Article Text

Abstract
Background: Few population-based studies have evaluated the association between birth weight or gestation and subsequent clinically significant asthma.
Methods: Birth records of 37 349 Alaska residents <10 years of age who were enrolled in Medicaid for at least 365 days during 1999–2002 were linked to a Medicaid billing file. The occurrence of asthma and lower respiratory infections during the study period was categorised on the basis of standard International Classification of Diseases 9th Revision codes. The association between gestational age or small for gestational age status and asthma outcomes was adjusted for recent history of lower respiratory infection, years of Medicaid enrolment, age at enrolment and a variety of birth-related factors.
Results: Among children <5 years of age, the adjusted odds ratio (OR) for developing asthma decreased by 5.5% (95% confidence interval (CI) −0.2 to 10.9) and 7.9% (95% CI 5.2 to 10.4) per additional week of gestational age for children without and with any lower respiratory tract infection, respectively. For children ⩾5 years of age, the adjusted OR for developing asthma decreased by 3.4% (95% CI −2.8 to 9.8) and 3.7% (95% CI −2.0 to 9.2) per additional week of gestation for those without and with lower respiratory tract infection, respectively. Among all children with asthma, the adjusted OR for hospitalisation due to asthma decreased by 6.9% (95% CI 2.1 to 11.5) for each additional week of gestational age. Small for gestational age status was not significantly associated with asthma outcomes.
Conclusions: Preterm birth but not small for gestational age status predicted subsequent asthma outcomes. Adverse effects of preterm birth on asthma outcomes persist beyond age 5 years.
- LRI, lower respiratory infection
- SGA, small for gestational age
Statistics from Altmetric.com
Previous studies have found an increased risk of asthma among low-birth weight1–,4 or preterm4–,8 infants. Most of these studies have evaluated differences in lung function, such as forced vital capacity or the forced expiratory volume in 1 s, rather than differences in seeking clinical care. Preterm or low-birth weight birth may lead to physiological changes, but not impairment severe enough to lead to care seeking.
Additionally, previously identified associations might have resulted partly from confounding by respiratory tract infection.9–,12 Studies that have adjusted for respiratory tract infection during analysis13–,15 have generally found reduced effects of birth characteristics.14,15 Few of these studies have had large or population-based study groups. Thus, questions still remain regarding the contribution of birth characteristics to subsequent asthma independent of the risk of respiratory tract infections, whether measurable effects are of clinical significance, and if so whether clinically significant effects remain beyond early childhood. The current study evaluated Medicaid-enrolled Alaskans <10 years of age to determine whether low-birth weight or preterm birth was associated with future diagnosis of asthma when controlling for temporally associated lower respiratory tract infection.
METHODS
Healthcare in Alaska
During the study period, healthcare services in Alaska were delivered through a variety of private, public, non-profit, Native Corporation and Indian Health Service entities. Alaska Natives constituted the state’s largest racial minority and predominant rural residents, and usually received services through Native Corporation and Indian Health Service facilities. Care in most small villages was provided at clinics staffed by Village Health Aides, with support provided by physicians based at regional centres. For Medicaid enrolled people, all in-state facilities billed Medicaid regardless of where a specific individual obtained care.
As per 2001 census data, the proportion of all Alaska Natives <10 years of age enrolled in Medicaid ranged from 62% to 80% over the study period compared with 15–21% for non-Natives. Little differences in Medicaid enrolment percentages existed with regard to Anchorage and non-Anchorage residence.
Data sources
The methods for the construction of the Medicaid data file have been described previously.16,17 A file was constructed containing information on all children <10 years of age enrolled in Medicaid at some time from 1 January 1999 to 31 December 2002. An outcomes file was created that contained all provider, inpatient facility and outpatient clinic approved billing claims for all outcomes of interest (see case definitions below). A separate file contained data on asthma drugs.
To link the Medicaid and birth certificate files, the Alaska Bureau of Vital Statistics performed six steps. The great majority of children were linked through an exact match of social security number and at least 1 of 6 (42%) additional criteria, or through an exact match of first and last names and date of birth (56%); four additional steps were used to link the remaining 2%.
Available data from the birth certificate included birth weight and gestational age, place of residence at the time of birth, method of delivery, presence of multiple gestation birth, maternal and paternal age and education, and prenatal maternal tobacco, oral tobacco and alcohol use. Other than asthma and respiratory infection variables, analysed data from the Medicaid file included age, sex and race.
Definitions
Asthma
Asthma was defined as an approved claim for any asthma-related drug and care based on International Classification of Diseases, 9th Revision codes 493.0x–493.9x, the standard codes for asthma. Hospitalisation related to asthma included any approved claim for which asthma was recorded as a discharge diagnosis.
Lower respiratory illness
Lower respiratory illness was recognised as an approved claim for International Classification of Diseases, 9th Revision code 466.0 (bronchitis), 466.1 (bronchiolitis), 480–487 (pneumonia and influenza), 490 (bronchitis not specified as acute or chronic) or 510–511 (empyema and pleurisy).
Preterm birth
Preterm birth was confirmed through a birth certificate report of gestation <37 weeks, calculated as the period beginning with the first day of the last menstrual period to the day of birth.
Small for gestational age
Based on the published data,18 small for gestational age (SGA) was defined as a weight <10th centile for gestational age at birth.
Analysis
There were 72 642 in-state residents <10 years of age enrolled in Medicaid at some point during the 4-year study period, and 54 412 (75%) could be matched to the birth certificate file. Owing to concern that some children enrolled for only brief periods would not have an opportunity to be identified as having one of the study outcomes, we limited the analysis to the 41 341 children enrolled for >365 days over the course of the study. Of these, 37 349 had data available for all analysed variables.
The primary risk factors of interest were gestational age and birth weight. To avoid issues of multi-collinearity between these two variables, we used SGA status rather than birth weight. Children with a history of preterm or SGA birth may present more frequently with asthma because they have an increased risk of concurrent respiratory infection. The study databases, however, did not allow us to evaluate the possibility that early respiratory tract infection constitutes part of the causal pathway of any identified association between preterm birth and asthma. Specifically, in this study, the diagnosis of asthma could precede or follow the development of lower respiratory tract infections.
Univariate models were constructed to evaluate the association between asthma outcomes and sex,19 Alaska Native status and Anchorage residence,16,17 caesarean20 and multiple gestation birth,21 maternal age, education and prenatal tobacco use,22 and any lower respiratory tract infection (inpatient and outpatient). Separate univariate models were constructed for children <5 years and those aged 5–9 years. Alaska Native status was based on the race reported during the first year of Medicaid enrolment, whereas Anchorage residence was determined at birth.
Multivariate models were constructed for two outcomes: any asthma diagnosis among all children and in-patient asthma admission among children with asthma. All models were adjusted for the following potential confounders: maternal prenatal tobacco use, Alaska Native status, Anchorage residence, caesarean and multiple gestation birth, mother’s age, mother’s education, years of Medicaid enrolment (minimum of 1 year) and age at Medicaid enrolment. In addition to these variables, stratification by lower respiratory infection (LRI) and age group varied by outcome (see below).
We constructed four sets of multivariate models. For all models we determined whether an interaction was present between SGA and gestational age; as an interaction was not identified during any analysis, these results are not presented. The four model sets were as follows:
In model set 1, gestational age was defined as a categorical variable with groups <32 weeks, 32–36 weeks and ⩾37 weeks. Asthma was the outcome variable, and models were stratified simultaneously by age (<5 and ⩾5 years) and history of LRI for a total of four strata.
In model set 2, analysis was restricted to children with asthma and the outcome was inpatient asthma. Gestational age groups were identical to those in the previous model set. Stratification by age group and LRI status was not possible when evaluating asthma hospitalisation due to asthma among children with asthma, as small numbers prevented meaningful analysis.
In model set 3, gestational age was left as a continuous variable to determine the overall percentage decrease in the odds ratio (OR)—per additional week of gestational age—for presentation for asthma or inpatient asthma among children with asthma. For models evaluating asthma as an outcome, stratification was done simultaneously by age group and history of LRI. Stratification was not possible when evaluating hospitalisation among children with asthma as small numbers prevented meaningful analysis.
In model set 4, to allow graphical representation of OR by gestational age, gestational age was categorised into <28 weeks, ⩾37 weeks, and 1 or 2-week periods between these two extremes. Outcomes included asthma and inpatient asthma among children with asthma. None of the models was stratified by history of LRI or age group as the number of children within gestational age categories was too small for meaningful analysis.
All analyses were conducted using SAS V.8.2 proc logistic procedure software.
RESULTS
Population characteristics
Of the 37 349 children studied, there were 1565 (4.2%) with asthma, of whom 236 (15.1%) had been hospitalised at least once due to asthma. There were 18 129 (48.5%) Alaska Natives, 12 498 (33.5%) Anchorage residents and 24 633 (66.0%) children <5 years of age. Among all children studied, 12 038 (32.2%) had a lower respiratory tract infection, of whom 1542 (12.8%) were hospitalised. Among 24 633 children aged <5 years, 9617 (37.2%) had a lower respiratory tract infection, of whom 1164 (12.1%) were hospitalised; 4298 total cases and 808 hospitalisations were associated with bronchiolitis. Among all children, 41 (0.1%) were born at <32 weeks and SGA, 435 (1.2%) at <32 weeks and not SGA, 401 (1.1%) at 32–36 weeks and SGA, 2480 (6.6%) at 32–36 weeks and not SGA, 2228 (6.0%) at ⩾37 weeks and SGA, and 31 764 (85.0%) at ⩾37 weeks and not SGA.
Univariate analysis
Among children <5 years of age, of the outcomes evaluated, a history of lower respiratory illness was most strongly associated with asthma and hospitalisation due to asthma among children with asthma (table 1⇓). Other variables associated with one or both outcomes included Anchorage residence, Alaska Native status, multiple gestation and caesarean birth, and gestational age. Findings were similar for children 5–9 years of age (table 2⇓).
Univariate association between risk factors and asthma or hospitalisations due to asthma among children <5 years old enrolled in Medicaid, Alaska, January 1999–December 2002
Univariate association between risk factors and asthma or hospitalisations due to asthma among children aged 5–9 years enrolled in Medicaid, Alaska, January 1999–December 2002
Multivariable analysis
Model set number 1
In models with gestational age grouped into three categories, the OR for the development of asthma was between 2.0 and 2.3 for gestational age <32 weeks regardless of stratification by age group at enrolment or history of LRI (tables 3⇓ and 4⇓). However, associations were not significant for all strata. Gestational age of 32–36 weeks was significantly associated with the development of asthma only for children <5 years of age with a history of LRI (OR 1.6, 95% confidence interval (CI) 1.2 to 2.0) and children aged ⩾5 years with no history of LRI (OR 1.6, 95% CI 1.0 to 2.5). Small for gestational age was not significantly associated with asthma across all strata.
Association between asthma and gestational age or small for gestational age status among Medicaid-enrolled children <5 years of age, stratified by lower respiratory infection; Alaska, January 1999–December 2002
Association between asthma and gestational age or small for gestational age status among Medicaid-enrolled children 5–9 years of age, stratified by lower respiratory infection; Alaska, January 1999–December 2002
Model set number 2
In the model evaluating the association between gestational age and hospitalisation for asthma among children with asthma, stratification by LRI and age group status was not performed. In this unstratified model, gestational age <32 weeks, but not 32–36 weeks, was associated with hospitalisation for asthma when compared with children of normal gestation (table 5⇓). Small for gestational age status was associated with asthma, but the association did not achieve statistical significance.
Association between inpatient asthma and gestational age or small for gestational age status among 1565 Medicaid-enrolled children with asthma <10 years of age; Alaska, January 1999–December 2002
Model set number 3
When gestational age was treated as a continuous variable, the adjusted OR for developing asthma decreased by 7.6% (95% CI 5.7 to 9.5) per additional week of gestational age among all children. Among children with asthma, the adjusted OR for hospitalisation due to asthma decreased by 6.9% (95% CI 2.1 to 11.5) for each additional week of gestational age.
Among children <5 years of age, the adjusted OR for developing asthma decreased by 5.5% (95% CI −0.2 to 10.9) and 7.9% (95% CI 5.2 to 10.4) per additional week of gestational age for children without and with any lower respiratory tract infection, respectively. For children 5–9 years of age, the adjusted OR for developing asthma decreased by 3.4% (95% CI −2.8 to 9.8) and 3.7% (95% CI −2.0 to 9.2) per additional week of gestation for those without and with lower respiratory tract infection, respectively.
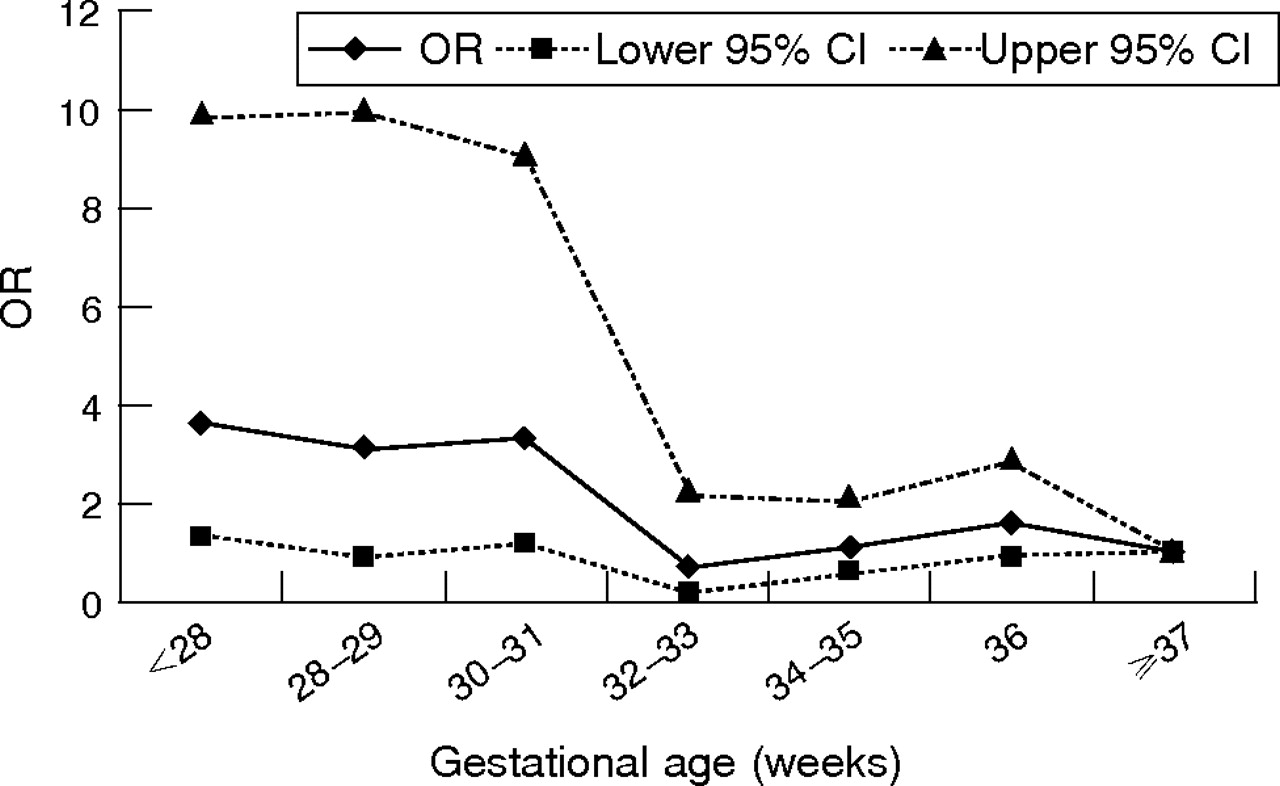
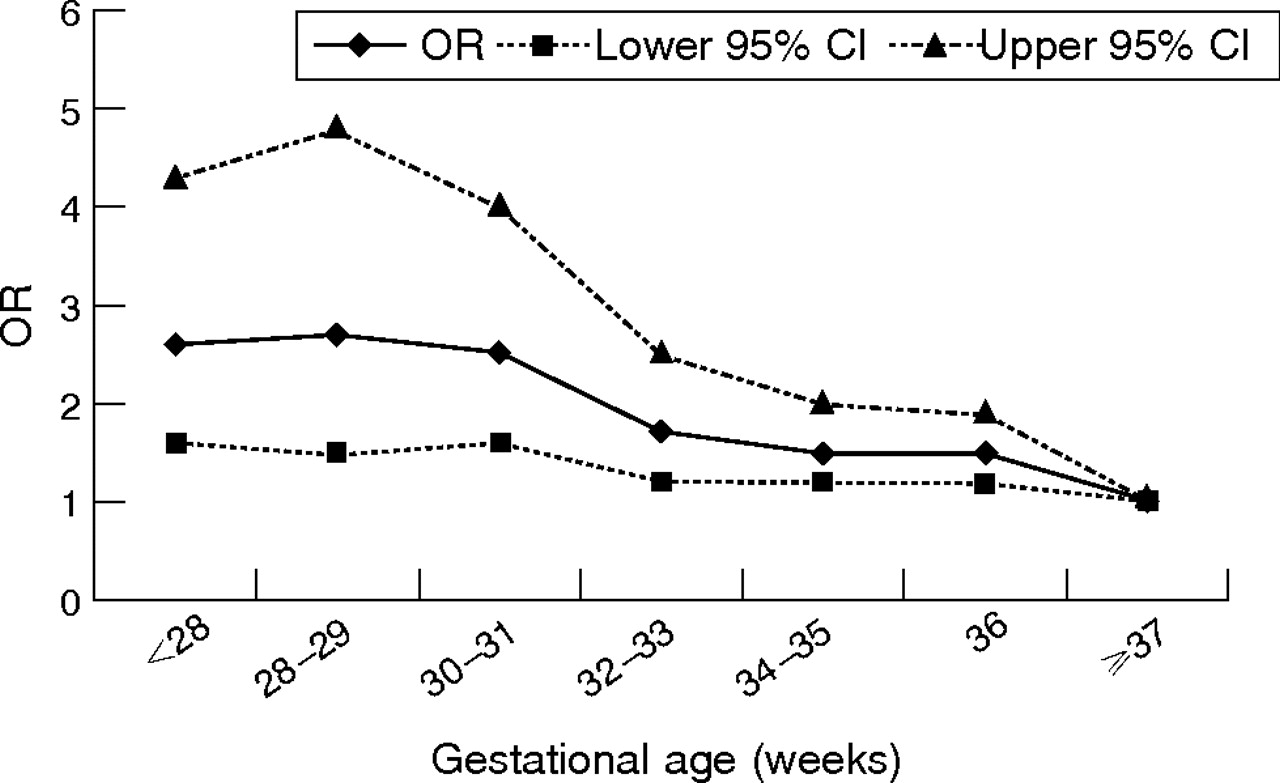
Model set number 4
When gestational age was grouped into seven categories, all categories of gestational age <37 weeks were significantly associated with the development of asthma. A dose–response effect was observed, with the adjusted OR decreasing as gestational age increased (fig 1⇓). For the model evaluating inpatient asthma among children with asthma, the adjusted OR was similarly high for the three categories of gestational age <32 weeks, whereas it was approximately 1 for all categories of gestational age of ⩾32 weeks (fig 2⇓).
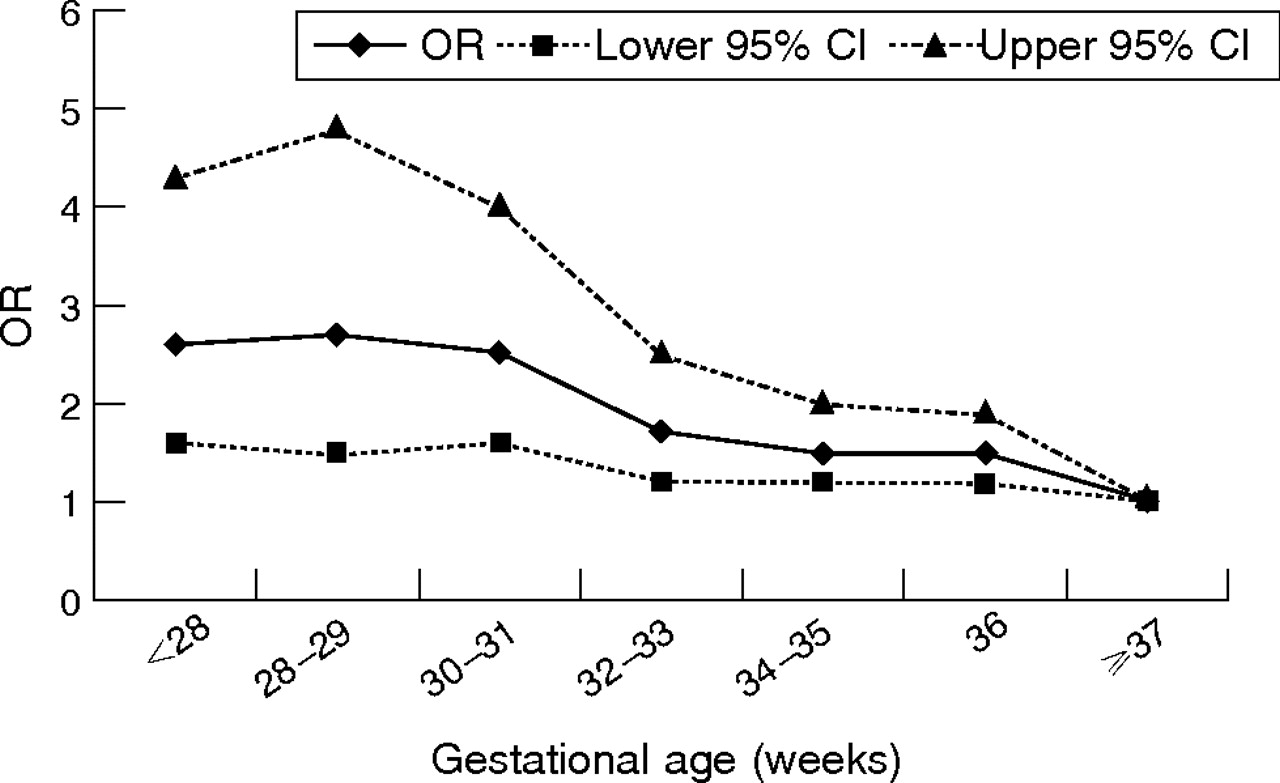
Association between asthma and gestational age among children <10 years old enrolled in Medicaid, adjusted for years of Medicaid enrolment, age at enrolment, sex, natives of Alaska, birth residence, caesarean and multiple birth, maternal prenatal tobacco use, maternal age, and maternal education; Alaska, January 1999–December 2002.
{kind=link}
{kind=link}
Association between inpatient asthma and gestational age among children with asthma <10 years old enrolled in Medicaid, adjusted for years of Medicaid enrolment, age at enrolment, sex, natives of Alaska, birth residence, caesarean and multiple birth, maternal prenatal tobacco use, maternal age, and maternal education; Alaska, January 1999–December 2002.
DISCUSSION
This large, population-based study identified an association between preterm birth, but not SGA status, and subsequent risk of clinical asthma among children <10 years of age. This effect was observed among children <5 years and 5–9 years of age. Among children with asthma, preterm birth also increased the risk of hospitalisation due to asthma. These data support previous studies that have identified an association between prematurity and changes in pulmonary function, including those that have found effects extending into adolescence1,5,7,23–,26 and adult life.27 Futher, our stratified analyses suggest that previously reported associations are probably not solely due to preterm birth increasing the risk of respiratory tract infection.
Recent studies have found a relationship between intrauterine growth retardation and bronchopulmonary dysplasia.28–,30 Pulmonary damage from bronchopulmonary dysplasia, in turn, has been associated with asthma,6,7,23–,25 providing a potential mechanism by which low-birth weight might increase the risk of asthma. All of these studies, however, evaluated the effect of asthma on lung function rather than clinical illness. Several studies evaluating clinical illness as an outcome have found an association between low-birth weight and future asthma risk31–,33 whereas others have not.5,34 These studies, however, did not evaluate the independent effect of prematurity and birth weight on asthma, or the association between SGA status and asthma. One study that evaluated gestational age and birth weight found that birth weight adjusted for gestational age was strongly associated with lung function, but that gestational age alone more accurately reflected respiratory illness.4 A second study found that after adjustment for confounding factors, birth weight was not associated with either adult lung function or asthma symptoms.35 Our results support existing evidence that low-birth weight independent of gestational age does not increase the risk of clinically significant asthma.
Most4–,8 but not all34,35 published studies have found that preterm birth leads to increased risk of clinical asthma or decreased lung function. Few studies, however, have attempted to quantify the effect of prematurity on asthma outcomes. Consistent with our results, a single study found that each additional week of gestation reduced the risk of severe wheezing by 10%.5 In our study, the largest effect occurred at <32 weeks of gestation. Nevertheless, some effect is observed between 32 and 36 weeks’ gestation. As the occurrence of births is much greater at 32–36 than at <32 weeks’ gestation, it is likely that the greatest effect on asthma will occur by extending these later gestation births.
Our study had several limitations. Because children were not necessarily continuously enrolled over the 4-year study period, we may have missed children with milder asthma who presented infrequently for care, and thus our results may not be generalisable to this population; we controlled for this to some extent by limiting analysis to children enrolled for at least 365 days. Children born prematurely may have more opportunities to have asthma diagnosed and reported because they present more frequently with other medical conditions; this ascertainment bias may have overestimated the association between preterm birth and asthma. We studied only the Medicaid population and thus results may not be generalisable to other groups. We did not evaluate lung function. Finally, we could not evaluate the possibility of a causal link between respiratory infection and asthma.
We believe that this is the largest population-based study yet conducted that has evaluated the association between birth outcomes and clinically relevant asthma. Among children born at <32 weeks, the 4-year asthma prevalence was ⩾10% regardless of whether children were <5 years or >5 years, although among those with asthma 15–43% required hospitalisation, depending on age. Consequently, preterm children should be evaluated for the development of asthma and treated aggressively when asthma is identified. Each additional week of gestation decreased the overall asthma risk by 7.6% and the risk of hospitalisation among children with asthma by 6.9%. Thus, measures that prolong gestation could possibly have a modest effect on asthma burden among children born preterm.
REFERENCES
Footnotes
Published Online First 13 October 2006
Funding: This work was supported in part by project H18 MC-00004-11 from the Maternal and Child Health Bureau (Title V, Social Security Act), Health Resources and Services Administration, Department of Health and Human Services. BDG has received funding support from Sanofi-Pasteur and TAP Pharmaceuticals.
Competing interests: None declared.
Ethical approval: This study involved linkage of existing legally authorised administrative databases housed at the Alaska Department of Health and Social Services. No novel data were obtained. Under these circumstances of routine public health evaluation, institutional review board approval and informed consent were neither sought nor obtained.
The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the US Centers for Disease Control and Prevention.