Article Text

Abstract
Asthma exacerbations may be triggered by a number of atmospheric and domiciliary environmental factors as well as by those encountered in schools and workplaces. The majority of exacerbations, particularly in children, coincide with respiratory viral infections, most commonly rhinovirus. As most respiratory viruses and many aeroallergens appear in seasonal patterns, asthma exacerbations, particularly those requiring emergency treatment, show analogous seasonal cycles which differ in form in children and adults. While similar in form between the sexes, they differ in amplitude, with boys having higher risks of exacerbation in childhood and women in adult life. Simultaneous exposure of asthmatics with respiratory viral infections to allergens or air pollutants may significantly increase the risks of exacerbation. Access to and compliance with inhaled corticosteroid treatment is an important predictor of the likelihood of asthma exacerbations occurring, including those that occur during respiratory viral infections. Epidemiologically, the degree of asthma control achieved by asthmatics is an important predictor of the likelihood of disease exacerbation including respiratory failure, death, and health service consumption.
- COPD, chronic obstructive pulmonary disease
- ER, emergency room
- FEV1, forced expiratory volume in 1 second
- ICS, inhaled corticosteroid
- PEF, peak expiratory flow
- RVI, respiratory viral infection
- asthma
- exacerbation
- epidemiology
- seasons
- allergen
- anti-asthmatic drugs
Statistics from Altmetric.com
- COPD, chronic obstructive pulmonary disease
- ER, emergency room
- FEV1, forced expiratory volume in 1 second
- ICS, inhaled corticosteroid
- PEF, peak expiratory flow
- RVI, respiratory viral infection
Exacerbations of asthma symptoms produce significant costs for healthcare systems and seriously diminish the quality of life of patients and their families when they occur.1–,3 Reduction in the number and severity of asthma exacerbations has been the goal of most pharmacotherapeutic interventions introduced in the last 50 years.4 However, understanding of the determinants of asthma exacerbations is imperfect, not surprisingly given the difficulty in determining exposures to causal factors and the complexity of interactions between them.
This review describes the epidemiology of asthma exacerbations, some of which occur sporadically while others appear to be clustered and often associated with seasons of the year. Some of the latter may be truly seasonal, such as those caused by pollens and moulds, while some apparent seasonality may be driven by administrative decisions that coincidentally foster exposure to factors that cause asthma exacerbations. Understanding of the factors provoking these seasonal cycles may offer significant opportunities for improved disease management. Some factors that can cause worsening of asthma symptoms, such as occupational dust and chemical exposures, are not intrinsically cyclic in their appearance but may be influenced by factors that are. Many exacerbations of asthma may result from a combination of insults, only some of which may be cyclic.
Seasonal cycles of asthma exacerbations requiring hospital treatment have been reported in many Northern Hemisphere countries including Canada, the USA, the UK, Mexico, Israel, Finland, and Trinidad, West Indies.5 Similar cycles have also been reported in Australia and New Zealand.6,7 The epidemic peak in early autumn (fall) in all countries examined is of greatest magnitude in children, less in younger adults, and barely detectable in the elderly.
The severity of asthma symptoms and the likelihood of their exacerbation is also significantly influenced by the medication available to and used by patients. While analysis of the relative efficacy of different asthma medications is outside the scope of this review, information about patterns and determinants of medication use important in the epidemiology of asthma exacerbations is included.
Descriptions of asthma have been recorded since the time of Hippocrates.8 Ben Maimon, writing in the 12th century, provided elegant descriptions of worsening asthma symptoms associated with seasons and also recognised that respiratory infections often triggered severe asthma exacerbations.9 In the 17th century Sir John Floyer,10 himself severely asthmatic, used diaries to collect data on his own symptoms and those of his patients, observing seasonal cycles and that exacerbations were frequently associated with storms. In the 19th century understanding of the determinants of asthma and its exacerbations grew dramatically and saw publication by Henry Salter, another asthmatic physician, of a definitive text on the disease which reported the importance of heredity as well as the effects of exposure to allergens, notably cat.11
DATA COLLECTION METHODS
Over the last several years we have, following ethical approval, collected data from multiple sources to make more comprehensive international comparisons of patterns of respiratory disease. Data for all in-patient respiratory disease hospital admissions were obtained from The Canadian Institute for Health Information (1990–2004, also all emergency room presentations in Ontario, Canada, 2001–2004), the Centre for Epidemiology (EpC) at the (Swedish) National Board of Health and Welfare (1992–2002), the New Zealand Health Information Service (1995–2004), and the Small Area Health Statistics Unit, Imperial College, London, UK (1990–2002). Prescription data for the year 2000 for Ontario, Canada were obtained from Brogan Consulting Inc, Ottawa, Canada.
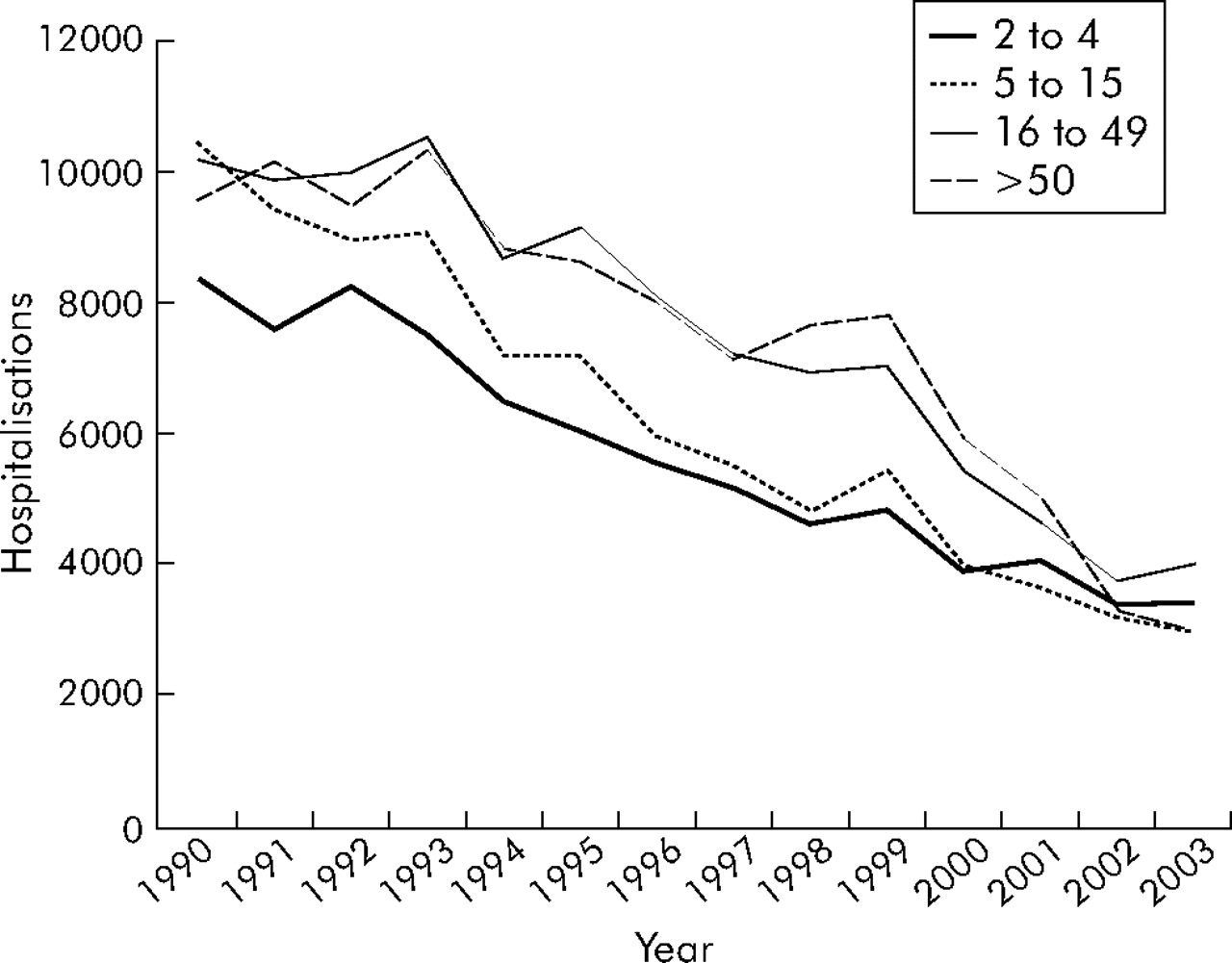
Many published reports of the epidemiology of asthma exacerbations have analysed data on hospital admissions or emergency room (ER) visits. Patterns of health service use for asthma have changed significantly over the last two decades, with consumption of many services increasing while in-patient hospital admission rates have declined (fig 1⇓). These changes may be related to multiple factors, the relative magnitude and direction of the effects of which can only be conjectured, including a possible increase in disease prevalence, increased use of asthma control medications, lower propensity of physicians to admit patients to hospitals, and administrative incentives in some countries to reduce hospital admissions.
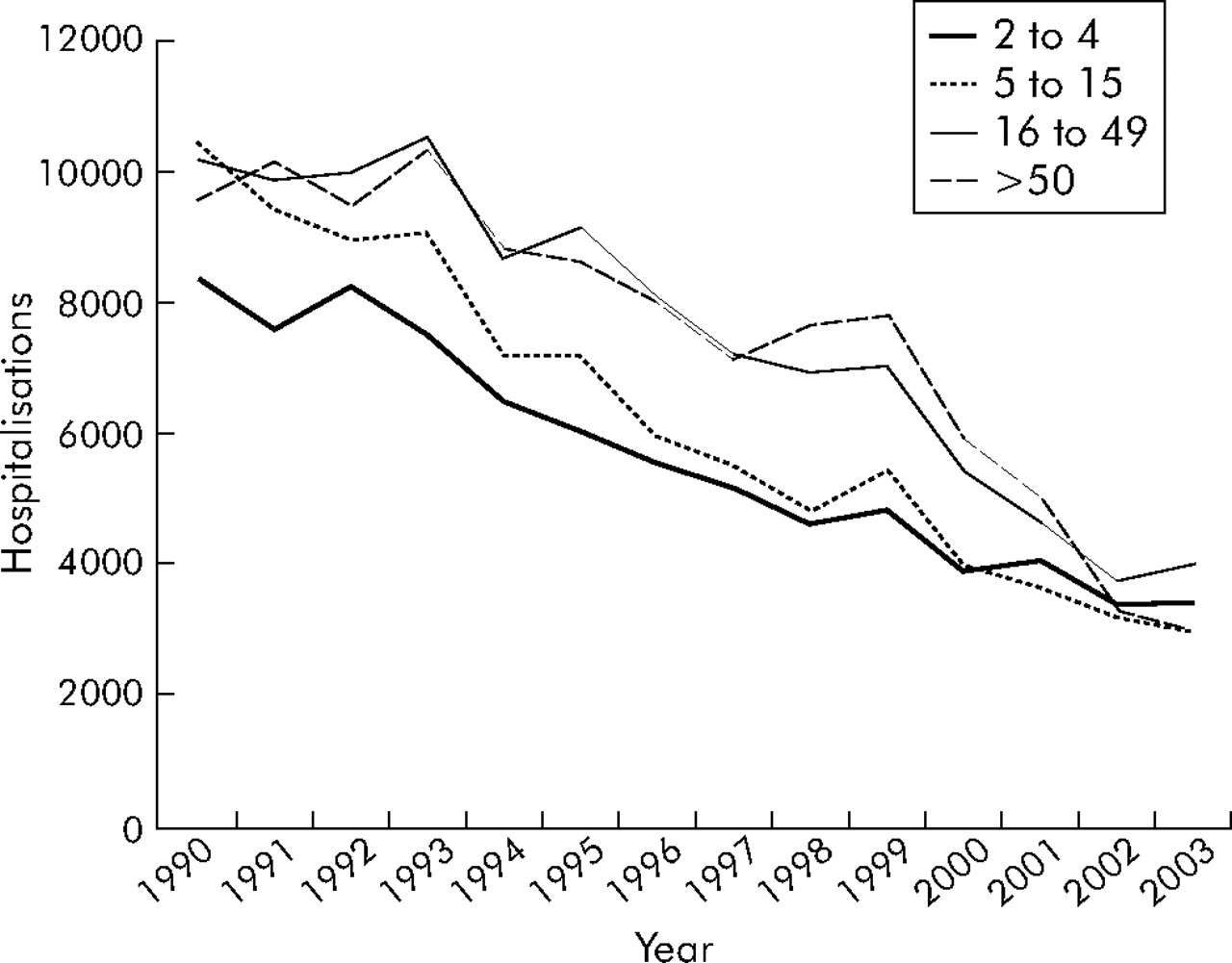
Numbers of hospital admissions by age group in Canada (excluding Quebec) from 1990 to 2003.
Data extracted from hospital records should be interpreted cautiously in epidemiology, particularly when temporal trends are being evaluated. Methods used to assign diagnoses vary between jurisdictions and are influenced by many factors including methods of reimbursement for hospital services. The International Classification of Diseases (ICD) has also changed over time. For example, the assignment of diagnoses of asthma and chronic obstructive pulmonary disease (COPD) in Canada changed in 2002 between ICD versions 9 and 10, reducing the validity of long term analyses of the patterns of these diseases. Very few studies have systematically audited hospital charts to verify differential diagnoses of respiratory diseases. Furthermore, the relation between asthma exacerbations and respiratory viral infections (RVIs) is complex and differential diagnosis not always straightforward.
There are important differences in the frequency and patterns of asthma exacerbations with age, possibly related to changes in responses to risk factors. Epidemiological studies of determinants of exacerbations in very young children are few. They may be affected by the same factors as older children, but this remains to be established.
Studies of asthma exacerbations fall into two broad groups—those that identify a short term fluctuation in asthma exacerbations and then seek to explain it by examining coincident changes in one or more variables, and those that set out to examine the relation of cycles of variation in asthma morbidity or mortality to specific risk factors. The first are typically based on hospital case series and the latter are generally population based. While valuable information is contributed by the former, these studies may be limited by not recognising the cyclical nature of variation in rates of asthma exacerbations, or the full range of variables that may contribute to them.
ANNUAL CYCLES OF ASTHMA MORBIDITY AND MORTALITY
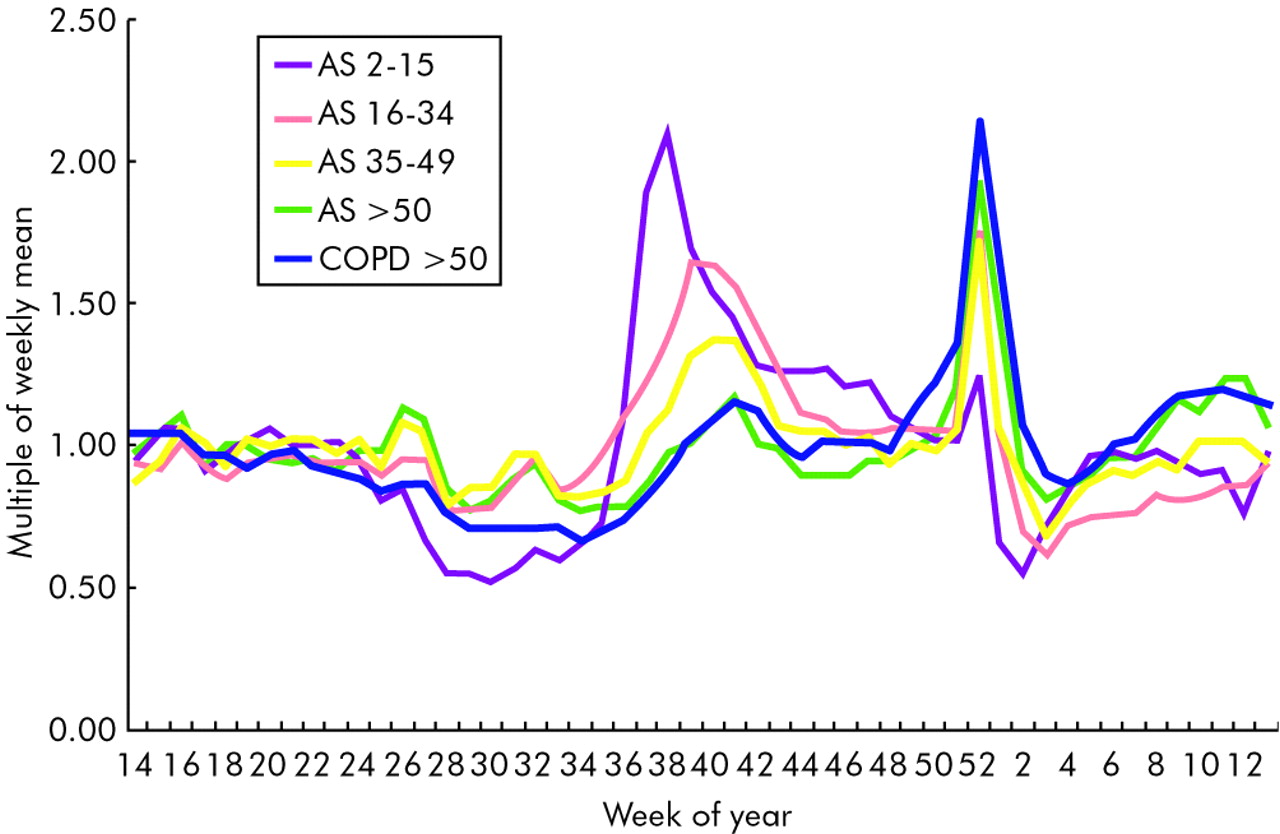
The annual cycles of ER presentations in Ontario, Canada (population approximately 11.5 million) for asthma of children and three adult age groups, using 3 years of aggregated data, are shown in fig 2⇓. Data for ER presentations for COPD of people over 50 years are also shown. The differences observed between age groups in annual cycles of asthma exacerbation are striking, suggesting age related differences in response to cyclic causal factors. The peaks in ER visits, which are identical to those of in-patient hospital admissions in late September (around week 38) are of greatest magnitude in children and decline in amplitude with age; however, detectable peaks are present at this time in adults aged over 50 for both asthma and COPD. There is also an apparent lag in timing between the peak of the autumn (fall) epidemic for children and those for other age groups which appear 1 or 2 weeks later. Over the 13 years from 1990 to 2002 the September peak of asthma hospital admissions in school age children in Canada occurred at a very precisely defined interval which was highly correlated with the day of school return after the long summer vacation.12 Peaks in other age groups occurred later, suggesting that school age children are the primary vectors of agents causing asthma exacerbations to both older and younger family members.

Annual cycles of emergency room presentations for asthma (AS) and chronic obstructive pulmonary disease (COPD) as multiples of the weekly mean number by week of the year, combining all events from April 2001 to March 2004 in Ontario, Canada. The scale has been set to run from week 14 to week 13 to permit an unbroken view of the New Year period.
Figure 2⇑ also shows that further peaks of asthma exacerbations requiring emergency care occur in the weeks either side of the New Year. The amplitude of these by age group is essentially the reverse of those seen in September. The implications of this observation and the possible causes of the phenomenon are not currently known and will be discussed in a future report.
The likelihood that the asthma hospitalisation peak in late summer and early autumn is directly related to school return is strengthened by international comparisons (fig 3⇓). In England and Canada, school return after the summer vacation is for most children in the first week of September, while in Scotland and Sweden it is in the third week of August. Large peaks in hospital admissions for asthma occur 2–3 weeks after school return in all four countries, despite their different vacation schedules. However, peaks in Scotland and Sweden are of a lower amplitude than those in Canada and England, suggesting that conditions in August underlying school related asthma exacerbation risk factors may be less favourable than those in September.

Aggregated annual cycles of hospital admissions for asthma as multiples of the weekly mean number, by week of the year, combining all events for 1998 and 1999 in Canada, Sweden, England, and Scotland.
Cycles of asthma exacerbations and respiratory viral infections (RVIs)
Viral respiratory tract infections, particularly of rhinoviruses, are associated with the majority of asthma exacerbations in both children and adults.13,14 Rhinovirus infections have been shown to be most common in early autumn,15 and school age children have been shown to introduce rhinovirus infections into their families three times more frequently than working adults.16 Increased rates of hospital admissions for asthma in children and adults and higher rates of RVI in children have been reported to coincide,17,18 both being greater during periods of school attendance.18 In a study of all children presenting to ERs for asthma in a major Canadian city during September 2001,19 62% were found to have respiratory virus infections of which two thirds were of rhinovirus. In the control group for that study, 42% of the asthmatic children not requiring ER treatment during September had RVIs at a single encounter during that month, suggesting that, over the full epidemic period, the figure may have been higher.
The observation that school age children experience the earliest peaks of asthma exacerbations after school return in September in the Northern hemisphere and that the timing of these is in synchrony with the date of school return12 suggests that rhinovirus infections may play a major part in these epidemics and in the overall annual cycle of asthma morbidity.
Cycles of asthma mortality
In contrast to hospital admissions for asthma in children and younger adults which peak in early autumn, it has been reported in both the US and Britain that deaths in these age groups attributed to asthma are more common in the summer months.20,21 With increasing age, deaths from asthma become less common in summer and more common in the winter months.20 However, it is possible that the coding of deaths in the elderly, particularly during periods of high risk of RVIs, may be imperfect. While deaths from asthma in the winter months, particularly in the elderly, may be associated with seasonal RVIs, the reasons for the summer peak in young people are unclear but have been hypothesised to be related to aeroallergen exposure.
EFFECTS OF AGE AND SEX
Asthma exacerbations
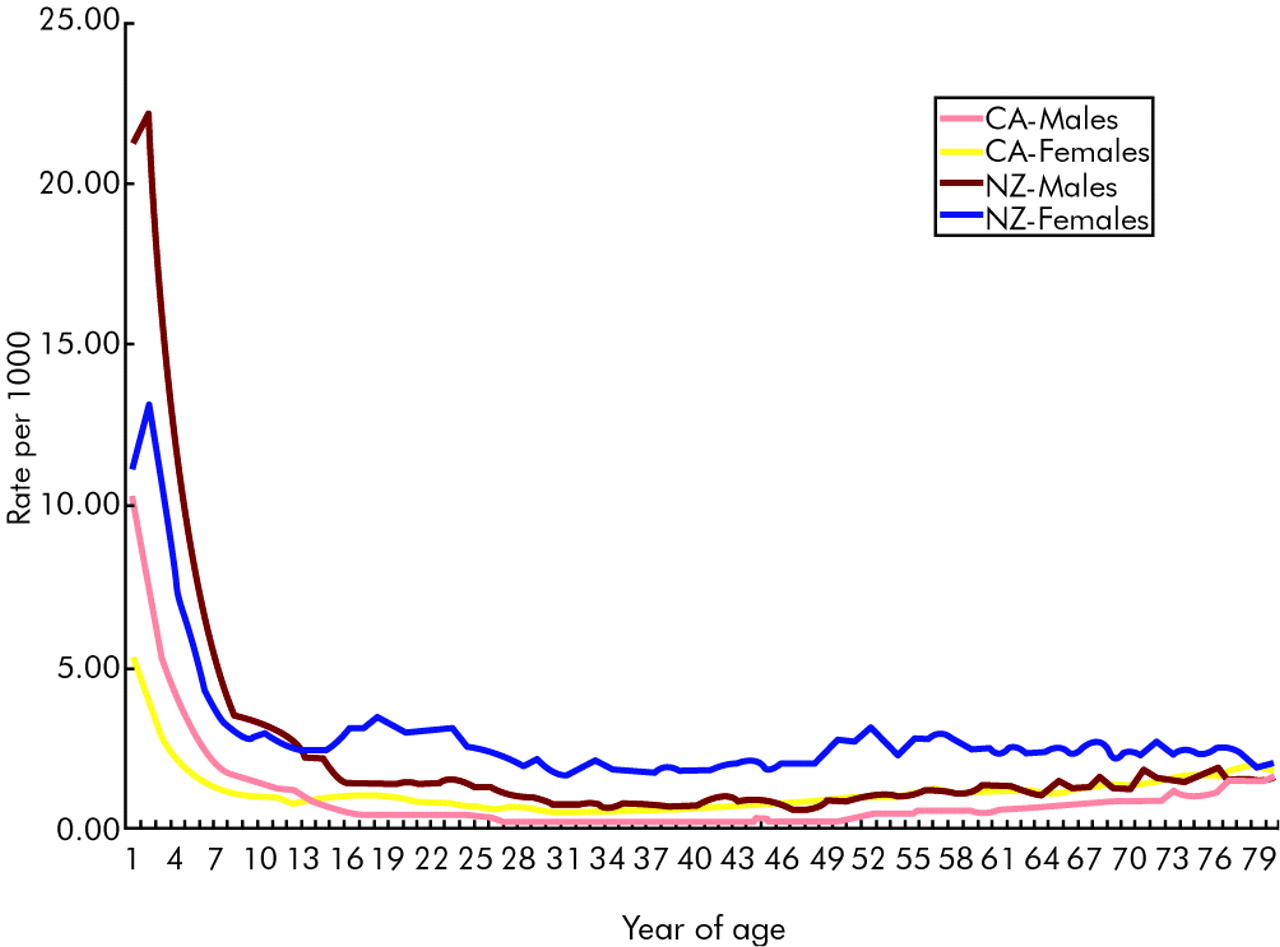
The risks of asthma exacerbations show striking differences with age and also between the sexes. Figure 4⇓ shows the rates of hospital admissions for asthma from 1995 to 1999 in Canada and New Zealand by sex and age. The rates decline dramatically throughout childhood where they are roughly twice as high in boys as in girls. Between the ages of 13 and 14 years a crossover of rates occurs and thereafter, as noted in other reports,22,23 the risk of an asthma exacerbation requiring admission to hospital in women is approximately double that in men. It has been suggested23 that these differences may be attributable to hormonal influences, although no specific mechanism for this has been postulated. However, while there is some variability in published reports, the risk of an asthma exacerbation during phases of the menstrual cycle does not appear to vary significantly.24

Rates per thousand population of hospital admissions for asthma by year of age and sex in Canada (CA) and New Zealand (NZ), combining data for all events from 1995 to 1999.
In a randomised controlled clinical trial comparing different regimens of inhaled corticosteroids (ICS) and long acting β2 agonists in adults aged 18–70 years, women were found to have 1.89 times the risk of a severe exacerbation than men.4,25 In the same study the risk of an exacerbation was found to increase by 1.011 (95% CI 1.001 to 1.023) for every year of age. Manfreda et al26 conducted a survey of the prevalence of asthma symptoms in adults in six centres in Canada: 7.75% of women and 5.4% of men reported an asthma attack in the previous year. All asthma symptoms were more frequent in women than men, but only moderately so. Nocturnal cough showed the greatest difference, being 33% more frequent in women.
Figures 5A and B⇓ show the rates of hospital admissions for asthma in Canada and New Zealand by week of the year and by sex for children aged under 16 years (fig 5A⇓) and for adults aged 16–49 years (fig 5B⇓). The form of the annual asthma hospital admission cycles in Canada and New Zealand is quite distinct. A major peak in children and a peak of lesser amplitude in adults occurs around week 7 in New Zealand, 2 or 3 weeks after school return following the summer vacation, seasonally analogous to the Canadian September experience. While there is an almost doubled risk of hospital admissions in boys compared with girls in both countries, the cycles are of almost identical form in both sexes. In adults, the form of the cycles is different from those in children but, again, within each country they are similar in both sexes. However, the change in risk between the sexes from childhood to adulthood seen in fig 4⇑ occurs over the whole annual cycle, with the risk of hospitalisation in adult women more than double that in adult men.

Rates per thousand population by sex of hospital admissions for asthma in (A) children aged 2–15 years and (B) adults aged 16–49 years in Canada (CA) and New Zealand (NZ), combining data for all cases from 1995 to 1999.
The differences between the risks of severe exacerbations and the prevalences of reported asthma symptoms in men and women suggest intriguing opportunities for further research. This is highlighted by the very consistent and narrowly defined age at crossover in risk that occurs at puberty, particularly increasing the risks in women.
Asthma mortality
As noted earlier, annual cycles of asthma mortality move with increasing age from peaks in the summer months to the winter. Asthma deaths are rare in children, but the risk increases progressively with age. In the US, rates observed between 1982 and 1986 were 0.17 per 100 000 population in the under 5 age group and 6.71 per 100 000 in adults over 65 years.20 In the same study, by sex over all ages, the risk of death was 1.27 per 100 000 in males and 1.75 per 100 000 in females.
The risk of death from asthma has declined over the last two or three decades in children and adults in both the US and Britain.27,28 In British children, between 1968 and 2000 the rates of asthma mortality per 100 000 population fell from 0.58 to 0.13 in 1–5 year olds, from 0.53 to 0.23 in those aged 6–10 years, and from 1.38 to 0.37 in those aged 11–16 years.27 In the US, between 1995 and 2001 across all ages in the white population death rates fell from 1.26 to 0.78 per 100 000.28 Notably, the same study found that, while a decline in asthma deaths had occurred in the black population, their risk of such events remains over three times that of white subjects.
ENVIRONMENTAL FACTORS AND ASTHMA EXACERBATIONS
Climate
Climate is defined by seasons and much human behaviour is dictated by them. Many factors associated with asthma exacerbations such as pollens, moulds, and fungal spores tend to appear at specific times of the year, and exposures to these are influenced by weather patterns. The prevalence of asthma has been reported to be higher in regions with warmer climates and lower in regions with greater variation in average temperature and relative humidity,29,30 both of which may affect the quality and quantity of aeroallergen exposure.
The annual cycle of asthma exacerbations of children in Trinidad, West Indies—approximately 10 degrees of latitude above the Equator—is very similar in form to that shown for the four northerly countries in fig 3⇑,31 suggesting that the autumn epidemic is substantially independent of climatic influence. The prevalence of asthma symptoms has been shown to be greater in regions with higher indoor relative humidity.29,30 It is possible that this is related to indoor allergen levels, but also that more humid indoor environments may promote more effective transmission of RVIs.32
Aeroallergens
A study using a uniform national data set examined Canadian cities with significantly different climates, adjusting for this, season and ambient air pollution levels, and found that a doubling in spore and pollen levels was associated with increases in daily asthma hospital admission rates of 3.3% (95% CI 2.3 to 4.1) for basidiomycetes and 2.0% (95% CI 1.1 to 2.8) for grasses.33
Thunderstorm activity is associated with significant increases in rates of asthma exacerbation. A sixfold increase in calls to a GP home visit call centre was recorded during a bout of severe thunderstorms in the UK,34 and increases in ER use for asthma coinciding with thunderstorms have been reported in well conducted studies in North America and Australia.35,36 High concentrations of aeroallergens, especially grass pollens and fungal spores, were found to coincide with thunderstorm activity in all of these studies.
Geographical clusters of asthma exacerbations also occur following atmospheric release of allergenic dusts from soy and castor beans. These invoke a specific allergenic response rather than simply irritant effects.37,38 While these allergens may be most commonly encountered in occupations related to their handling, both soy and castor dust have been shown to affect general populations. Other dusts of known or yet unknown risk for causing asthma development may pose threats to those exposed through atmospheric or domiciliary contamination or secondary transmission from family members’ clothing. Primary or secondary exposures to the multitude of irritant or allergenic dusts related to hobbies or domestic pets are also of great clinical importance in asthma management.
Asthma deaths and aeroallergens
In children and young adults, deaths from asthma in the summer months have been hypothesised to be associated with higher levels of aeroallergens.20,21 It has been estimated that the risk of death from asthma increased 20% for every increase in daily atmospheric spore level of 1000 spores per cubic metre in Chicago in the period from 1985 to 1989.39
One study from the US Midwest found that 10 of 11 cases of severe respiratory arrest, including two deaths, were skin test positive to Alternaria alternata compared with 31 of 99 matched asthmatic controls with no history of respiratory arrest.40
Ambient air pollution
Some of the methodological challenges to segregating the individual effects of aeroallergens, climatic factors, and ambient air pollution levels to asthma exacerbations, particularly those relating to the use of time series analysis, have been discussed by Atkinson and Strachan.41 It is possible as well that the degree of risk posed to asthmatics by similar ambient air pollution levels may vary with seasonal changes in air mass conditions.42 Air pollutants, particularly those associated with diesel exhaust, are unquestionably associated with increases in the occurrence and severity of respiratory symptoms, and the magnitude of local exposures may not be reflected in ambient pollutant monitoring data.43,44 The influence of ambient air pollution on asthma exacerbations may initially be a short term effect which varies in magnitude with seasonal changes in weather patterns and aeroallergen levels. However, it is also likely that exposure of asthmatics to combinations of high risk atmospheric conditions and/or domiciliary air pollution during RVIs (the most common cause of exacerbations) may increase the risk of these occurring.45
In a case-control study comparing children aged 3–17 years hospitalised for asthma with a stable asthmatic group and a group hospitalised for non-respiratory diseases, a combination of an RVI and sensitisation to and exposure to high levels of allergen increased the risk of hospital admission significantly (odds ratio 19.4, 95% CI 3.7 to 101.5).46
The difficulties referred to earlier of attributing changes in asthma symptom to levels of individual aeroallergens or air pollutants and their complex interaction with climate and other possible exposures may thus be compounded if both, in turn, amplify the effects of RVIs. It is also possible—but remains to be investigated—that the nature of such interactions is different between age and sex groups of the asthmatic population.
ASTHMA CONTROL AND ASTHMA EXACERBATIONS
While the incidence of asthma symptoms—as opposed to the prevalence of the disease itself—may be partly related to climate, existing evidence suggests that, in countries in which asthma control medications are widely available, much of the variation among them in rates of asthma exacerbation is related to drug use.47–,49 Epidemiologically, there is a striking relationship between the number of prescriptions for inhaled steroid products filled by patients and health service use for asthma exacerbations or asthma related death.50
The efficacy of ICS in asthma control has been clearly demonstrated in both children and adults.51 However, paradoxically, some investigators conclude that ICS may not prevent asthma exacerbations accompanying RVIs52–,54—which are associated with the majority of exacerbations in adults and over 80% in children13,14—and that ICS should not be prescribed for mild intermittent viral infection associated asthma, particularly in children.55,56 The results of three clinical investigations that have examined the effects of ICS in RVI associated asthma exacerbations bear close scrutiny.
The first,57 a randomised trial of ICS in children, can be interpreted as showing no difference between the effects of ICS and placebo on symptoms of a cold per se, but may more appropriately be interpreted as showing a clinically and statistically significant benefit overall in the respiratory health of asthmatics favouring ICS, including during RVI. The study was conducted to determine the value of ICS compared with placebo over a 1 year period in children aged 7–9 years who had wheezing associated with upper and lower respiratory tract infections. Outcome measurements included forced expiratory volume in 1 second (FEV1), methacholine PD20, and the percentages of days with episodes of upper and lower respiratory symptoms and of reduced peak expiratory flow (PEF). The study was designed for 112 children, recruited 104, and was completed by 50 receiving ICS and 44 receiving placebo. During the study both FEV1 and methacholine PD20 showed significant and consistent improvement in the ICS treated children. The authors conclude that no statistically significant differences were found in the percentages of days with symptoms or in the frequency, severity, or duration of upper and lower respiratory tract and PEF between ICS and placebo. However, the mean percentage of days with lower respiratory tract symptoms was 31 in the placebo group and 20 in the ICS group (p = 0.1). It would perhaps be fair to conclude that this study may not have been adequately powered and shows a mixture of results that do not wholly support a conclusion that there is no benefit of ICS in asthmatics during RVI.
The second study of 43 initially poorly controlled asthmatic subjects58 examined asthma symptoms during a baseline period of poor control and a period of subsequent good control including asthma exacerbations. Patients in the study were assessed during the baseline period and then prescribed budesonide twice daily and followed with daily collection of PEF measurements and other data for 18 months. They were asked to contact study personnel if symptoms worsened. Of the 43 patients, 26 experienced a total of 40 asthma exacerbations during the study, of which 38 followed apparent RVIs. In the period of poor control, diurnal variation in PEF (amplitude as a percentage of the mean) averaged 21.3 (95% CI 18.8 to 23.7) compared with 5.4 (95% CI 3.3 to 7.4) during the well controlled period and 7.7 (95% CI 5.7 to 9.8) during exacerbations. Mean morning PEF was 63.5% of the predicted value (95% CI 57.3 to 69.6) in the poorly control period, 90.2% (95% CI 83.8 to 96.7) in the well controlled period, and 77.2% (95% CI 71.3 to 83.1) during exacerbations. The authors state that “pre-existing inflammation may have been kept to a minimum by inhaled corticosteroid treatment, so the PEF changes that we observed during clinical respiratory infections may more closely represent an effect attributable to the viral infection itself”.
In the third study,59 25 steroid naive asthmatic subjects were randomised to budesonide (n = 12) or placebo (n = 13), inoculated with rhinovirus, and biopsy specimens were subsequently taken to evaluate inflammatory changes in the bronchi. Histamine challenge PC20 before treatment did not differ between the groups. Two drug and two placebo treated subjects were withdrawn from the study. Following 2 weeks of treatment the budesonide treated group showed a statistically significant improvement in PC20 (p = 0.02) which was sustained when measured at day 4 following rhinovirus infection (p = 0.02). The beneficial effect of budesonide on PC20 continued until the end of the study at day 13 following infection but was no longer statistically significant at that point (p = 0.18). One may speculate that, in a study with even a slightly larger sample size, the beneficial effect of budesonide would have been detected at every point of measurement.
Wide international variation has been reported in the degree of symptom control achieved by asthmatics. In the Asthma Insights and Reality in Europe (AIRE) study,60 complete control of severe persistent disease varied in adults from 85.7% in Germany to 52.3% in Britain. In children, 68.4% reported complete control in France (the highest) while the lowest (29.4%) was also found in Britain. ER treatment for adults was required by 4.7% in France and by 22.2% in Spain and, in children, ranged from 6.8% in the Netherlands to 39.5% in Spain. The methodological difficulties of formally examining a relation between self-reported control and ER use between countries are obvious, and this was not attempted in the AIRE study.
The European Community Respiratory Health Survey (ECRHS)61 examined rates of medication prescription and compliance with their use and related these to ER visits for asthma. A weak relation was found between low compliance with medications and higher ER use, with the lowest rate of compliance in the US (40%) and the highest in Iceland (78%).
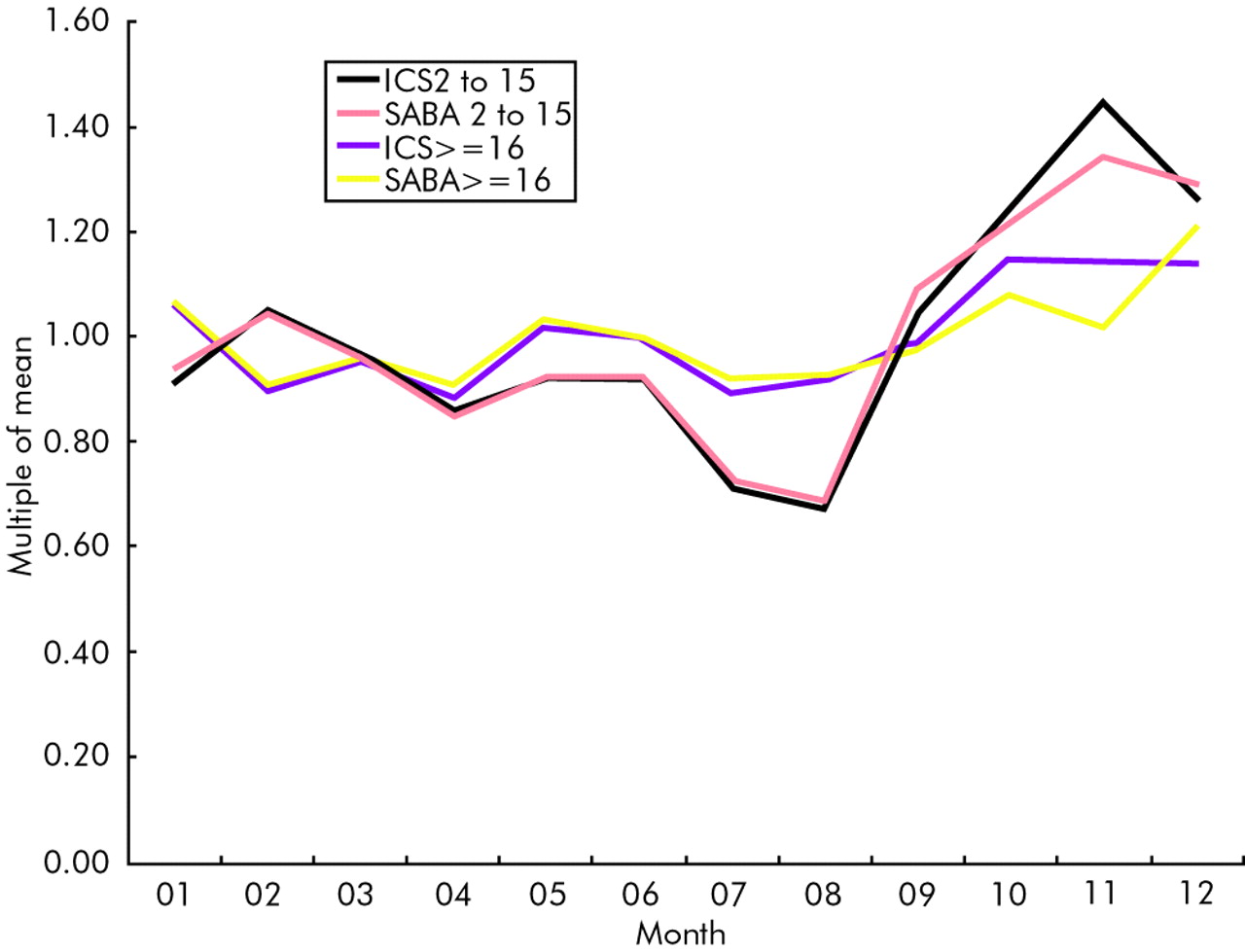
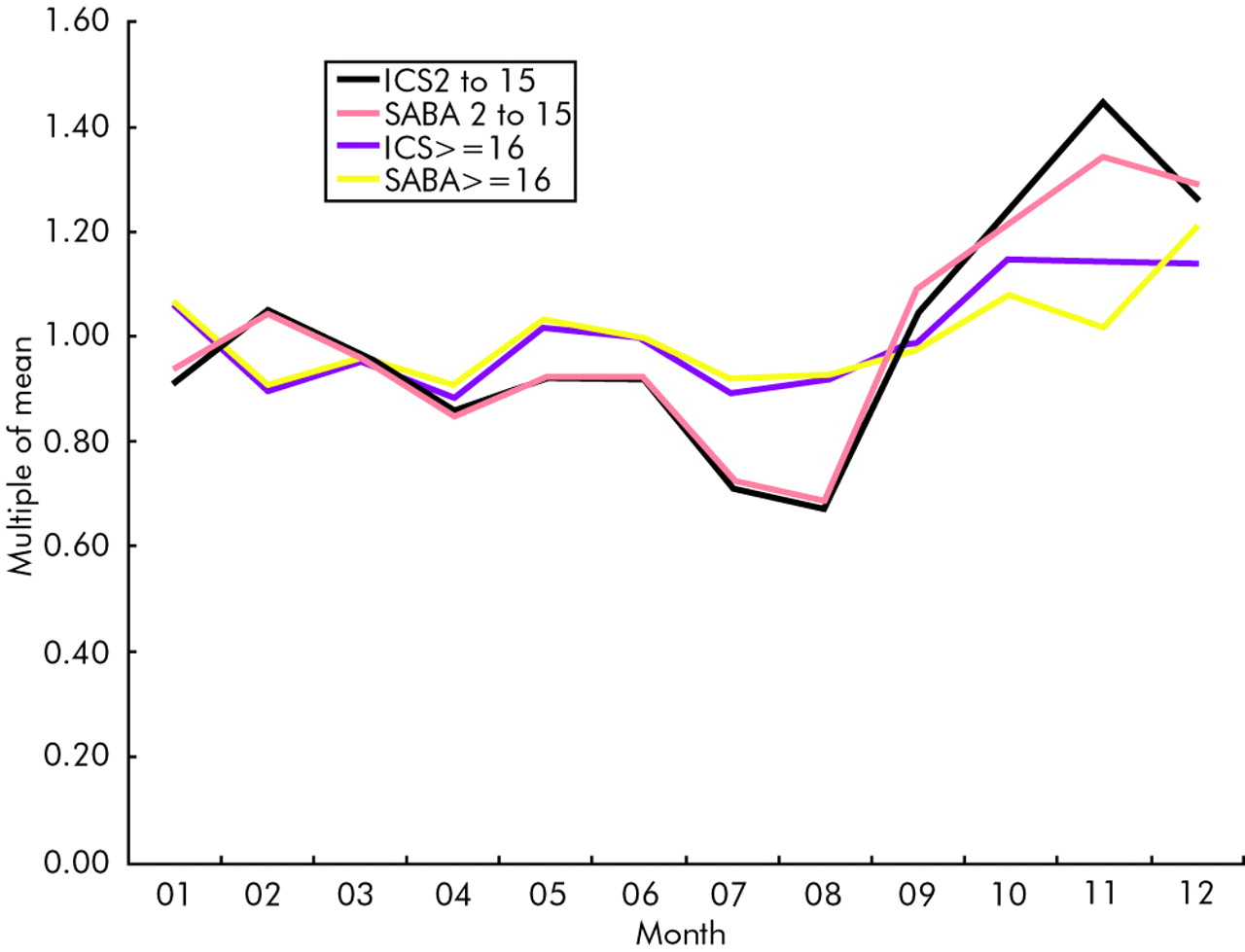
Figure 6⇓ shows the numbers of prescriptions filled for ICS and short acting β2 agonists in Ontario, Canada by month for children and adults in the year 2000. Lower levels of prescription filling occurred in the summer months (especially in children), with a rapid acceleration (again particularly in children) following school return in September. The pattern in adults is smoother, with highest prescription filling levels at the turn of the year. These patterns suggest that prescriptions are most often filled after symptoms worsen or exacerbations occur. In combination with the ecological data in the AIRE and ECRHS surveys and the results of the study by Suissa et al50 relating the numbers of ICS prescriptions filled to health service use and asthma mortality, lack of asthma control may be the most important determinant of variation in asthma exacerbation rates.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Number of prescriptions for inhaled corticosteroids (ICS) and short acting β2 agonists (SABA) filled in the year 2000 expressed as multiples of the monthly mean number in children aged 2–16 years and adults aged 16–49 years. (Data from Brogan Consulting Inc).
CONCLUSIONS
Asthma exacerbations show remarkable patterns of seasonal variation that may, at least in most countries, be substantially related to factors that condition the transmission of RVIs. These include whether or not schools are open and the occurrence of other events that may foster RVI transmission. While the majority of asthma exacerbations coincide with RVIs, the effects of these on asthmatics may be amplified by poor air quality (both ambient and domiciliary) and exposure to allergens, but the severity of asthma symptoms experienced during exposure to these insults will depend primarily on the degree of asthma control achieved in a given patient.
The long term effects on respiratory health of the frequency and/or severity of asthma exacerbations are not well characterised, but it is likely that, in asthmatics of comparable disease severity, those who experience more or worse exacerbations may show consequential decline in lung function.62 This is an area in which there are few studies from which to draw information and where further research is required.
The apparent differences in the character of asthma exacerbations between the sexes and particularly the sudden change in the risk of their occurrence that occur at puberty present significant opportunities to explore the role of sex hormones in asthma, and possible differences in responses to treatment.
The degree of access to, and compliance with, ICS treatment of asthmatics is likely to be the single most important factor in determining if symptom exacerbations will occur, whether or not they occur during RVIs. However, in practice, patient compliance with ICS is often poor.63
Given the primacy of RVI—particularly rhinovirus infections—in the genesis of asthma exacerbations and the likelihood that the role of these is compounded by other exposures, development of therapeutic interventions that can specifically inhibit the mechanisms by which respiratory viruses initiate asthma exacerbations should be a priority.
REFERENCES
Footnotes
Supported in part by unrestricted grants from AstraZeneca, Canada and GlaxoSmithKline, Canada.
Competing interests: MS has received research funds, consulting fees, and speaking fees from pharmaceutical companies with asthma products including Altana, AstraZeneca, Centocor, GlaxoSmithKline, Merck Frosst Canada, Merck-Sharpe Dohme, and Schering. NJ has received research funds and/or consulting and/or speaking fees from the following pharmaceutical companies with asthma products: GlaxoSmithKline Canada, AstraZeneca Canada, Merck Frosst Canada, and Altana Pharma.