Article Text

Abstract
Background: Asthma is a chronic inflammatory disorder of the airways driven by T cell activation. Th2 cells and their cytokines are thought to play a role in the pathophysiology of allergic as well as non-allergic asthma.
Methods: Airway cells were obtained by sputum induction from 15 healthy and 39 asthmatic individuals and the airway T cell cytokine profiles (interleukin (IL)-4, IL-5, IL-13, IL-10 and interferon (IFN)-γ) at the mRNA level were studied by real time RT-PCR.
Results: Asthma patients had increased expression of IL-5 (p = 0.001) and IL-13 (p = 0.03) mRNA in sputum compared with non-asthmatic controls. IL-4 mRNA and IFN-γ mRNA were detectable in the sputum of 44% and 21% of patients, respectively, but not in controls. Sputum IL-10 mRNA levels did not differ significantly between patients and controls. Sputum mRNA expression levels of IL-4, IL-5, and IL-13 were significantly correlated with the percentage of eosinophils and were higher in subjects with allergic asthma than in those with non-allergic asthma (p = 0.03, p = 0.02 and p = 0.0002, respectively); they did not differ between mild asthmatic subjects and those with moderate to severe asthma. In contrast, IFN-γ mRNA expression was higher in non-allergic than in allergic patients (p = 0.04) and higher in patients with moderate to severe asthma than in those with mild asthma (p<0.01). Sputum IL-5 mRNA levels (but not the other cytokine mRNA levels) were also correlated with exhaled nitric oxide (eNO) and with bronchial hyperreactivity expressed as the histamine concentration resulting in a 20% decrease in forced expiratory volume in 1 second.
Conclusion: Real time RT-PCR analysis of mRNA in induced sputum confirms a predominance of Th2 cytokines in both allergic and non-allergic asthma. IL-5 levels reflect eosinophil infiltration as well as eNO levels and hyperreactivity, and levels of the Th1 cytokine IFN-γ indicate asthma severity. The technique is a promising tool for use in further studies of asthma severity and disease activity.
- ASS, asthma symptom score
- eNO, exhaled nitric oxide
- FEV1, forced expiratory volume in 1 second
- ICS, inhaled corticosteroids
- IFN-γ, interferon γ
- IL, interleukin
- mAb, monoclonal antibody
- mRNA, messenger RNA
- PC20, histamine concentration provoking a 20% decrease in FEV1
- Th, T helper
- induced sputum
- Th1/Th2 cytokines
- asthma
- severity
Statistics from Altmetric.com
- ASS, asthma symptom score
- eNO, exhaled nitric oxide
- FEV1, forced expiratory volume in 1 second
- ICS, inhaled corticosteroids
- IFN-γ, interferon γ
- IL, interleukin
- mAb, monoclonal antibody
- mRNA, messenger RNA
- PC20, histamine concentration provoking a 20% decrease in FEV1
- Th, T helper
Asthma is histologically characterised by inflammatory cell infiltration of the bronchial mucosa, epithelial cell desquamation, globlet cell hyperplasia, and thickening of the submucosa.1 Local overproduction of T helper (Th) 2 cytokines (interleukin (IL)-4, IL-5, IL-9 and IL-13) by Th2 cells plays an important role in its pathophysiology.1,2 Although initial studies showed that interferon γ (IFN-γ), a Th1 cytokine, was able to prevent airway inflammation,2 recent studies suggest that IFN-γ may cause severe airway inflammation.3 Eosinophils recruited to the airways also produce cytokines as well as several chemokines by which they maintain or even increase the airway hyperreactivity.1,2 Furthermore, mast cells and basophils contribute to the pathogenesis of airway inflammation by the release of cytokines and chemokines, whereas epithelial cell damage can induce cytokine production by epithelial cells which, in turn, elicits the recruitment of inflammatory cells.1,2
Analysis of induced sputum is a non-invasive method to obtain viable cells from the lower airways to evaluate airway inflammation,4 and is useful for the diagnosis and monitoring of asthma.5 Sputum can be used to measure cytokines at the protein and mRNA levels.6,7 IL-5 mRNA was detected in sputum by a semi-quantitative RT-PCR technique in more subjects with asthma than in atopic non-asthmatic subjects or healthy controls.7 The number of IL-4 and IL-5 mRNA expressing CD3+ cells detected by in situ hybridisation in cytospins of induced sputum was higher in asthmatic subjects than in healthy controls.8 More recently, quantitative RT-PCR techniques have been developed to measure cytokine production in cell cultures and/or tissues.9
We therefore combined the technique of sputum induction and quantitative real time RT-PCR to study differences in the expression of an extensive panel of T cell cytokines in the airways of healthy controls and asthmatic subjects. We further tried to define differences in cytokine mRNA expression in the airways of subjects with allergic or non-allergic asthma and those with mild or moderate to severe asthma, and to correlate mRNA expression with other parameters regularly used to study inflammatory activity (such as exhaled nitric oxide (eNO) and the histamine concentration provoking a 20% decrease in FEV1 (PC20)).
METHODS
Subjects
This study was performed between September 2002 and August 2004 (except for April, May and June which is the tree and grass pollen season). Patients attended the outpatient clinic of either the Pneumology Department or the Allergy Department of our University Hospital. A diagnosis of asthma was based on previous or current proof of reversibility of FEV1 ⩾12% after inhalation of salbuterol. Healthy volunteers were recruited from university students and co-workers.
Thirty nine asthmatic subjects (16 women, 23 men) who were not taking systemic steroids and 15 healthy controls (8 women, 7 men) aged 18–65 years were recruited. There were no significant differences in age distribution between patients and controls (p = 0.2 for women and p = 0.07 for men). Thirty two of the 39 asthmatic subjects were non-smokers, two were occasional smokers (less than three cigarettes a day), one smoked regularly (20 or more cigarettes a day), and no data were available on the smoking habits of four. All the healthy controls were non-smokers. Five of the controls had a clinical history suggestive of allergic rhinoconjunctivitis in the grass pollen season and had specific IgE antibodies to grass pollen but not to any of the other allergens tested (house dust mite, cat, dog, tree and weed pollen, and moulds). Two others had a history of oral symptoms on contact with a food allergen and specific IgE antibodies to hazelnut (n = 1) and tomato (n = 1) but not to the other allergens tested.
Disease activity was evaluated using asthma symptom scores (ASS)10 and validated Dutch translated Juniper scores.11 Bronchial hyperresponsiveness was quantified as the PC20 (n = 25) and eNO was measured online based on the old ERS guidelines with Ecophysics CLD 700 AL MED (Dürnten, Switzerland) (n = 16).10 Healthy controls had normal spirometric parameters, no clinical symptoms of upper or lower airway disease, an ASS of zero, and did not or had not used any anti-asthma medication in the previous 5 years.
The study was approved by the local ethical committee of the Faculty of Medicine, Leuven. Informed consent was obtained from all study subjects.
Sputum induction
Sputum was induced with an aerosol of inhaled hypertonic saline in concentrations of 3%, 4% and 5% for 7 minutes (unless a fall in FEV1 of >10% occurred in which case the procedure was stopped) generated by a De Vilbiss nebuliser (Ultra-Neb 2000 model 200HI) after pretreatment with 400 μg inhaled salbutamol.
Sputum examination
Sputum was processed by a modification of the technique described by Pizzichini et al.4 All portions that appeared free of salivary contamination were selected to minimise the possibility that cells were obtained from different airway compartments and to limit squamous cell contamination. A volume of Hanks’ balanced salt solution containing 0.1% ditriothreitol (Sigma, St Louis, MO, USA) and 3% bovine serum albumin (Sigma) of four times the weight was added. Portions were agitated with a vortex, placed on a bench rocker for 5 minutes, filtered through a 70 μm Falcon cell strainer, and centrifuged at 1500 rpm for 10 minutes. The cell pellet was resuspended in 1000 μl RPMI 1640 (Bio Whittaker Europe, Cambrex) containing 2 mM l-glutamine, penicillin (100 U/ml), streptomycin (100 μg/ml) (Bio Whittaker Europe), and 10% bovine calf serum (BCS; Hyclone, Logan, UT, USA). Trypan blue was used to evaluate the percentage of dead cells (Bio Whittaker Europe) in a Bürker chamber.
Differential cell count
Cytospins were prepared from 32 of 39 patient samples and 11 control samples. The cell suspension was adjusted to 1.0×106 cells/ml and 50 000 cells were placed in a Shandon 3 cytocentrifuge (Techgen, Zellik, Belgium). The cytospins were air dried and stained using May-Grünwald-Giemsa stain.
Quantitative cytokine mRNA
RNA could be isolated from 34 of the 39 patient sputum samples and 11 control samples with the Qiagen Mini Rneasy kit (Maryland, USA). Differential cell counts and cytokine mRNA could be measured in 27 of the patients. RNA was transcribed to cDNA with the Ready-to-go T-primed First Strand Kit (Amersham Pharmacia Biotech, Uppsala, Sweden). Real time quantitative RT-PCR was performed for IL-4, IL-5, IL-13, IL-10, IFN-γ, and β-actin in the ABI prism 7700 Sequence Detector System (Applied Biosystems, Foster City, CA, USA) as described.9 The primer and probe sequences for IL-4, IL-10, and IFN-γ have been previously published.9 The primer and probe sequences for IL-5 and IL-13 were designed with the computer program Primer Express (Applied Biosystems) and are shown in table 1.
Primer and probe sequences of IL-5 and IL-13
PCR amplifications were performed in a total volume of 25 μl containing 5 μL cDNA, 12.5 μL Universal PCR Master Mix, no AmpErase UNG (Applied Biosystems), 100–300 nM concentrations of each primer, and 200 nM concentrations of the corresponding detection probe (Applied Biosystems or Eurogentec, Belgium). Each PCR amplification was performed in duplicate wells under the following conditions: 94°C for 10 minutes followed by 40 cycles at 94°C for 15 seconds and 60°C for 1 minute. cDNA plasmid standards, consisting of purified plasmid DNA specific for each individual target, were used to quantify the target gene in the unknown samples, as described elsewhere.9 All results were normalised to β-actin to compensate for differences in the amount of cDNA.
Data analysis
Statistical analyses were performed using GraphPad Prism (GraphPad Software Inc, San Diego, USA) using the two tailed Mann-Whitney U test. The one tailed Mann-Whitney U test was only used to test differences between allergic and non-allergic subjects. The Kruskall-Wallis test was used to study differences between three or more groups and Dunn’s multiple comparison test was used as post-test. Normality was analysed with the Kolmogorov-Smirnov test. Correlations were studied by the Spearman non-parametric test or Pearson test where appropriate. Contingency tables were analysed using the Fisher’s exact test. A difference was considered to be significant when p⩽0.05.
RESULTS
Patient characteristics
Table 2 shows the characteristics of the patients and medication use. Asthma severity was scored on the basis of the Global Initiative for Asthma (GINA) criteria.12 Patients with mild intermittent asthma (n = 11) and mild persistent asthma (n = 12) were grouped as mild asthmatics, and moderate (n = 8) and severe (n = 8) asthmatics were grouped as moderate to severe asthmatics. Patients were allowed to continue their usual treatment. Thirteen patients regularly used inhaled corticosteroids (ICS): <500 µg/day beclomethasone dipropionate (BDP) or equivalent (n = 1), 500–1000 µg/day BDP or equivalent (n = 5), and >1000 µg/day BDP or equivalent (n = 7); “non-users” either had never used ICS or had not used them for at least 3 months. A significantly larger proportion of patients with moderate to severe asthma used ICS than patients with mild asthma (p<0.0001, Fisher’s exact test).
Patient characteristics
Twenty one asthmatic subjects were classified as allergic according to the presence of serum specific IgE antibodies for house dust mite (n = 19), pets (n = 12), moulds (n = 2), and/or grass or tree pollen (n = 17) and a clinical history suggestive of allergic responses to those allergens (analysis was not performed in one patient; none of the patients had specific IgE to weed pollen). No differences in FEV1% (p = 0.48, Fisher’s exact test), asthma severity (GINA classification; p = 0.49, Fisher’s exact test), and ICS use (p = 0.28, Fisher’s exact test) were found between allergic and non-allergic asthmatic subjects.
Comparison of Th1/Th2 cytokine mRNA levels in induced sputum from asthmatic patients and healthy controls
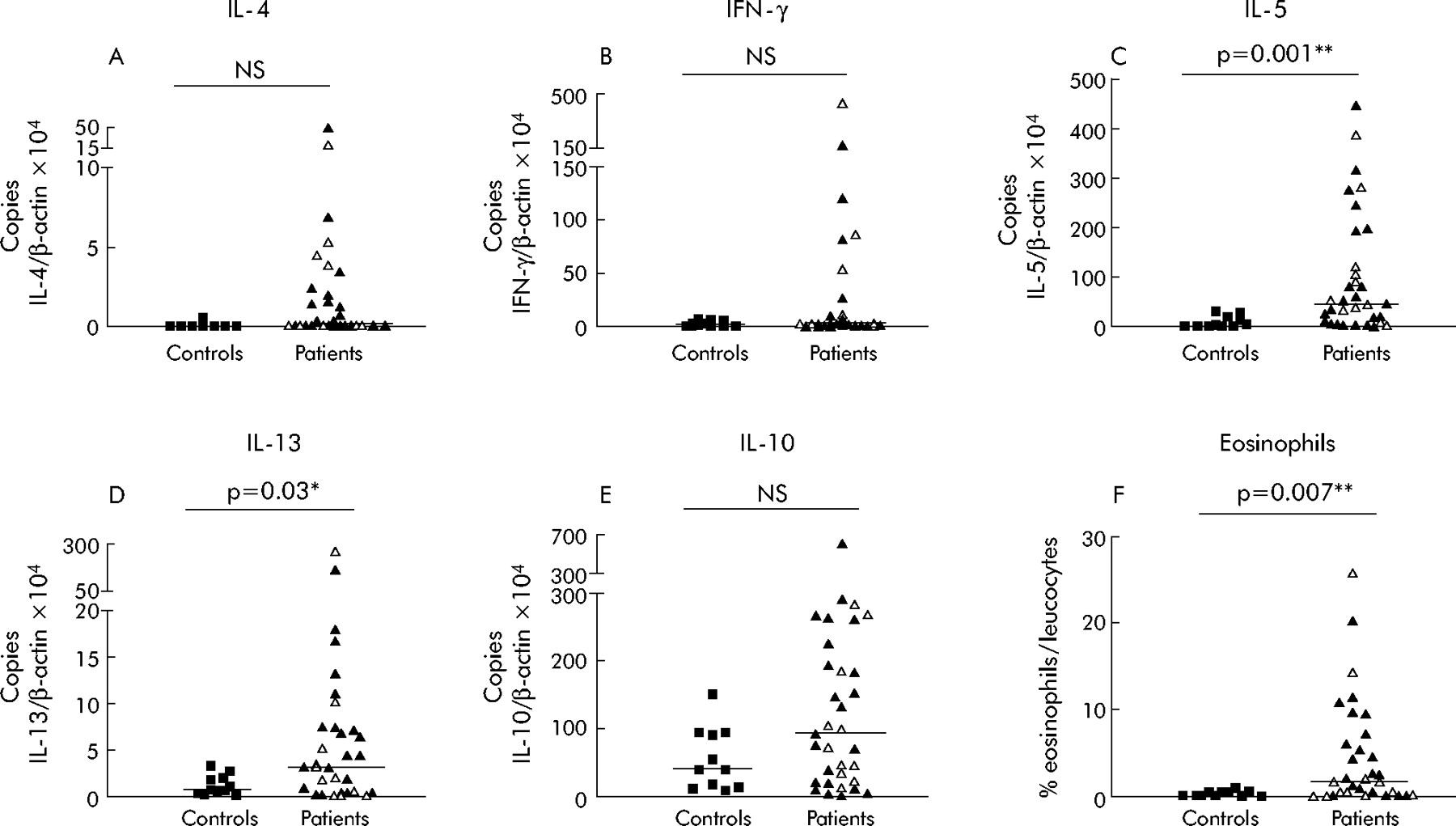
mRNA was extracted from the samples of induced sputum, transcribed to cDNA, and real time RT-PCR was performed. All values were normalised to β-actin mRNA in order to compensate for variations in cell numbers and RNA quantity between the samples. IL-4 and IFN-γ were selected as the typical representatives of Th2 and Th1 cytokines, respectively. None of the healthy volunteers had values of IL-4 mRNA above 1 or IFN-γ mRNA above 10, while 44% and 21%, respectively, of the patients had values above these cut off points (fig 1A, B). This resulted in a significant difference for IL-4 between controls and asthmatics (cut off copies IL-4/β-actin ×104⩾1: p = 0.02; cut off copies IFN-γ/β-actin ×104⩾10: p = 0.07, Fisher’s exact test). A significant correlation was found in the asthmatic patients between sputum IL-4 and IFN-γ mRNA levels (p = 0.03; Spearman r = 0.387, data not shown). All the patients except one with increased sputum IFN-γ mRNA levels also had increased sputum IL-4 mRNA levels, indicating that both Th2 and Th1 cytokines might simultaneously be increased in the airways of asthmatic patients. With regard to the other Th2 cytokines, there was a significantly higher expression of IL-5 and IL-13 mRNA in the sputum of patients than in healthy controls (fig 1C, D). IL-5 and IL-13 mRNA levels correlated significantly with each other (p = 0.0001, r = 0.6162), while no correlation was found between IL-4 and either IL-5 or IL-13 mRNA (p = 0.18, r = 0.234 and p = 0.74, r = 0.06, respectively). IL-10 mRNA levels in sputum were similar in healthy controls and asthmatics (fig 1E).

Eosinophils and cytokine mRNA levels in induced sputum: comparison between healthy controls and asthmatics. Cells were isolated from induced sputum of 11 healthy controls and 33 asthmatic patients. RNA was extracted and 1 μg RNA was transcribed to cDNA which was used in duplicate to perform real time RT-PCR using AB Universal Mastermix with either β-actin (A–E) or cytokine (A) IL-4, (B) IFN-γ, (C) IL-5, (D) IL-13, or (E) IL-10 specific primers and VIC-(β-actin) or FAM-(cytokines) labelled specific probes. The results were quantified using a cDNA plasmid standard (A–E). Cytospins were prepared, stained with May-Grünwald-Giemsa, and the percentage of eosinophils in the leucocytes was counted (F). Open symbols represent patients treated with inhaled corticosteroids, closed symbols represent patients without inhaled corticosteroid treatment. Comparisons were performed using the two tailed Mann-Whitney U test as parameters did not pass the normality test. The median is indicated with a horizontal line. NS = not significant.
IL-4, IFN-γ, IL-5, IL-13, and IL-10 sputum mRNA levels did not differ significantly between steroid naïve and steroid treated patients (open and closed symbols in the patient groups in fig 1).
Correlation of eosinophil count with cytokine mRNA levels in asthmatic patients
Inflammatory cell subtypes were counted in cytospins from 11 healthy controls and 32 asthmatic subjects. A significantly higher percentage of sputum eosinophils was found in asthmatic subjects than in healthy controls (fig 1F). In approximately half the patients only a few or no eosinophils were found; most of them were treated with ICS. No differences between patients and controls were found in the percentage of lymphocytes and macrophages (data not shown). The cytokine mRNA levels in induced sputum were compared with the percentage of sputum eosinophils. As indicated in fig 2, the levels of IL-5 as well as IL-4 and IL-13 mRNA correlated significantly with the percentage of airway eosinophils. IL-5 and IL-13 (but not IL-4) mRNA levels also correlated with airway eosinophils in steroid naïve patients (fig 2A–C), but these correlations were not found in those treated with steroids (open symbols).
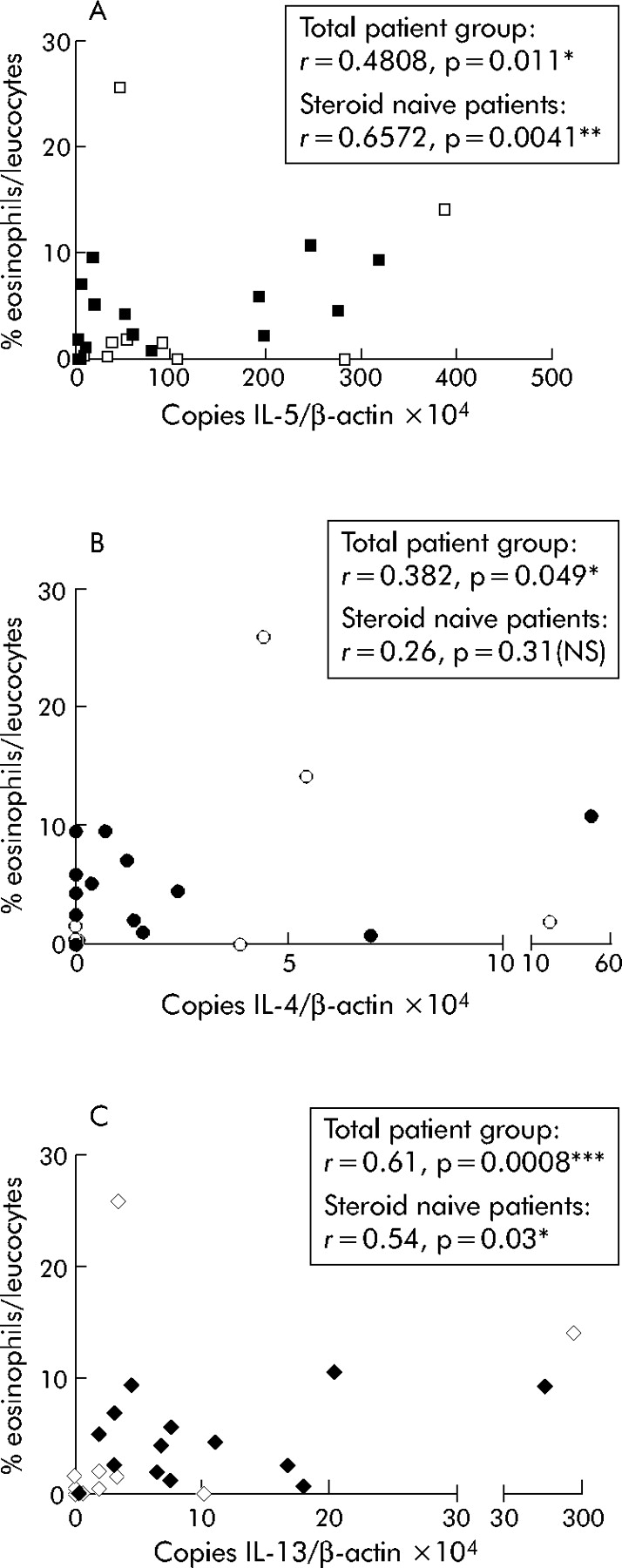
Correlation of sputum cytokine mRNA levels with sputum eosinophil count. Analysis of cells and cytokine mRNA from induced sputum were performed in parallel in 27 asthmatic patients. Cytokine mRNA levels and eosinophil counts were determined as explained in fig 1. Open symbols represent patients treated with inhaled corticosteroids and closed symbols represent patients who were not treated with inhaled corticosteroids. Spearman non-parametric correlation studies were performed as parameters did not pass a normality test. NS = not significant.
Differences in cytokine and chemokine patterns between allergic and non-allergic asthmatics
We further compared the sputum mRNA pattern in allergic and non-allergic asthma. Two asthmatic individuals who were allergic to grass pollen only were excluded from the comparison as asthma symptoms outside the pollen season in those patients were probably not related to their allergy. A significantly higher percentage of eosinophils was found in the sputum of patients with allergic asthma than in those with non-allergic asthma (table 3). Patients with allergic asthma had significantly higher sputum IL-4, IL-5 and IL-13 mRNA levels than non-allergic asthmatic patients. IFN-γ levels, on the other hand, were significantly higher in the non-allergic group (table 3). When compared with control subjects, sputum IL-4 and IL-13 mRNA levels were significantly raised in allergic individuals only (p = 0.03 and p = 0.0001, respectively) and not in non-allergic individuals (p = 0.4 and p = 0.3, respectively) (data not shown), while IFN-γ levels were significantly increased in non-allergic asthmatic subjects and not in those with allergic asthma (p = 0.05 and p = 0.6, respectively). Sputum IL-5 mRNA levels differed significantly from control levels in both allergic and non-allergic patients (p = 0.0001 and p = 0.03, respectively). Sputum IL-10 mRNA levels did not differ significantly between the two groups (table 3), with comparable levels to those in controls for both groups.
Comparison of airway eosinophil count and cytokine pattern between allergic and non-allergic asthmatics†
Correlation of cytokine mRNA levels in induced sputum with exhaled NO, airway hyperresponsiveness, FEV1, and asthma severity
To determine whether cytokine mRNA levels could reflect airway inflammation, eNO levels were compared with sputum cytokine mRNA expression. As shown in fig 3A, there was a significant correlation between eNO levels and sputum IL-5 mRNA levels but no correlation was found between eNO levels and IFN-γ, IL-13, IL-4, or IL-10 mRNA. We also found that eosinophil levels correlated significantly with eNO levels in a subgroup of 16 patients (data not shown).

(A) Correlation of cytokine mRNA levels with exhaled NO (eNO) levels in 13 patients and (B) airway hyperreactivity to histamine expressed as log PC20 (in mg/ml) in 21 asthmatic patients. Cells were isolated from induced sputum of asthmatic patients and IL-5 mRNA levels were determined as explained in fig 1. Open symbols represent patients treated with inhaled corticosteroids and closed symbols represent patients without inhaled corticosteroid treatment. All parameters passed a normality test and Pearson linear correlation studies were performed. NS = not significant.
To study whether sputum cytokine mRNA levels reflect airway hyperresponsiveness, the log PC20 values were correlated with sputum cytokine mRNA levels in a subgroup of 25 patients. As indicated in fig 3B, there was a significant inverse correlation between IL-5 mRNA levels and log PC20. The correlation was even stronger in steroid naïve patients (fig 3B). Thus, high sputum IL-5 mRNA levels correlate with increased airway hyperresponsiveness. In steroid naïve patients we also confirmed a significant correlation between airway hyperresponsiveness (PC20) and eNO levels (r = −0.82, p = 0.007; data not shown),10 and also between PC20 and eosinophil counts (r = −0.68, p = 0.004; data not shown). There was no correlation between sputum IFN-γ, IL-4, IL-13 or IL-10 mRNA levels and PC20 in the total patient group or in the different subgroups in relation to their treatment (data not shown).
The validated Dutch translated Juniper scores11 measuring asthma symptoms and the ASS commonly used in our hospital10 significantly correlated with each other in 21 patients interviewed for both (p = 0.0005, r = 0.694; data not shown). ASS were obtained at the time of sputum induction in nearly all patients. No correlation was found between the ASS and sputum levels of IL-4, IL-5, IL-10, IL-13 or IFN-γ mRNA in the total patient group or in the steroid naive group (data not shown).
Correlation between cytokine mRNA levels in induced sputum and asthma severity based on GINA criteria
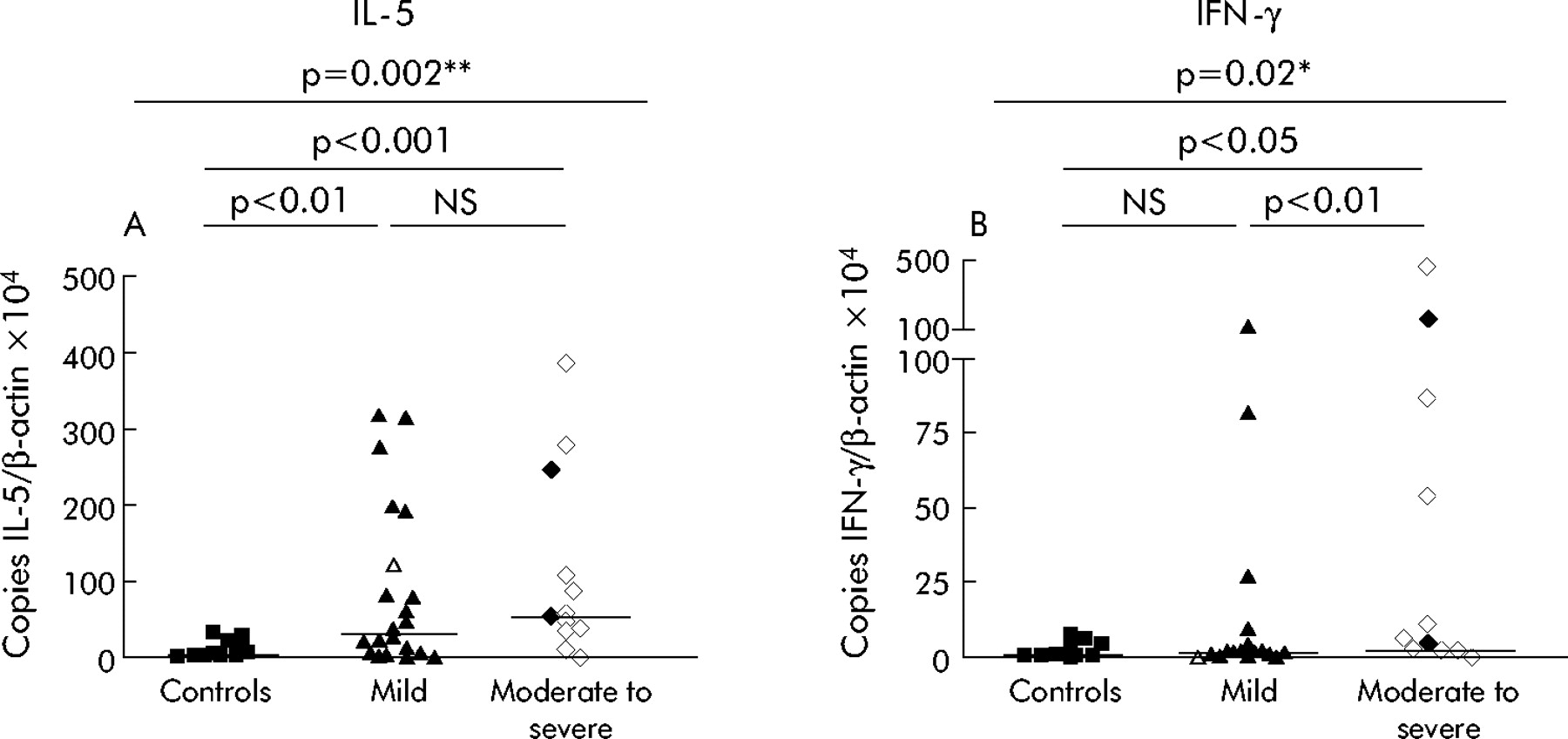
Differences between asthmatic subjects classified according to the revised GINA criteria of severity12 were examined by comparing sputum cytokine mRNA patterns in these patient groups. The Kruskall-Wallis test revealed no significant differences in IL-4, IL-10 or IL-13 mRNA levels between the groups (data not shown). IL-5 mRNA levels were increased to a similar extent in mild asthmatics and in those with moderate to severe asthma (fig 4A). Sputum IFN-γ mRNA levels, on the other hand, were significantly increased in moderate to severe asthmatics to levels above those in healthy controls and patients with mild asthma (fig 4B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cytokine mRNA levels in the different groups classified according to asthma severity. Cells were isolated from induced sputum of asthmatic patients (n = 34) and patients were classified following the revised GINA criteria.12 Mild intermittent and mild persistent asthmatics were grouped together as “mild” and moderate and severe persistent asthmatics were also grouped together as “moderate to severe” asthmatics. Cytokine mRNA levels were determined as explained in fig 1. Open symbols represent patients treated with inhaled corticosteroids, closed symbols represent patients without inhaled corticosteroid treatment. The Kruskall-Wallis non-parametric test with Dunn’s multiple comparison test as post test was used as parameters did not pass a normality test. The median is indicated with a horizontal line. NS = not significant.
DISCUSSION
In this study we have used induced sputum to analyse the cells and cytokines in the airways of asthmatic patients and healthy controls. Compared with biopsy specimens and bronchoalveolar lavage fluid obtained by bronchoscopy, induced sputum has the advantage of being a non-invasive, easy, and well tolerated technique. We combined the technique of sputum induction with real time RT-PCR, a technique that has recently been developed to quantify cytokine mRNA levels in research settings. We were able to show that mRNA levels for several cytokines differ between allergic and non-allergic asthma patients and that some correlate with disease activity and severity.
Sputum IL-4 mRNA was only detectable in asthmatics (detected in 44% of the patients) and never in healthy controls. Increased IFN-γ mRNA levels (present in 21% of the patients only) were also found only in asthmatic subjects, which is consistent with recent findings by other authors.13 When patients were classified according to the revised GINA criteria,12 the increase in sputum IFN-γ levels occurred predominantly in those with moderate to severe asthma. IFN-γ is a classical Th1 cytokine. Impaired Th1 function was initially proposed as the underlying factor in atopy and/or asthma. Most individuals with increased IFN-γ mRNA levels, however, also had increased IL-4 mRNA levels and there was a significant correlation between IL-4 and IFN-γ levels. Thus, both Th1 and Th2 cytokines can be increased in parallel in the airways and both might contribute to disease development. We furthermore found significantly higher sputum expression of IL-5 and IL-13 mRNA in asthmatic subjects, and IL-5 and IL-13 mRNA levels correlated significantly with each other. Increased IL-5 and IL-13 mRNA levels have also been found by others in bronchial biopsies14,15 and in cells obtained by induced sputum from asthmatic patients.8 Increased IL-5 and IL-13 protein levels have been found in induced sputum from asthmatics.16,17 Komai-Koma et al reported that IL-13 production was downregulated in corticosteroid treated patients.17
Importantly, we found that allergic and non-allergic asthmatics appear to have slight differences in airway inflammation. It is debatable whether or not allergic and non-allergic asthma are distinct inflammatory diseases.18 Some authors state that even non-allergic asthma might be caused by inhalation of a known or unknown allergen or, in contrast, that the allergic status is associated with but not required for asthma development.18–20 Others have stressed the differences between allergic and non-allergic asthma.21 We found a higher percentage of eosinophils in patients with allergic asthma than in non-allergic subjects. Amin et al22 also found higher numbers of eosinophils in allergic patients than in non-allergic patients. Our results are also in accordance with results from an epidemiological study in which atopic subjects with bronchial hyperreactivity were found to have higher levels of serum eosinophilic cationic protein (ECP) and a higher number of blood eosinophils than non-atopic subjects with bronchial hyperreactivity.23 However, not all studies are in agreement on this, and other authors have reported a similar increase in the number of eosinophils in allergic and non-allergic asthmatics.18,24
Our results show significantly higher IL-4, IL-5 and IL-13 mRNA expression in induced sputum from patients with allergic asthma than non-allergic asthmatics, whereas non-allergic subjects had higher IFN-γ mRNA levels. Compared with control subjects, IL-4 and IL-13 mRNA levels were increased in the allergic patient group only, while IFN-γ levels were increased in the non-allergic group. Dysregulation of IL-4 production25 or a change in IL-4 responsiveness26 have been suggested as basic underlying abnormalities in atopy. In allergic asthma the number of IL-4 mRNA copies detected in bronchial biopsies correlated with the serum IgE levels.27 This indirectly suggested that allergic patients should, indeed, have higher IL-4 mRNA levels in the airways. However, the same authors did not find any differences in IL-4 mRNA levels between allergic and non-allergic asthmatics.19 Our study is the first to show such a difference and confirms that there are—besides the many similarities—also quantitative differences in the cellular and cytokine profiles between allergic and non-allergic asthmatics.
Another issue is whether sputum cytokines could be helpful in evaluating disease severity, symptom control, and in monitoring treatment. We found that IL-5, IL-4, and IL-13 mRNA levels were significantly correlated with the percentage of airway eosinophils, and the latter is known to correlate with airway inflammation in steroid naïve patients.5 We found that bronchial hyperresponsiveness (measured by histamine provocation) and eNO levels (which reflect airway inflammation28) were significantly correlated with the IL-5 mRNA level but not with other cytokines in steroid naïve patients. This indicates that, in steroid naïve patients, those with increased airway hyperreactivity and those with more active disease have higher IL-5 mRNA levels. Similarly, Humbert et al27 found that the level of IL-5 mRNA expression in bronchial biopsies from patients with asthma was inversely correlated with their FEV1 value, also leading to the conclusion that IL-5 levels are higher in patients with more severe asthma. Exhaled NO levels in patients with steroid naïve asthma have been shown to correlate with their eosinophil count and airway hyperresponsiveness.10,29 It is therefore not surprising that we also found a correlation between IL-5 mRNA levels and eNO in steroid naïve patients. In our study, sputum IL-5 mRNA levels were also increased in the subgroup of steroid treated asthma patients, which makes the quantification of IL-5 mRNA levels a possible means of evaluating residual airway inflammation in steroid treated patients even if eosinophils are no longer present in the airways. This might be used to help to adapt the treatment protocol, but further studies are required. A similar finding regarding serum IL-5 levels in patients treated with corticosteroids has recently been reported by Joseph et al.30 However, we should stress that the method of sputum induction fails in some patients and the quantification of cytokine mRNA from the samples is time and money consuming. It could therefore perhaps be reserved for use in difficult to treat asthma patients only. It also needs to be borne in mind that cytokine mRNA levels correlated poorly with asthma symptoms as measured by ASS and Juniper score. An intriguingly high proportion of patients had a high ASS but only low cytokine mRNA levels. We can only speculate that symptoms reported by patients might persist, even if the inflammation is less prominent, or that the inflammation in patients with high ASS and low cytokine mRNA expression has different characteristics. Another explanation could be that the ASS correlates with airway hyperreactivity which could be dissociated from airway inflammation.31
Because we studied cytokine mRNA expression in induced sputum, we were not able to determine the cellular source of these cytokines. Cytokines are produced by several cell types besides T cells. Cho et al13 have shown by intracellular staining that sputum CD4+ and CD8+ cells producing IL-4, IL-5 and IFN-γ are increased in asthmatic airways. Eosinophils were shown to be the main cell type expressing IL-4 and IL-5 mRNA in the nasal mucosa upon allergen challenge,32 and their role as Th2 cytokine producers in the lower airways is becoming more clear.31 Moreover, airway basophils have been shown to produce IL-4 on allergen provocation.33
There has recently been considerable interest in IL-10 as an immunomodulatory cytokine in allergy.34 It was suggested that IL-10 produced by regulatory T cells is essential for immune homeostasis and that this mechanism might be defective in asthmatics.34 Decreased IL-10 expression at both the protein level and the mRNA level has, indeed, been reported in bronchoalveolar lavage fluid from asthmatic patients compared with healthy controls.35 However, we were not able to demonstrate decreased IL-10 mRNA expression in the airways of asthmatic patients; rather, there was a tendency towards increased IL-10 expression in the airways of asthmatic patients. In accordance with our findings, Robinson et al36 also reported increased IL-10 mRNA levels in asthmatic airways.
We conclude that, of the cytokines analysed, the most interesting for further study at the mRNA level are IL-4 because of the differences between patients with allergic and non-allergic asthma; IFN-γ which is more prominent in more severe asthma; and IL-5 because it correlates with eosinophilic inflammation as well as with eNO and airway hyperreactivity. These conclusions should now be further validated in larger patient groups and in prospective studies in order to evaluate the effects of treatment.
Acknowledgments
The authors thank the technicians in the Divisions of Allergy and Pneumology for their cooperation.
REFERENCES
Footnotes
-
Published Online First 31 January 2006
-
This research was supported by a grant from the Institute for the Promotion of Innovation through Science and Technology in Flanders (IWT Vlaanderen), a grant from the Fund for Scientific Research (FWO) Vlaanderen, a grant from the Study Center for Allergy Projects (SCAP), a postdoctoral fellowship from FWO to AmAB, and a fellowship to ET from IWT Vlaanderen.
-
Competing interests: none declared.
Linked Articles
- Airwaves