Article Text

Statistics from Altmetric.com
A 49-year-old woman had been treated with carbamazepine for 2 years because of epilepsy. She was referred to us for progressive exertional dyspnea and prolonged productive cough. Chest computed tomography (CT) scan showed bilateral infiltrates including ground glass opacities and consolidations predominantly in the lower lung fields. Her laboratory findings showed severe hypogammaglobulinemia, that is, immunoglobulin (Ig) G 418 mg/dl (normal, 748–1694 mg/dl), Ig A 20 mg/dl (91–391 mg/dl) and Ig M 51 mg/dl (33–254 mg/dl). Carbamazepine and other suspected antibiotics were all negative for drug-induced lymphocyte stimulation tests. Histological examination by trans-bronchial lung biopsy showed intraluminal fibrosis of distal airspaces with foamy alveolar macrophages, suggesting bronchiolitis obliterans organising pneumonia (BOOP). After the cessation of carbamazepine, all abnormalities in gammaglobulins and roentgenogram findings gradually improved without any medication. This good clinical course also considerably supports the diagnosis of BOOP.
BOOP may result from diverse causes such as drugs, acute respiratory infections and radiation treatment, or appear idiopathically.1,2 Here, we show a case of secondary BOOP, which was associated with repeated respiratory infections caused by carbamazepine-induced hypogammaglobulinemia. Although the exact mechanisms of carbamazepine-induced hypogammaglobulinemia are unknown, they can be classified into three groups, that is, an absence of B cells,3 an extensive impairment of the synthesis of Igs in B cells3 and a disorder of the class-switch of Igs in B cells.4 Our case described above would belong to the second group. Generally, drug-induced BOOP often develops within several weeks or less. However, our report indicates that even in the case of several years after use, anticonvulsants such as carbamazepine may have some adverse effects on the immune system and cause frequent airway infections, resulting in the development of secondary BOOP.
Learning points
-
A drug-induced hypogammaglobulinemia after long term use of carbamazepine is very rare.
-
A hypogammaglobulinemia should be considered as one of the causes of secondary bronchiolitis obliterans organising pneumonia with repeated airway infections.

(A) Chest CT scans on admission. Bilateral infiltrates including ground glass opacities and consolidations are seen predominantly in lower lung fields. (B) Chest CT scans seven months after the cessation of carbamazepine showing marked improvement. The serum levels of Ig G, Ig A and Ig M are also increased to 1328, 69 and 355 mg/dl, respectively.
{kind=link}
{kind=link}
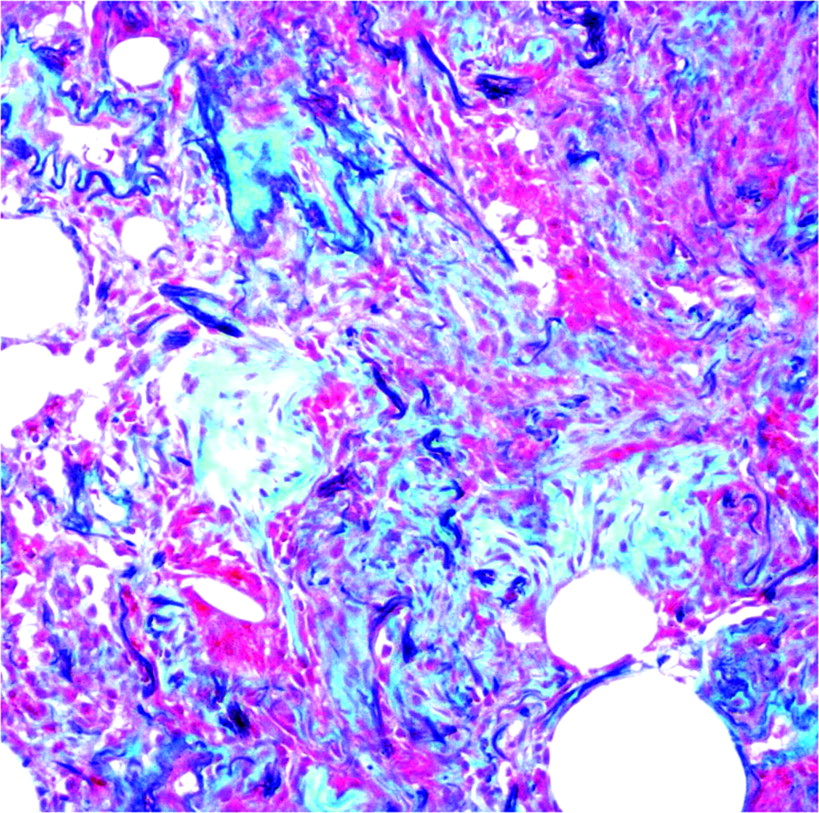
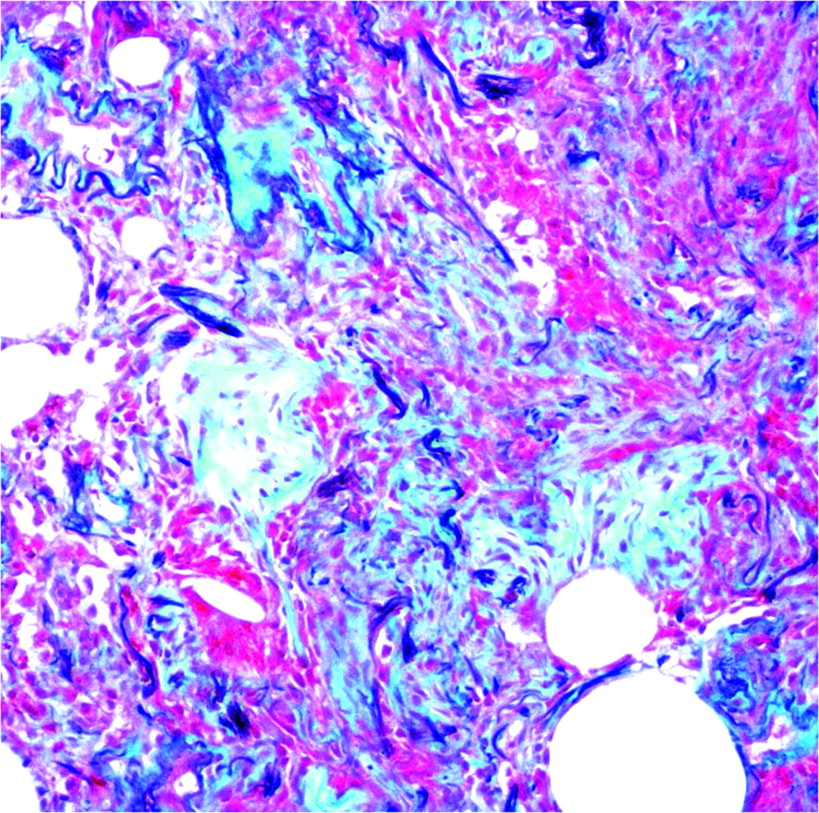
Elastica-Masson staining of specimens from TBLB. Immature fibroblastic foci and foamy alveolar macrophages are obstructing the alveolar ducts and adjacent alveoli. These features are consistent with BOOP.
Acknowledgments
The authors acknowledge Mr Brent K. Bell for reading the manuscript.
Footnotes
-
Competing interests: None declared.