Article Text

Abstract
Background: Acute lung injury (ALI) and its extreme manifestation the acute respiratory distress syndrome (ARDS) complicate a wide variety of serious medical and surgical conditions. Thioredoxin is a small ubiquitous thiol protein with redox/inflammation modulatory properties relevant to the pathogenesis of ALI. We therefore investigated whether thioredoxin is raised extracellulary in patients with ALI and whether the extent of any increase is dependent upon the nature of the precipitating insult.
Methods: Bronchoalveolar lavage (BAL) fluid and plasma samples were collected from patients with ALI (n = 30) and healthy controls (n = 18, plasma; n = 14, BAL fluid). Lung tissue was harvested from a separate group of patients and controls (n = 10). Thioredoxin was measured by ELISA in fluids and by immunohistochemistry in tissue. Interleukin (IL)-8 levels were determined by ELISA. Disease severity was assessed as APACHE II and SOFA scores.
Results: BAL fluid levels of thioredoxin were higher in patients with ALI than in controls (median 61.6 ng/ml (IQR 34.9–132.9) v 16.0 ng/ml (IQR 8.9–25.1), p<0.0001); plasma levels were also significantly higher. When compared with controls, sections of wax embedded lung tissue from patients with ALI showed greater positive staining for thioredoxin in alveolar macrophages and type II epithelial cells. BAL fluid levels of thioredoxin correlated with IL-8 levels in BAL fluid but not with severity of illness scores or mortality. BAL fluid levels of thioredoxin, IL-8, and neutrophils were significantly greater in patients with ALI of pulmonary origin.
Conclusions: Extracellular thioredoxin levels are raised in patients with ALI, particularly of pulmonary origin, and have a significant positive association with IL-8. Extracellular thioredoxin levels could provide a useful indication of inflammation in ALI.
- ALI, acute lung injury
- ARDS, acute respiratory distress syndrome
- BAL, bronchoalveolar lavage
- IL, interleukin
- Trx, thioredoxin
- acute lung injury
- acute respiratory distress syndrome
- interleukin-8
- inflammation
- thioredoxin
Statistics from Altmetric.com
- ALI, acute lung injury
- ARDS, acute respiratory distress syndrome
- BAL, bronchoalveolar lavage
- IL, interleukin
- Trx, thioredoxin
Acute lung injury (ALI) and its extreme manifestation the acute respiratory distress syndrome (ARDS) complicate a wide variety of serious medical and surgical conditions. Mortality remains high (30–70%) and survivors frequently require extensive periods of intensive care, thereby representing a considerable clinical and fiscal burden. Underlying the defining (clinical) characteristics of ALI/ARDS (refractory hypoxemia secondary to alveolar oedema) is an intense dysregulated inflammatory response and a disruption of the reduction/oxidation (redox) balance. Indeed, increased levels of pro-inflammatory cytokines are associated with development of ALI in “at risk” populations1 and represent an adverse prognostic sign in established ARDS.2,3 Also, persistence of alveolar neutrophilia4 and oxidative modification of plasma proteins in ALI/ARDS5 predict an adverse outcome. However, despite improved understanding of the pathology, effective pharmacotherapy for ALI/ARDS has not emerged.6
The most significant improvement in survival from ALI/ARDS results from limiting the extent to which mechanical ventilation exacerbates existing lung injury.7 Moreover, the heterogeneous nature of non-pulmonary pathology that precipitates ALI/ARDS may preclude the demonstration of outcome benefit in clinical trials. Indeed, there is a growing acceptance of the theory that the extent to which the lung is directly involved in precipitating pathological changes may have an impact on predisposition to ALI/ARDS and to the clinical course of the established syndrome. Thus, evidence suggests that ALI/ARDS associated with pulmonary and non-pulmonary insults result from distinct pathophysiological processes as differences in morphology, physiology and response to treatment have been reported.8,9,10 To our knowledge, however, differences in the biochemical and inflammatory alveolar response to injury between these subgroups have not yet been described.
Thioredoxin (Trx) is a ubiquitous thiol protein originally identified in bacteria as a key enzyme involved in DNA synthesis, and has potent anti-oxidant properties. Trx also promotes cell growth, inhibits apoptosis, and modulates a number of essential inflammatory processes.11,12 Many of these effects result, in part, from the direct action of Trx on signal transduction pathways and gene expression.13 Most functions of Trx rely on its ability to transfer reducing equivalents to disulphide groups in target proteins. Trx is now known to impact on nearly all aspects of cell function in mammalian cells.14,15 As a result, the role of Trx in health and disease has become a focus of research in many disciplines. Oxidative stress and inflammation are hallmarks of conditions in which extracellular levels of Trx are increased, including viral infection, autoimmune disease, heart disease, and ischaemia-reperfusion injury.11,12 However, the role of Trx in ALI/ARDS has not yet been studied.
The aim of this study was therefore twofold: (1) to assess whether Trx levels are raised in plasma and bronchoalveolar lavage (BAL) fluid in patients with ALI/ARDS; and (2) to determine whether levels of Trx and other inflammatory markers differ depending on the nature of the precipitating insult.
METHODS
Selection of ARDS/ALI and control patients
Plasma and BAL fluid samples were collected from 30 patients fulfilling the European-American consensus criteria for ALI.16 Twenty six of these patients fulfilled the criteria for ARDS. Two separate healthy control groups were recruited for collection of plasma (n = 18) and BAL fluid (n = 14). From a second group of ALI/ARDS patients, lung biopsy (n = 2) and autopsy (n = 8) specimens were collected for examination of immunoreactive cell associated Trx. Tissue was frozen immediately at −80°C for subsequent examination. In this part of the study, patients undergoing lung resection for malignancy (n = 9), in whom lung tissue (normal appearance on microscopic examination) was sampled at a distance from the tumour area, acted as controls.
Study protocols were approved by the Royal Brompton and Harefield NHS Trust research ethics committee. Informed written consent was obtained for all control patients and assent from relatives was obtained for patients with ALI/ARDS.
Collection and storage of BAL fluid and plasma
BAL fluid and plasma were collected from patients and controls as previously described.17 Bronchoscopy was performed at the earliest possible time following diagnosis of ARDS/ALI, or immediately after admission to the AICU of the Royal Brompton Hospital for patients transferred with the established syndrome. Briefly, a flexible fibreoptic bronchoscope was wedged into the lateral section of the right middle lobe and 60 ml of 0.9% saline was instilled, allowed to settle for 5 seconds, and gently aspirated into a sterile container. This process was repeated three times (180 ml total volume) and the collected fluid pooled and immediately centrifuged (1300 g, 6 min, 4°C) to remove cell and membranous debris and stored at −80°C until analysed. Return volumes were not recorded. In keeping with the recommendations of the European Respiratory Society Task Force, measurements of non-cellular constituents were reported in concentrations per ml of recovered BAL fluid.18 The volume of BAL fluid obtained from four patients with ALI was either insufficient for analysis of all parameters or too heavily haemolysed to be used for accurate analysis. Blood samples were collected from patients on the day bronchoscopy was performed (via an indwelling arterial cannula), or from control subjects via antecubital venepuncture. Blood was collected into lithium heparin tubes and immediately centrifuged at 1300 g at 4°C for 6 minutes to separate plasma. Plasma samples were stored at −80°C.
Assessment of disease severity
Disease severity was assessed using the Acute Physiology and Chronic Health Evaluation II (APACHE II) score19 and the Sequential Organ Failure Assessment (SOFA) score.20 P:F ratios and lung injury scores (LIS) were also calculated.21 Scores were calculated using the worst physiological and biochemical parameters recorded during the 24 hour period in which bronchoscopy was performed.
Measurement of Trx and IL-8 by ELISA
Trx and IL-8 were measured in duplicate samples using sandwich ELISA kits (Redox Biosciences, Kyoto, Japan and R&D Systems, Abingdon, UK, respectively). Erythrocytes have high Trx levels relative to the amount found in plasma.22 Thus, Trx concentrations were corrected for the amount of Trx introduced by haemolysis using haemoglobin levels as an index of haemolysis. Free plasma haemoglobin was measured using a colorimetric kit (Sigma Diagnostics, Poole, UK). Plasma Trx was calculated using the following formula:
corrected plasma Trx (ng/ml) = measured Trx (ng/ml) − [0.937 × measured Hb (mg/dl)]
where 0.973 is the amount of Trx in ng/ml released from fully haemolysed erythrocytes.23 The accuracy of the haemolysis correction formula was r2 = 0.95 in 88 samples.
BAL fluid cell counts
Slide preparations for differential counting of nucleated cells in BAL fluid were made in a Shandon centrifuge using 100 μl aliquots of lavage cell suspensions adjusted to 1.5×106 cells/ml. After fixation in methanol, preparations were stained with May-Grunweld Giemsa stain as previously described.24 Differential cell counts were made from a minimum count of 300 cells and results were expressed as a proportion of total cell population. Cell counts were thus expressed for neutrophils, macrophages, lymphocytes, eosinophils, and epithelial cells.
Determination of immunoreactive cell associated Trx
To assess immunoreactive cell associated Trx, wax embedded lung sections (4 μm) mounted on positively charged slides were dewaxed in xylene, taken to water through graded alcohols, and pretreated for heat retrieval of antigen by pressure cooking at 8 psi in 0.01 M citrate buffer pH 6 for 3 minutes. Sections were cooled and stained as previously described25 using a DAKO Autostainer and the ChemMate streptavidin-biotin-HRP detection system. The primary antibody was goat anti-human Trx (ATRX-03, 1 in 500 dilution, IMCO Corp, Stockholm, Sweden). The ChemMate secondary antibody was replaced by a biotinylated rabbit anti-goat antibody (Dakocytomation, Glostrup, Denmark). Sections were counterstained with Mayer’s haematoxylin, a nuclear stain, dehydrated through graded alcohols, cleared in xylene, and permanently mounted in p-Xylene-bis(N-pyridinium bromide). In two separate experiments, irrelevant species matched antibody was substituted for the primary antibody (goat gamma globulin, Jackson Immunoresearch, West Grove, PA, USA) and anti-Trx antibody was pre-incubated for 30 minutes with a 500 M excess of Trx to saturate Trx binding sites. Specimens were assessed by a single observer blinded to the identity of the slides using a light microscope (Leitz Dialux 20). A semi-quantitative point scoring system from 0 (absence of staining) to 5 (strong staining) in 0.5 intervals was used to assess intensity of staining. Any staining was considered to be positive, although staining was present in most cells when positive. Analysis was performed by eye using an average of six fields of view at 10× magnification. Images were captured using a Zeiss AxioCam.
Statistical analysis
Data were expressed as median values and interquartile ranges and analysed using non-parametric analysis. Comparisons between groups were made using a two tailed Mann-Whitney U test and correlations between variables were assessed by use of Spearman analysis. p values of <0.05 were considered significant.
RESULTS
Patient characteristics
Of the 30 patients recruited for BAL fluid and plasma analysis, 12 were men. The median age was 33 years (IQR 26.5–49.5). In the plasma control group there were eight men and the median age was 30.5 years (IQR 28.5–36.0), and in the BAL fluid control group there were seven men and the median age was 25.5 years (IQR 24.5–38.5). There was no significant difference between the control and patient groups in terms of age and sex. The cause of ARDS/ALI was direct lung injury in 22 patients (related to pneumonia, n = 12; lung resection, n = 6; aspiration pneumonia, n = 4) and indirect lung injury in eight patients (related to non-pulmonary sepsis, n = 3; trauma, n = 3; transfusion, n = 2). The median duration of lung injury at BAL fluid sampling was 13 days for the extrapulmonary group (IQR 9–25.5) and 12 days for the pulmonary group (IQR 3.5–23). There was no significant difference between these figures (p = 0.511). The median age of the ALI/ARDS patient group used for immunocytochemistry was 52.5 years (IQR 26.0–74.5) and was not significantly different from their control group 68.0 years (IQR 50.5–76.5). The aetiologies of the lung injury in this population were pneumonia (n = 5), aspiration pneumonia (n = 1), pancreatitis (n = 1), pulmonary haemorrhage (n = 1), post-cardiopulmonary bypass (n = 1), and pneumonectomy (n = 1). Nine of the 10 patients did not survive to hospital discharge.
Thioredoxin levels in plasma and BAL fluid from healthy controls and ALI/ARDS patients
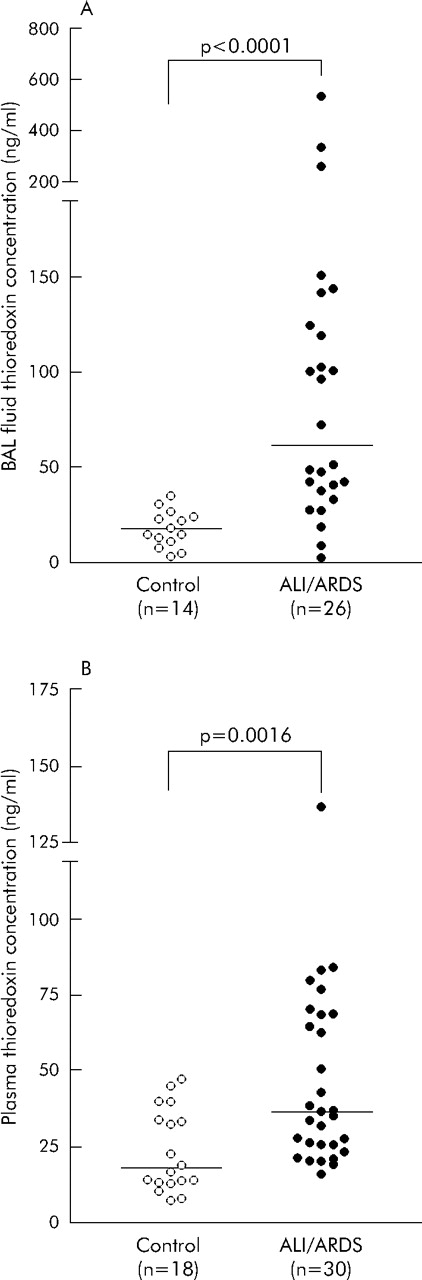
BAL fluid levels of Trx in patients with ALI/ARDS were significantly higher than in controls (61.6 ng/ml (IQR 34.9–132.9) v 16.0 ng/ml (IQR 8.9–25.1), p<0.0001; fig 1A⇓). Similarly, plasma Trx levels in patients were also significantly higher than in controls (36.1 ng/ml (IQR 24.4–68.5) v 18.0 ng/ml (IQR 13.2–36.8), p = 0.0016; fig 1B⇓). When individual patients with ALI/ARDS were considered, measured levels of Trx in BAL fluid were higher than in plasma in 73% of cases. Moreover, the median BAL fluid level of Trx in patients was significantly higher than in plasma (p<0.05). However, there was no significant correlation between plasma and BAL fluid Trx concentrations for individual patients (r = 0.341, p = 0.088), nor were there any significant differences between surviving and non-surviving patients with ALI/ARDS in Trx levels in BAL fluid (48.6 ng/ml, n = 21 and 141.4 ng/ml, n = 5; p = 0.104) or plasma (36.1 ng/ml, n = 22 and 38.3 ng/ml, n = 8; p = 0.558).
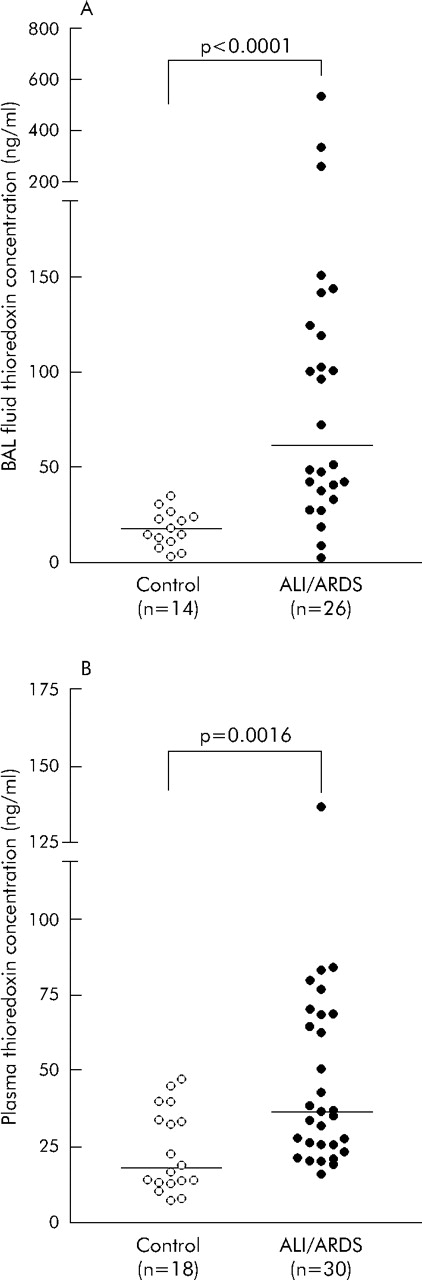
Thioredoxin concentrations in (A) bronchoalveolar lavage (BAL) fluid and (B) plasma from healthy controls (open circles) and patients with acute lung injury/acute respiratory distress syndrome (ALI/ARDS) (closed circles). Horizontal bars represent the median valued. Groups compared by Mann-Whitney U test.
Immunoreactive thioredoxin in lung specimens from patients with ALI/ARDS and controls
Scores for Trx immunostaining in different cell types are shown in table 1⇓. The intensity of staining for Trx was greater in alveolar macrophages and type II alveolar epithelial cells from patients with ALI/ARDS than from controls. Trx immunostaining was also seen in bronchial epithelial cells and interstitial macrophages, although there was no difference in the intensity of staining between ALI/ARDS and control populations. No staining of neutrophils, fibroblasts, lymphocytes, or endothelial cells was seen in specimens from either group. Representative images from a patient with ALI/ARDS and a control subject are shown in fig 2⇓. No staining in any cell type was seen when the anti-Trx antibody was substituted with the irrelevant (control) antibody. Pre-incubation of the primary antibody with soluble Trx completely abrogated staining in specimens from patients with ALI/ARDS.
Immunoreactive Trx associated with various cell types in autopsy and biopsy lung specimens from patients with ALI/ARDS and controls

Trx expression in (A) a lung tissue specimen from a representative patient with acute respiratory distress syndrome and (B) histologically normal lung tissue from a control patient. M, alveolar macrophage; P, pneumocyte; F, fibroblast; L, lymphocyte.
Interleukin-8 levels in plasma and BAL fluid from patients with ALI/ARDS and controls
IL-8 levels were significantly higher in patients than in controls in both BAL fluid (852 pg/ml (IQR 399–1488) v 22.8 pg/ml (IQR 5.9–47.0), p<0.0001; fig 3A⇓) and plasma (37.4 pg/ml (IQR 27.6–64.0) v 0.9 pg/ml (IQR 0–16.3), p<0.0001; fig 3B⇓). Moreover, there was a positive correlation between BAL fluid levels of IL-8 and Trx in patients with ALI/ARDS (p<0.001, r = 0.631) but no correlation between plasma levels of IL-8 and Trx (p = 0.347, r = 0.178). The BAL fluid correlation remained when IL-8 and Trx were corrected for total protein content before analysis (r = 0.618, p = 0.001), thereby excluding the possibility that this relationship reflected a correlation between Trx and general protein levels in the BAL fluid in patients with ARDS/ALI.

IL-8 concentrations in (A) bronchoalveolar lavage (BAL) fluid and (B) plasma from healthy controls (open circles) and patients with acute lung injury/acute respiratory distress syndrome (ALI/ARDS) (closed circles). Horizontal bars represent the median values. Groups compared by the Mann-Whitney U test.
Severity of illness
The median APACHE II, SOFA and LIS scores and also P:F ratio were calculated from data collected during the 24 hour period in which the bronchoscopy was performed. The scores were 11.0 (IQR 8.5–14.0), 5.5 (IQR 3.0–7.0), 2.4 (IQR 1.9–3.2), and 18.1 kPa (IQR 14.5 –22), respectively. In ALI/ARDS patients there was no relationship between severity of illness assessed by APACHE II score and Trx levels in either BAL fluid (r = 0.113, p = 0.553) or plasma (r = −0.153, p = 0.419). Likewise, there was no relationship between severity of illness assessed by SOFA scores and Trx levels in either BAL fluid (r = −0.145, p = 0.479) or plasma (r = 0.259, p = 0.201). Also, BAL fluid and serum levels of Trx were not correlated with LIS (r = −0.124, p = 0.702 and r = 0.225, p = 0.438, respectively) or P:F ratio (r = −0.311, p = 0.123 and r = 0.044, p = 0.817, respectively).
Thioredoxin, IL-8 levels, and neutrophil counts in direct and indirect lung injury
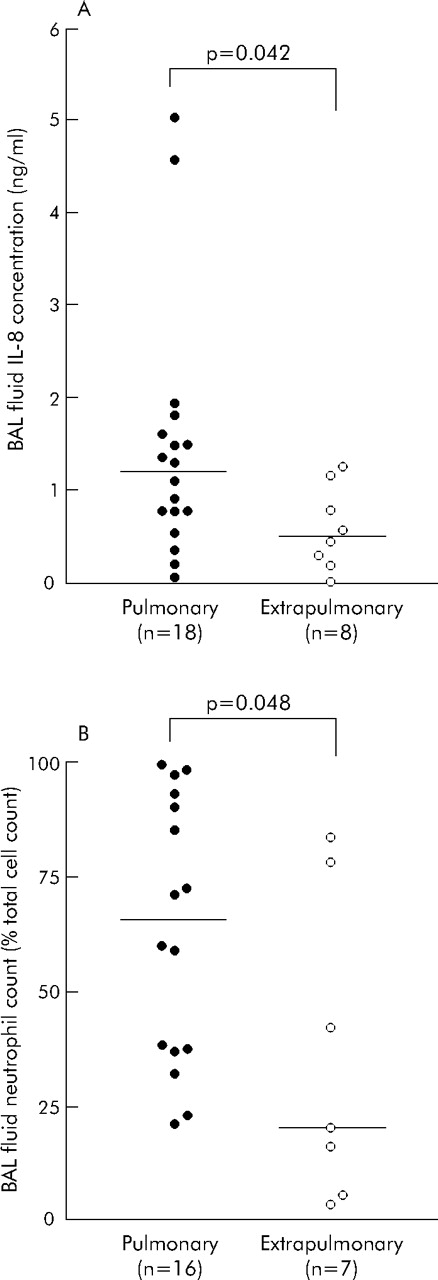
Plasma levels of Trx did not differ between patients with ALI/ARDS of direct or indirect aetiology (fig 4A⇓). By contrast, Trx concentrations were significantly higher in BAL fluid from patients with pulmonary ALI/ARDS than in those with lung injury of non-pulmonary cause (101.3 ng/ml (IQR 47.8–147.1) v 34.9 ng/ml (IQR 27.1–42.1), p = 0.0083; fig 4B⇓). There was no significant difference between BAL fluid levels of Trx in the control and non-pulmonary groups (p>0.05). IL-8 concentrations were also significantly higher in BAL fluid from patients with pulmonary ALI/ARDS than in those with non-pulmonary ALI/ARDS (1203 pg/ml (IQR 663–1710) v 513 pg/ml (IQR 252–980), p = 0.042; fig 5A⇓). Similarly, neutrophil counts in BAL fluid were higher in the pulmonary than in the non-pulmonary insult group (65.7% (IQR 37.4–91.8) v 20.3% (IQR 5.6–78.4), p = 0.048; fig 5B⇓). Finally, there was no difference between the score for severity of illness (APACHE II, SOFA) and lung injury (LIS) between the pulmonary and non-pulmonary groups (p = 0.411; p = 0.605; p = 0.518, respectively).
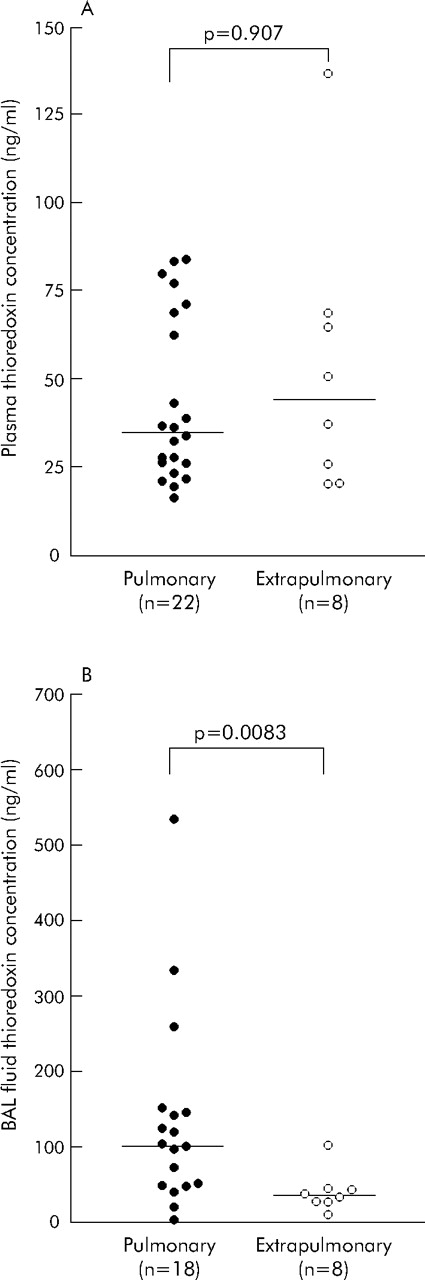
Thioredoxin concentrations in (A) plasma and (B) bronchoalveolar lavage (BAL) fluid from patients with ALI/ARDS of pulmonary aetiology (closed circles) and extrapulmonary aetiology (open circles). Horizontal bars represent median values. Groups compared by the Mann-Whitney U test.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) IL-8 concentrations and (B) neutrophil counts (as a percentage of the total cell count) in bronchoalveolar lavage (BAL) fluid from patients with ALI/ARDS of pulmonary aetiology (closed circles) and extrapulmonary aetiology (open circles). Horizontal bars represent median values. Groups compared by the Mann-Whitney U test.
DISCUSSION
Trx is a ubiquitous thiol protein, extracellular levels of which are increased under conditions of oxidxative stress and inflammation. In this study we have shown that levels of Trx are raised in BAL fluid and plasma from patients with established ALI/ARDS compared with controls. The increase in BAL fluid levels of Trx correlated with increased levels of IL-8, a cytokine implicated in the pathogenesis of ALI. When patients with ALI/ARDS were subdivided according to the aetiology of disease, BAL fluid levels of Trx were significantly higher in those with a direct (pulmonary) insult. Moreover, IL-8 levels and neutrophil counts were also highest in BAL fluid from patients with a pulmonary insult. This is the first study to report extracellular levels of Trx in ALI/ARDS, and to show significant differences depending upon the nature of the lung injury.
Patients recruited for this study had a median duration of lung injury of 12.5 days, reflecting the nature of our institution as a tertiary referral centre to which patients are transferred from other intensive care units. Despite this unavoidable limitation, all our patients still met American/European consensus guidelines for ALI/ARDS at bronchoscopy and all remained sufficiently hypoxaemic to require mechanical ventilation (median duration of ventilation until collection of BAL fluid 13 days for survivors and 11 days for non-survivors; total median duration of ventilation 50 days for survivors and 34 days for non-survivors). Moreover, their BAL fluid levels of IL-8 remained within the range described for patients with ALI/ARDS, suggesting that alveolar inflammation continued. We therefore suggest that our conclusions relating to patients with established ALI/ARDS are valid. Our choice of a control population (self-ventilating healthy adults) was largely dictated by ethical considerations as objections were raised in relation to the collection of BAL fluid from other critically ill, ventilated patients for use as control samples.
Over the last decade extracellular levels of Trx have been measured in a wide array of conditions characterised by inflammation and oxidative stress, including viral infection, autoimmune disease, heart disease, and ischaemia-reperfusion injury.11,12 These studies report raised levels in all cases. In keeping with these studies, the results presented here show raised Trx levels in BAL fluid and plasma from patients with ALI/ARDS. However, a previous study showed that serum levels of Trx measured in patients with chronic hepatitis type B were not increased compared with healthy controls.26 This finding therefore reinforces the importance of measuring changes in Trx levels in a given condition as an essential part of the investigation of its role in disease.
Previous reports of serum/plasma levels of Trx suggest that levels in healthy volunteers are in the range 20–30 ng/ml, and become elevated to about 100 ng/ml in various oxidative/inflammatory stress associated disorders.27 These findings are similar to those shown in the current study. The only other published study of BAL fluid levels of Trx reported a median level of 122.6 ng/ml in patients with pulmonary sarcoidosis.28 This compares with 61.6 ng/ml in our ALI/ARDS patients in which a similar method of BAL fluid collection was employed. However, the actual concentration of Trx in the alveolar space is likely to be considerably in excess of that measured in BAL fluid due to the dilutional effects of lavage techniques, usually calculated to be in the order of 50-fold. If correct, alveolar Trx levels in ALI/ARDS must be between 1 and 7 μg/ml. Even without considering a dilutional effect, levels of Trx were higher in BAL fluid than in plasma in most of the patients in our study. This suggests (allowing for dilution) that BAL fluid levels of Trx in patients with ALI/ARDS are approximately 100-fold greater than those in plasma. It is therefore unlikely that leakage from plasma to BAL fluid accounts for Trx levels in BAL fluid, unless a specific concentrating mechanism is involved, and suggests that the source of Trx is local to the lung.
Immunostaining with anti-Trx antibody of biopsy or autopsy tissue from patients with ALI/ARDS and controls showed strong reactivity in alveolar macrophages, type II epithelial cells, bronchial epithelial cells, and interstitial macrophages. We show, for the first time, that staining was significantly greater in alveolar macrophages and type II epithelial cells in ALI/ARDS compared with control tissue. Thus, the stronger immunoreactivity for Trx in ALI/ARDS tissue corresponds with higher levels of Trx in BAL fluid from these patients. A similar finding has been reported in patients with sarcoidosis in which tissue and BAL fluid levels of Trx were higher than in controls.28 In this study, positive staining was seen in macrophages, epithelioid cells, and Langhans’ type giant cells. Whether increased staining represents induction of expression or an increase in uptake of Trx is unclear. Assessment of cellular mRNA levels would be necessary to make this distinction and we had insufficient specimens to make this measurement.
The correlation between BAL fluid levels of Trx and IL-8 suggests a link between extracellular Trx and the inflammatory response that characterises this condition. Whether Trx and IL-8 are causally linked or whether the relationship simply reflects the intensity of the inflammatory response is unclear. The expression and release of IL-8 from a variety of primary cells and cell lines is known to be upregulated by exposure to extracellular Trx used at concentrations between 2 and 20 μg/ml.29,30 Taking into account the dilutional effects, these are achievable levels in the alveolar space.
Despite the correlation between BAL fluid concentrations of Trx and IL-8, and that between IL-8 and outcome described by others,2 we identified no relationship between Trx levels in plasma and BAL fluid and disease severity or survival. However, results concerning severity should be regarded with caution as only five deaths occurred in the study group. A study comparing serum Trx levels with disease severity in asthma also showed no significant differences among subgroups of mild and moderate asthma sufferers.31 By contrast, a study in patients with chronic heart failure showed that Trx levels increased in proportion to the severity of disease (NYHA class III > NYHA class II) and the degree of impairment of left ventricular function.32
ALI/ARDS precipitated by pulmonary and non-pulmonary insults are thought increasingly to represent distinct pathophysiological processes.8,9,10 Trx levels in BAL fluid were significantly higher in patients with pulmonary ALI/ARDS than in those with a non-pulmonary cause. Similarly, IL-8 levels and neutrophil counts were higher in patients with a direct pulmonary insult. As the median time between insult and collection of BAL fluid was the same for pulmonary and non-pulmonary groups, this is unlikely to account for the differences between the groups. Moreover, APACHE II, SOFA, and LIS scores were not significantly different between the groups, suggesting that a difference in Trx levels is unlikely to be explained simply in terms of differences in severity of injury. Instead, these differences could represent a more intense inflammatory response in the alveolar space following direct pulmonary insults. The recognition of two forms of ARDS—pulmonary and non-pulmonary—may lead to improved clinical management. Recognition of differences in disease markers may help in making this distinction.
In summary, Trx levels were raised in BAL fluid and plasma in patients with ALI/ARDS with established lung injury and BAL fluid levels were higher in those in whom the insult was direct. Levels of IL-8 and neutrophil counts were also higher. Further studies are warranted to determine whether other biochemical/cellular disease markers are significantly greater in patients with direct versus indirect lung injury, and to further elucidate the role of Trx in ALI/ARDS.
Acknowledgments
The authors thank Sharon Mumby for help with collection and storage of samples and Simon Davidson for help with haemoglobin measurements.
REFERENCES
Footnotes
Published Online First 6 April 2006
MEC received a Wellcome Trust Clinical Training Fellowship. ABG is supported by a Wellcome Trust University Award. The Dunhill Medical Trust made a financial contribution to the study.
Competing interests: none declared
Linked Articles
- Airwaves