Article Text

Abstract
Background: Asthma is a complex polygenic disease in which gene–environment interactions are important. The gene encoding tumour necrosis factor alpha (TNFα) is one of several candidate loci for asthma pathogenesis and is highly polymorphic. A number of studies have investigated the polymorphism of TNFα-308 gene promoter (substitution G→A, designated as TNF1 and TNF2) in relation to asthma susceptibility in different populations. However, the results of individual studies have been inconsistent.
Methods: To address the inconsistent findings in studies of the association of the polymorphism of TNFα-308 gene promoter with susceptibility to asthma, a systematic review was undertaken of the published data and a meta-analysis was performed. The MEDLINE database was searched for case-control studies published in English language journals from 1966 to October 2005. Data were extracted using standardised forms and pooled odds ratios (ORs) with 95% confidence intervals (CIs) were calculated.
Results: Fifteen eligible studies, comprising 2409 patients with asthma and 3266 controls, were included in the meta-analysis. Using the random effects model, the pooled result showed that the TNF2 allele is associated with overall susceptibility to asthma (OR 1.37, 95% CI 1.02 to 1.84, p = 0.04). The ORs for asthma susceptibility in TNF2 homozygote individuals were significantly increased at 2.01 (95% CI 1.26 to 3.20, p = 0.009) and 1.51 (95% CI 1.02 to 2.22, p = 0.041) compared with TNF1 homozygotes and TNF2/1 heterozygotes, respectively. In addition, the pooled OR for asthma risk in TNF2/1 heterozygotes was also significantly higher than that in TNF1/1 homozygotes (OR 1.47, 95% CI 1.01 to 2.13, p = 0.045).
Conclusions: The TNF2 allele confers a significant risk for developing asthma. A large scale case-control study is needed to clarify the functional effect of the polymorphism of the TNFα gene in the pathogenesis of asthma.
- TNFα, tumour necrosis factor alpha
- asthma
- genetics
- tumour necrosis factor
- polymorphism
- meta-analysis
Statistics from Altmetric.com
Asthma is a complex disorder characterised by airway inflammation that involves the interaction of genetic and environmental factors. The genes predisposing to asthma are likely to contain polymorphisms that modify function. Tumour necrosis factor alpha (TNFα) is a potent inflammatory cytokine whose encoding gene lies on the short arm of chromosome 6.1 The TNFα gene may influence asthma through modulation of non-specific inflammation.2 The TNFα-308 promoter polymorphism is a bi-allelic G (named TNF1 allele) to A (named TNF2 allele) polymorphism,3 and the TNF2 allele is associated with increased levels of TNFα in plasma and bronchoalveolar lavage fluid from asthmatic airways.4,5 Thus, the central role of airway inflammation in asthma and the increased levels of TNFα in asthmatic lungs suggest that functional variants of the TNFα gene could be important in this disease.
A number of studies have assessed the association between the TNFα-308 promoter polymorphism and asthma in different populations; however, the results are inconsistent and inconclusive.6–,25 Different methodologies have been used but, in particular, most of the studies used a small sample size and it is therefore not surprising that there has been a lack of replication between the various studies. By using all the available published data to increase the statistical power, it was hypothesised that a meta-analysis might allow plausible candidate genes to be excluded and causative genes to be identified with reliability. We therefore performed a meta-analysis of all of the published case-control studies to ascertain whether the polymorphisms of TNFα-308 gene promoter increased the risk of asthma.
METHODS
Study selection
The MEDLINE database was comprehensively searched (last updated search being October 2005) using PubMed and Highwire search engines. The keywords used were as follows: asthma, asthma genetics, tumour necrosis factor AND polymorphism or variant or genotype. We also manually searched the reference lists of relevant publications for additional studies.
To be included in the meta-analysis, studies had to meet the following criteria: (1) the design had to be a case-control study;(2) the outcome had to be asthma; and (3) there had to be at least two comparison groups (asthma v control groups). Participants could be of any age. Studies were excluded if one of the following existed: (1) the design was based on family or sibling pairs; (2) the genotype frequency was not reported; or (3) there was insufficient information for extraction of data.
The asthma definition used in the individual studies was accepted and we documented this in our analysis.
Data extraction and inclusion criteria
A standardised reporting form was used to abstract the data from each publication including: first author’s name, year of publication, country in which the study was conducted, ethnicity, study design, age range of study subjects, sample size, asthma definition, asthma related phenotypes, and genotyping methods used. Data were extracted independently and in duplicate by two investigators (JMG and GLS). The results were compared and disagreements were resolved by consensus.
Statistical analysis
A logistic regression model was used to assess the overall genetic effect of the TNFα-308 gene on having asthma. To examine the risk of asthma with a specific polymorphism of the TNFα-308 gene, we pooled the odds ratios (ORs) from each study weighted by the inverse of variance. A random effects model was used for the analysis which considered both within- and between-study variation.26 The effects of ethnicity on the pooled ORs were examined with the meta-regression method.27,28 Sensitivity analysis was conducted to examine whether the inclusion criteria affected the pooled ORs. We included the study by Beghe,19 which has been shown to be in Hardy-Weinberg disequilibrium (p = 0.018). We then compared the pooled ORs with the results from the main analysis.
Heterogeneity among studies was examined with the Q, H, and I2 statistics.29 A p value of <0.1 was consider significant for the Q statistic; H <1.2 suggested no heterogeneity among studies; and I2 was interpreted as the proportion of total variation contributed by between-study variation. Publication bias was examined with funnel plots and with the Begg test and Egger test.30–,32 If there is evidence of publication bias, the funnel plot is noticeably asymmetric. For the Begg and Egger test the significance level was set at 0.1. Statistical analyses were performed with SAS statistical software Version 8.2 (SAS Inc, Cary, NC, USA).
RESULTS
Characteristics of included studies
We identified 23 publications that had evaluated the association of TNFα-308 gene polymorphism with asthma. Eight studies were excluded for the following reasons: sibling paired and family based study design (n = 2),8,25 no allele or genotyping frequency (n = 3),7,14,20 and analysis of the TNFβ (lymphotoxin-α, LTα) NcoI polymorphism rather than TNFα (n = 5).33–,37
Fifteen original case-control studies, comprising 2409 patients with asthma and 3266 controls, were included in the meta-analysis (table 1⇓).6,9–13,15–19,21–,24 Seven were performed in Caucasian subjects,6,9,11–13,16,24 two in Italian subjects,18,19 four in East Asian populations,17,21–,23 one in a South Asian population,12 and two in a mixed race cohort.10,15 Four studies involved paediatric subjects alone,13,21,23,24 three included both children and adults,6,18,22 and eight recruited adults only.9–12,15–17,19 Seven studies extended their examination to the TNFα neighbouring gene lymphotoxin (LT) α variant and asthma;6,15–17,22–,24 two of these showed an association between LTα NcoI polymorphism with asthma.6,24
Characteristics of 15 publications included in meta-analysis of TNFα-308 polymorphism and asthma susceptibility
PCR based genotyping method was mentioned in each study. Four studies particularly stated that double blind genotyping was conducted.6,10,12,13
Association between TNF2 allele and asthma
Nine studies found a positive association between TNF2 and asthma (table 2⇓).6,9,10,12,15,17,21,23,24 Five studies reported a negative association,11,13,16,18,19 and one study reported a positive association between TNF1 and asthma.22 Nine of 15 publications indicated Hardy-Weinberg equilibrium in their subjects;9,11,12,16,17,21–,24 we calculated Hardy-Weinberg equilibrium for the remaining six publications and found that only the study by Beghe was in Hardy-Weinberg disequilibrium (p = 0.018).19
Association between TNF2 allele and asthma
There was a statistically significant heterogeneity among the ORs in the included studies (Q test: p<0.01; H = 1.98; I2 = 0.75). When the study by Beghe was not included, the overall pooled OR for asthma susceptibility was 1.37 (95% CI 1.02 to 1.84, p = 0.04) for TNF2 carriers compared with TNF1 carriers. When Beghe’s study was included, the overall pooled OR did not change (OR 1.36, 95% CI 1.03 to 1.79, p = 0.03; fig 1⇓).

Odds ratios for asthma comparing any TNF2 allele with TNF1 allele. (1) Pooled odds ratios excluding Beghe’s study (n = 14). (2) Pooled odds ratios including Beghe’s study (n = 15). OR, odds ratios, CI, confidence interval.
Association between genotypes of TNFα-308 and asthma
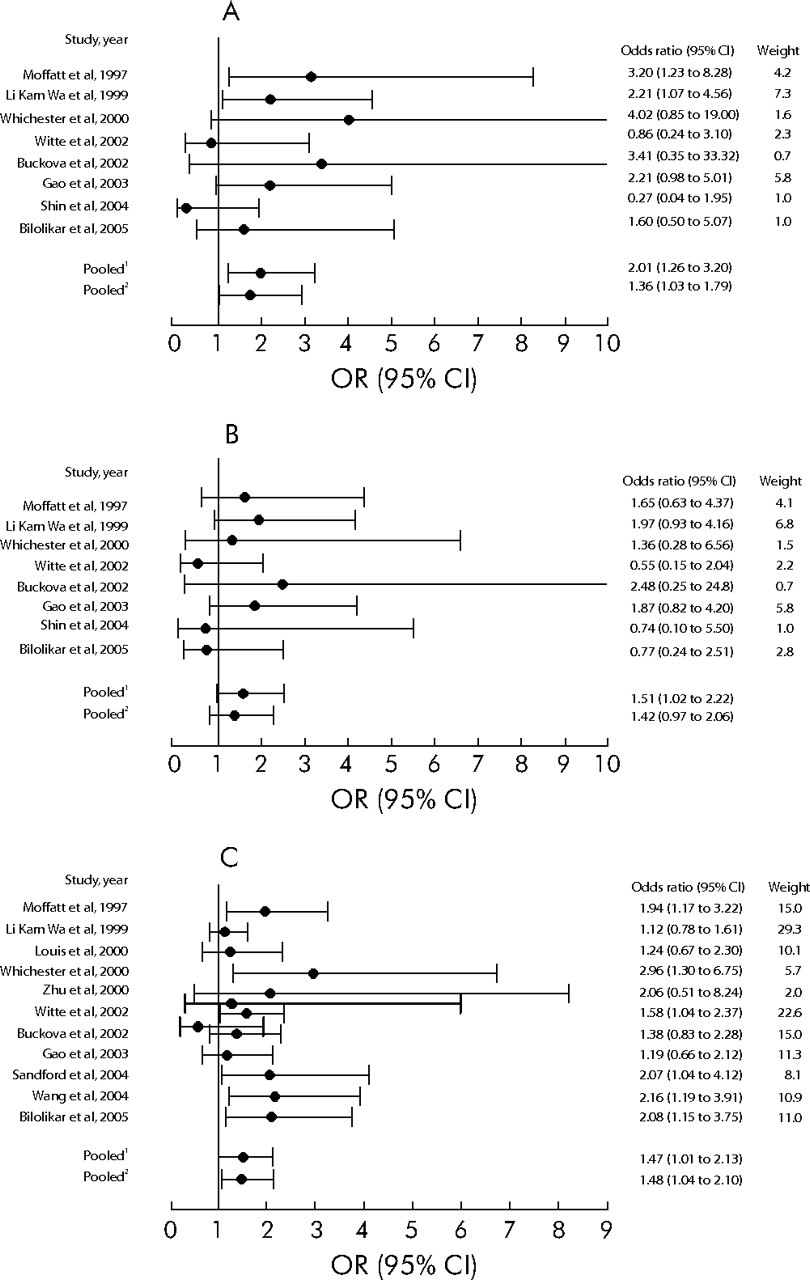
Thirteen publications reported the genotype frequency of TNFα-308 in asthmatics and controls (table 3⇓). Eight publications that observed Hardy-Weinberg equilibrium were pooled to examine the effect of TNF2/2 homozygote on asthma susceptibility. The overall genetic effect using logistic regression showed that the polymorphisms of TNFα-308 were significantly associated with a risk of having asthma (p<0.01). The pooled OR was increased at 2.01 (95% CI 1.26 to 3.20, p = 0.009) for individuals carrying the TNF2/2 homozygote compared with individuals carrying the TNF1/1 homozygote, and there was statistically significant heterogeneity among studies (Q test: p = 0.029; H = 1.53; I2 = 0.46); if Beghe’s study was included, the pooled OR was 1.74 (95% CI 1.04 to 2.93, p = 0.039; fig 2A⇓). The pooled OR was increased at 1.59 (95% CI 0.99 to 2.55, p = 0.054) for individuals carrying the TNF2/2 homozygote compared with individuals carrying the TNF2/1 heterozygote and there was no heterogeneity among publications (Q test: p>0.1; H = 1; I2 = 0); if Beghe’s study was included, the pooled OR was 1.38 (95% CI 0.83 to 2.28, p = 0.184; fig 2B⇓).
Genotype frequencies of TNF α-308 gene polymorphism in asthma and control groups
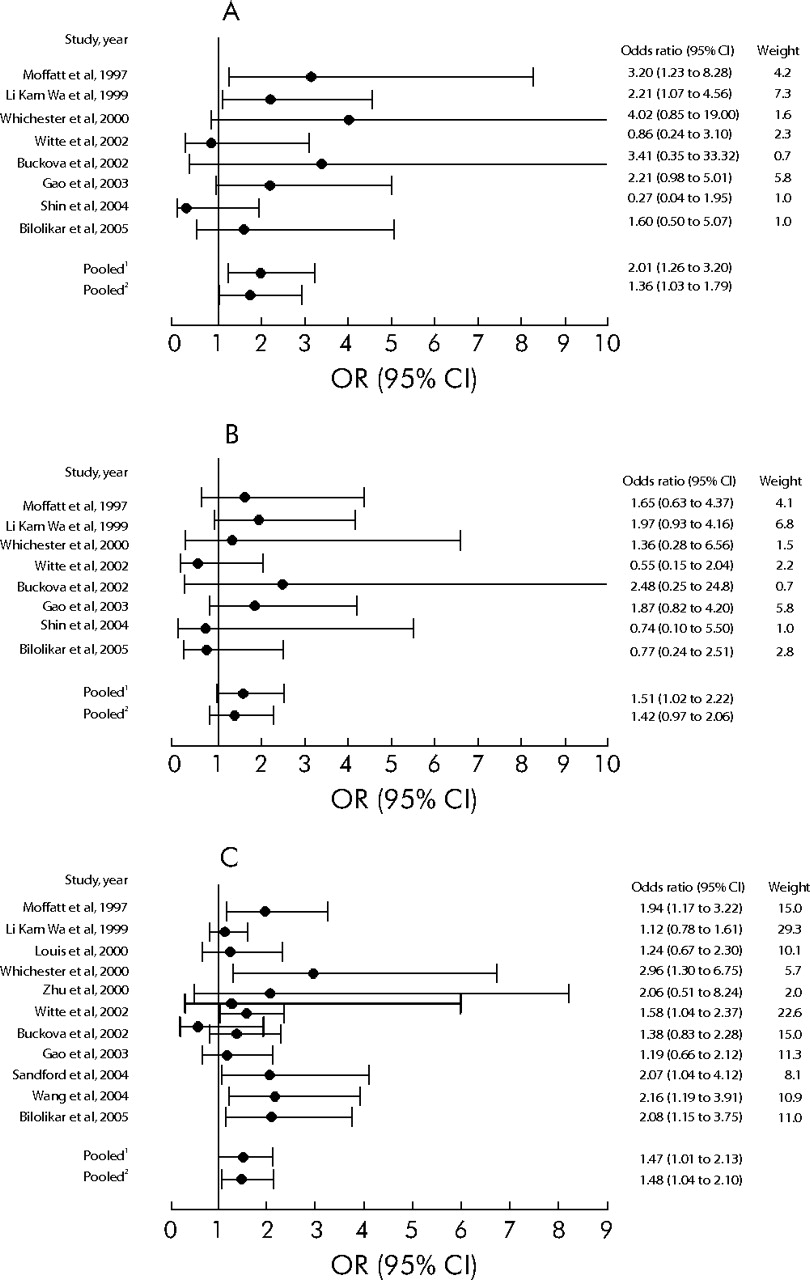
(A) Odds ratios for asthma comparing TNF2/2 homozygotes with TNF1/1 homozygotes.: (1) pooled odds ratios excluding Beghe’s study (n = 8); (2) pooled odds ratios including Beghe’s study (n = 9). (B) Odds ratios for asthma comparing TNF2/2 homozygotes with TNF2/1 heterozygotes: (1) pooled odds ratios excluding Beghe’s study (n = 8); (2) pooled odds ratios including Beghe’s study (n = 9). (C) Odds ratios for asthma comparing TNF2/1 heterozygotes with TNF1/1 homozygotes: (1) pooled odds ratios excluding Beghe’s study (n = 11); (2) pooled odds ratios including Beghe’s study (n = 12). OR, odds ratios; CI, confidence intervals.
We compared the influence of two major genotypes—namely, TNF2/1 heterozygote and TNF1/1 homozygote—on asthma in 12 publications. With the removal of Beghe’s study, the pooled OR was increased at 1.47 (95% CI 1.01 to 2.13, p = 0.045) and there was statistically significant heterogeneity among the remaining 11 publications (Q test: p<0.01; H = 1.97; I2 = 0.74). With inclusion of Beghe’s study, the pooled OR was increased at 1.48 (95% CI 1.04 to 2.10, p = 0.03) (fig 2C⇑).
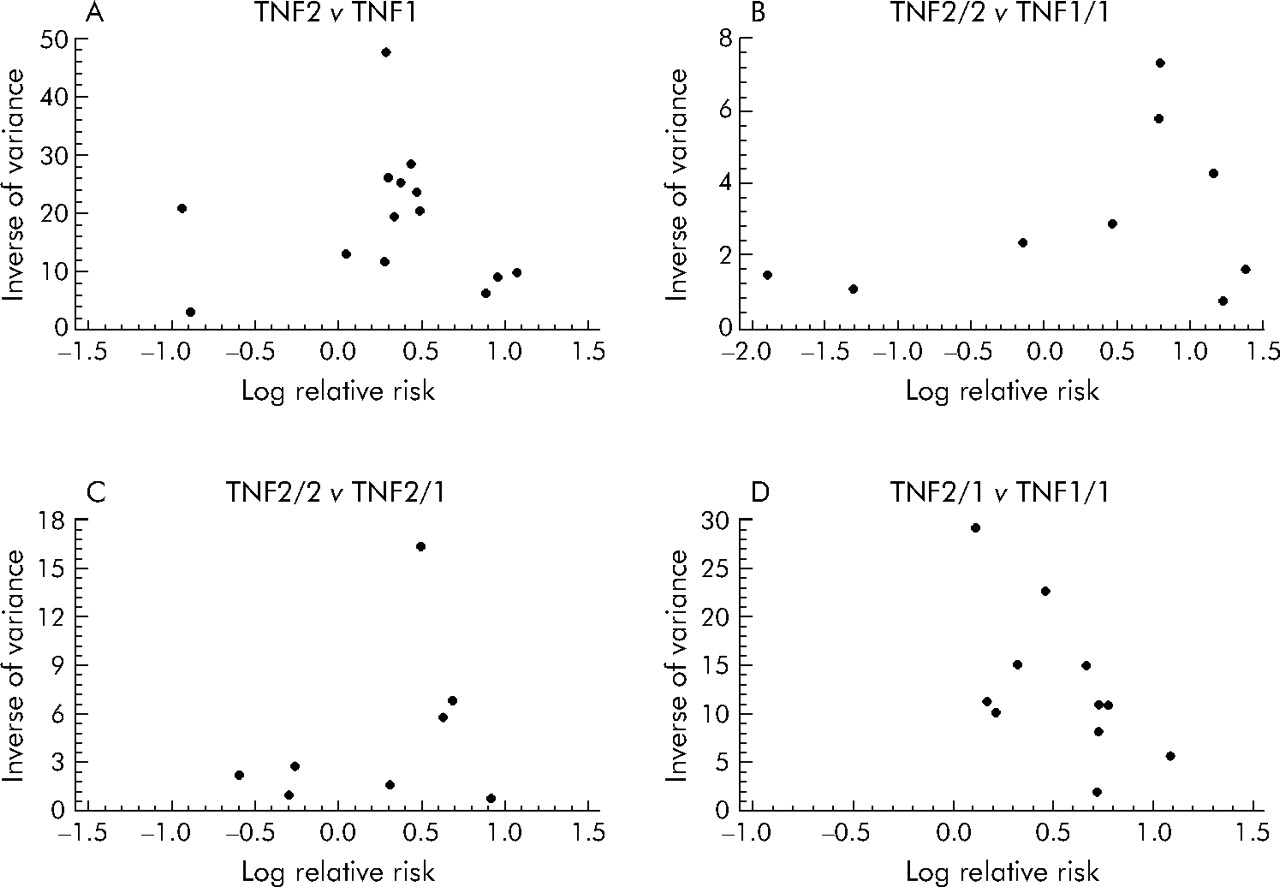
There was little evidence of publication bias; p values obtained from the Begg test and Egger test were >0.2 for all studies with the exception of the comparison between TNF2/1 heterogeneity and TNF1/1 homozygote (p = 0.04, table 4⇓). However, funnel plots (fig 3A⇓–D) showed some asymmetry, reflecting a relative absence of studies with both small numbers and larger effects for comparisons between TNF2 and TNF1 alleles, TNF2/2 homozygotes and TNF2/1 heterozygotes, and TNF2/2 homozygotes and TNF2/1 heterozygotes. Equally, the studies of comparisons between TNF 2/1 heterozygotes and TNF1/1 homozygotes had both small numbers and small or null effects.
Pooled odds ratios for TNFα-308 gene polymorphism and asthma susceptibility in meta-analyses: comparisons of alleles and genotypes
{kind=link}
{kind=link}
{kind=link}
Funnel plots of the log relative risk (for the highest possibility of asthma versus the lowest possibility of asthma) versus the inverse of variance among (A) TNF2 allele v TNF1 allele; (B) TNF 2/2 homozygote v TNF 1/1 homozygote; (C) TNF2/2 homozygote v TNF 2/1 heterozygote; and (D) TNF 2/1 heterozygote v TNF 1/1 homozygote studies.
DISCUSSION
The data from this meta-analysis clearly suggest that the TNF2 allele is a genetic contributor to overall asthma susceptibility. We observed that the TNF2/2 homozygote had a stronger association with asthma susceptibility than the TNF 2/1 heterozygote, indicating a dose response. These results suggest a possible beneficial role for the TNF1 allele versus the TNF2 allele in asthma, as well as synergy of the TNF2-TNF2 alleles. The TNF2/2 homozygote represents a greater risk factor for the development of asthma. These findings are consistent with TNFα contributing to asthma inflammation both in vitro and in vivo. This reflects a direct functional effect of the TNFα gene through its upregulation of TNFα levels in asthma.
Based on known or presumed mechanisms of disease pathophysiology, candidate gene strategies provide a useful approach for evaluating gene-disease associations. However, candidate gene case-control studies have been criticised because of a lack of replication. Some TNFα studies have found positive associations between the TNF2 allele and asthma but others have not. Several factors may be influencing these differences. Firstly, if another variant in or near the TNFα gene was the causal variant, the true association could easily be missed. Different linkage disequilibrium patterns with the functional variant may lead to variable results in different populations. It is feasible that the TNFα gene variant is playing a role in asthma in cooperation with other gene variants exhibiting a more limited biology. Previous studies have shown that there is a strong linkage disequilibrium between TNFα and LTα polymorphism (D/Dmax = 1, p<0.0001).38 A haplotype analysis by Bilolikar et al24 showed that the LTα 252A/TNF2 combination was associated with a markedly increased risk for both asthma and infant wheezing. The study by Randolph et al25 supported the suggestion that the haplotype LTα-1/LTα 4371T/TNF1/TNF1078G is associated with both asthma overall and asthmatic phenotypes. Of note, the TNFα gene is found within a 7 kb section of the informative major histocompatibility complex (MHC) class III region. Due to the close proximity of the TNF locus to HLA loci, linkage disequilibrium exists with several HLA alleles. For example, TNF2 is strongly associated with the HLA A1, B8 and DR3 alleles.39 Moreover, Moffatt et al7 found that the extended haplotype LTα-1/TNF2/HLA-DRB2 was associated with asthma (OR 6.68, p = 0.002) and even more strongly associated with bronchial hyperresponsiveness (OR 21.9, p<0.0001) in a study of over 1000 patients.
Secondly, several asthma association studies have shown inconsistent results in Caucasian versus Asian populations. This suggests that there are racial differences in genetic risk, but the current evidence is that genetic effects are usually consistent across human populations.40 Small sample size, study design flaws, population stratification, genotyping error, and other biases may be more common reasons than true racial heterogeneity for the observed discrepancies between studies of genetic risks.41 Specific environmental exposures such as smoking or allergen exposure are another confounding factor for a disease with a strong gene-environmental interaction in explaining the inconsistencies among observational studies.42,43
There are several limitations that should be considered when interpreting our results. Firstly, the pooled ORs were obtained from heterogeneous studies. Secondly, asthma itself is heterogeneous and thus the divergent inclusion criteria among patient groups might also lead to difficulties in pooling the various studies. Thirdly, our meta-analysis was restricted to English language publications. The fourth limitation is publication bias. Although significance tests did not suggest the presence of publication bias for most studies, funnel plots did not provide totally consistent results. The presence of possible bias could lead to an underestimation of the effect sizes of TNF2 allele v TNF1 allele, TNF2/2 homozygote v TNF2/1 heterozygote, and TNF 2/2 homozygote v TNF 2/1 heterozygote, but overestimation for TNF 2/1 heterozygote v TNF1/1 homozygote.
Our data suggest that the TNF2 allele may be a risk factor in the aetiology of asthma. The pooled ORs in this study—both with respect to the TNF2 allele and the TNF2/2 homozygote—suggest a modest but definite genetic effect. A larger study population needs to be assessed to help answer the question of whether or not a given genetic variant confers susceptibility to specific asthma phenotypes.44 The early identification of children at genetic risk of asthma has the potential to offer new approaches to the prevention of asthma. The involvement of particular genes will identify particular clinical courses and anticipate response to treatment.
Acknowledgments
The authors thank Dr Youming Zhang for helpful suggestions.
REFERENCES
Footnotes
Published Online First 3 March 2006
This work was in part funded by a grant from National Natural Sciences Foundation of China (No 30470767 to Jinming Gao). Jinming Gao is also supported by the Youth Fellowship from Peking Union Medical College Hospital. Philip J Thompson’s involvement in this research was supported by the CRC for Asthma and Airways.
The authors declare no financial conflict in the preparation of this manuscript.