Article Text

Statistics from Altmetric.com
Pulmonary arterial hypertension (PAH) is a life threatening condition characterised by progressive obliteration of the small pulmonary arteries leading to increased pulmonary arterial resistance and right heart failure. Treatment for PAH has developed in the last few years since the description of new pathways related to the disease.1 Recently, short term (6 months) use of imatinib, a platelet derived growth factor (PDGF) receptor antagonist, in combination with maximal PAH treatment (prostacyclin derivative, endothelin receptor antagonist, and type 5 phosphodiesterase inhibitor) has been shown to improve the haemodynamics and functional capacity in a single case of severe PAH.2 We here report the first two cases of the long term (3 years or more) use of imatinib, as monotherapy or in combination with bosentan, a dual endothelin receptor antagonist.
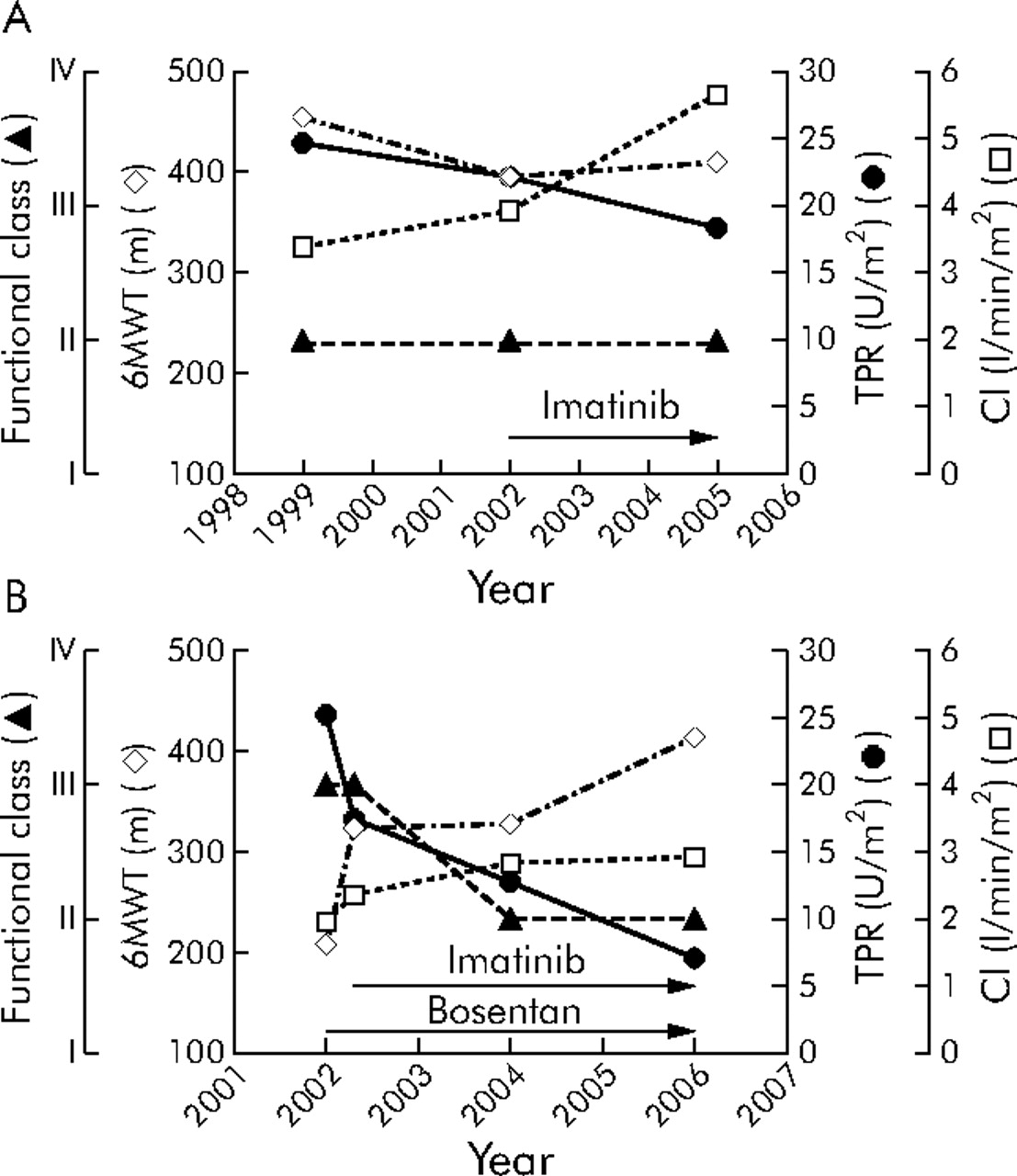
Case 1 was a 34 year old man with PAH associated with type I glycogen storage disease. Until 1999 the patient had remained stable with functional class II PAH (New York Heart Association classification) without any specific treatment. In 2002 he presented with an increased white blood cell count at his routine evaluation resulting in the diagnosis of chronic myeloid leukemia, a known late complication of type I glycogen storage disease. The patient remained in functional class II and the haemodynamic pattern showed a trend to worsening without a significant change at the 6 minute walk test (fig 1A⇓). Imatinib was started as first line treatment for leukemia without any associated PAH treatment. During 3 years of imatinib use his leukemia was adequately controlled, functional capacity was sustained, and the haemodynamic profile was improved.

{kind=link}
Long term haemodynamic and functional effects of treatment in (A) case 1 and (B) case 2. 6MWT, six minute walk test; TPRi, indexed total pulmonary resistance; CI, cardiac index; functional class, NYHA classification.
Case 2 was a 65 year old woman with a known diagnosis of chronic myeloid leukemia since 1994 which was satisfactorily controlled with hydroxycarbamide, cytarabine, and interferon. In 1996 she reported dyspnoea on exercise with insidious progression during the next 4 years. In 2000 an echocardiogram showed a right ventricular systolic pressure of 65 mm Hg. In 2002 she presented with functional class III PAH and was referred. The investigation showed no other condition associated with PAH but significant haemodynamic impairment (fig 1B⇑). Treatment with bosentan was initiated with a good haemodynamic and functional response after 3 months. At that time interferon was withdrawn and imatinib was started as treatment for leukemia. Since then, after more than 3 years of treatment with imatinib and bosentan, there has been functional and haemodynamic improvement (fig 1B⇑).
In these two cases of long term use of imatinib (alone or in combination with bosentan), functional and clinical stabilisation or improvement in PAH were observed. Of note is the progressive increase in cardiac index during the 3 years of treatment with imatinib. Such a progressive increase in cardiac index is certainly an indicator of a good prognosis, as previously discussed in PAH.3 PDGF is a potent mitogen that has been related to the chemotaxis and proliferation of pulmonary vascular smooth muscle cells. Its inhibition has been shown to prevent and reverse pulmonary hypertension in experimental models, raising the potential of its use in clinical practice.4 Imatinib is approved for the treatment of chronic myeloid leukemia, which was the reason for using it in the two reported cases leading to haematological remission. In parallel, the haemodynamic response to imatinib alone or in combination with bosentan was significant. Although many side effects have already been described with the long term use of imatinib,5 only mild anaemia was observed in our first case. We conclude that PDGF inhibition should be tested in future PAH clinical trials in order to establish its safety and efficacy.
Footnotes
Funding: Chancellerie des Universités de Paris (Legs Poix), Université Paris-Sud 11 and European Respiratory Society, Fellowship number 192.