Article Text

Abstract
The case history is presented of a lung transplant recipient who developed malignant mesothelioma. This is thought to be the first such report. Mesothelioma should be suspected in lung transplant recipients with a haemorrhagic pleural effusion in the native lung when there is no convincing evidence for bronchogenic carcinoma or post transplant lymphoproliferative disease, even in the absence of exposure to asbestos.
- asbestos
- lung transplant
- mesothelioma
- thoracoscopy
Statistics from Altmetric.com
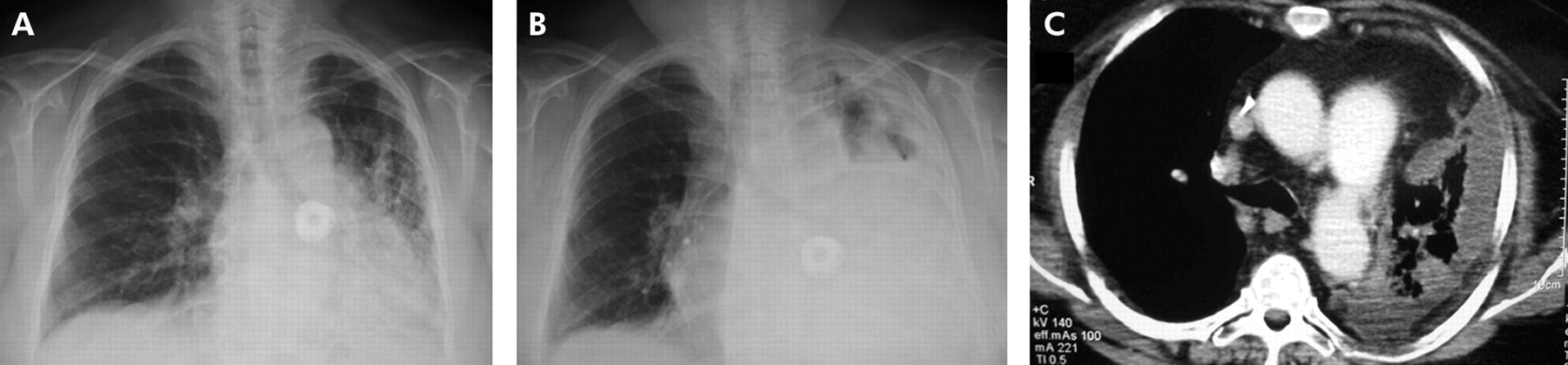
A 63 year old woman underwent right single lung transplantation for idiopathic pulmonary fibrosis in June 1998. The immunosuppression regimen consisted of cyclosporine, mycophenolate mofetil, and prednisolone. A high risk cytomegalovirus constellation was treated prophylactically with a 2 week course of intravenous ganciclovir followed by oral ganciclovir. Five years after transplantation there were no signs of bronchiolitis obliterans syndrome (fig 1A⇓).

(A) Chest radiograph after lung transplantation but before development of the pleural effusion. (B) Chest radiograph and (C) CT scan showing pleural effusion on the left side.
In July 2003 squamous cell carcinoma of the scalp was surgically excised. In the same month she developed a haemorrhagic pleural effusion on the left side (fig 1B⇑). A CT scan of the chest also showed marked consolidation of the underlying left lung (fig 1C⇑). Bronchoalveolar lavage did not show evidence of infection or malignancy, pleural fluid studies did not reveal organisms, and cytological examination showed cells suspicious for adenocarcinoma. Chromosomal analysis by fluorescence in situ hybridisation revealed polysomy for chromosome 6, 7p12 (EGFR), 5p15, and 8q24 (MYC). However, membranous staining for epithelial marker Ber-EP4 was negative, which raised the possibility of a non-epithelial tumour. Thoracoscopy under local anaesthesia revealed fibrinoid inflammation and nodules. Multiple pleural biopsy specimens were obtained from abnormal as well as healthy looking areas. Histological examination revealed diffuse infiltration of the pleura by highly atypical tumour cells exhibiting epithelioid and spindle cell features with a prominent myxoid change in stroma and infiltration of the fatty tissue (fig 2⇓). Immunohistochemical markers for glandular tumours (TTF1 and CD15) and the epithelial marker Ber-EP4 were negative. Biopsy specimens stained positively for vimentin, pancytokeratin 22, and calretinin. Taken together, the histological and immunohistochemical findings led to the diagnosis of malignant mesothelioma of mixed epithelioid and sarcomatoid subtype. A 99m technetium scan showed no perfusion of the native left lung.

{kind=link}
{kind=link}
Histological and immunohistochemical findings. Biphasic malignant mesothelioma with (A) epithelioid and (B) sarcomatoid components (stain: haematoxylin and eosin). Typical immunohistochemical marker profile with strong positivity for (C) pancytokeratin 22, (D) vimentin, (E) calretinin, and (F) negativity for Ber-EP4 (magnification ×400).
Because of the patient’s general condition and co-morbidities, radical pleuropneumonectomy was not considered and chemotherapy was not chosen because of its limited benefit in malignant mesothelioma. Pleurodesis was not possible because the underlying fibrotic lung was unable to expand following drainage for 10 days. A few weeks after discharge from the hospital the patient was readmitted with dyspnoea and signs of infection. Only palliative care was given due to the poor prognosis and the patient eventually died. Histological examination at autopsy confirmed the diagnosis of a biphasic malignant mesothelioma. The tumour showed extensive infiltration of the pleura, pericardium and diaphragm. Asbestos bodies were not seen in the lung tissue.
DISCUSSION
Malignant mesothelioma is a primary cancer that originates from mesothelial cells which line the serous cavities including the pleura, pericardium and peritoneum. It most often occurs in the pleural cavity and is associated with exposure to asbestos, although about 20% of mesotheliomas occur in individuals not exposed to asbestos.1 There was no history of asbestos exposure in our patient.
In lung transplant recipients lymphoid neoplasms have the highest incidence among 1 year survivors, and skin cancers are the most common malignancy in 5 year survivors.2 By 5 years after lung transplantation about 20% of patients will have some form of cancer.2 In a series of 316 lung transplant recipients the incidence of post transplantation lymphoproliferative disease was 2.9%, and one patient had a recurrent haemorrhagic pleural effusion.3 Bronchogenic carcinoma has been reported to develop in the native lung of lung transplant recipients with emphysema and pulmonary fibrosis with frequencies of 2% and 4%, respectively.4 Pulmonary nodules are not uncommon in lung transplant recipients and the causes include bronchogenic carcinoma, post transplantation lymphoproliferative disease, metastatic carcinoma, invasive pulmonary aspergillosis, cytomegalovirus pneumonitis, and bronchiolitis obliterans.5 In a cohort of 3374 solid organ transplant recipients, bronchogenic carcinoma was detected in 0.3% of patients and, of these, it occurred in one of 396 lung transplant recipients.6 Primary non-small cell lung cancer has been reported in the donor lung following lung transplantation.7 Lung transplantation has also been reported for the treatment of bronchoalveolar carcinoma, but the recurrence rate is high and lung transplantation for this indication is controversial.8
Although solid organ transplant recipients have a recognised risk of developing malignancies, there is no evidence in the literature of an enhanced risk for mesothelioma. Most malignancies in transplant recipients are of viral origin and mesothelioma has been linked to infection with simian virus 40 (SV 40).1 Our patient was negative for SV 40 by PCR, as well as JC virus and BK virus. The origin of mesothelioma therefore could not be determined in this case.
To our knowledge, this is the first report of malignant mesothelioma in a lung transplant recipient. Mesothelioma should be suspected in lung transplant recipients with a haemorrhagic pleural effusion in the native lung when there is no convincing evidence for bronchogenic carcinoma or post transplant lymphoproliferative disease, even in the absence of exposure to asbestos.
Footnotes
Funding: none
Competing interests: none declared