Article Text

Statistics from Altmetric.com
Empyema is most often a complication of bacterial pneumonia or, less commonly, thoracic trauma or surgery. There have been reports of increasing numbers of children presenting to regional units in the UK,1–3 but there are no published national data that may provide evidence of a clear trend. Analysis of national routine admissions data provides information on health service utilisation and may provide a marker for the incidence of this relatively uncommon disease.
Hospital admissions in England were obtained from the hospital episode statistics system (www.dh.gov.uk). This database contains personal, administrative, and medical data on all patients admitted to NHS hospitals in England. It records episodes of care following admission to hospital and assigns a primary diagnosis on discharge using the WHO International Classification of Diseases (ICD). Data are available by financial year (1 April to 31 March). From April 1995 diagnoses were classified using the 10th revision of ICD (ICD 10).
We identified admissions with a primary diagnosis of pyothorax (which includes the diagnoses of empyema, pyopneumothorax (pneumoempyema) and abscess of the pleura or thorax) in ICD 10 (code J86) between April 1995 and March 2003. The numbers of admissions for abscess of the pleura or thorax are likely to be small compared with those for empyema and pyopneumothorax, hence this code provides a good indication of trends in empyema. Age-specific admission rates were calculated using population data from the corresponding period. To investigate changes over time we used rate ratios to describe the increases over the 8 year period and tested for time trend by fitting linear regression equations for each age group. All analyses were undertaken using Stata version 8.
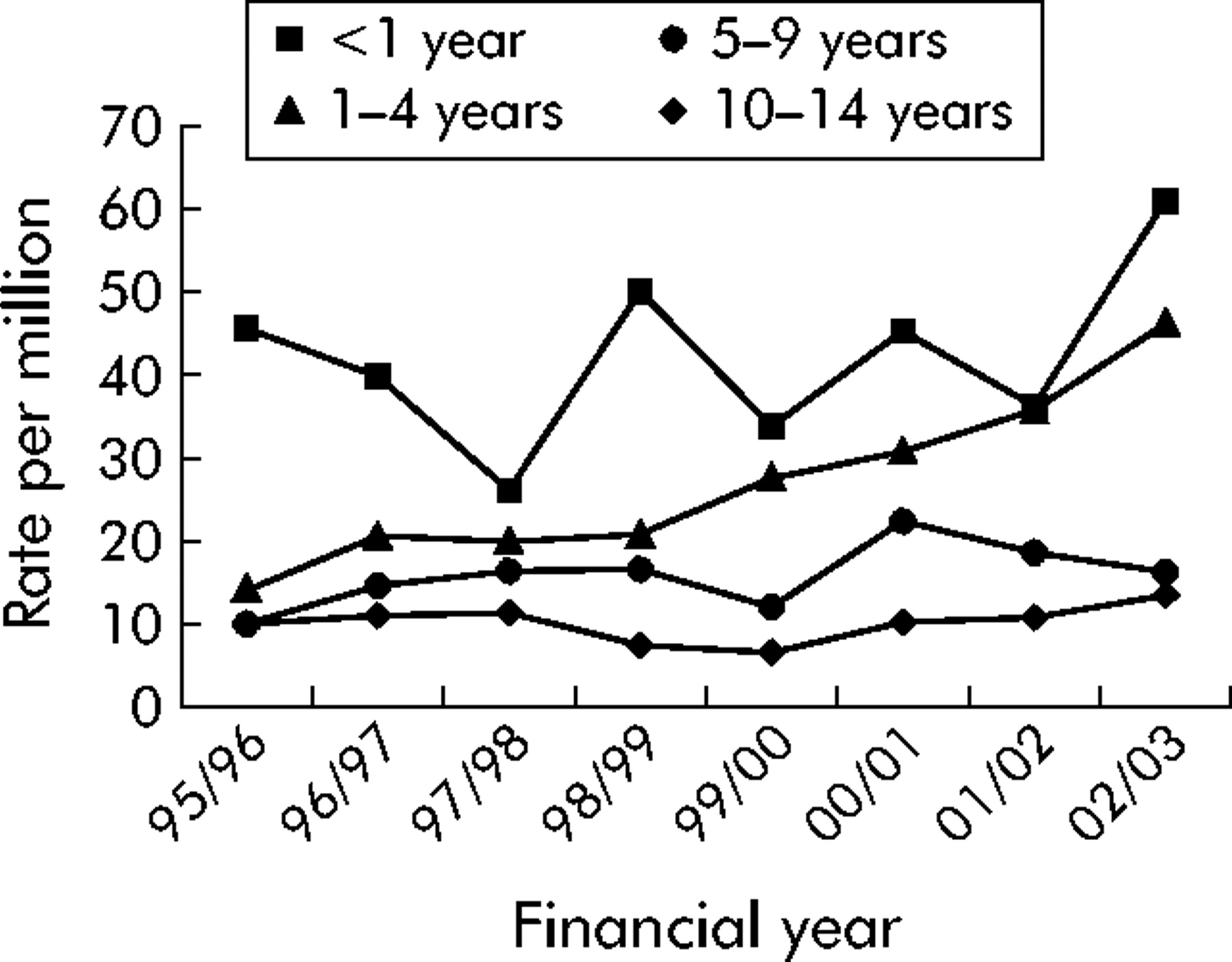
There were a total of 1379 admissions for pyothorax from April 1995 to March 2003 in children aged 0–14 years. The rate of admission increased from 14 per million in 1995/6 to 26 per million in 2002/3 with a significant upward linear trend (p = 0.003). The rises were greatest in children aged 1–4 years in whom admissions rose threefold over the 8 year period (fig 1). There were smaller rises in infants under the age of 1 year and in children aged 5–9 years and those aged 10–14 years, but a test for linear trend was not significant in any of these age groups (table 1). Admissions were slightly higher in boys than girls throughout the period, although the rates of increase were similar in both sexes.
Number and rate of admissions for pyothorax in children aged 0–14 years in England in 1995/6 and 2002/3: rate ratios between 2002/3 and 1995/6 with 95% confidence intervals and linear regression p values
{kind=link}
Trends in admission rates for pyothorax by age in England, 1995–2003.
We have identified increased admission rates from 1995 to 2003 for pyothorax in children of all ages between 0 and 14 years and across both sexes, most prominent in the 1–4 year olds. Trends in admissions must be interpreted with caution as they can reflect changes in health care, in disease labelling, coding or recording, as well as in the underlying epidemiology of the condition. We were unable to assess the accuracy of clinician diagnoses or recording. However, we consider it likely that any diagnostic transfer would remain within the ICD labels of pyothorax and “pleural effusion, not elsewhere classified (NEC)” (J90) which includes pleurisy with effusion but excludes chylous and tuberculous effusions and pleurisy not otherwise specified. Over this period admissions for pleural effusion NEC also rose significantly (not presented). It is also likely that some empyema cases could be coded as a secondary diagnosis under a primary diagnosis of pneumonia, in which case these data would under-represent the incidence of the problem. These rises are unlikely to be explained by major shifts in health seeking behaviour as empyema is a serious condition requiring hospital admission. This increase in pyothorax admissions is therefore likely to be due largely to an increase in the incidence of empyema.
Thoracic surgery and trauma account for less than 2% of empyema, which is most commonly caused by bacterial pneumonia. A rising incidence in childhood empyema associated with Streptococcus. pneumoniae serotype 1 infection has been observed in the USA.4,5 The majority of children in the north east of England presenting with empyema from February 1997 to August 2001 were infected with serotype 1,3 which is not included in the heptavalent conjugate pneumococcal vaccine. There was also a consistent year-on-year rise in the number of children presenting with empyema in the same region from 1998 to 2001.3 We recognise that the number of admissions nationally for empyema is small, but these large increases in recent years warrant further investigation.
Footnotes
-
RG is funded by Asthma UK, British Lung Foundation, and British Thoracic Society.
-
Competing interests: none declared.