Article Text

Abstract
Background: London accounts for nearly half of the national burden of tuberculosis. The incidence of tuberculosis has more than doubled in London in the past 15 years.
Methods: Data from the enhanced tuberculosis surveillance 1999–2003, the national tuberculosis surveys of 1993 and 1998, and tuberculosis notifications were compared and analysed.
Results: In 2003, 3048 patients with tuberculosis were reported in London, 45% of the national total. This represents an incidence of 41.3/100 000, five times higher than the rest of England and Wales, and in parts of London the incidence of tuberculosis is nine times the national average. 75% of people with tuberculosis in London are born abroad; nearly half have lived in the UK for <5 years, but a third for >10 years. 86% are from an ethnic minority group, and the incidence is highest in black Africans at 283/100 000 compared with 141, 141 and 8/100 000 for Pakistanis, Indians and whites, respectively. In absolute terms, a third of patients with tuberculosis in London are from Africa and nearly a third from the Indian subcontinent. Specific groups affected also include the homeless, prisoners, and hard drug and alcohol users as well as the immunosuppressed.
Conclusions: London reflects the worldwide rise in tuberculosis, with increasing incidence in ethnic minorities. Work has been carried out to combat this rise, but more is needed. Tuberculosis control and prevention strategies should be mindful of the changing epidemiology of tuberculosis in London, and provide information, diagnosis and treatment tailored to the specific needs of the capital and its at-risk groups.
- ETS, enhanced tuberculosis surveillance
- LTBR, London Tuberculosis Register
- NYC, New York city
Statistics from Altmetric.com
Tuberculosis is increasing across the UK and is a particular public health concern in London. In England and Wales, the incidence of tuberculosis declined throughout most of the 20th century.1 However, since the mid-1980s this trend has reversed.2 Contributing to the rise are changing patterns of immigration,3–6 increased homelessness3,7,8,9,10,11 and HIV infection,3,9 as well as an ageing population. More than 40% of patients with tuberculosis in England and Wales live in London.2 Research published in the past few years showed that the incidence of tuberculosis in London is especially high in recently arrived immigrants,2,12 and varies significantly by borough.13 This paper provides a summary of the changing epidemiology of tuberculosis in London over the past decade and a half.
METHODS
London data from the enhanced tuberculosis surveillance (ETS) 1999–2003, the national tuberculosis surveys of 199314 and 1998,2 and tuberculosis notifications were compared and analysed. Since 2002, surveillance in London has been possible through the Health Protection Agency London Tuberculosis Register (LTBR), which is a web-based system used in every tuberculosis clinic across the city. Validation of these data is ongoing at both regional and national levels, and methods for the 1993 and 1998 national tuberculosis surveys have been described elsewhere.2,14 Estimates of population denominator data were obtained from the 1991 and 2001 census. Geographic information systems were used to plot cases by postcode and borough.
RESULTS
Cases, age and sex
In 2003, London accounted for 45% of the national tuberculosis burden; 3048 cases of tuberculosis were reported via ETS (the LTBR). This represents an incidence of 41.3/100 000, five times higher than the rest of England and Wales at 8.2/100 000. Over the past 15 years, tuberculosis notifications have doubled in London from just over 20/100 000 in 1987, but have remained fairly constant in the rest of England and Wales (fig 1).

Tuberculosis notifications in London and outside London, 1982–2003. ETS, enhanced tuberculosis surveillance data; NOIDs, notification of infectious diseases.
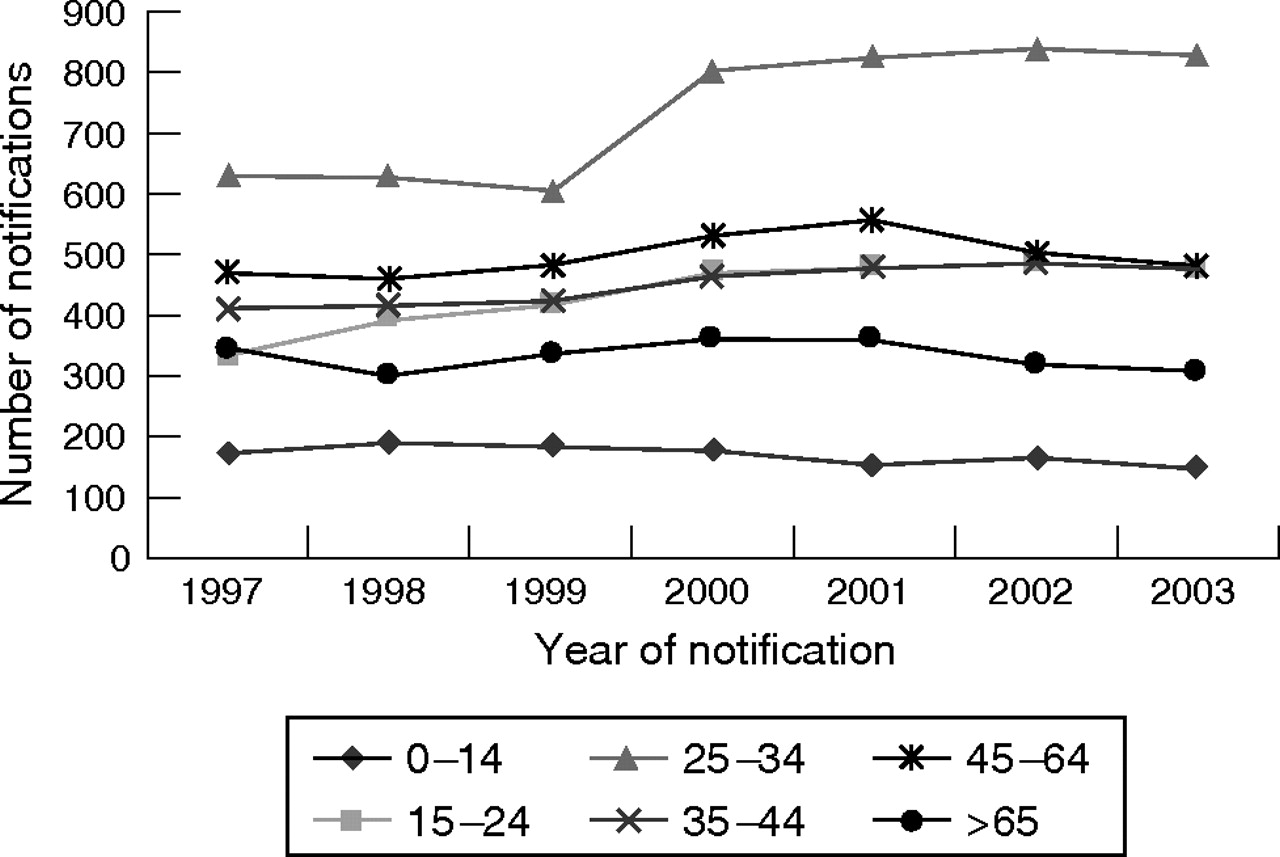
The age distribution of new cases of tuberculosis in London has changed over the past 7 years (fig 2). Tuberculosis notifications rose most rapidly in the 25–34-year-old age group and remain highest in this group. In 2003, the incidence of tuberculosis in 25–34-year-old men was 60/100 000 and in women 52/100 000 (fig 3). Since 2001, rates have fallen slightly in those >45 years.

Tuberculosis notifications in London by age group, 1997–2003.

Tuberculosis notification rates in London by age and sex in 2003.
Geographical distribution
Tuberculosis is concentrated in particular areas of London. In 2003, of 33 London boroughs, 14 (one third) had an incidence of tuberculosis >40/100 000; these “hot spots” are not exclusively inner-city districts but also include suburban areas with well-established ethnic communities. Hot spots have not changed much over the time period of our review (fig 4).

Geographical distribution of patients with tuberculosis in London, 2003.
In 2003, Newham, Hackney and Brent had the highest formal notification rates (96.4, 91.8 and 64.2/100 000 population, respectively). However, there has been a decrease from a high in 2001 of 116/100 000 in Newham (northeast London) and 103 in Brent (northwest London). Since 1987, tuberculosis rates have risen fivefold in Hillingdon (west) and Sutton (southwest), fourfold in Greenwich (southeast) and threefold in Enfield (north), Hackney, Barking and Dagenham (northeast).
Ethnicity and country of birth
In 2003, 86% of tuberculosis cases in London were from a non-white ethnic group, 35% were black African and 31% were from the Indian subcontinent. Between 1999 and 2003, the proportion of tuberculosis notifications in the white population fell, but rose in nearly all other ethnic groups. In the past 5 years, tuberculosis in black African communities has risen markedly. In 2003, the tuberculosis incidence in black Africans was 283/100 000 compared with 141, 141 and 8/100 000 for Pakistanis, Indians and whites, respectively (fig 5). The incidence in black Africans aged 25–44 years was 407/100 000 compared with 41/100 000 for all ages and ethnic groups across London, and 8.2/100 000 across the rest of England and Wales. In black Africans, tuberculosis is found more commonly in new entrants and those who have lived in the UK for <5 years.
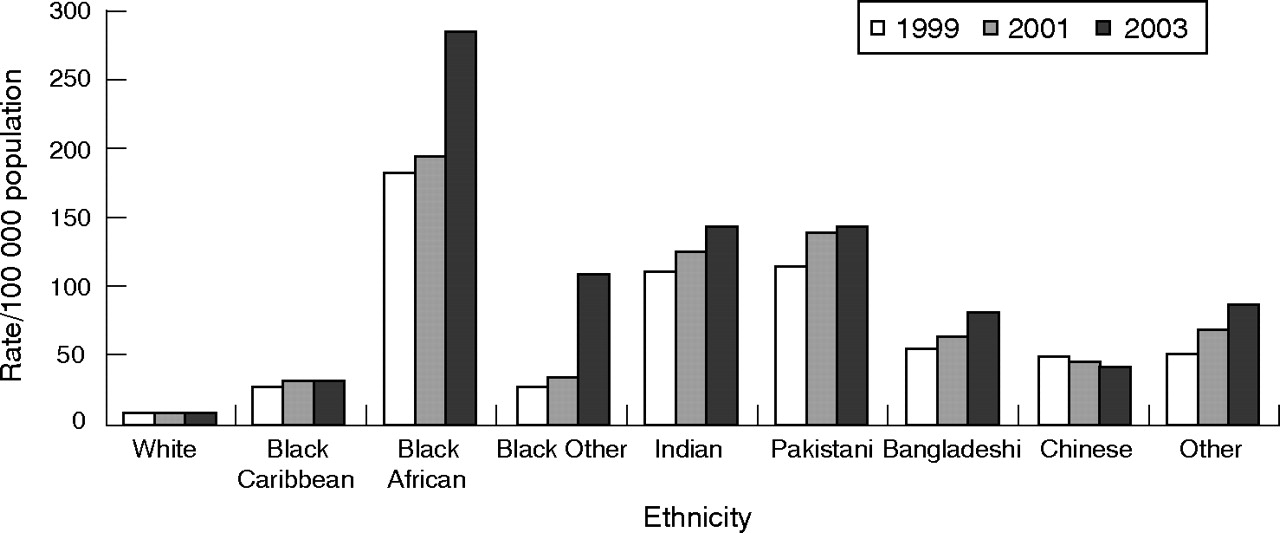
London tuberculosis notification rates by ethnic group: 1999, 2001 and 2003.
ETS data from the LTBR show that most of the patients with tuberculosis in the white population are aged >45 years, whereas in black African communities, most patients are aged 25–44 years and in the community from the Indian subcontinent, there is a mix of middle and old-aged people (fig 6).

Number of patients with tuberculosis in London by age and ethnic group, 2003.
The vast majority of patients with tuberculosis in London are born abroad (fig 7). In 2003, 75% were born abroad (where place of birth was known). This percentage has risen steadily, from 55% since 1993. In the past 10 years, India has remained the most commonly reported country of birth for patients born abroad. The other top 10 countries have remained similar, apart from a substantial rise in Somalian patients between 1993 and 1998, and a rise in Afghan patients since 1999.
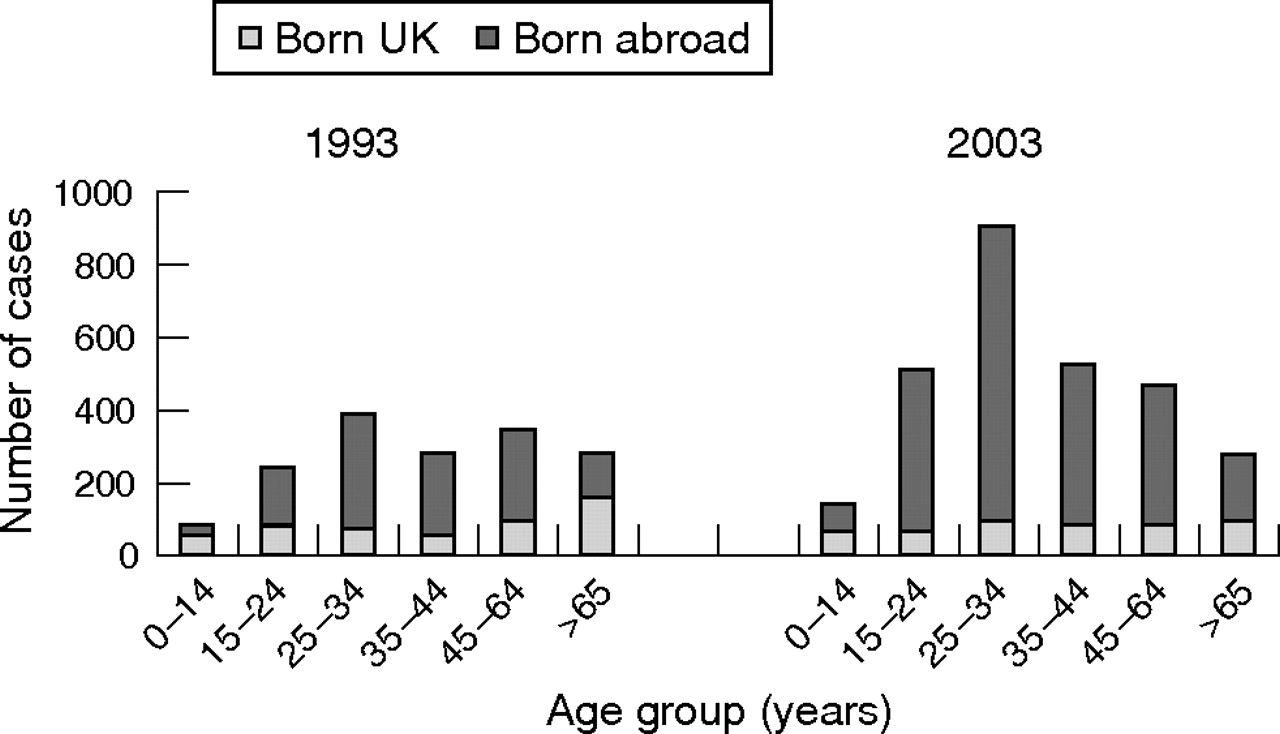
Number of patients with tuberculosis born in the UK and abroad in 1993 and 2003 by age group
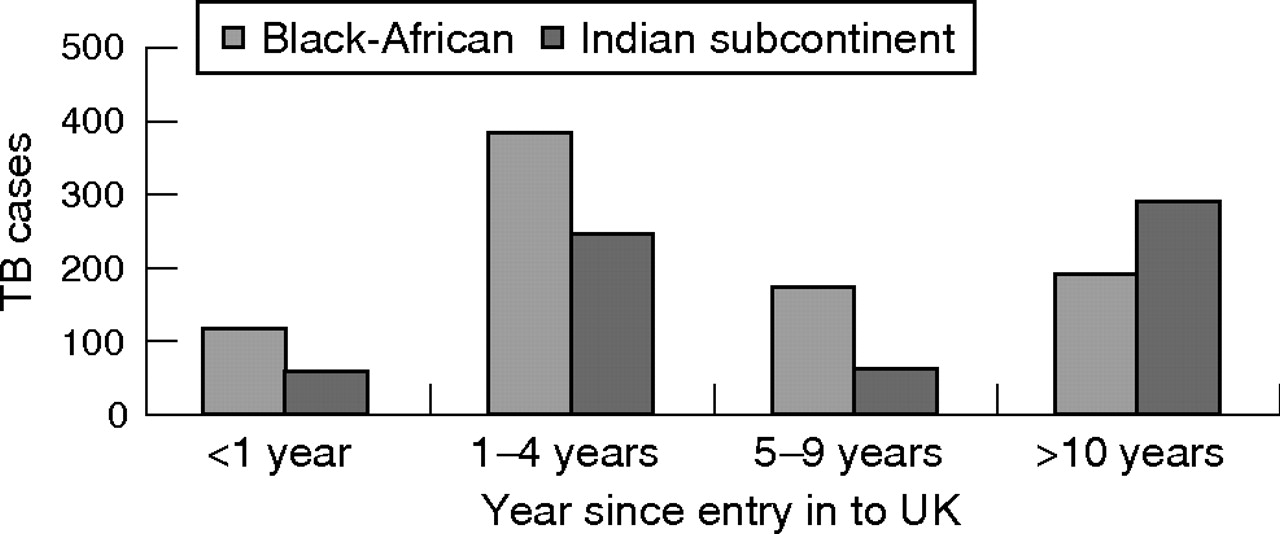
In 2003, 46% of patients with tuberculosis born abroad had entered the UK in the past 5 years and 27% had lived in the UK for >10 years. On further analysis of those born abroad in the two largest ethnic minority subgroups, black Africans were more likely to be new entrants or residents in the UK for <5 years (52%), whereas patients with tuberculosis from the Indian subcontinent were more likely to have lived in the UK for >10 years (fig 8).

Years since entry into the UK for patients with tuberculosis (TB) from Africa and the Indian subcontinent
Tuberculosis and HIV
Coinfection with tuberculosis and HIV is an increasing problem in London (table 1). In 1993, 3.3% of patients with tuberculosis were coinfected; by 1998, this had risen to 5.4%15 and by 2001 the rate was 6.5% (V Delpech, HPA Colindale, personal communication, 2005). This is thought to be an underestimate. Reports from London hospitals suggest that rates of coinfection are as high as 17–25%.16,17 It has been estimated that about three quarters of the national population coinfected with HIV and tuberculosis live in London, most of whom are black African.15 Between 1993 and 1998, coinfection increased by a factor of 2.5 in black Africans and by a factor of 0.6 in whites.15 It was estimated that between 1993 and 1998, 11% of the rise in London’s tuberculosis cases could be attributed to HIV.15 It is important to offer and recommend HIV testing for all patients with tuberculosis in London so that both infections can be properly treated.
Tuberculosis/HIV coinfection
Drug-resistant tuberculosis
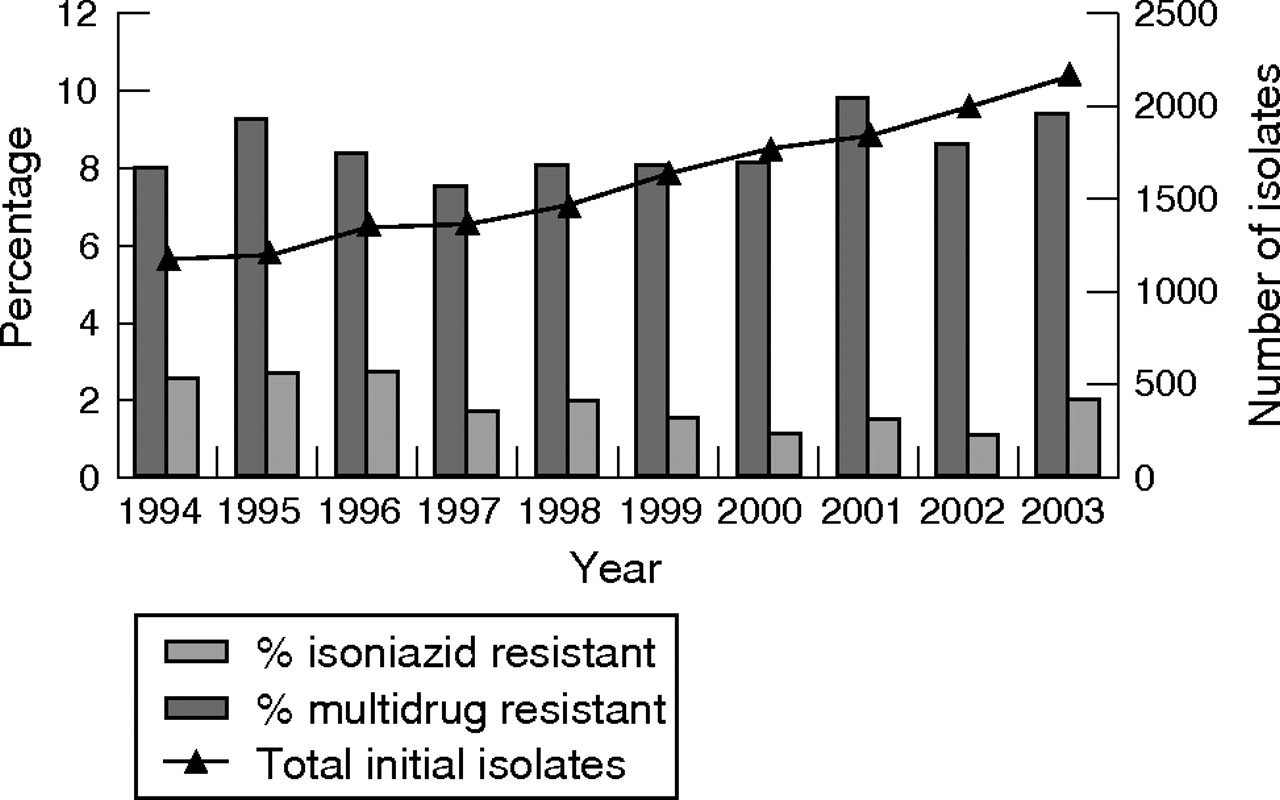
Both isoniazid-resistant and multidrug-resistant tuberculosis are bigger problems in London than elsewhere in England and Wales. In 2003, 9.4% of isolates were isoniazid resistant in London (fig 9) compared with 7.5% nationally. Rates of isoniazid-resistant tuberculosis were relatively stable until 2000, but have risen slightly since then mainly because of a large outbreak of isoniazid-monoresistant tuberculosis.18 Over the past 5 years, rates of multidrug-resistant tuberculosis have been about 1–1.5% in London, with just a slight rise to 2% in 2003 (the most recent year for which data are available).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tuberculosis drug resistance in London, 1994–2003. Source: Health protection agency Mycobacterial Resistance Network (MycobNet).
Outcome of treatment
In 2003, treatment outcome data were available through the LTBR. Patients notified during 2002 were followed-up 1 year after starting treatment. In all, 82% had completed a full course of treatment, 10% had not completed treatment and 8% were either lost to follow-up or had an unknown outcome. Of the 10% not completing treatment, two thirds had died and for just under half of these tuberculosis had caused or contributed to death.
Molecular epidemiology of tuberculosis
Research published in 2002 using molecular typing showed that tuberculosis in London was mainly caused by reactivation or importation of infection by recent immigrants.19 New infections were common in people with recognised risk factors such as alcoholism or HIV. The main findings were the importance of preventive interventions and early diagnosis in immigrants, along with thorough contact tracing and monitoring of treatment outcome in groups at higher risk of new infection. This molecular study was conducted in the late 1990s before a large outbreak of drug-resistant tuberculosis in north London; its findings may now have changed. The outbreak has emphasised the vulnerability of groups such as drug users and prisoners in London to recent new infection.18
Risk groups
A cross-sectional survey performed in London in July 2003 found the overall prevalence of tuberculosis to be 27/100 000, but reached 788 in people sleeping rough or using direct-access homeless hostels, 550 in prisoners, 172 in drug users and 878 in patients diagnosed HIV positive. This survey showed a prevalence of disease of 149/100 000 in recent migrants and of 92/100 000 among refugees and asylum seekers.20
DISCUSSION
Tuberculosis is an increasing problem in London. Over the past 15 years, its incidence has doubled to 41.3/100 000 and continues to rise. In 2003, 3048 cases were reported via the ETS, 45% of the national total. A discrepancy exists between statutory notifications and LTBR data, as fig 1 shows. In 2003, 2745 patients with tuberculosis were formally notified in London compared with 3048 notified via the LTBR. The ETS is likely to better reflect the true incidence of tuberculosis as it undergoes more rigorous validation than statutory notifications. Caution has been advised in the interpretation of statutory notification data.21
The incidence of tuberculosis varies substantially between different ethnic groups. In 2003, 86% of patients with tuberculosis in London were from an ethnic minority, a reflection of the effect of the global epidemic of tuberculosis.22 Three quarters of patients were born abroad, in countries where the incidence of tuberculosis is much higher. The importance of this for prevention and control is that primary care or community services need to be increasingly aware of at-risk groups, and target case finding and treatment appropriately. We have shown that incidence varies across London boroughs from <10/100 000 to 96/100 000 (nearly 10 times the national average) and in recent years London’s tuberculosis hot spots have remained largely unchanged, although a few areas have seen increases of up to fivefold. The hot spots are not exclusively inner-city districts but also include suburban areas with well-established ethnic communities. Immigration patterns to the UK have changed over time,6 with more people arriving from the Indian subcontinent >10 years ago and young Africans more recently. Africans made up 41% of all asylum applications in 2003 and Asians 27%.23 Our results reflect the changing patterns of immigration (with higher rates of tuberculosis in older Asians with longer residency and younger more recently arrived Africans) and highlight the fact that it is not just recently arrived immigrants who are developing tuberculosis. Tuberculosis control and prevention strategies need to be mindful of this, and provide information, diagnosis and treatment to newly arrived immigrants, as well as for more established ethnic communities.
According to 2001 census data, about seven million people live in London. From 1991 to 2001, the proportion of people from an ethnic minority increased from 20% to 29%. The increase was evident in all ethnic minority groups, with the greatest increase seen for black Africans, a doubling from 2.4% to 5.4%. As a reflection of this, tuberculosis in black African communities has risen markedly in the past 5 years. The current notification rate for all ages is 283/100 000 and for the 25–44-year age group 407/100 000. In black Africans, tuberculosis is found more commonly in new entrants and in those who have lived in the UK for <5 years. This suggests that a greater understanding of this group is needed, and more resources to assess and diagnose newly arrived black Africans in addition to further prevention work.
The rise in tuberculosis notification in London is likely to have many causes. Apart from the changing patterns of immigration, other factors that affect tuberculosis epidemiology include: increased detection through increased staff-to-patient ratios and heightened awareness of tuberculosis in both the public and healthcare staff; increased opportunities for international travel with exposure to tuberculosis in countries with a high incidence; HIV infection in London at an all time high; and the emergence of drug-resistant tuberculosis—rising slowly, and mainly because of a large outbreak of isoniazid-monoresistant tuberculosis.18 In addition, incidence and prevalence rates of tuberculosis are documented to be high in the homeless8,11 and in prison populations,18,20 groups that are often marginalised and difficult to reach and engage.24
Can we learn from the New York experience?
In the early 1990s, tuberculosis had reached epidemic proportions in New York City (NYC). This epidemic differed in several ways from that in London; London has a much higher proportion of immigrants infected with tuberculosis (London, 80% v NYC, 25%), a much lower proportion of patients with tuberculosis coinfected with HIV (London, 6.5% v NYC, 38%) and lower levels of multidrug-resistant tuberculosis (London, 1.2% v NYC, 19%).25 However, there are similarities between the two epidemics, such as similar numbers of cases at the epidemic peak and a higher prevalence in lower socioeconomic classes, ethnic minorities and the homeless. The epidemic in NYC was brought under control by broadening treatment regimens, using directly observed treatment and structured guidelines for control and prevention.26 The reduction in patients in NYC has largely been confined to those born in the US.27 As tuberculosis in London is mostly found in non-UK born ethnic minorities, all the lessons learnt in New York may not be appropriate. However, New York had a sub-epidemic of drug resistant tuberculosis and the lessons learnt from its containment might be helpful for London. Similarly, for patients with tuberculosis coinfected with HIV, London might benefit from reviewing New York’s policies, as the fastest growing group of patients with tuberculosis are 25–34-year-old black Africans who also have the highest rates of coinfection.
What does all this mean for London?
Tuberculosis in London is an increasing public health concern, but there have been some service improvements reported in each of London’s five sectors together with the creation of multidisciplinary tuberculosis networks. Service improvements include greater monitoring of treatment completion, an increase in the number of tuberculosis nurses and the use, since 2002, of the Health Protection Agency LTBR in all tuberculosis clinics. The LTBR is a web-based electronic case management and surveillance system that allows patients to be tracked as they move between clinics, and thereby improves local service monitoring of patient outcomes. A mobile screening project using targeted digital radiography is being piloted in London to evaluate how this approach could strengthen the screening of defined populations, including for example prisoners or hostel dwellers.
Further improvements are possible, and these include: improved case finding in high-risk groups by screening those known to be at particular risk—for example, residents of hostels for refugees, asylum seekers or the homeless11,28; early detection in new entrants and better access to primary care services12,28–30; early recognition of symptoms by doctors and patients; a continuing emphasis on treatment continuity and completion, with the use of directly observed therapy where appropriate to help reduce drug resistance26,31; better diagnosis of tuberculosis/HIV coinfection to enable treatment of both conditions appropriately32,33; and an increased awareness of the social dimensions of tuberculosis control so that health services work more closely with other agencies.26,29,34
The Chief Medical Officer’s tuberculosis action plan35 published in October 2004 provides a framework to assist tuberculosis prevention and control, and builds on the existing structures and multidisciplinary working across London’s tuberculosis networks. The National Institute for Health and Clinical Excellence has recently issued clinical diagnosis and management guidelines for tuberculosis.28 These guidelines make recommendations on good practice and attempt to focus National Health Service resources where they will most effectively combat the spread of tuberculosis.
CONCLUSION
The global rise in tuberculosis continues, and tuberculosis in London reflects this with increasing rates in ethnic minorities. Drug resistance and coinfection with HIV are growing problems. Control of tuberculosis in London needs to improve, and ultimately treatment and control services should be tailored to the specific needs of the capital and its at-risk groups. This is the time to apply the full weight of political, organisational and individual will to tackle London’s tuberculosis problem.
Acknowledgments
We thank the London community tuberculosis teams, NHS staff at tuberculosis clinics and HPA colleagues across London and at the Mycobacterium Reference Unit.
REFERENCES
Supplementary materials
Attached is the correct version of Figure 9.
Files in this Data Supplement:
Footnotes
-
Published Online First 13 November 2006
-
Competing interests: None.
Linked Articles
- Correction