Article Text

Abstract
Background: The prevalence and severity of chronic cough in the community is uncertain. In a large population of representative normal subjects, we explored the relationship between self-reported cough severity and frequency, and factors known to be related to the aetiology of chronic cough. In particular, we have examined the relative association between cough and symptoms of gastrointestinal disease.
Methods: A cross-sectional survey was undertaken in 36 general practices with subjects randomly selected from practice computer databases. Baseline lifestyle and demographic characteristics were recorded. Participants were asked how often in the previous 2 months they had experienced bouts or spasms of coughing. Cough symptom status was dichotomised into symptomatic using a cut off of bouts or spasms of coughing at a frequency of between once a week and once a day or above. Gastrointestinal data were collected using validated methodology.
Results: Questionnaires were sent to 6416 subjects and 4003 (62%) responded. The prevalence of chronic cough was 12%, and was severe in 7%. Following multivariate analysis, regurgitation (OR 1.71; 99% CI 1.20 to 2.45) and irritable bowel syndrome (OR 2.00; 99% CI 1.47 to 2.72) were strong predictors of cough. Smoking (OR 1.61; 99% CI 1.18 to 2.19), declining social class (OR 1.63; 99% CI 1.04 to 2.57), and quality of life at baseline (OR 1.63; 99% CI 1.13 to 2.35) were also significantly associated.
Conclusion: Chronic cough is a common symptom in the general population. Its strong association with gastrointestinal disease may have aetiological significance.
- BMI, body mass index
- IBS, irritable bowel syndrome
- NSAID, non-steroidal anti-inflammatory drug
- cough
- gastro-oesophageal reflux
- prevalence
- survey
- irritable bowel syndrome
Statistics from Altmetric.com
Cough is the most common symptom of medical importance representing over half of new patient consultations in primary care.1 The majority of this morbidity is due to viral respiratory tract infections, which are acute and self-limiting. In some patients, however, cough is a chronic unremitting symptom leading to a marked decrement in quality of life.2,3 The prevalence of chronic cough has been estimated at between 3% and 40% of the population.4–6 A survey by the European Respiratory Society of 18 277 subjects aged 20–48 years from 16 countries worldwide reported nocturnal cough in 30%, productive cough in 10%, and non-productive cough in 10%.7 However, the distribution of cough in the population in terms of severity and frequency is still poorly understood.
It has been suggested that there are three common causes of chronic cough: asthma, post-nasal drip, and gastro-oesophageal reflux.8 While there is no doubt that the various syndromes of eosinophilic inflammation of the airways such as cough variant asthma and eosinophilic bronchitis may cause chronic cough, the existence of post-nasal drip as a separate clinical entity has been called into question.9 Gastro-oesophageal reflux has been recognised as an important cause of chronic cough for over 25 years, but the frequency with which it is reported to be causally related varies widely.10 This variation reflects difficulties in confirming—either clinically11 or by investigation12—an association between cough and a reflux event.
In this present study we have sought to establish the prevalence of self-reported chronic cough in a large population of representative normal subjects, and have explored the relationship between cough severity and frequency and factors known to be related to gastro-oesophageal reflux.
METHODS
Study population
The study was a cross-sectional survey performed as part of a 10 year follow up of individuals recruited into a population Helicobacter pylori screening and treatment programme. This was conducted in Leeds and Bradford, cities in West Yorkshire, UK with a combined population of approximately 1 200 000. The original study started in 1994 with 2 years of follow up. Recruitment was via 36 general practices, with subjects aged 40–49 years randomly selected from the practice computer databases. This age group was chosen to maximise the prevalence of H pylori infection in the individuals under study. Over 30 000 people were contacted originally, of whom 8407 attended and were eligible for inclusion in the study. These individuals were invited to attend for screening for H pylori by 13-carbon labelled urea breath test.13 Exclusion criteria for the original study included receiving antibiotics or bismuth within the last 2 weeks or proton pump inhibitors (PPIs) within the last week; a documented allergy to macrolides, 5-nitroimidazoles, or PPIs; concomitant treatment with warfarin, theophylline, digoxin, anticonvulsants, and antihistamines; and those who were unable to abstain from alcohol for 1 week.
In order to trace those involved, the general practices that recruited the individuals were visited and their databases accessed to obtain a current address for all participants. Those successfully located were sent questionnaires by post. Informed written consent to access the primary care records was requested. Non-responders were sent a second postal questionnaire. The local research ethics committees in Leeds and Bradford approved the study in March 2003, and questionnaires were sent out in August 2003.
Data collection
Baseline lifestyle factors and demographic characteristics for study participants including age; sex; marital status; ethnicity; tobacco, alcohol, and coffee consumption; social class (as defined by occupation); and H pylori status were stored on file from the original study.
In addition, at study entry participants completed a copy of the psychological and general well-being index (PGWBI),14 a validated quality of life scale consisting of 22 questions, with a higher score indicating a better health status. Baseline quality of life data were split into three equal sized groups according to total PGWBI score: low (scores 31–100); medium (101–112); and high (113 and above).
At 10 year follow up, participants were asked how often in the previous 2 months they had experienced bouts or spasms of coughing. Responses were rated on a 5-point Likert scale (not at all; less than once a month; between once a month and once a week; between once a week and once a day; and once a day or more). To explore the association of cough frequency with other variables, cough symptom status was dichotomised into symptomatic or asymptomatic, using a cut off point of bouts or spasms of coughing at a frequency of between once a week and once a day and above. Cough severity was assessed by enquiring how often the symptoms had interfered with normal activities of daily living in the previous 2 months on a comparable 5-point Likert scale.
Dyspepsia data at 10 years were collected using the short form Leeds dyspepsia questionnaire (S-FLDQ). The S-FLDQ assesses both the frequency and severity of four symptoms—indigestion, heartburn, regurgitation, and nausea (all of which are rated on a 5-point Likert scale identical to that used for the cough question)—as well as asking the subject to identify the most troublesome of these four symptoms. This questionnaire has been previously validated and is acceptable, reliable, and responsive.15 In addition, it is self-administered, which makes it ideal for use in a postal survey. Individual symptom status was dichotomised into symptomatic or asymptomatic for both heartburn and regurgitation, using a symptom frequency of once a month to once a week and above to define symptomatic.
A second questionnaire used the Manning criteria for the diagnosis of irritable bowel syndrome (IBS).16 It enquired about the presence of six symptoms: abdominal pain eased by defecation; stool frequency when abdominal pain commenced; loose stools when abdominal pain commenced; tenesmus; mucus per rectum; and abdominal distension. Symptom frequency was rated on a 3-point Likert scale (never; occasionally; or more than once a week). Individuals were defined as having IBS if they provided a positive response to any of the six symptoms at a frequency of more than once a week.
Finally, participants were asked to give their current weight (in kg) and their height (in metres) to allow calculation of their body mass index (BMI) at 10 years. These were divided into three categories: normal (18.5–24.9); overweight (25–29.9); and obese (30 or more). Data on non-steroidal anti-inflammatory drug (NSAID) and/or aspirin use in the preceding year were also obtained, but only for those individuals allowing access to their primary care records.
Sample size
The original power calculation was based on the expected prevalence of H pylori and the difference in dyspepsia rates predicted in those receiving eradication treatment compared with placebo. This is not the relevant outcome for this study. Retrospective sample size calculations were performed to determine the power of the study. A sample size of 3300 subjects would detect an odds ratio of cough of 1.5 between cases (subjects with reflux symptoms and/or IBS) and controls at the 80% power and 5% significance level. This assumes that 10% of controls report chronic cough and IBS and/or reflux symptoms are present in at least 20% of the population.
Statistical analysis
The associations between demographic data, lifestyle factors, gastro-oesophageal reflux (including the individual symptoms of heartburn and regurgitation), quality of life, IBS, and NSAID and/or aspirin use and the presence of cough were explored using univariate analysis. Age and presence of cough were analysed using the Student’s t test and expressed as the mean difference with 99% confidence intervals (CI). Independent risk factors for the presence of cough were determined by performing multivariate logistic regression, controlling for all demographic data, lifestyle factors, symptoms of gastro-oesophageal reflux, quality of life, and presence of IBS (NSAID and/or aspirin use were not examined in these analyses as data were only available for those who had given consent to review their primary care records). Due to a priori concerns regarding multiple comparisons being made, a two tailed p value of <0.01 was considered to be statistically significant, and the results of univariate and multivariate analyses were expressed as odds ratios (OR) with 99% CI.
All statistical analyses were performed using StatsDirect statistical software version 2.2.5 (StatsDirect Ltd, Sale, Cheshire, UK), and SPSS for Windows version 11.5 (SPSS Inc, Chicago, Illinois, USA).
RESULTS
Of the 8407 original participants, 1991 (24%) could not be traced to a current address. Questionnaires were sent to the remaining 6416 and 4003 (62%) responded, 3246 (81%) to the first questionnaire. Of those who responded, 3883 (97%) completed the cough question (fig 1). We were less likely to successfully contact males, smokers, and those with dyspepsia at baseline, and more likely to contact those of higher social class. The demographic data of those who responded are given in table 1.
Demographic data of responders

Flow of study participants at 10 year follow up.
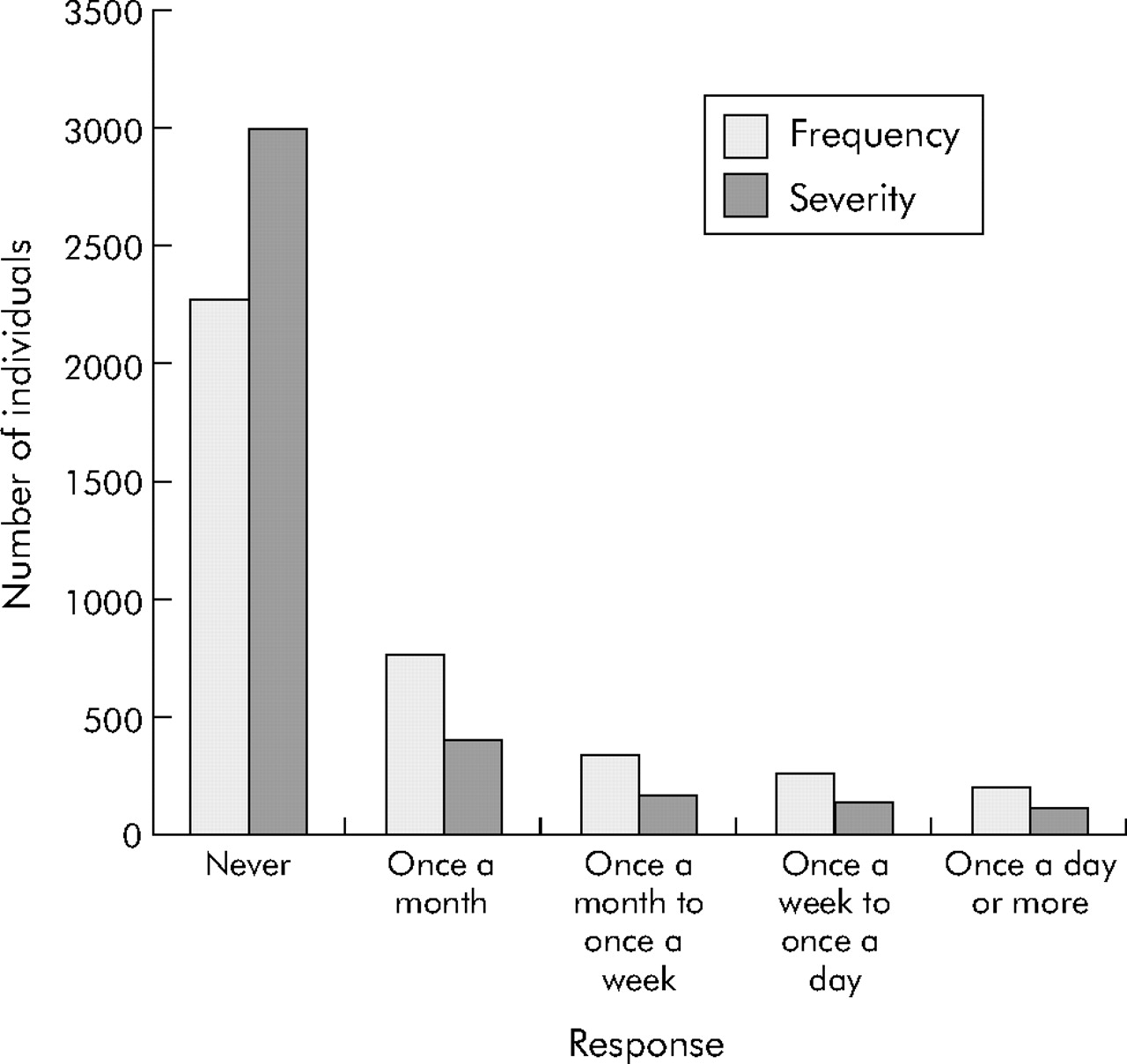
Cough frequency in the previous 2 months was reported as never by 59%, less than monthly by 20%, between monthly and weekly by 9%, between weekly and daily by 7%, and daily by 5%. The overall prevalence of chronic cough (defined as greater than weekly coughing bouts) in the population under study was therefore 12% (n = 481). Cough severity affecting activities of daily living was reported as occurring never in 78%, less than monthly in 11%, between monthly and weekly in 4%, between weekly and daily in 4%, and daily in 3%. Cough severe enough to interfere with normal activities of daily living was therefore experienced on a daily or weekly basis in 7% (n = 264, fig 2). When these data were examined according to sex, the prevalence of chronic cough was 13% (n = 287) in women and 11% (n = 194) in men, while severe cough was present in 7% (n = 155) of women and 6% (n = 109) of men. The prevalence of cough occurring on a daily basis was significantly higher in women than in men (6.2% (n = 135) v 4.6% (n = 78), p = 0.03).

{kind=link}
{kind=link}
Frequency and severity of cough in all study subjects.
Univariate analysis revealed several positive associations (table 2). Those with cough were more likely to have heartburn (OR 2.17; 99% CI 1.65 to 2.85) and regurgitation at 10 year follow up (OR 2.61; 99% CI 1.93 to 3.52). In addition, those with IBS were more likely to complain of cough (OR 2.93; 99% CI 2.24 to 3.82). Lifestyle factors associated with cough included smoking tobacco (OR 1.91; 99% CI 1.44 to 2.52), abstinence from alcohol (OR 1.83; 99% CI 1.21 to 2.71), and obesity (OR 1.66; 99% CI 1.19 to 2.32). Finally, declining social class (OR 2.03; 99% CI 1.33 to 3.06 for social class IV+V v social class I+II) and quality of life at baseline (OR 2.26; 99% CI 1.62 to 3.17 for low v high) were both significantly associated with the presence of cough. Age appeared to have no significant impact on the presence of cough (mean difference in age between those with cough and those without = 0.31 years; 99% CI –0.04 to 0.67, p = 0.02).
Univariate and multivariate analyses for presence of cough
Following multivariate analysis, the presence of regurgitation (OR 1.71; 99% CI 1.20 to 2.45) and IBS (OR 2.00; 99% CI 1.47 to 2.72) at 10 years remained strong predictors of the presence of cough. Other significant associations included smoking (OR 1.61; 99% CI 1.18 to 2.19), declining social class (OR 1.63; 99% CI 1.04 to 2.57 for social class IV+V v social class I+II), and quality of life at baseline (OR 1.63; 99% CI 1.13 to 2.35 for low v high). The presence of heartburn at 10 years as a predictor of cough approached statistical significance (OR 1.32; 99% CI 0.95 to 1.83), as did obesity (OR 1.34; 99% CI 0.93 to 1.91).
DISCUSSION
Our study is the first to report the self-assessment of the frequency and severity of cough in the community. Previous surveys have sought to determine the prevalence of cough, but have not differentiated between the universal phenomenon of cough due to acute respiratory tract infection and chronic cough of other aetiology. By enquiring as to the frequency and severity of coughing bouts over the preceding 2 months, we attempted to select those individuals who have significant chronic cough but not those suffering from acute short lived upper respiratory tract infection (URTI) who we suggest would be unlikely to describe their cough as weekly or daily. To minimise the confounding effects of URTI further, questionnaires were sent out in July and August so responses would be expected to reflect the nadir of seasonal URTI in England.17 The 12% of individuals reporting the composite end point of daily and weekly cough emphasises the fact that chronic cough is one of the most common symptoms of medical importance.
Self-reported cough severity was used as a surrogate for the impact of chronic cough on quality of life. 7% of individuals reported daily or weekly chronic cough severe enough to interfere with activities of daily living. Previous studies have shown a marked decrement in quality of life with chronic cough, similar to that seen in patients with severe chronic obstructive pulmonary disease.7 Our study suggests that considerable psychosocial morbidity due to chronic cough is present within this representative population.
The primary aim of this study was to shed light on the association between chronic cough and gastrointestinal disease. We found a close association between self-reported chronic cough and the classic symptoms of gastro-oesophageal reflux, heartburn and regurgitation. It has become increasingly recognised that the manifestations of gastro-oesophageal reflux disease are not confined to the classic symptoms of reflux, but can be associated with a number of extraoesophageal symptoms. Cough, voice disorders, and sinusitis have all been established as reflux related symptoms.18 Indeed, gastric contents may reflux as far as the middle ear.19 The clinical recognition of these extraoesophageal manifestations of reflux has been slow. This is explained in part by their relatively poor correlation to acidic reflux as manifest by heartburn. 24-hour pH monitoring studies in patients with gastro-oesophageal reflux disease have shown a good correlation between symptoms of heartburn and documented episodes of acid reflux.20 In contrast, oesophageal pH monitoring is poor at predicting response to treatment in reflux cough.12 Our finding of a relatively weak correlation between cough and heartburn confirms this observation and implies that non-acid reflux may be a more important factor in extraoesophageal reflux symptoms. We suggest that, while the known association between heartburn and acid reflux is correct, cough may also be precipitated by non-acid irritation of the upper airway. Thus, a better correlation was seen between cough and regurgitation—the other classic symptom of reflux disease. These latter symptoms may be more related to abnormal oesophageal motility and clearance. In population based studies such as ours, symptoms commonly overlap between individuals with endoscopic evidence of gastro-oesophageal reflux disease and those with gastrointestinal dysmotility.21 We have recently shown that there is a high degree of dysmotility in patients with reflux cough.22 Our additional and previously unreported finding of a close association between chronic cough and symptoms of IBS suggest the existence of a generalised disorder of gut motility causing symptoms from the top to the bottom!
The close association between self-reported cough and regurgitation seen in this study suggests that reflux may be one of the major aetiological factors for chronic cough. Indeed, 59% of individuals who reported chronic cough also reported one classic symptom of reflux and 45% reported two.
Sex related differences in cough reflex have been described. Women are overrepresented in patients attending cough clinics and are more sensitive to cough challenge.23 It was therefore surprising that a similar percentage of men and women coughed on a daily or weekly basis. If, however, daily or more frequent cough was taken as the end point, women outnumbered men by 3:2. This frequency of troublesome cough may be more representative of the population presenting to cough clinics.
The link between obesity and chronic cough may again be through reflux mechanisms. With classic reflux symptoms, a high degree of correlation has been shown with increased BMI.24 Obesity increases the tendency for reflux to occur by mechanisms including hormonal and increased intra-abdominal pressure.24
The link between cough and smoking is hardly surprising and has been previously shown to be dose related.7 The precipitation of cough by cigarette smoke is likely to be due to the development of airway inflammation manifested as an increase in macrophages and cells expressing interleukin and adhesion molecule receptors.25 The consequence of this inflammation is an increase in the sensitivity of the cough reflex when frank bronchitis is present.26 However, this mechanism does not exclude reflux as a precipitant of coughing bouts in smokers. The act of cigarette smoking significantly increases reflux events.27
The impact of chronic cough on quality of life has recently been extensively documented.3,28 When patients with chronic cough are compared with those with severe chronic obstructive pulmonary disease, the impact on life quality is similar.2 However, we are unable to suggest whether the association between chronic cough and a lower quality of life seen in our study is a cause or consequence of the cough, particularly as quality of life was measured during the baseline study.
There are some limitations to this study. The fact that over half of those originally enrolled were either not successfully traced or did not respond to the questionnaire is almost inevitable when performing studies such as this, especially in a group of individuals who were randomly selected from the general population. There may therefore be differences between those who provided data and those who were lost to follow up, meaning that the population examined in this study is not entirely representative of the original sample of individuals. The restricted age range of subjects (now aged 50–59 years) means that the results might not be generalisable to any age group in the general population. There could also be a potential volunteer bias, where those who returned questionnaires at 10 years were more likely to be experiencing cough or dyspepsia symptoms at that point in time. This was certainly the case in the original study, where those who agreed to participate were more likely to have consulted their general practitioner with dyspepsia in the preceding 2 years than those who declined to participate. This could have resulted in the prevalence of cough and its relationship with gastro-oesophageal reflux disease being overestimated. However, as some individuals with gastro-oesophageal reflux induced cough may otherwise be asymptomatic, it is also possible that this association has been underestimated. Finally, the cough questionnaire used in the study had not been previously validated in terms of its ability to discriminate between acute and chronic cough although, as mentioned previously, the questionnaires were sent out in the summer months. There remains the possibility, however, that individuals reporting cough in this study may not be typical of patients with chronic cough.
In summary, 12% of our respondents had coughing bouts on at least a weekly basis. These subjects were significantly more likely to suffer from gastrointestinal symptoms characteristic of reflux disease. These findings support the hypothesis that gastro-oesophageal reflux is an important cause of chronic cough in the community.
REFERENCES
Footnotes
-
Published Online First 29 June 2006
-
Funding: none.
-
ACF has no competing interests. DF has received speaker and consulting fees from AstraZeneca, Wyeth Laboratories and Takeda. PM has received speaker fees and research funds from AstraZeneca, Wyeth Laboratories, and Abbott Laboratories. AHM has received speaker fees and research funds from AstraZeneca, GlaxoSmithKline, and Merk Sharpe & Dome.