating bubble studies, in contrast to mixtures of phospholipids and hydrophobic surfactant proteins, a protein-free mixture consisting of phospholipids and neutral lipids never reached a minimum surface tension of <20 mN/m.34 Furthermore, investigations with the pulsating bubble surfactometer showed that the addition of cholesterol to different surfactant preparations can impair the surface tension-lowering ability on bubble pulsation and may destabilise surface films on maximum compression.36 Finally, all of the preceding studies have been undertaken with “physiological” neutral lipid concentrations (∼5% neutral lipids wt/wt of phospholipids). Higher neutral lipid concentrations, as reported for the first time in this study of patients with ARDS, have not yet been investigated in detail. The present findings suggest that an increased and “non-physiologically” composed neutral lipid fraction within the LA fraction may cause instability of the interfacial surfactant film on lateral film compression, with increased minimum surface tension values. This interpretation is reinforced by our finding that, in particular, the minimum surface tension values obtained under cyclic surface area changes were increased, whereas adsorption remained largely unchanged with neutral lipid supplementation.
The source of increased neutral lipids and altered composition in ARDS is presently unknown. One possibility is altered synthesis or secretion by type II cells. Alternatively, changes may be due to spillover of neutral lipids from the systemic circulation via a leaky endothelial and epithelial barrier. However, the plasma neutral lipid profile is characterised by a large amount of cholesterol ester (46%) and triglycerides (30%), whereas only traces of free fatty acids, monoglycerides and diglycerides can be detected.37 The plasma neutral lipid profile is thus strikingly different from the neutral lipid profile in the LA fraction, regardless of whether the LA fraction was obtained by high speed centrifugation or further purified from blood contaminants by sucrose gradient centrifugation. Thus, “contamination” by plasma-derived neutral lipids seems unlikely. Moreover, if the type II cell is indeed the main source of increased neutral lipids in ARDS, our observation of a persistently raised neutral lipid content despite application of large amounts of exogenous surfactant material would suggest the existence of a mechanism that maintains a particular neutral lipid/phospholipid ratio in the acutely injured lung.
We conclude that increased levels and an altered neutral lipid profile may contribute to the impairment of surface activity in ARDS. Remarkably, neutral lipid abnormalities of the LA fraction were found to persist even after intrabronchial surfactant administration and may prevent full normalisation of the alveolar surface tension by surfactant treatment. Further studies are needed to address the mechanisms underlying the disturbances in surfactant neutral lipid homeostasis in ARDS. One implication of this study would be to test if neutral lipid-free exogenous surfactant preparations are more suitable for the treatment of ARDS.
Acknowledgments
The authors thank all the European/South African clinical centres that participated in the Venticute phase I/II trial and Leigh Marsh for proofreading the manuscript.
REFERENCES
Supplementary materials
Files in this Data Supplement:
Footnotes
-
Published Online First 7 February 2007
-
This study was supported by Deutsche Forschungsgemeinschaft (DFG), SFB 547, SCHM 1524/2-1, ALTANA Pharma AG, Konstanz, Germany.
-
Competing interests: WS receives grant and contract support and fees for consulting services by the following companies: Schering AG, Pfizer Ltd, Altana Pharma AG, Lung Rx, Myogen. None of the other authors has any financial relationship with a commercial entity that has an interest in the subject matter or materials discussed in the manuscript.
-
The study was approved by local institutional review boards/ethics committees at each participating institution and informed consent was obtained from all patients or their legal representatives.