Article Text

Statistics from Altmetric.com
The need to highlight the risks of high flow oxygen in clinical teaching
In a recent commentary we argued that the traditional representation of the haemoglobin oxygen dissociation curve developed by physiologists may be disconcerting for clinicians because of the prominence of the steep slope of oxygen desaturation with falling oxygen tension.1 We proposed that a different alignment may be preferable for clinicians in demonstrating its beneficial characteristics, enhancing both the “pick up” of oxygen despite cardiorespiratory disease and the “drop off” of oxygen to the tissues despite falling oxygen saturation (fig 1). It was hoped that, through a different perspective of the haemoglobin oxygen dissociation curve, it might be possible to overcome the ingrained practice of doctors, nurses and paramedics to prescribe high flow oxygen to breathless patients who do not necessarily have arterial hypoxaemia.2–4 However, such a change of long established practice would also require a recognition of the risks of inappropriate high flow oxygen therapy.5,6

Left: Traditional representation of the oxyhaemoglobin dissociation curve with the “slippery slope” (SS). Right: Oxyhaemoglobin dissociation curve realigned to demonstrate its two key characteristics: (a) haemoglobin maintains high levels of saturation despite marked reductions in oxygen tension, and (b) oxygen tension remains relatively stable as oxyhaemoglobin saturation declines. These characteristics result in (a) the pick up of oxygen by haemoglobin being maintained despite reduced oxygen tension, and (b) delivery of oxygen to the tissues being maintained despite progressively falling oxyhaemoglobin saturation. Figure reproduced with permission from Beasley et al.1
The potential adverse pulmonary effects of high flow oxygen therapy were recognised soon after its widespread use in clinical practice. High flow oxygen was shown to result in worsening ventilation-perfusion mismatch due to absorption atelectasis and inhibition of reflex pulmonary vasoconstriction.7,8 These effects may contribute to the reduction in lung volumes and decreased transfer factor observed with high flow oxygen.9
High flow oxygen resulting in hyperoxia also has the potential to cause significant adverse cardiovascular effects with increased systemic vascular resistance and blood pressure, decreased cardiac output and reduced coronary, cerebral and renal blood flow.10–14 These cardiovascular effects can potentially contribute to the worse outcomes observed with high flow oxygen therapy in myocardial infarction,15 stroke,16 neonatal resuscitation17 and fulminant sepsis,18 although the enhanced production of reactive oxygen species causing reperfusion injury may also play a role.
Paradoxically, high flow oxygen in excess of that required to relieve arterial hypoxaemia may cause a reversible decrease in oxygen consumption.19 This effect is likely to be due to maldistribution of blood flow, with functional shunting to protect the vital organs from non-physiological effects of high oxygen tension. Regardless, the impaired oxygen delivery at the tissue level results in depressed cellular respiration and potential organ dysfunction.
These adverse effects are not widely known and high flow oxygen is widely prescribed to breathless patients, regardless of the presence of arterial hypoxaemia. Even in patients with exacerbations of chronic obstructive pulmonary disease in respiratory failure, the risks of high flow oxygen therapy are often not recognised.20
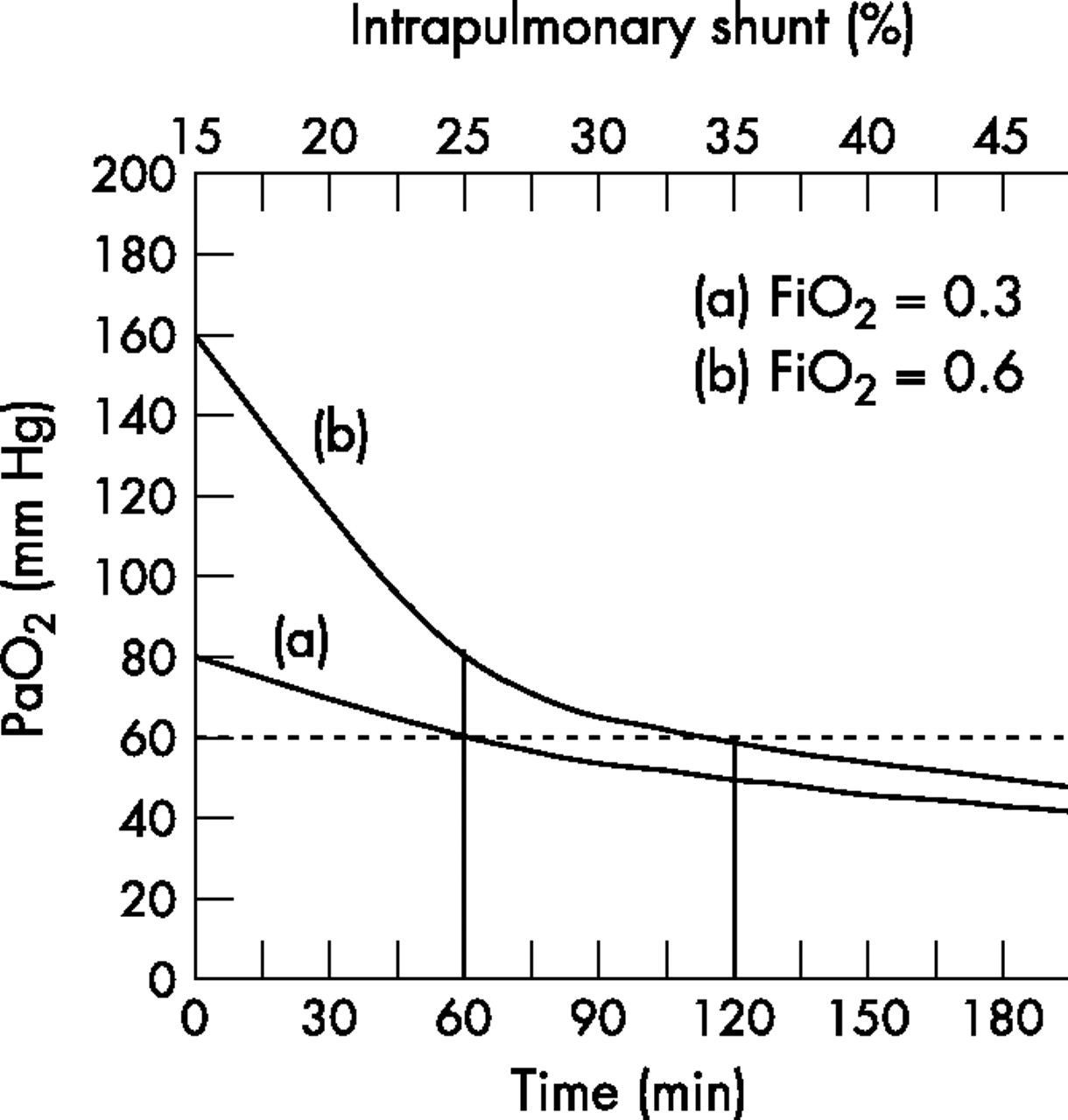
Perhaps the least recognised risk with high flow oxygen is that its use may lead to a delay in the ability to recognise and treat a progressive deterioration in pulmonary function.6,21 This risk has been well quantified by Downs and colleagues through modelling of the effects of different oxygen regimes in the situation of a progressively increasing intrapulmonary shunt (fig 2).21 In this clinical scenario, the use of high flow oxygen can delay the recognition of a deterioration in respiratory function as there is likely to be no major change in vital signs22 and minimal decrease in oxygen saturation assessed by pulse oximetry23 until a life threatening situation has developed. This may provide a false reassurance that the patient is stable. At this stage there is limited opportunity to further increase the oxygen therapy while medical review and an intervention such as transfer to the intensive care unit (ICU) is undertaken. In contrast, if low flow oxygen therapy is initially used to achieve oxygen saturations around 95%, a subsequent clinical deterioration is likely to be recognised sooner through pulse oximetry, and there is the option of increasing the oxygen therapy while medical review and the required intervention is undertaken (see case example and fig 2).
{kind=link}
{kind=link}
Arterial oxygen tension (Pao2) plotted as a function of intrapulmonary shunt increasing at a rate of 1% per 6 min with fractional inspired oxygen (Fio2) of (a) 0.3 and (b) 0.6. In example (a) with Fio2 0.3, the time required for the Pao2 to decrease from 80 mm Hg (95% saturation) to <60 mm Hg (<90% saturation) is around 60 min. At this stage, with the same rate of increasing intrapulmonary shunt, an increase in Fio2 from 0.3 to 0.6 will maintain the Pao2 above 60 mm Hg for about a further 60 min. In example (b), if the patient receives an Fio2 of 0.6, it would take around 120 min for the Pao2 to decrease to <60 mm Hg (<90% saturation). At this stage, with the same rate of increasing intrapulmonary shunt, there will be a further deterioration in Pao2 despite maintenance of the Fio2 at 0.6. Reproduced with modification from Downs and Smith.21
Thus, inappropriately high flow oxygen has the potential to cause both a delay in recognising clinical deterioration and a reduction in the time available to institute additional treatment. This is contrary to the common assumption that administration of high flow oxygen in a breathless patient will have a protective effect in the event that pulmonary function deteriorates.
In accepting that there are significant risks with high flow oxygen, what is the alternative to the current practice of immediate placement of high flow oxygen in the breathless patient regardless of the presence of arterial hypoxaemia? We recommend that, as part of the initial assessment of an acutely breathless patient, oxygen saturation is measured by oximetry. If the oxygen saturation is >92%, oxygen therapy need not be routinely administered. If the oxygen saturation is 85–92%, oxygen therapy could be initially instituted at 2–3 litres via nasal cannula which would be expected to increase the saturation above 92%. An oxygen saturation of <85% is likely to require higher flows through a simple mask, titrated to achieve a saturation above 92%. Importantly, in the situation of arterial hypoxaemia, the priorities are to identify the cause and severity of the underlying disorder and to administer the required specific treatment in addition to titrated oxygen therapy.
Case example*
A 30-year-old patient with community acquired pneumonia presents with a CURB-65 severity score of 1, with no confusion, urea 6.5 mmol/l, respiratory rate 35/min and blood pressure 115/65. He is admitted because of the associated clinical features of an oxygen saturation of 88% (Pao2 58 mm Hg) and bilateral changes on his chest radiograph. He is admitted to the ward, treated with intravenous antibiotics, and monitored with continuous pulse oximetry and clinical recordings. His pneumonia worsens, with right to left intrapulmonary shunting of blood increasing by 1% every 6 min.
(a) With an Fio2 of 0.3 (2–3 litres via nasal cannula), the saturation initially increases to 95% but then, with the progressive deterioration, decreases to a saturation of <90% in about 60 min. At this stage the oxygen therapy can be increased to an Fio2 of 0.6, with a saturation increasing to and remaining >90% despite further deterioration during the 30–60 min required to arrange medical review and transfer to the ICU.
(b) An Fio2 of 0.6 (8–10 litres via Hudson mask) would initially increase the saturation to around 100% but, with the same rate of deterioration, the decrease to a saturation of <90% would take about 2 h. During this period it is unlikely that the deterioration would be recognised clinically through monitoring of clinical signs22 or pulse oximetry. Once the saturation has fallen to <90%, there is limited opportunity to further increase the inspired oxygen and the saturations would decrease further during medical review and ICU transfer.
*This case example was derived from Downs and Smith.21 The rate of increase in right to left shunting was 2% per minute in the original reference compared with 2% per 12 min in this case example to ensure a more clinically relevant deterioration.
We suggest that, in clinical teaching, the risks of high flow oxygen are presented with discussion of both the adverse physiological effects and potential for delay in the recognition of a deteriorating clinical condition. This would reinforce the awareness that oxygen is a drug that should be prescribed for defined indications in which the benefits outweigh the risks, and that prescriptions should specify the dose, method and duration of delivery and the patient’s response to oxygen therapy should be monitored.24
The need to highlight the risks of high flow oxygen in clinical teaching
REFERENCES
Footnotes
-
Competing interests: None.