Article Text

Abstract
Aim: To quantify the incidence of unsuspected pulmonary emboli (PE) in an unselected inpatient population undergoing contrast enhanced multidetector CT (MDCT) scanning of the thorax and to assess aetiological factors in their development.
Methods: All inpatients undergoing MDCT scanning of the thorax over a 10 month period were prospectively identified. Patients with previous or suspected current PE were excluded. CT scans were reviewed and the degree of contrast enhancement and presence of PE recorded. Where PE was found, the level of the most proximal thrombus was identified. Patient age, length of admission, slice scan thickness and clinical indication were noted.
Results: 547 inpatients who had undergone MDCT scanning were identified. Following exclusions 487 remained, 28 of whom (5.7%) had PE. Unsuspected PE was more common with increasing age, occurring in 9.2% (20/218) of all patients over 70 years and 16.7% (11/66) of those over 80 years (p<0.001). Eighteen of the 28 positive scans (64.3%) were at the segmental or subsegmental level. No other aetiological factor was identified which significantly increased the incidence of unsuspected PE. No significant difference was noted between 4-slice and 16-slice MDCT. Nine of the cases of incidental PE (32.1%) were not identified by the original reporting radiologists.
Conclusion: PE is an unsuspected finding on contrast enhanced MDCT scanning of the thorax in 5.7% of all inpatients. The incidence is higher in older patients. Most are peripheral and >30% are missed on initial review. PE should be routinely sought in all contrast enhanced MDCT scans of the chest, irrespective of the indication for the CT scan.
- CTPA, CT pulmonary angiogram
- MDCT, multidetector computed tomography
- PE, pulmonary embolism
Statistics from Altmetric.com
Pulmonary embolism (PE) is a common disease estimated to be a contributory factor in approximately 200 000 deaths per year in the USA, occurring in 5–10% of hospital deaths.1 It is a difficult condition to positively diagnose clinically, presenting with varied and sometimes minimal symptoms that mimic a myriad of other pathologies. The actual annual incidence of PE is therefore difficult to determine, but has been estimated at around 60–70 per 100 000 people.2
In the past, PE was only ever firmly diagnosed after the diagnosis had first been considered by a clinician and then proved by radiological study (either an isotope perfusion lung scan, a conventional pulmonary angiogram or, in recent years, a CT pulmonary angiogram (CTPA)). With the advent of multidetector CT (MDCT) scanning, which allows assessment of the chest with thin section collimation using rapid acquisition, it is now possible to visualise the pulmonary arterial tree down to the subsegmental level on most contrast enhanced scans allowing unsuspected PE to be detected on routine MDCT scans of the chest.
METHODS
Patient inclusion
Over a period of 10 months from 1 January 2004 to 13 October 2004, consecutive inpatients undergoing contrast enhanced MDCT scanning of the chest for an indication other than suspected PE were identified at a large teaching hospital. Inpatients were selected for the patient study group as this was the population thought to be most at risk and in whom it was considered most likely that unsuspected PE might be detected. Patients were scanned using either a 4-slice or 16-slice scanner (both Toshiba Aquilion Series, Toshiba Medical Systems, Tokyo, Japan).
Patient details were recorded for the purpose of identification of the computer images and for accessing demographic information from the hospital database. From the request card, logbooks and hospital database, records were made of age, referring speciality, date of admission (to calculate length of hospital stay before scanning), scan slice thickness and brief clinical information or reason for referral. Recruited patients were hospital inpatients from the wards, admissions unit, day case unit or accident and emergency (excluding trauma cases). Patients were excluded if they were suspected or known to have had a PE. CTPA studies were not included.
Scan parameters
The scan protocol varied depending on the indication for study. In most studies 100 ml iodinated contrast was injected at 3–4 ml/s with the scan commencing at around 20 s after the start of the contrast injection. Scan parameters are outlined in table 1.
Scan parameters
Image interpretation
All studies were initially reported as per routine practice in our institution. Subsequently, a single consultant thoracic radiologist who was blinded to the initial report reviewed the studies. All images were assessed using a workstation allowing multiplanar reformatting. For each patient the degree of contrast enhancement and presence or absence of PE was noted. If the scan was positive, the level of thrombus was recorded as central, lobar, segmental or subsegmental. Contrast enhancement was classified as good (good enhancement of segmental and subsegmental arteries), moderate (good enhancement of segmental but not of subsegmental branches) or poor (inadequate enhancement of entire pulmonary arterial tree). Patients were excluded from the study at this stage if there was poor or absent contrast enhancement, if the lungs were only partially imaged or the images were not retrievable on the workstation (technical difficulties).
If scans were found to show PE which had not previously been reported, the appropriate clinical team was informed.
RESULTS
During the study period 547 consecutive inpatients undergoing MDCT scanning of the thorax were identified from the scanner logbooks. Sixteen patients were excluded because of absence of intravenous contrast, 25 for incomplete lung imaging and 19 were excluded because of poor contrast enhancement.
Following exclusions, 487 study patients remained. These were inpatients with good or moderate contrast enhancement of the pulmonary arteries and no suspected or prior history of PE. The study group included 200 female patients (41%) and 287 male patients (59%). The median age was 69 years (range 15–93).
Twenty-eight of the 487 scans showed PE, an incidence of 5.7% of the total study population. Twenty of the 218 patients over 70 years of age had unsuspected PE, an incidence of 9.2% in this cumulative grouping. This rose in the group aged over 80 years to an incidence of 16.7% (11/66). The median age of all patients with a positive scan was 77 years (range 52–88). There was a statistically significant association between age group and the rate of unsuspected PE (χ2 = 13.28, p<0.001) with a significant difference in the rate of PE with increasing age. The distribution of PE by age is recorded in table 2 although, for the purposes of analysis, the <50 and 50–59 age groups have been combined.
Age distribution of positive scans
Of the 28 positive scans, 27 (96.4%) showed good contrast enhancement; the one scan that showed only moderate enhancement had thrombus at a segmental level.
Four hundred and two patients (82.5%) were scanned on a 16-slice scanner and images reconstructed at 1 mm thickness. The incidence of PE among this subgroup was 6.0% (24/402). Eighty-five patients (17.5%) were scanned on a 4-slice scanner with slice reconstructions at either 2 mm or 3 mm. Four of these scans were positive for PE, an incidence of 4.7%. Of these, three were scanned with 3 mm slice thickness. No statistically significant difference was noted between 4-slice and 16-slice scanners in their ability to identify unsuspected PE (p = 0.80, Fisher’s exact test).
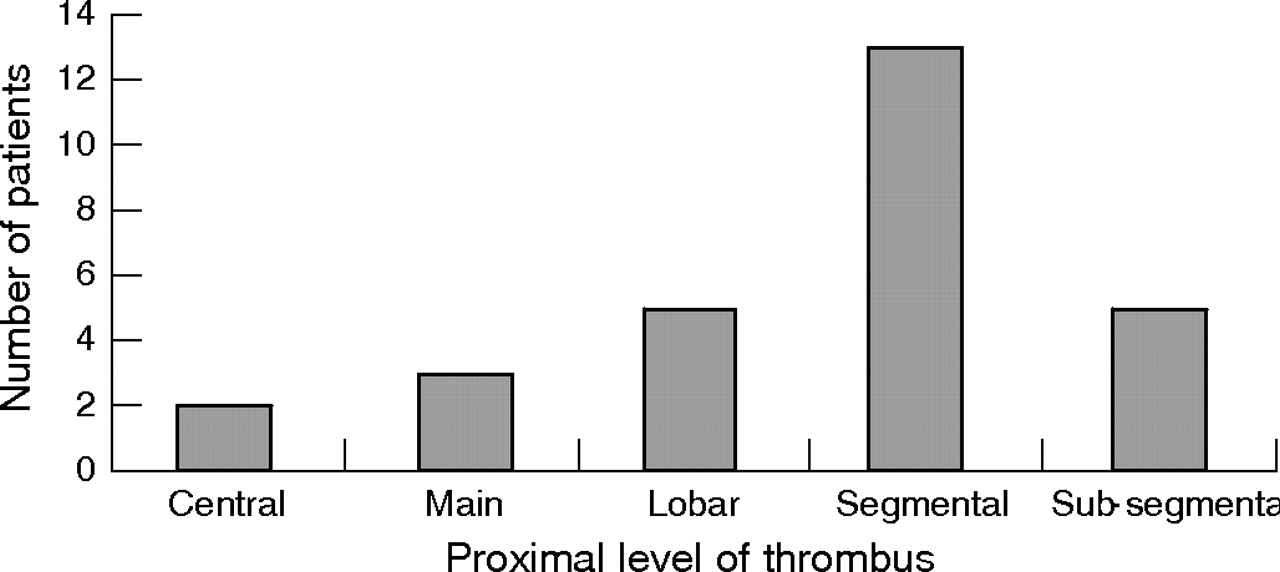
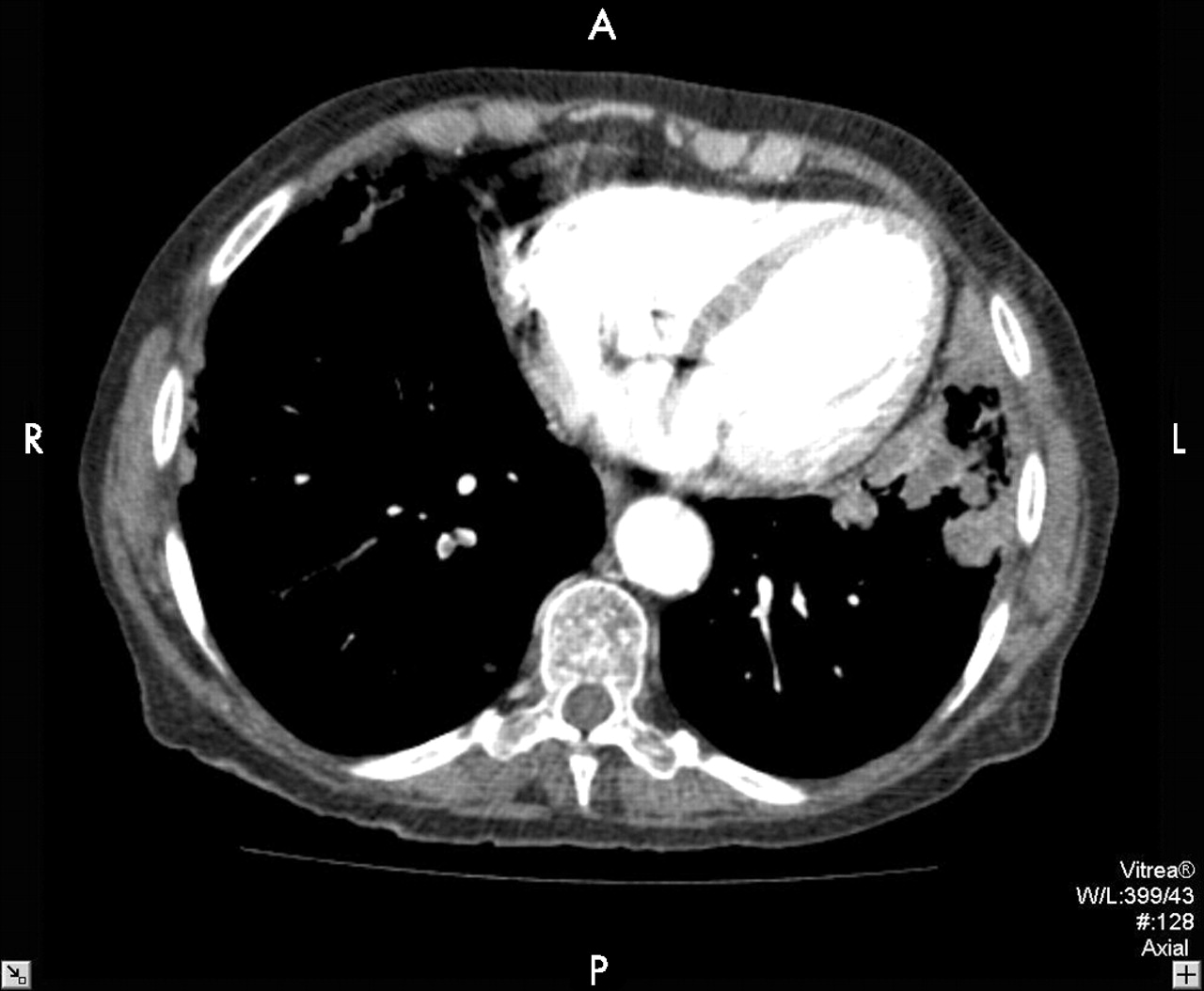
The distribution of proximal thrombus in the entire population is shown in fig 1. Figure 2 is an example of subsegmental thrombus in the right lower lobe, fig 3 shows segmental level thrombus and fig 4 shows more proximal PE in the main pulmonary arteries bilaterally. All were unsuspected. Nineteen of the 28 cases of PE (67.9%) were positively identified on the initial report. Of the nine positive studies not identified at initial review, thrombus was segmental in six cases and subsegmental in three. The distribution of involved lobes is summarised in fig 5.

Proximal extent of thrombus in the study population.

Subsegmental thrombus in the right lower lobe.

Segmental level thrombus.
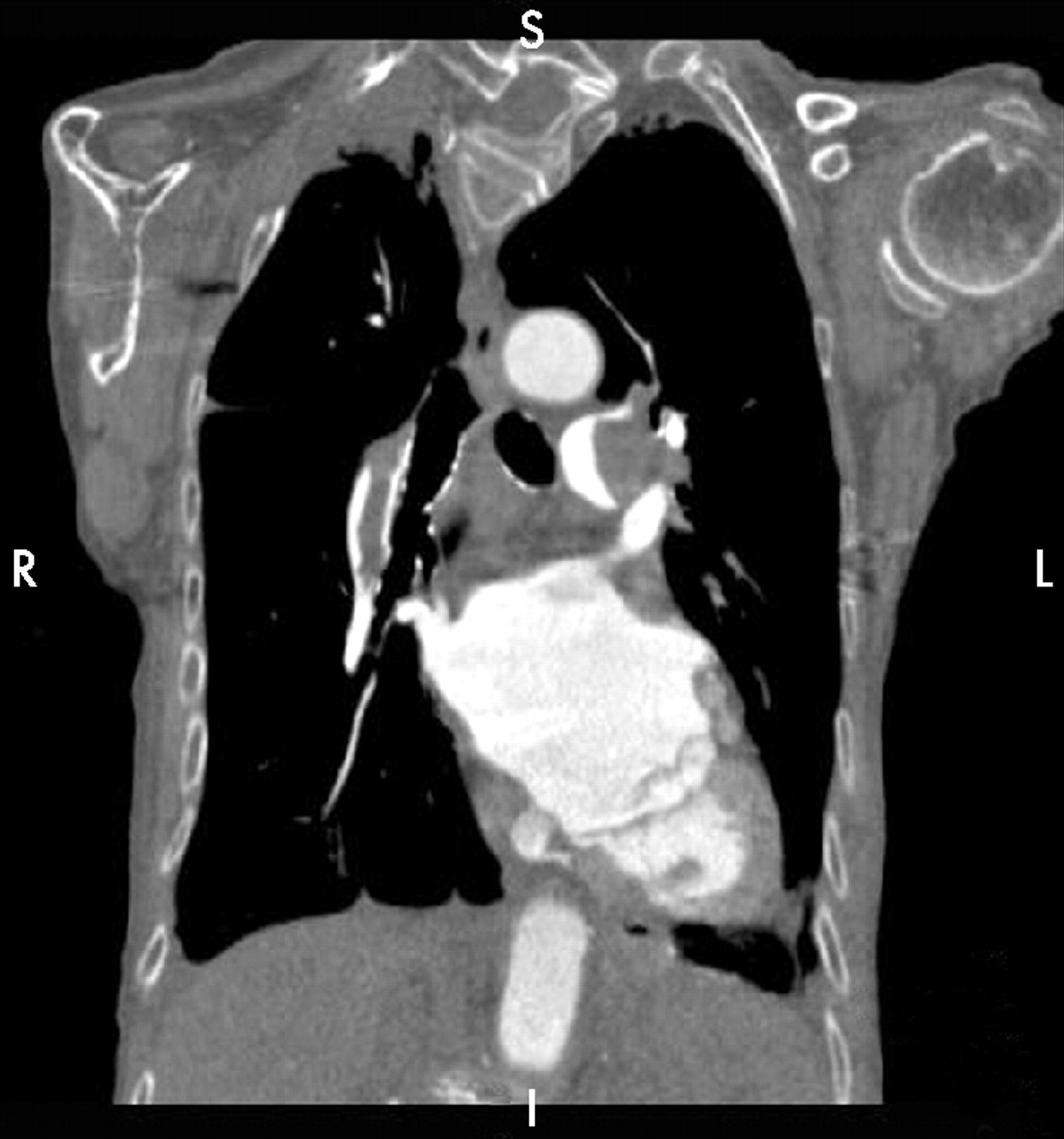
Pulmonary embolism in the main pulmonary arteries bilaterally.
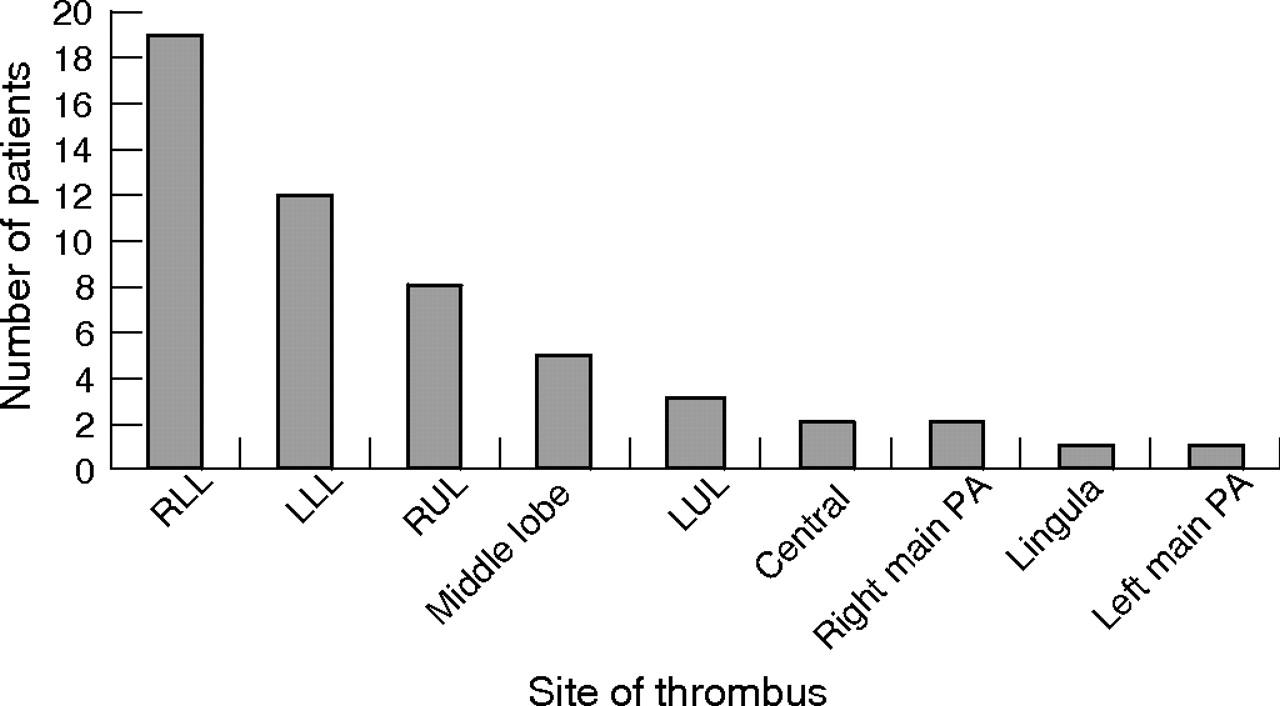
Site of thrombus in study population.
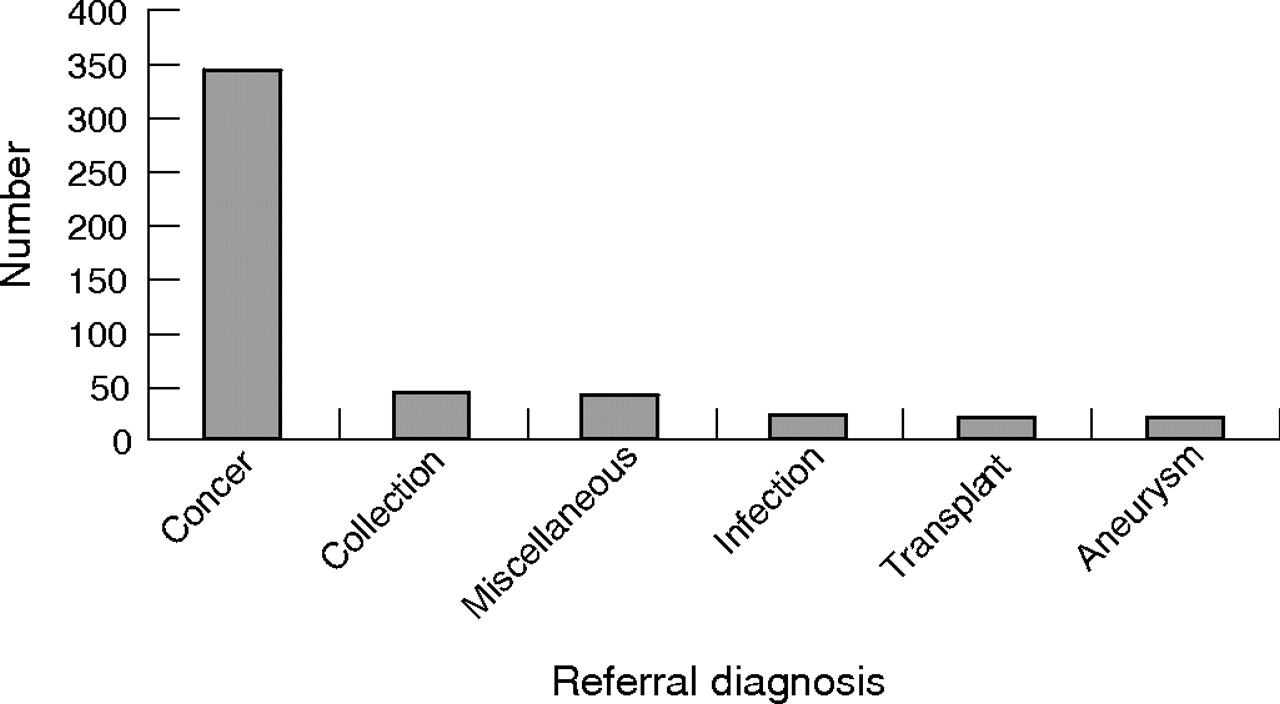
Referral speciality and clinical information given on the request card were used to determine any prior risk. The presumptive diagnosis of all patients at referral is illustrated in fig 6. Most referrals, accounting for just over a third, were from respiratory physicians (166/487); general surgeons and general medical teams accounted for just over 10% of referrals each, with fewer referrals from gastrointestinal medicine, the transplant unit, geriatrics and intensive care.

Presumptive diagnosis at referral. Cancer refers to any patient with known or suspected cancer, mediastinal or pulmonary mass. Collection covers patients being imaged to evaluate pleural or pericardial collections. Infection includes patients with slow to resolve pneumonia or sepsis. Transplant identifies a group of patients being assessed for hepatic and renal transplantation. Aneurysm covers patients with thoracic aneurysm as well as patients suspected of having acute aortic syndrome. Miscellaneous describes a heterogeneous group with diverse presumptive diagnoses including pulmonary fibrosis, emphysema, collapse, hoarseness and dysphagia.
Studies were performed as determined by clinical urgency, based largely on information provided on the patient request card. At our institution most inpatient CT scans are performed within 3 days of request.
Eighteen of the 28 positive scans (64.3%) and 343 of the total scans (70.4%) were carried out for confirmed or presumed malignancy. There was no evidence of a statistically significant difference in the proportion of PE cases in those with suspected malignancy and those not suspected of malignancy (18/343 (5.2%) vs 10/144 (6.9%), difference −1.7% (95% CI −6.47% to 3.08%), p = 0.486, binomial test for proportions).
The median duration of inpatient admission before scanning was 3 days (range 0–255). The distribution of hospital stay for patients with a positive scan is shown in fig 7. When the length of hospital stay was grouped into 0–1, 2–3, 4–6 and 7+ days, there was no statistically significant relationship between length of hospital stay and likelihood of finding unsuspected PE (χ2 = 2.169, p = 0.538).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Days in hospital before diagnosis of PE.
DISCUSSION
Terminology and significance of unsuspected PE
Previous studies3,4 have described the finding of PE in situations where this is not suspected as “incidental” PE. In this study we have chosen to use the term “unsuspected” PE, previously also used by Gosselin et al.5 The term “incidental” to some suggests clinical insignificance. We feel there is little evidence to support the implication that these emboli are necessarily of less clinical significance just because they are identified as an incidental finding.
Recent meta-analysis of necropsy studies has shown that PE remains a common condition where there is a discrepancy between clinically suspected and necropsy proven cause of death.6 The significance of small PE has been called into question. While discussion as to the importance of small emboli is beyond the scope of this article, a comprehensive summary of the evidence regarding small PE is contained in a recent editorial by Goodman.7 It is of note that, of the 28 emboli identified in this study, 18 were at the segmental or subsegmental level and might be classified as small.
Identification and estimates of prevalence of PE
Contrast enhanced CT scanning, specifically CTPA, has become the first line investigation in many centres in the diagnosis of PE due to a high inter-observer agreement,8 identification of unsuspected pathologies9 and because it is a cost effective method of imaging PE.10
Unsuspected PE has previously been identified in patients undergoing contrast enhanced CT scanning of the chest for reasons other than suspected PE. Using older technologies in a study of 1879 patients undergoing contrast enhanced helical CT scanning of the thorax, Winston et al4 identified 18 patients with unsuspected PE, estimating the prevalence at 1%. A similar study by Gosselin et al5 found an overall rate of 1.5%, with up to 5% of inpatients having PE. More recently, using a 4-slice MDCT scanner, Storto et al3 found incidental PE in 4% of 474 inpatients. No previous studies have reported rates of unsuspected PE using a 16-slice MDCT scanner.
Our study has shown an overall rate of unsuspected PE of 5.7%. We identified only those inpatients in whom PE was an unexpected finding. Because we excluded CTPA examinations and patients with a known PE, this figure must be an underestimation of the actual prevalence of PE in the hospital population. The fact that we are now identifying these unsuspected PE on a regular basis implies that PE is much more common than previously appreciated. Many of the unsuspected PE were in the smaller segmental and subsegmental arteries. While large central PE may seem more likely to be clinically apparent, peripheral emboli are also important because of the tendency to cause pulmonary infarction, pleuritic chest symptoms and as a possible prelude to larger potentially life threatening emboli. Until the natural history of these smaller PE is better understood, it remains the responsibility of the radiologist to report them and of the clinician to define the treatment. We cannot conclude from this study whether or not patients with unsuspected PE should be anticoagulated or not. We would expect that the larger emboli at least require treatment. Evidence is uncertain as to the optimal management for the smaller asymptomatic emboli. In our institution, clinicians certainly still consider all detected PE as significant and treat them as such.
The question which our study does raise is whether PE, and in particular small PE, are more common than previously recognised. If this is the case, then these small PE may be of lesser clinical significance than larger clinically evident PE and may merit a different management strategy. A possible strategy, which would need to be fully evaluated, would be to do a leg ultrasound in patients with unsuspected or asymptomatic emboli to look for possible deep vein thrombosis and avoid anticoagulation if negative.
Spatial resolution and identification of PE
The higher incidence of PE found in our study compared with previous studies may be due to improved spatial resolution. Previous work has indicated that MDCT scanning increases conspicuity of small peripheral arteries.11,12 Several studies have also shown increased sensitivity for detection of pulmonary embolism in subsegmental vessels using MDCT scanning.13–15 Patel et al16 have previously shown that MDCT scanning demonstrates more PE and in smaller vessels than single slice scanning. In addition, the same study showed that use of MDCT decreasing slice thickness from 2.5 mm to 1.25 mm improved visualisation of segmental and subsegmental vessels and PE.
If spatial resolution is the principal determining factor in identification of peripheral emboli, it is perhaps not surprising that we found more incidental PE in patients scanned using a 16-slice scanner with 1 mm slice thickness than in a 4-slice scanner with a 2 or 3 mm slice thickness. The difference in this study between 4-slice and 16-slice scanning was not statistically significant. This probably reflects the small number of positive scans identified.
In this study only 67.9% of the positive scans were initially reported as showing PE. In all nine cases (32.1%) where PE was not identified, thrombus was at the segmental level or more distally. This suggests that smaller clots are more easily overlooked, and highlights the need to include a thorough assessment of pulmonary arteries in all contrast enhanced thoracic CT scans.
Aetiological factors in unsuspected PE
Age
Older patients are significantly more likely to develop symptomatic thromboembolic disease.2,17,18 This study shows that older people are also more likely to develop unsuspected PE. This was most dramatically illustrated in the 80+ age group in whom PE occurred in 16.7% of cases (table 2). We recognise that age may be a surrogate for other risk factors known to be associated with an increased risk of PE such as malignancy, immobility or heart failure.
Malignancy
The suggestion that rates of incidental PE are higher in patients with confirmed or presumed malignancy is not new. In a subgroup assessment following the PIOPED study, 14 of 20 patients in whom unsuspected PE was proved to be the principal cause of death at autopsy had advanced associated diseases with malignancy in 4 patients.19 The link between thromboembolic disease and malignancy is further suggested by the finding of an increased risk of the diagnosis of malignancy in the 2 years following diagnosis of venous thromboembolism in a large retrospective study.20 In a recent paper regarding incidental PE, Storto et al3 noted that 70% of patients with incidental PE had malignancy. No statistically significant correlation between malignancy and the incidence of PE was noted in this study. The reasons for this are uncertain, but may reflect in part the small number of positive cases and the fact that most of the patients having a contrast enhanced CT scan of the thorax fell into this category and that many of the scans were for presumed rather than confirmed malignancy.
Hospital admission
No significant association was seen in this study between length of hospital admission and presence of PE. Hospital inpatient stays are now relatively short. The average stay for all patients scanned in this study was only 3 days and 17 of the 28 positive cases were identified within 5 days of admission. We would suggest that at least some of these emboli had been present before admission. We would also suggest that, for patients with longer admissions, the use of low molecular weight heparin as prophylaxis might have a protective effect; however, this information was not easily available during this study.
The rate of unsuspected inpatient PE will not reflect the general outpatient incidence. This population theoretically should have fewer risk factors for PE and therefore presumably a lower incidence.3 A small number of outpatient scans were inadvertently assessed before exclusion from our study. Of 43 such studies, four patients (9.3%) showed incidental PE. This is at odds with the suggestion that prolonged hospital admission increases the rate of PE, but is felt likely to be spuriously high due to the small number of patients involved and a larger study is needed in this outpatient group.
In conclusion, unsuspected PE was found in 5.7% of inpatients undergoing a contrast enhanced MDCT scan of the thorax. The detection of these thrombi suggests that the actual prevalence of PE in the hospital population is greater than previously appreciated. The incidence increases significantly with age, with 9.2% of those aged over 70 and 16.7% of those aged over 80 being affected. We found no statistical correlation with the length of admission or associated malignancy. More than 30% of emboli were missed on initial review; all of these were found in segmental or subsegmental vessels, but the clinical significance of these smaller thrombi remains uncertain. Routine assessment of the pulmonary arteries should be considered standard practice when reporting any contrast enhanced MDCT scan of the thorax.
REFERENCES
Footnotes
-
Published Online First 8 December 2006
-
Funding: None.
-
Competing interests: None.
-
Institutional approval was obtained for the study.