Article Text

Abstract
Background: Identification of the risk factors for bronchial hyperresponsiveness (BHR) would increase the understanding of the causes of asthma. The relationship between physical activity and BHR in men and women aged 28.0–56.5 years randomly selected from 24 centres in 11 countries participating in the European Community Respiratory Health Survey II was investigated.
Methods: 5158 subjects answered questionnaires about physical activity and performed BHR tests. Participants were asked about the frequency and duration of usual weekly exercise resulting in breathlessness or sweating. BHR was defined as a decrease in forced expiratory volume in 1 s of at least 20% of its post-saline value for a maximum methacholine dose of 2 mg.
Results: Both frequency and duration of physical activity were inversely related to BHR. The prevalence of BHR in subjects exercising ⩽1, 2–3 and ⩾4 times a week was 14.5%, 11.6% and 10.9%, respectively (p<0.001). The corresponding odds ratios were 1.00, 0.78 (95% CI 0.62 to 0.99) and 0.69 (95% CI 0.50 to 0.94) after controlling for potential confounding factors. The frequency of BHR in subjects exercising <1 h, 1–3 h and ⩾4 h a week was 15.9%, 10.9% and 10.7%, respectively (p<0.001). The corresponding adjusted odds ratios were 1.00, 0.70 (95% CI 0.57 to 0.87) and 0.67 (95% CI 0.50 to 0.90). Physical activity was associated with BHR in all studied subgroups.
Conclusions: These results suggest that BHR is strongly and independently associated with decreased physical activity. Further studies are needed to determine the mechanisms underlying this association.
- BHR, bronchial hyperresponsiveness
- BMI, body mass index
- ECRHS II, European Community Respiratory Health Survey II
- FEV1, forced expiratory volume in 1 s
- FVC, forced vital capacity
Statistics from Altmetric.com
- BHR, bronchial hyperresponsiveness
- BMI, body mass index
- ECRHS II, European Community Respiratory Health Survey II
- FEV1, forced expiratory volume in 1 s
- FVC, forced vital capacity
The prevalence of asthma has increased over the last few decades, becoming a major public health problem, especially in the developed world. Any intervention that reduces the risk of asthma, even modestly, would have a major effect on public health. In this respect, physical inactivity is a frequent and modifiable potential risk factor.
Studies have shown that a large proportion of the population are less physically active than is necessary for maintaining good health.1 It is widely accepted that regular physical activity is strongly associated with reduced rates of long-term diseases such as cancer, cardiovascular events and non-insulin-dependent diabetes mellitus. However, there is much less evidence for the potential beneficial effect of physical activity on lung health.
Some prospective studies in children2 and in adult twins3 have shown that the development of asthma was associated with decreased physical activity. Although exercise can induce bronchospasm in patients with asthma, several recent studies have highlighted the health benefits of exercise such as an improved level of cardiorespiratory fitness and quality of life.4–6 Physical exercise may also improve lung function and health in patients with cystic fibrosis which is thought to be due in large part to secretion clearance, and it is an essential component of pulmonary rehabilitation in patients with chronic obstructive pulmonary disease (COPD), probably by improving the level of cardiovascular fitness.7
Bronchial hyperresponsiveness (BHR) is a risk factor for the development8,9 and progression of asthma.10,11 It is considered one of the hallmarks of airway inflammation in asthma, and is increasingly being recognised as a clinical end point for therapeutic intervention in asthma management. Assessment of bronchial responsiveness as an objective measure is advocated in epidemiological studies on asthma,12 particularly in multicentre studies.13
The relationship between usual levels of physical activity and BHR is unknown in the general population. This large population-based study aimed to investigate the association between usual levels of physical activity and BHR in a representative sample of adults participating in the European Community Respiratory Health Survey II (ECRHS II).14
METHODS
Study design
The methods for ECRHS I and ECRHS II have been published in more detail elsewhere,14,15 and further information is available from the study website (http://www.ecrhs.org).
ECRHS I (1991–1993)
Centres from 11 countries (Iceland, Norway, Sweden, Estonia, Germany, France, Switzerland, Spain, Italy, UK and USA) participated in ECRHS I. Each centre represented an area defined by pre-existing administrative boundaries with a population of at least 150 000 people. For stage 1, at least 1500 men and 1500 women aged 20–44 years randomly selected from a community-based sampling frame were sent a short postal questionnaire. For stage 2, a sub-sample of 600 responders was randomly selected and invited to a local testing centre to answer a more detailed administered questionnaire and perform lung function measurement by spirometry and bronchial responsiveness challenge with methacholine. In most centres a further sample of symptomatic subjects was also invited to participate. These subjects are not included in this analysis.
ECRHS II (1998–2002)
Participants in stage 2 of ECRHS I were eligible for ECRHS II. Subjects completed a short postal questionnaire and were then invited to the local testing centre where, as in ECRHS I, they answered a detailed administered questionnaire that included questions on physical activity. Twenty-four centres taking part in ECRHS II performed bronchial responsiveness challenge with methacholine.
Questionnaire
A standardised questionnaire was administered by trained interviewers to collect sociodemographic details and information on respiratory symptoms during the preceding 12 months, smoking history, allergic symptoms, family history of asthma, home and work environment, medication and usual physical activity.
Physical activity assessment
Usual physical activity per week was estimated by asking participants how often (frequency) and for how many hours (duration) a week they usually exercised so much that they got out of breath or sweaty. The responses for frequency were: “every day”, “4–6 times a week”, “2–3 times a week”, “once a week”, “once a month”, “less than once a month” and “never”. For statistical analyses we grouped together the first two categories, the next two categories and then the last three categories. The responses for duration were: “7 hours or more”, “about 4–6 hours”, “about 2–3 hours”, “about 1 hour”, “about half an hour” and “none”. For statistical analyses we grouped together the first two categories, the next two categories and then the last two categories.
Despite the fact that the two physical activity questions were correlated, we analysed them separately. We also analysed a combined variable based on the responses to these two questions. Subjects who exercised with a frequency of “2–3 times a week” or more and with a duration of “about 1 hour a week” or more were classified as “active”. The rest were classified as “inadequately active”. The cut-off values for these categorisations were based on earlier publications16,17 and the more conservative recommendations18 for health-promoting physical activity.
Height and weight
In a few centres participants were asked for their height and weight which were measured only if they were unsure. In the other centres height was measured and participants were weighed in light clothing without shoes. Weight was recorded to the nearest kilogram at each survey.19
Lung function testing
The maximum forced expiratory volume in 1 s (FEV1) and maximum forced vital capacity (FVC) from up to five technically acceptable blows were determined according to the American Thoracic Society criteria.20 Of the 24 centres that measured bronchial responsiveness at each survey, 20 used the same spirometer (Biomedin srl, Padova, Italy). The remaining centres used different spirometers. These differences in equipment did not lead to heterogeneity in lung function assessment compared with other centres.19
Methacholine challenge
Details of methacholine challenge have been described elsewhere.13,21 Bronchial responsiveness to methacholine was measured in eligible subjects (those having an FEV1 of at least 70% predicted and more than 1.5 l and not suffering from heart disease or epilepsy, not pregnant or breastfeeding and not taking a β blocker). Methacholine was delivered via a Mefar dosimeter (Mefar, Bovezzo, Italy). The test started with inhalation of saline diluent, with the maximum post-diluent FEV1 being recorded as the control value. FEV1 was measured 2 min after each inhalation of methacholine. The test was stopped either when FEV1 fell by 20% or when a maximum cumulative dose of 2 mg had been given according to the protocol.
Total and specific immunoglobulin E (IgE)
Blood samples were collected and total serum IgE and IgE specific to cat, house dust mite (Dermatophagoides pteronyssinus), Cladosporium and timothy grass were measured centrally at King’s College London in ECRHS II using the Phamacia CAP system. The measurement range was 2–2000 kU/l for total IgE and 0.35–100 kU/l for specific IgE.
All data presented in this report (including BHR and physical activity assessments) come from ECRHS II and are cross-sectional (physical activity questions were not included in the ECRHS I).
The study was approved for each centre by the appropriate institutional or regional ethics committee and informed written consent was obtained from each participant. Quality controls were carried out at different levels. All field workers involved in the study received identical training, quality control visits were made by ECRHS investigators and equipment was subject to regular quality controls.
Data analysis
Body mass index (BMI) was calculated as weight in kilograms divided by the square of the height in metres. It was analysed as a categorical variable divided into normal weight (<25 kg/m2), overweight (25 to <30 kg/m2) and obese (⩾30 kg/m2). The subjects were categorised into four groups according to smoking habits: never smokers, past smokers, moderate smokers (<20 cigarettes per day) and heavy smokers (⩾20 cigarettes per day).
“Current asthma” was defined as currently using asthma medication or as reporting asthma attacks during the previous 12 months. “Asthma-like symptoms” were defined as wheeziness, shortness of breath at rest and/or nocturnal shortness of breath at rest during the last 12 months. Total IgE was transformed logarithmically. “Atopy” was defined as a positive specific IgE (>0.35 kU/l) to at least one of the four allergens tested. Each allergen was included individually in the multivariable model because each allergen is differently related to BHR.22
Linear regression was used to calculate the internally derived predicted value of FEV1 based for each sex on age and height. The difference between measured and predicted values (residual FEV1) was used in multivariate analyses. In tables 1 and 3 the results are presented using a reconstituted FEV1 (ie, residual FEV1 + mean value of the group) to make them more explicit,. FEV1 as a percentage of the predicted value (FEV1 % pred) and FVC as a percentage of the predicted value (FVC % pred)23 were also considered in the multivariate analyses.
Characteristics of participants included in the analysis
BHR was defined as a decrease in FEV1 of at least 20% of its post-saline value for a maximum dose of 2 mg methacholine. As well as this binary response variable, a dose-response slope used for between-centre analyses in the ECRHS13 was used to analyse the response to methacholine as a continuous variable in a linear regression model. This allows the data from all subjects to be interpreted regardless of whether FEV1 declined by 20% during the test or not. The term “slope” is used for a transformed log slope as used in the ECRHS, with a low “slope” indicating high BHR.13
Associations of frequency and duration of physical activity (three categories each) with the categorical variables were assessed using the χ2 test and with the continuous variables using ANOVA. Logistic regression models were fitted using BHR as the dependent variable and physical activity as an independent variable. The models were adjusted for country, sex, age, BMI (three categories), smoking (four categories), education level, specific and total IgE, asthma-like symptoms, current asthma, family history of asthma and FEV1. Multiplicative interactions (smoking/BMI, age/sex and age/smoking) were assessed using product-terms in the fully adjusted logistic model but had no effect on the association. Sensitivity analysis was performed to test the consistency of the association between BHR and physical activity in men and women, classes of BMI, smoking categories and according to atopy, asthma and asthma-like symptom status. We also tested the association after excluding subjects who answered positively to the question: “Do you avoid taking vigorous exercise because of wheezing or asthma?”.
Statistical analysis was carried out using SAS V.8.2 (SAS Institute Inc, Cary, North Carolina, USA). Tests for heterogeneity and combined odd ratios were determined using standard methods for meta-analysis, with country included in the model as a random effect, using the STATA package (STATA Corporation, College Station, Texas, USA). p values <0.05 were considered significant.
RESULTS
Characteristics of subjects
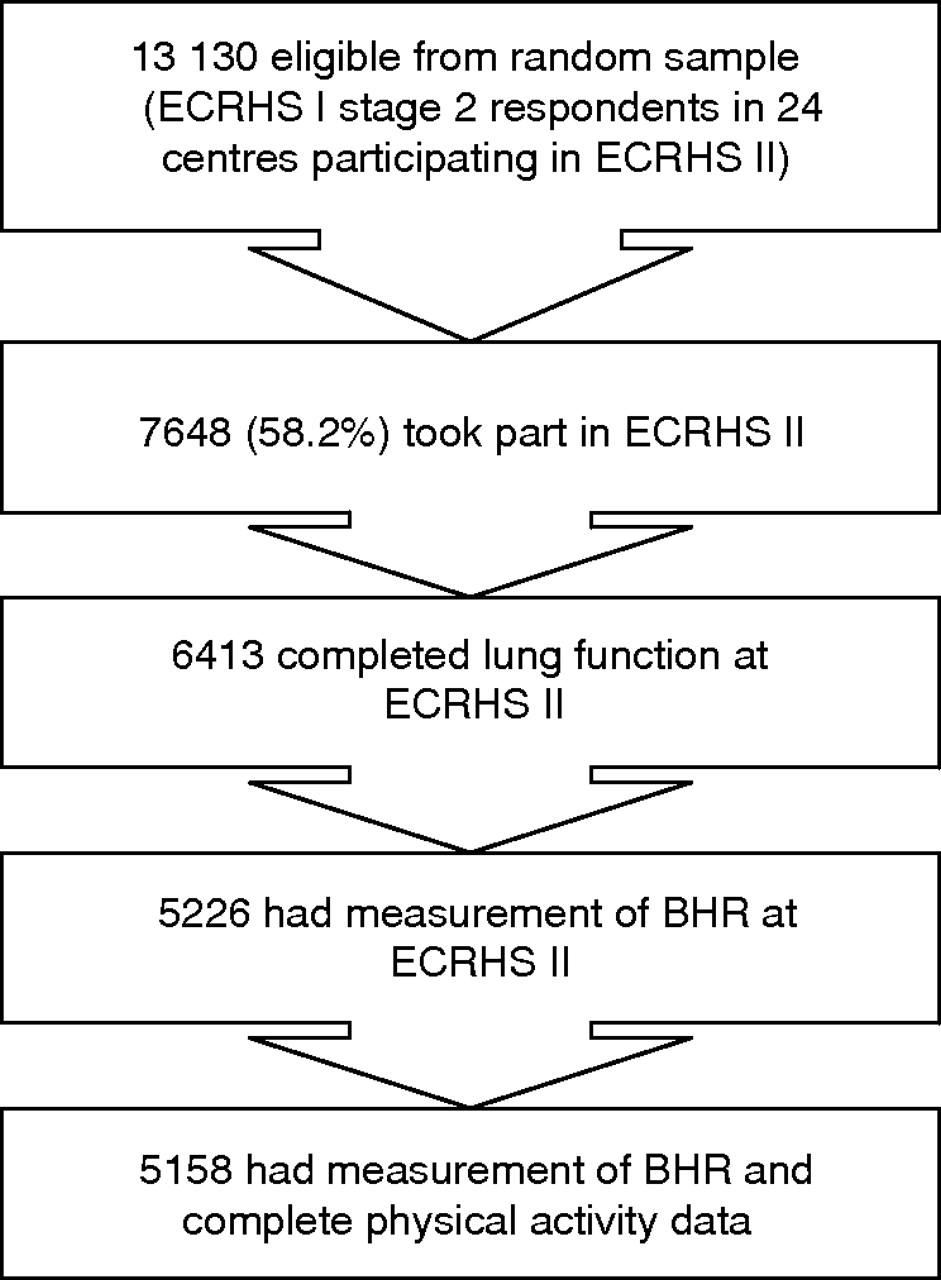
A total of 13 130 people randomly selected in 24 centres were eligible to take part in ECRHS II. Details of the response to ECRHS II have been reported previously.24 Of these, 7648 (58.2%) were traced and responded to the main questionnaire at ECRHS II, 6413 of whom had their lung function measured and 5158 had a valid airway challenge and complete physical activity data collected at ECRHS II (fig 1).
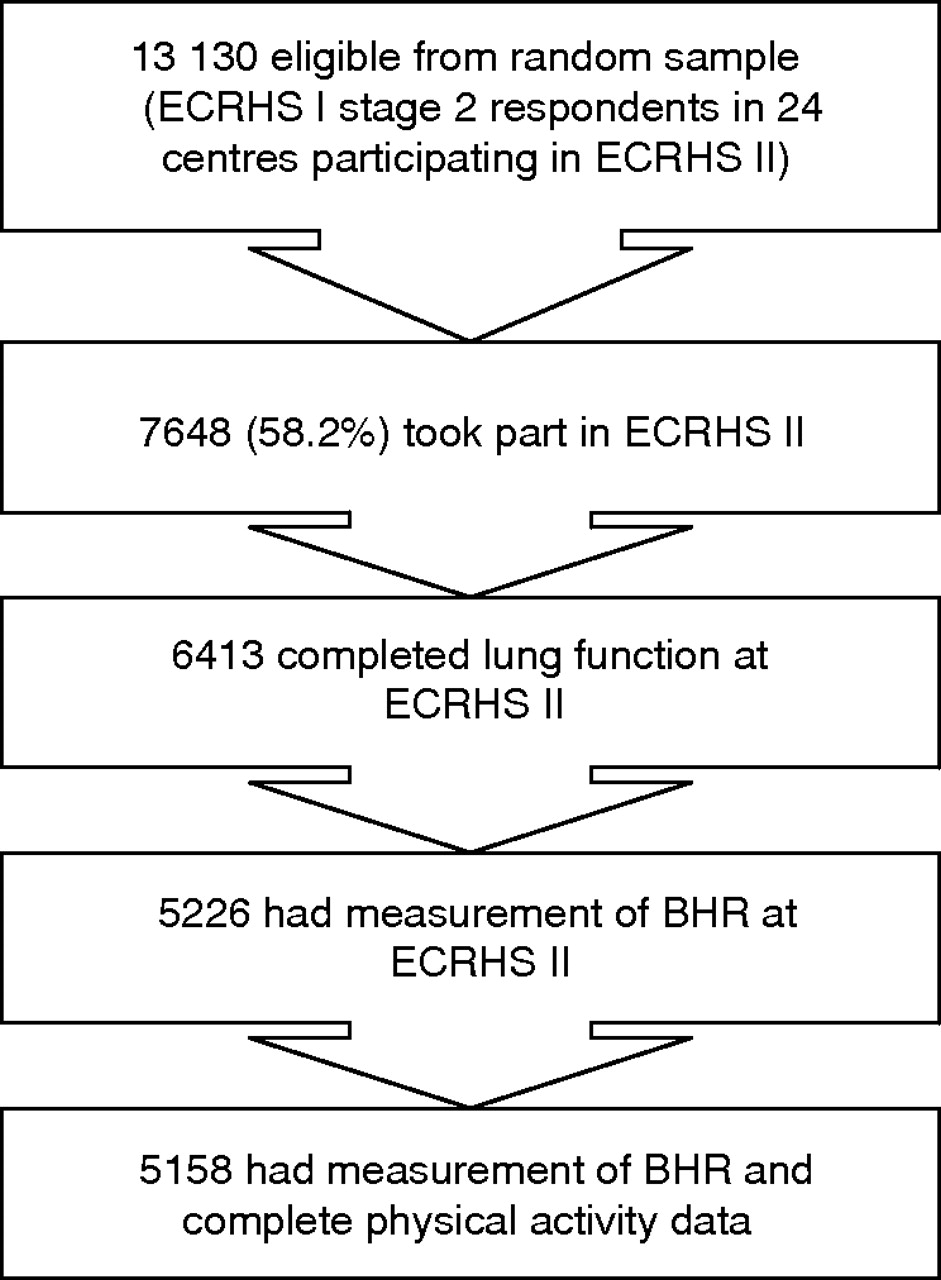
Subjects participating in the present analysis of the European Community Respiratory Health Survey II (ECRHS II). BHR, bronchial hyperresponsiveness.
The age range of the 5158 subjects was 28.0–56.5 years (mean 42.6). Table 1 shows the characteristics of the participants and their distribution by sex. The prevalence of BHR in this general population was 13.0%, with women having a higher prevalence than men (p<0.001). Overall, 60.0% of the population usually exercised to breathlessness or sweating either once a week or less than once a week, 26.5% exercised 2–3 times a week and 13.5% exercised regularly at least four times a week. The duration of exercise was <1 h per week for 41.5% of population, 1–3 h per week for 42.4% and ⩾4 h per week for 16.1%.
BHR, physical activity and potential confounding factors
The associations between BHR and potential confounding factors are shown in table 2. BHR was significantly more frequent in subjects with a low level of education than in subjects with a high level of education (p = 0.0024). It was also more prevalent in obese subjects (p = 0.038), subjects with atopy, (p<0.001) those with asthma (p<0.001), asthma-like symptoms (p<0.001) or a family history of asthma (p<0.001). BHR was positively associated with smoking in women but not in men. Subjects with BHR had significantly lower FEV1 levels than those without BHR (3.07 (0.91) l/s vs 3.67 (0.99) l/s, p<0.001). This association was similar for men and women (results not shown).
Frequency of bronchial hyperresponsiveness (BHR) according to potential confounding factors
Factors associated with the duration of physical activity are shown in table 3. Older subjects tended to have lower physical activities than younger subjects. Obese subjects (BMI >30 kg/m2) and current smokers were more prevalent in the lower physical activity category. Subjects with a high level of education were more active than subjects with a low level of education. Similar results were observed for frequency of physical activity (data available from the authors).
Relationships between the duration of physical activity per week and potential confounding factors
BHR and physical activity
BHR was negatively associated with the frequency and duration of physical activity (p<0.001 for each). The prevalence of BHR was 14.5% for subjects exercising once a week or less, 11.6% for subjects exercising 2–3 times a week, and 10.9% for those exercising four or more times a week (p<0.001). The corresponding adjusted ORs were 1.00, 0.78 (95% CI 0.62 to 0.99) and 0.69 (95% CI 0.50 to 0.94), respectively, after controlling for country, sex, age, BMI, smoking, education level, specific and total IgE, asthma-like symptoms, current asthma, family history of asthma and residual FEV1 (table 4). For duration of physical activity the prevalence of BHR was 15.9% for subjects exercising <1 h per week, 10.9% for subjects exercising for 1–3 h per week, and 10.7% for those exercising ⩾4 h per week (p<0.001). The corresponding adjusted ORs were 1.00, 0.70 (95% CI 0.57 to 0.87) and 0.67 (95% CI 0.50 to 0.90) (table 4). Including both FEV1 (as percentage predicted) and FVC (as percentage predicted) in the models instead of residual FEV1 gave similar results. The ORs were 0.79 (95% CI 0.62 to 1.01) in subjects exercising 2–3 times a week and 0.64 (95% CI 0.46 to 0.90) in those exercising ⩾4 times a week compared with subjects exercising once a week or less (reference group). Similarly, the ORs for BHR were 0.71 (95% CI 0.57 to 0.89) in subjects exercising for 1–3 h a week and 0.70 (95% CI 0.51 to 0.95) in those exercising ⩾4 h a week compared with subjects exercising <1 h a week (reference group).
Association between BHR and categories of physical activity by logistic regression
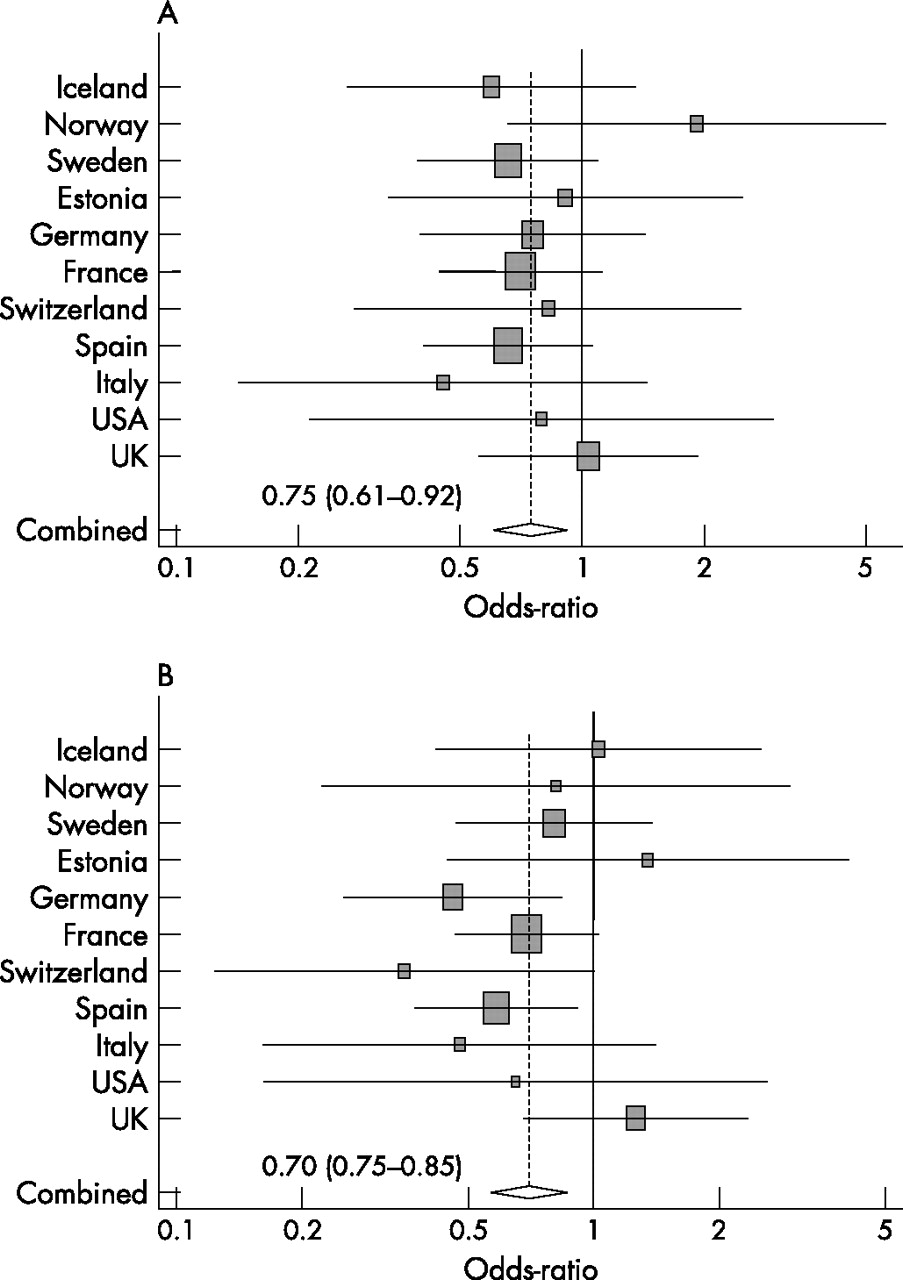
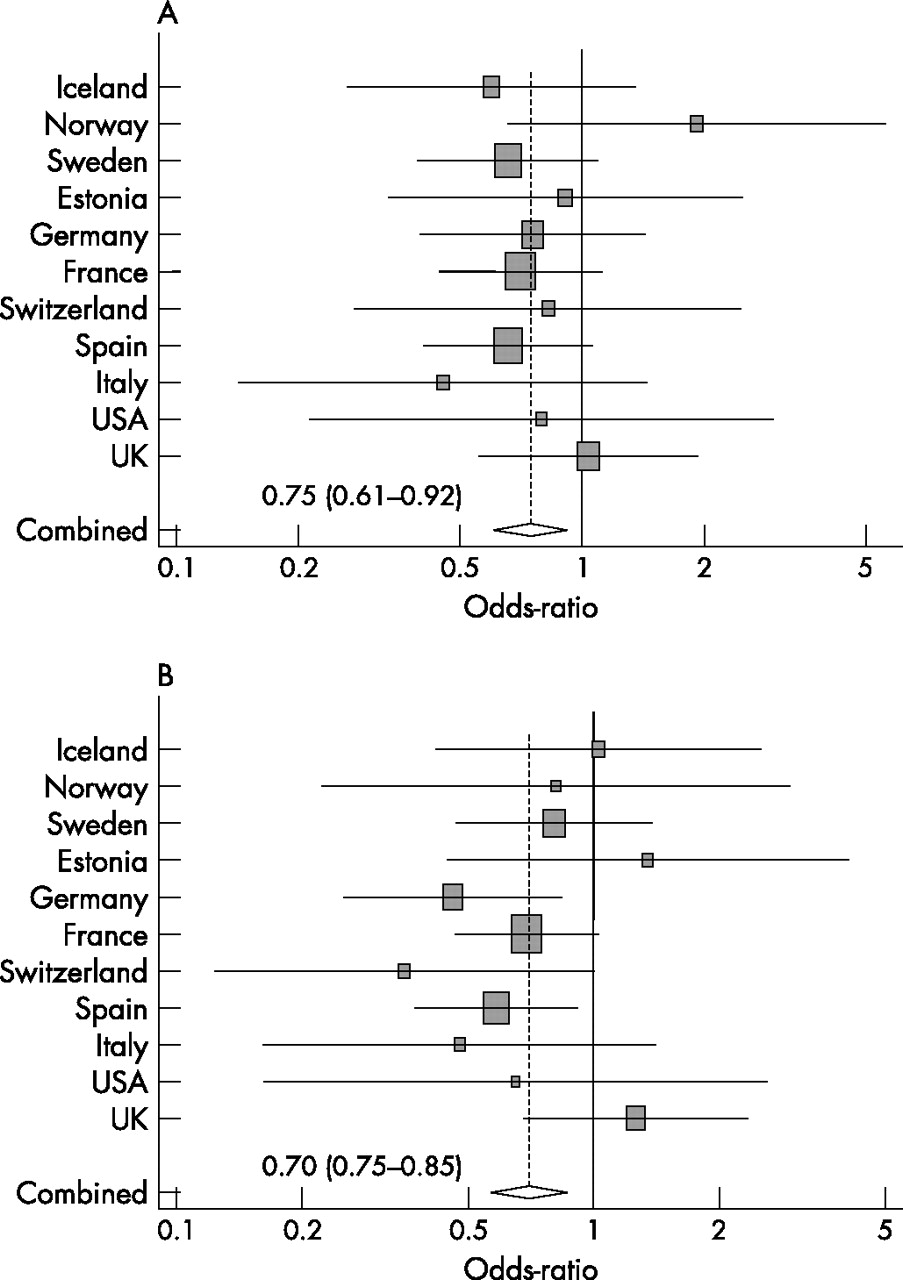
We also found that the adjusted OR for BHR in subjects exercising two or more times a week AND for one or more hours (considered active) versus the other subjects (considered inadequately active) was 0.74 (95% CI 0.60 to 0.92). We found no heterogeneity between countries in the association between BHR and physical activity (fig 2).
{kind=link}
{kind=link}
Multivariable adjusted odds ratios (95% confidence interval) for the association between bronchial hyperresponsiveness and (A) frequency of physical activity (exercise ⩾2 times/week vs ⩽1 time/week) and (B) duration of physical activity (exercise ⩾1 h/week vs <1 h/week) by country adjusted for sex, age, body mass index, smoking, education level, specific and total IgE, respiratory symptoms, current asthma, family history of asthma and residual forced expiratory volume in 1 s. The area of the squares is proportional to the reciprocal of the variance of the estimate for the country. The diamond represents the combined odds ratio, calculated using country as a random effect, with its 95% confidence interval. The dashed line, plotted vertically through the combined odds ratio, crosses the horizontal lines of all individual country results (p values for the test of heterogeneity between countries 0.83 and 0.40 for (A) and (B) respectively).
There was no significant interaction between physical activity and any of the studied risk factors in determining BHR. Hence, a similar pattern of results was observed in men and in women, BMI classes, smoking categories, and in atopic and non-atopic subjects (results not shown). In addition, after excluding subjects with asthma or asthma-like symptoms, the negative association between physical activity and BHR remained significant (n = 3580, adjusted OR 0.73 (95% CI 0.57 to 0.95)). Even after excluding all subjects with any respiratory symptoms (asthma-like symptoms, chronic cough and/or phlegm), atopy and/or asthma, the result was unchanged (n = 2790, adjusted OR 0.70 (95% CI 0.50 to 0.98)) and the same result was observed when we excluded 127 subjects who avoided taking vigorous exercise because of wheezing or asthma (n = 2777, adjusted OR 0.68 (95% CI 0.49 to 0.96)). Finally, as atopy, asthma and smoking correlated strongly with BHR, additional multiple regression analysis was performed in never smokers without asthma and atopy (n = 1371, adjusted OR 0.62 (95% CI 0.39 to 1.00)).
Dose-response slope and physical activity
A multiple linear regression confirmed the consistent relationship between physical activity and the dose-response slope. Bronchial responsiveness decreased with increasing frequency or duration of exercise after adjustment for the same independent variables as shown in table 5.
Relationship between ECRHS “slope”* of bronchial hyperresponsiveness (BHR) and levels of physical activity by multivariable linear regression
DISCUSSION
The results from this large scale population-based study show a negative association between physical activity and BHR. This association was consistent across several subgroups and was independent of potential confounders for BHR and physical activity. To the best of our knowledge, this is the first study to investigate the association between physical activity and BHR in adults from the general population. The study shows that the cut-off point for the frequency (or duration) of physical activity at which BHR would be significantly reduced is relatively low. This suggests that, if causal, even modest physical activity can have a beneficial effect on BHR.
The participation rate at ECRHS II was 58.2% (7648 of 13 130) which is comparable to several recent population studies and higher than that of the one population study of change in BHR.21 Eligible men were slightly more likely to respond to the main questionnaire at ECRHS II than women. Responders were slightly older than non-responders at baseline (mean age 34.1 years vs 33.8 years). No significant difference in baseline lung function was observed between responders and non-responders (mean FEV1 3.90 l vs 3.86 l). Subjects lost to follow-up were more frequently smokers at baseline. These small differences were unlikely to bias the reported relations between physical activity and BHR substantially. Of the 7648 participants, 16% completed the questionnaire only and did not perform lung function tests. Of the 6413 with an acceptable FEV1 measurement, 519 (8.1%) had contraindications for the methacholine test and bronchial responsiveness was measured in 5158 (80.4%); thus only 39% of the original population were included in the present analysis. The distributions of smoking and atopy status were comparable between subjects with and without bronchial responsiveness data. Subjects who were tested for BHR had slightly greater BMI and slightly greater FEV1 than those not tested. Asthma and asthma-like symptoms were more common in subjects who did not perform a methacholine challenge than in those with BHR data. Inadequately active subjects were over-represented in those without BHR data. It therefore seems likely that the association between physical activity and BHR is underestimated in our study.
Some studies have investigated the relationship between inactivity and increased levels of BHR in children. In a cross-sectional study, a negative relationship between physical activity and BHR was shown in children currently with asthma but this relationship was not observed in children without asthma.25 A longitudinal study of 757 previously asymptomatic children found a weak association between physical fitness in childhood and the response of the airways to methacholine at follow-up, and physical fitness tended to be correlated with a reduced risk of developing adolescent asthma.26 Another prospective study of 262 twin pairs showed that the twin who participated in conditioning exercise had a lower risk of asthma than the sedentary twin.3 Previous studies of the relationship between physical activity and BHR in adults have focused on athletes and showed positive associations between BHR and intense exercise.27–29 In such populations, this positive relationship may be related to thermal stimuli—heat loss that leads to vascular engorgement as the airways warm back up after intense exercise, initiating bronchoconstriction. Alternatively, it may be related to osmotic stimuli—water loss that leads to a change in airway osmolarity, initiating epithelial and mast cell activation and resulting in the release of inflammatory mediators in the airways that cause bronchoconstriction.30 However, these studies carried out in high level sportsmen cannot be compared with our study of subjects from the general population.
Two outcome definitions of bronchial responsiveness were used—the dichotomous BHR variable and the logarithmically transformed slope, as suggested by Chinn et al.13 Whichever outcome was used, the results were similar.
The validity of the physical activity data may be questionable because there is no gold standard for assessment of physical activity. Although physical activity was assessed by a standardised interviewer-administrated questionnaire, as in most epidemiological studies,31 the responses reflect self-assessment of physical activity level or frequency. However, the questions used in the ECRHS have been validated previously.32–34 Moreover, assessing physical activity by questionnaire may be the only practical method of collecting data in large epidemiological studies with intensive respiratory tests such as the ECRHS. Given that self-reported physical activity may not reveal the real levels of physical activity, which may be overestimated,35 the results may be influenced by some misclassification. However, it was possible to categorise the subjects and misclassification is likely to be random as the physical activity data were collected before the BHR test was carried out. Such a bias, if any, would therefore lead to an underestimation of the true association.
The mechanisms linking physical activity to BHR are not clear. Moderate and vigorous physical activity may be one component of a healthy lifestyle or may be a marker of a generally better constitution. We therefore adjusted for possible confounding influences of age, smoking status, BMI and educational levels, and still observed the independent associations between BHR and physical activity. Moreover, some over-adjustment may have occurred for BMI. Obesity and being overweight may partly be a result of low physical activity,36,37 and adjusting for BMI would lead to underestimation of the associations between physical activity and BHR. Some subjects with asthma or respiratory symptoms may refrain from vigorous physical activity to avoid unpleasant respiratory effects. However, when we adjusted for asthma and respiratory symptoms and, more importantly, stratified for these variables, the results did not change (results not shown). Also, the exclusion of subjects who avoided taking vigorous exercise because of wheezing or asthma had no effect on the results. We further reduced the potential for reverse causation, that is, serious disease causing low physical activity rather than vice versa, by asking subjects whether they were disabled from walking due to their diseases. The exclusion of these subjects (n = 361) also had almost no effect on the observed association (results available from authors).
A more plausible hypothesis is that physical activity might influence airway physiology and BHR. A deep inspiration, as in exercise, seems to be the first line of defence against bronchospasm (bronchoprotective effect) and can partially reverse it once bronchoconstriction is established (bronchodilatory effect) because of its effect on the constriction of smooth airway muscles.38–41 It has therefore been suggested that a decrease in the amount of these sighs or periodic expansions of the lungs while sedentary may contribute to non-specific BHR in children.42 Another possible explanation is that moderate physical activity might be associated with a reduction in systemic inflammation. Physical activity has been shown to be associated with an improvement in the lipoprotein profile and a reduction in the level of some inflammatory markers (such as plasma fibrinogen and C-reactive protein).43–46 On the other hand, chronic systemic inflammation has recently been shown to be associated with BHR.47
The strengths of the present study are its large size, the use of high quality data from a random general population sample, the use of a standardised questionnaire and the strictly standardised assessment of BHR in all participating countries. The percentage of BHR (13%) observed in our study was comparable to that obtained in other population-based studies by different methods.48 The present study confirmed previous findings that sex, BMI, smoking, atopy, asthma-like symptoms and asthma are associated with an increased risk of BHR. The observed associations of physical activity with age, BMI, smoking habits and education level are also consistent with previously published results.49 However, our findings should be considered in the context of the study limitations. First, a cause-and-effect relationship cannot be established between exercise and BHR because of the cross-sectional design of the study. Second, despite controlling for a large number of potentially confounding variables in our multivariable analyses, we are unable to completely exclude residual confounders due to unknown factors.
In conclusion, this study shows a strong and consistent negative relationship between physical activity and BHR in adults. If causal, our findings suggest that relatively small amounts of physical activity would markedly reduce BHR in the general population. This implies that another beneficial effect of physical activity may be added to the already known benefits. Further data are needed to clarify the relationship between physical activity and BHR and to determine the optimal amount (frequency and duration) and type of physical activity required. If confirmed, our results may contribute to the development of primary prevention programmes for pulmonary diseases.
REFERENCES
Footnotes
-
Published Online First 22 November 2006
-
RS had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: RS, BL, FN, and MZ. Data collection in local centres: BL, JA, RM, JH, CJ, JS, CS, MW, PB, and FN. Analysis and interpretation of data: RS, BL, DS, FN, and MZ. Drafting of the manuscript: RS, BL, FN, and MZ. Interpretation and presentation of the results: All authors. Study supervision: FN and MZ.
-
The coordination of ECRHS II was supported by the European Commission as part of their Quality of Life programme. The following bodies funded the local studies in ECRHS II in this article. Albacete—Fondo de Investigaciones Santarias (grant code: 97/0035-01, 99/0034-01, and 99/0034-02), Hospital Universitario de Albacete, Consejeria de Sanidad. Barcelona—Fondo de Investigaciones Santarias (grant code: 99/0034-01, and 99/0034-02), Red Respira (RTIC03/11 ISC IIF). Basel—Swiss National Science Foundation, Swiss Federal Office for Education & Science, Swiss National Accident Insurance Fund (SUVA). Bergen—Norwegian Research Council, Norwegian Asthma & Allergy Association (NAAF), Glaxo Wellcome AS, Norway Research Fund. Bordeaux—Institut Pneumologique d’Aquitaine. Erfurt—GSF–National Research Centre for Environment & Health, Deutsche Forschungsgemeinschaft (DFG) (grant code FR 1526/1-1). Galdakao—Basque Health Department. Goteborg—Swedish Heart Lung Foundation, Swedish Foundation for Health Care Sciences & Allergy Research, Swedish Asthma & Allergy Foundation, Swedish Cancer & Allergy Foundation. Grenoble—Programme Hospitalier de Recherche Clinique-DRC de Grenoble 2000 no. 2610, Ministry of Health, Direction de la Recherche Clinique, Ministere de l’Emploi et de la Solidarite, Direction Generale de la Sante, CHU de Grenoble, Comite des Maladies Respiratoires de l’Isere. Hamburg—GSF–National Reasearch Centre for Environment & Health, Deutsche Forschungsgemeinschaft (DFG) (grant code MA 711/4-1). Ipswich and Norwich—National Asthma Campaign (UK). Huelva—Fondo de Investigaciones Santarias (FIS) (grant code: 97/0035-01, 99/0034-01, and 99/0034-02). Montpellier—Programme Hospitalier de Recherche Clinique-DRC de Grenoble 2000 no. 2610, Ministry of Health, Direction de la Recherche Clinique, CHU de Grenoble, Ministere de l’Emploi et de la Solidarite, Direction Generale de la Sante, Aventis (France), Direction Régionale des Affaires Sanitaires et Sociales Languedoc-Roussillon. Oviedo—Fondo de Investigaciones Santarias (FIS) (grant code: 97/0035-01, 99/0034-01, and 99/0034-02). Paris—Ministere de l’Emploi et de la Solidarite, Direction Generale de la Sante, UCBPharma (France), Aventis (France), Glaxo France, Programme Hospitalier de Recherche Clinique-DRC de Grenoble 2000 no. 2610, Ministry of Health, Direction de la Recherche Clinique, CHU de Grenoble. Pavia—Glaxo-SmithKline Italy, Italian Ministry of University and Scientific and Technological Research (MURST), Local University Funding for Research 1998 & 1999 (Pavia, Italy). Portland—American Lung Association of Oregon, Northwest Health Foundation, Collins Foundation, Merck Pharmaceutical. Reykjavik—Icelandic Research Council, Icelandic University Hospital Fund. Tartu—Estonian Science Foundation. Turin—ASL 4 Regione Piemonte (Italy), AOCTO/ICORMA Regione Piemonte (Italy), Ministero dell’Università edella Ricerca Scientifica (Italy), Glaxo Wellcome spa (Verona, Italy).Umeå—Swedish Heart Lung Foundation, Swedish Foundation for Health Care Sciences & Allergy Research, Swedish Asthma & Allergy Foundation, Swedish Cancer & Allergy Foundation. Uppsala—Swedish Heart Lung Foundation, Swedish Foundation for Health Care Sciences & Allergy Research, Swedish Asthma & Allergy Foundation, Swedish Cancer & Allergy Foundation. Verona—University of Verona; Italian Ministry of University and Scientific and Technological Research (MURST); Glaxo-SmithKline Italy.
-
Competing interests: None.