Article Text

Abstract
Background: Serological methods to monitor Pseudomonas aeruginosa colonisation in patients with cystic fibrosis (CF) are advocated but the diagnostic value of a commercially available P aeruginosa antibody test to detect early and chronic P aeruginosa colonisation in a non-research setting has not been assessed.
Methods: Colonisation with P aeruginosa was estimated by regular culture of sputum or oropharyngeal swabs during three consecutive years in 220 patients with CF aged 0–65 years. Commercially available ELISA tests with three P aeruginosa antigens (elastase, exotoxin A, alkaline protease) were performed at the end of the study period. In a subgroup of 57 patients (aged 4–14 years) serological tests were performed annually.
Results: Using culture as the reference standard, the ELISA tests using the advised cut off values had a sensitivity of 79% and a specificity of 89% for chronic colonisation. Receiver-operator characteristic curves were created to optimise cut off values. Applying these new cut off values resulted in a sensitivity of 96% and a specificity of 79%. All three individual serological tests discriminated well between the absence and presence of chronic P aeruginosa colonisation. The sensitivity of the individual antibody test was 87% for elastase, 79% for exotoxin A, and 76% for alkaline protease. First colonisation was preceded by positive serological results in only five of 13 patients (38%).
Conclusion: In patients with CF, serological tests using specific antigens are sensitive for diagnosing chronic P aeruginosa colonisation. However, the failure of serological tests to detect early colonisation in young patients emphasises the need for continued reliance on cultures.
- CF, cystic fibrosis
- ELISA, enzyme linked immunoassay
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- Pseudomonas aeruginosa
- cystic fibrosis
- serology
- serum antibodies
- prognostic value
Statistics from Altmetric.com
- CF, cystic fibrosis
- ELISA, enzyme linked immunoassay
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
Pulmonary colonisation with biofilm producing strains of Pseudomonas aeruginosa in patients with cystic fibrosis (CF) is associated with a decline in pulmonary function and subsequent morbidity and mortality.1,2 In infancy 10–30% of patients are colonised with P aeruginosa, and this increases to 80–90% during adolescence.3,4 Initial colonisation and early asymptomatic infection are close entities; these precede chronic colonisation and infection. The transition duration of initial asymptomatic colonisation and infection to chronic tissue destroying infection and colonisation varies among patients. In this paper we will therefore use the term “colonisation”. It is of major importance to detect P aeruginosa at an early stage since aggressive treatment of early colonisation might delay or prevent chronic colonisation.5,6 Acquisition of P aeruginosa is often monitored by culture of sputum or oropharyngeal swabs. Serological methods such as crossed immune electrophoresis (CIE), Western immunoblot, and enzyme linked immunoassay (ELISA) to detect P aeruginosa are not routinely used in CF centres.3,7,8 Precipitin measurement by CIE has been largely taken over by ELISA and Western blotting techniques. CIE and whole cell protein ELISA have a high sensitivity (96–100%) for chronic colonisation.9 ELISA with purified antigens has a lower sensitivity (15–100%), depending on the antigen and stage of colonisation.10 Recent prospective studies suggested that antibodies may be present before the first positive culture.11–,13
Antibody development is influenced by the immunological condition of the host, corticosteroid use, antibiotic treatment targeted against P aeruginosa, and P aeruginosa related factors such as phenotype and production of exoproteins.8,10,11 Only a few data are available on the clinical relevance of anti-P aeruginosa antibody responses. Obviously, these antibodies fail to eliminate P aeruginosa and lack protective effects.14,15 The antibody response seems to be more prominent in patients with severe clinical disease, suggesting they might play a pro-inflammatory role.16
In this study we assessed the value of a commercially available serological test using three purified antigens to detect chronic P aeruginosa colonisation in a large CF population. We also examined the value of these serological tests for early detection of P aeruginosa colonisation.
METHODS
Participants
The study was performed in the CF Centre, Utrecht, The Netherlands. All patients with a diagnosis of CF, confirmed by a sweat chloride test >60 mmol/l and/or genotyping were eligible to participate in the study. Fifty two adults and 168 children (age <18 years) participated in the cross sectional study; 57 of the 168 children also participated in a 3 year prospective study.
The medical ethics committee of the University Medical Centre Utrecht approved the study. All participants or their parents gave written informed consent.
Cultures
Sputum or oropharyngeal cultures were carried out for all patients according to the treatment protocol of the centre in three consecutive years from January 2002. When a patient was not able to produce sputum, an oropharyngeal swab was taken. The sensitivity and positive predictive value of oropharyngeal swabs ranges from 44% to 83%. However, for the classification of colonisation status, negative predictive values (percentage of patients with a negative test (oropharyngeal culture) who do not have the disease (P aeruginosa colonisation)) are more important. These negative predictive values range between 85% and 97%.12,17,18 The mean number of cultures per patient was six (median 4, range 3–43), depending on pulmonary condition.
Culture samples were inoculated onto blood and McConkey agar plates. After incubation at 37°C, media were inspected for any growth of P aeruginosa after 24 and 48 hours.
Classification of P aeruginosa colonisation status of patients over the 3 year period was based on the criteria of Lee et al19 (chronic colonisation: >50% of all cultures positive; intermittent colonisation: ⩽50% of all cultures positive with at least one positive culture; no colonisation: all cultures negative for P aeruginosa).
Enzyme linked immunoassay (ELISA)
At the end of the observation period in 2004, serum samples were obtained from the cross sectional study group. In the prospective cohort of 57 paediatric patients, annual serum samples were drawn concomitantly when cultures were taken. All serum samples were stored at −20°C.
Serological testing was performed using a commercially available ELISA kit (Mediagnost, Reutlingen, Germany). This semi-quantitative IgG ELISA consists of three common P aeruginosa antigens: elastase, exotoxin A, and alkaline protease. In brief, serum samples were diluted by a factor of 103 with phosphate buffered saline (PBS). In each well of a 96-well microtitre plate, 100 μl of a diluted sample was added and incubated at 37°C for 2 hours. After aspirating and washing three times intensively with PBS/Tween-20, 100 μl of conjugate solution (anti-human IgG peroxidase) was added to each well. The plate was further incubated for 2 hours at 37°C. After washing thoroughly, wells were filled with 100 μl substrate solution (tetramethyl benzidine) and again incubated at room temperature in the dark. After half an hour the reaction was stopped by sulphuric acid. Within 10 minutes the optical density was read by a photometer set at 450 nm. Titres were extrapolated from optical density values of two negative and two positive control serum samples according to the manufacturer’s manual.
Lung function
Clinical data for every CF patient are collected in a database annually. Data collected at the end of the observation period in 2004 were used to compare the lung function of patients chronically colonised with P aeruginosa with non-colonised patients (forced expiratory volume in 1 second as percentage of predicted (FEV1 % pred) and forced vital capacity as percentage of predicted (FVC % pred)).
Analysis of data
The ELISA manual advised a cut off titre against one or more of the tested antigens of 1:500 or 1:1250 (borderline positive or positive, respectively). When applying these cut off titres to our study group, low sensitivities of the ELISA for chronic P aeruginosa colonisation, with cultures as a reference standard, were found. The ability of the serological tests to discriminate between chronic colonisation and no colonisation was therefore estimated using the area under the receiver-operator characteristic curve (ROC area). The difference in discriminatory power between the individual serological tests was estimated by calculating the difference in ROC area (ΔROC area) with 95% confidence intervals, taking into account the correlation between the expressions as they were based on the same cases. Cut off titres with best discrimination (defined as the point on the ROC curve closest to the upper left corner) were used to classify patients as having negative or positive serological test results.20
The lung function data of chronically colonised and non-colonised patients were compared using the Student’s t test and multiple linear regression. These parameters were expressed as mean (SD). Differences were considered significant if the p value exceeded 0.05. Calculations were performed by Statistical Package for the Social Sciences (SPSS) Version 12.0 (Chicago, IL, USA).
RESULTS
Characteristics of study subjects
The mean (SD) age of the patients in the cross sectional study at the end of the observation period was 14.5 (10.6) years, and for those in the prospective study was 8.1 (2.8) years. Sixty seven patients had chronic colonisation with P aeruginosa, 60 were intermittently colonised, and 93 patients were not colonised. The characteristics of the study population are summarised in table 1⇓.
Characteristics of participants in the cross sectional and prospective studies
The impact of chronic P aeruginosa colonisation on clinical characteristics was estimated. Mean FEV1 % pred and FVC % pred were significantly lower in chronically P aeruginosa colonised patients than in non-colonised patients (FEV1 % pred 64.8 (29.2) v 89.0 (19.4); FVC % pred 80.0 (22.4) v 94.1 (13.4); p< 0.001, adjusted for age).
Diagnostic value of serological tests for chronic P aeruginosa colonisation
The ELISA manual regarded a titre of >1:500 against one or more of the tested antigens as borderline positive and a titre of >1:1250 as positive. With these cut off titres, sensitivity for chronic colonisation was 79% and 66%, respectively. The specificity was 89% and 96%, respectively.
The ROC curves (fig 1⇓) show that all three serological tests discriminate well between colonised and non-colonised patients. The ROC area was highest for elastase (0.926), followed by alkaline protease (0.909) and exotoxin A (0.874). There were no significant differences in discriminatory power (ROC areas) between the three serological tests. Test characteristics associated with best discriminatory cut off titres are shown in table 2⇓. Although alkaline protease has a higher ROC area than exotoxin A, it has a somewhat lower sensitivity (79% v 76%).
ROC areas and cut off titres with test characteristics
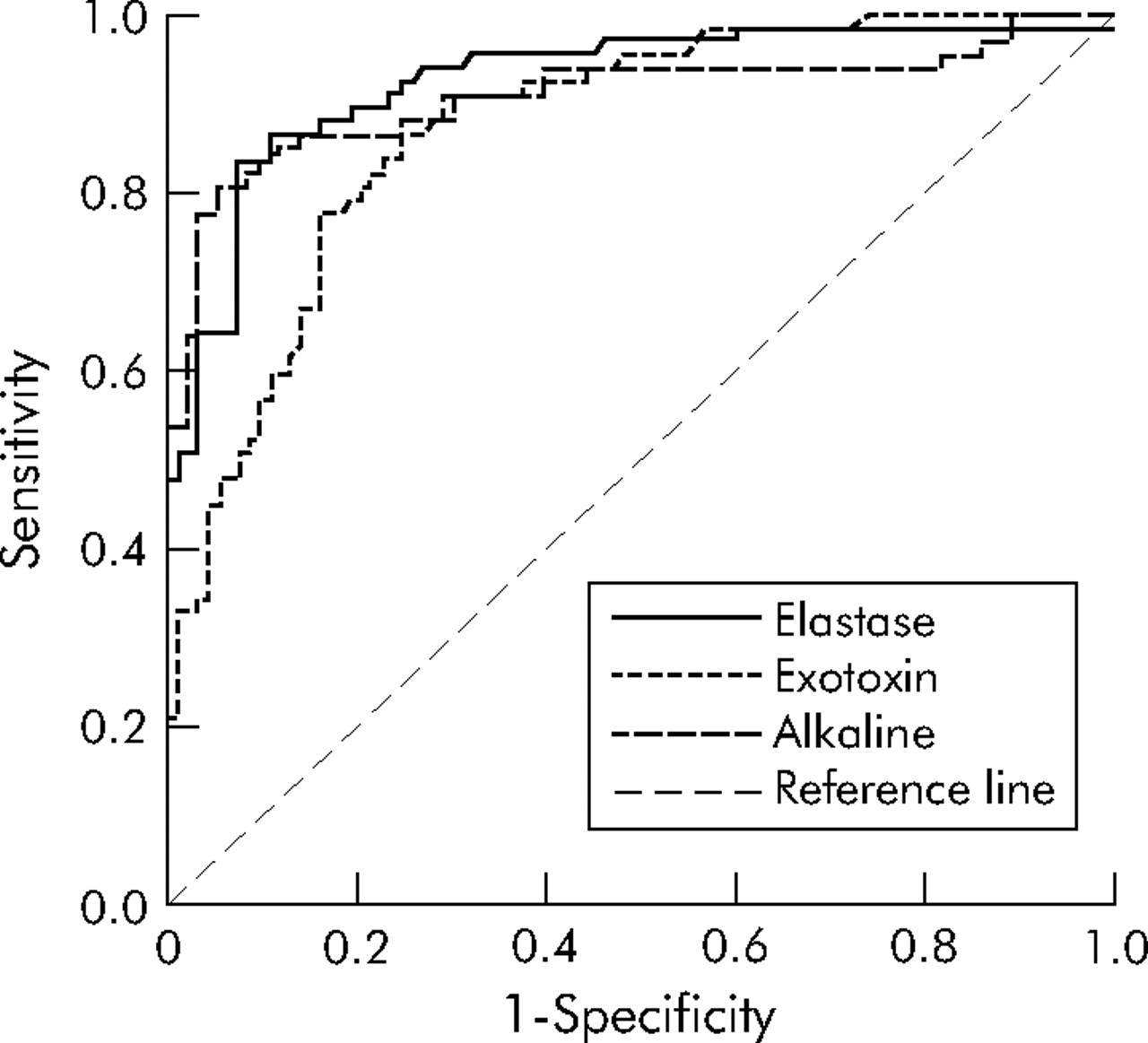
Receiver-operator characteristic (ROC) curves of three individual serological tests.
Positive serological results for elastase, exotoxin A, and alkaline protease were found in 87%, 79%, and 76%, respectively, of patients with chronic colonisation compared with 42%, 48%, and 17% of patients, respectively, in the intermittently colonised group and 11%, 19%, and 3%, respectively, in the non-colonised group. Combining the results of individual serological tests, 96% of chronically colonised patients had at least one positive antibody titre. Elastase serology was the most sensitive, but six elastase antibody negative patients appeared positive for other P aeruginosa antibodies if a combination of antibody tests was used. The specificity of the combination of serological tests was 79%. Test characteristics calculated with the cut off values for borderline positivity of the ELISA manual and test characteristics using the cut off values listed in table 2⇑ were compared: the sensitivity increased from 79% to 96% while the specificity decreased from 89% to 79%.
Prevalence of P aeruginosa positive cultures and positive serological tests
To measure the additional value of serological tests in comparison with cultures to detect P aeruginosa, data from cultures and serological tests for different age groups were analysed. One or more P aeruginosa positive cultures and/or positive serological tests were observed during the 3 year study period in 20% of the youngest patients (aged 0–2 years) and in 81% of the adult group (>18 years) (fig 2A⇓). All the paediatric age groups had more patients with positive cultures than with positive serological tests. In the two youngest age groups (0–2 and 3–5 years), no additional P aeruginosa was detected by serology. For children in the age group 6–8 years and older, evidence for additional P aeruginosa colonisation was obtained by serological testing rather than from culture alone in 3–11%. Chronic colonisation for each age group is shown in fig 2B⇓. None of the youngest patients (0–2 years) and 53% of the adult cohort (>18 years) were chronically colonised with P aeruginosa. Positive serological results accompanied chronic colonisation in all age cohorts except those aged 12–14 and 15–17 years.

{kind=link}
{kind=link}
(A) Prevalence of P aeruginosa positive cultures and positive serological results per age cohort. (B) Prevalence of chronic P aeruginosa colonisation per age cohort and positive serological results in chronically colonised patients.
Value of serological tests in early detection of P aeruginosa colonisation
Prospective data of 57 children show that 15 of these patients had a culture conversion during the follow-up period. Data of these patients are shown in table 3⇓. In this group, 5 patients showed positive serology prior to a positive culture, 7 patients remained seronegative and 1 patient had a simultaneous conversion for both culture and serology. Timing of positive serology did not depend on age. No uniform antibody pattern was seen in early detection by positive serology (table 3⇓). Evidence for positive serology at first positive culture and height of antibody titres could not predict P. aeruginosa colonisation to become transient or chronic. Ten patients from the prospective cohort showed a transient positive serology without any following positive culture.
Serological patterns in patients with culture conversion during follow up period
DISCUSSION
To our knowledge, this is the first published study to address the value of a commercially available ELISA test for detecting P aeruginosa colonisation in a large CF population. Using cut off values according to the manufacturer’s manual, this serological test has relatively low sensitivity for the detection of chronic P aeruginosa colonisation. After adjusting the cut off values extrapolated from ROC curves from our own population, serological tests against common P aeruginosa antigens had a higher sensitivity without a significant loss in specificity. However, from the prospective cohort data it seems that the additional value of serological testing for diagnosis of early P aeruginosa colonisation in comparison with successive cultures is limited, especially in young children.
Colonisation with P aeruginosa is a clinically relevant issue; P aeruginosa colonisation has a significant impact on lung function, even when adjusted for age. These data confirm previous studies that show worsening of clinical parameters after acquisition of P aeruginosa.2
To detect P aeruginosa colonisation, measurement of P aeruginosa antibodies is advocated. Previous studies show high sensitivity and specificity of serological tests for chronic P aeruginosa colonisation, depending on the serological method used.9,21,22 However, some of these studies included very small numbers of patients and test characteristics can be influenced by different definitions of P aeruginosa colonisation. Culture is often used as a reference standard. Culture sampling errors may occur and therefore may influence the characteristics of the serological test. We therefore examined cultures during three consecutive years to make a clear division between non-colonised and chronically colonised patients.
The ROC curves show that elastase, exotoxin A, and alkaline protease serological tests all discriminate well between colonisation and non-colonisation. Test characteristics depend on cut off values. Instead of using the cut off values suggested by the ELISA manual, new cut off values were estimated from the ROC curve to obtain the best discrimination. Using these cut off values, we calculated a higher sensitivity than with the cut off values advised by the manufacturer. With regard to the clinical relevance of P aeruginosa colonisation, the sensitivity of the test needs to be high. When a positive serological result appears without other signs of P aeruginosa infection, close monitoring of cultures can be performed to detect any underlying P aeruginosa colonisation.
Elastase serology is the most sensitive test for chronic colonisation, with a sensitivity of 87%. Hollsing et al,10 using a different ELISA assay, found an elastase sensitivity of only 23% for chronic colonisation in a small study cohort. A possible explanation for the large difference is the definition of chronic colonisation used. They used a classification of colonisation status based on cultures over a 6 month period prior to serological measurement while we defined colonisation over a 3 year period. Another explanation might be the low cut off titres that we used but, even with the cut off titres advised by the manufacturer, the sensitivity of our test was much higher. The sensitivity of the other two antibodies is also higher in our study than in other studies. Exotoxin A had a sensitivity of 79%, but the specificity was lowest of the three antigens. Alkaline protease had the lowest sensitivity (76%) but a very high specificity (97%) and might therefore be useful for ruling out P aeruginosa colonisation.
Single antigen ELISAs directed against P aeruginosa virulence factors fail to show an immunological response in all P aeruginosa colonised patients. In our study the detection rate increased from 87% to 96% compared with single antibody testing with elastase.
With regard to the use of successive cultures as reference standard, problems with definition of specificity may arise because early P aeruginosa colonisation might not yet be proved by positive cultures although the serological test is positive. On the other hand, a transient positive serological result without positive cultures was also seen in our follow up cohort. We did not determine antibodies in healthy controls but, as P aeruginosa is a common pathogen from the environment, it is possible that contact with these bacteria leads to transient antibody formation. Healthy controls might have positive antibody titres, as was shown by Pedersen et al.9
In children aged 4–6 years, serological tests were of no additional value for diagnosing P aeruginosa colonisation. Older patients have a higher prevalence of antibodies in the absence of positive cultures. At ages 6–17 years, only a small proportion of patients (3–11%) had positive serological results without a positive culture. The prevalence of P aeruginosa colonisation in the youngest patients was lower than described in recent literature. Burns et al12 showed that 72.5% of patients had evidence of P aeruginosa colonisation by culture and 97.5% by both culture and serology before the age of 3 years. In the study by Li et al,4 almost 90% of 3 year old patients had acquired P aeruginosa in their cultures.
The prospective data of 57 children show that, in case of culture conversions to a positive culture, no uniform serological pattern is seen. From the 13 patients who showed culture conversion, only five had early positive serological tests that could have been helpful in diagnosis. Thus, serological methods with one or more individual antigens as a screening tool for early P aeruginosa colonisation in a clinical setting do not seem to be very sensitive. The failure of serological tests to detect early colonisation in young patients emphasises the need for continued reliance on culture. West et al13 also found that only 54% of children had positive exotoxin A serology before or at the time a culture became positive. In our cross sectional study the antibody that was raised most often in non-colonised patients was exotoxin A, but in the longitudinal follow up it was not clear that exotoxin A titres increased before other titres. The height of the antibody titres could not predict whether early colonisation would become chronic. The cohort may have been too small to show a relation between increasing antibody titres and chronic P aeruginosa colonisation.
In the majority of patients with positive serological tests and negative culture the antibodies disappeared. It seems that single positive antibody titres without concomitant positive cultures do not predict whether a patient will become colonised.
In conclusion, serological tests using specific antigens are sensitive for diagnosing chronic P aeruginosa colonisation in patients with CF but, except in study settings, they are not of great additional diagnostic value in comparison with successive cultures. The antibody elastase is most sensitive for chronic colonisation. In early colonisation no uniform serological pattern is seen; titres might be raised before a culture becomes positive, but this is not a rule. To detect early colonisation in young CF patients, we would favour regular culturing instead of serological testing with specific antigens.
Acknowledgments
The authors thank Hanneke van Deutekom for performing part of the laboratory work.
REFERENCES
Footnotes
Published Online First 6 April 2006
Funding: none.
Competing interests: none.