Article Text

Abstract
Background: Current guidelines recommend the use of a combination of inhaled β2 agonists and anticholinergics, particularly for patients with acute severe or life threatening asthma in the emergency setting. However, this statement is based on a relatively small number of randomised controlled trials and related systematic reviews. A review was undertaken to incorporate the more recent evidence available about the effectiveness of treatment with a combination of β2 agonists and anticholinergics compared with β2 agonists alone in the treatment of acute asthma.
Methods: A search was conducted of all randomised controlled trials published before April 2005.
Results: Data from 32 randomised controlled trials (n = 3611 subjects) showed significant reductions in hospital admissions in both children (RR = 0.73; 95% CI 0.63 to 0.85, p = 0.0001) and adults (RR = 0.68; 95% CI 0.53 to 0.86, p = 0.002) treated with inhaled anticholinergic agents. Combined treatment also produced a significant increase in spirometric parameters 60–120 minutes after the last treatment in both children (SMD = −0.54; 95% CI −0.28 to −0.81, p = 0.0001) and adults (SMD = −0.36; 95% CI −0.23 to −0.49, p = 0.00001).
Conclusions: This review strongly suggests that the addition of multiple doses of inhaled ipratropium bromide to β2 agonists is indicated as the standard treatment in children, adolescents, and adults with moderate to severe exacerbations of asthma in the emergency setting.
- CCS, corticosteroids
- ED, emergency department
- FEV1, forced expiratory volume in 1 second
- NNT, number of patients needed to treat
- PEF, peak expiratory flow
- RR, relative risk
- SMD, standardised mean difference
- WMD, weighted mean difference
- anticholinergics
- β2 agonists
- ipratropium bromide
- oxitropium bromide
- glycopyrrolate
- acute asthma
- children
Statistics from Altmetric.com
- CCS, corticosteroids
- ED, emergency department
- FEV1, forced expiratory volume in 1 second
- NNT, number of patients needed to treat
- PEF, peak expiratory flow
- RR, relative risk
- SMD, standardised mean difference
- WMD, weighted mean difference
Treatment of acute asthma includes inhaled short acting β2 agonists, systemic corticosteroids (CCS), and supplemental oxygen.1,2 In addition, current guidelines recommend the use of a combination of β2 agonists and anticholinergics, particularly for patients with acute severe or life threatening asthma.2,3 This statement is based on a relatively small number of randomised controlled trials and related systematic reviews.4–6 However, new studies have since been published.7 The aim of this systematic review was to update the evidence on the effectiveness of a combination of inhaled anticholinergics and β2 agonists compared with β2 agonists alone for the treatment of children, adolescents, and adults with acute asthma in the emergency department (ED).
METHODS
Search strategy and selection criteria
The search was conducted using five search strategies to identify potentially relevant trials. (1) MEDLINE (1966–April 2005), EMBASE (1974–April 2005) and CINAHL (1982–April 2005) databases were searched using the following MeSH, full text and keyword terms: emergency OR acute asthma OR status asthmaticus OR severe asthma OR wheeze, AND anticholinergics OR ipratropium OR oxitropium, OR glycopirrolate. (2) An advanced search of the Cochrane Controlled Trials Register (first quarter 2005) was completed using the above search strategy to identify any additional trials. (3) References from included studies, reviews, and texts were searched for citations. (4) Hand searching of the top 20 respiratory journals was completed. (5) We made inquires to Boehringer Ingelheim regarding other published or unpublished trials supported by the company. Trials published solely in abstract form were excluded.
Included studies met the following criteria: (1) Target population: children (18 months to 17 years) and adults (⩾18 years) with acute exacerbations of asthma presenting to an ED or equivalent care setting. (2) Intervention: single or repeated doses of inhaled anticholinergic agents given in combination with inhaled β2 agonists compared with inhaled β2 agonists alone. Studies involving the use of atropine were excluded. (3) Design: randomised and placebo controlled trials without language restriction. (4) Primary outcomes: admission to hospital and spirometric testing (final absolute values or change from baseline 60–120 minutes after the last combined anticholinergic and β2 agonist inhalation). Because the peak bronchodilator effect after the administration of anticholinergics occurs within 1–2 hours, it is reasonable to expect significant improvement during this time. Secondary outcome measures were clinical score, duration of treatment in the ED, respiratory rate, oxygen saturation, heart rate, and side effects.
Data abstraction and validity assessment
Titles, abstracts, and citations were independently reviewed by two reviewers (GJR and JACR) to assess potential relevance for full review. From the full text, both reviewers independently assessed studies for inclusion based on the criteria for population, intervention, study design and outcomes. Data extraction included the following items: (1) Population: age, sex, number of patients studied, patient demographic data, withdrawals. (2) Intervention: agent, dose, route of delivery, and duration of treatment. (3) Control: concurrent treatments. (4) Outcomes. (5) Design: method of randomisation and allocation concealment. Any disagreement over study inclusion was resolved by consensus. The methodological quality of each trial was evaluated using the 5-point scale (0 = worst and 5 = best) described by Jadad et al.8 This instrument assesses the adequacy of randomisation, blinding, and the handling of withdrawals and drop outs.
Data analysis
The data were combined in the meta-analysis by means of random effects models.9 Binary outcomes were pooled using common relative risk (RR) and 95% confidence intervals (CI). The number of patients needed to treat (NNT) to prevent the adverse outcome of interest was calculated. For continuous outcomes the weighted mean difference (WMD) (for variables using the same unit of measure) or the standardised mean differences (SMD) (reported in SD units where different units were used) and 95% CI were calculated. We tested for heterogeneity using the DerSimonian and Laird Q statistic and also measured heterogeneity with the I2 test.10 Values of 25%, 50%, and 75% represent low, moderate, and high heterogeneity, respectively. Publication bias was evaluated by means of formal statistical analysis.11 Otherwise, a p value of <0.05 using a two tailed test was considered significant. When heterogeneity was found, subgroup analyses were carried out in an attempt to explain the findings. Sensitivity analysis was performed to identify sources of heterogeneity. These subgroups included: intensity of anticholinergic protocol, baseline severity, co-therapies, and methodological quality of the studies. The meta-analysis was performed using Review Manager 4.2.7 software (Cochrane Review Manager, Cochrane Collaboration, Oxford, UK, 2004).
RESULTS
A total of 88 studies were examined in full text for possible inclusion, 56 of which were excluded for the following reasons: non-randomised trials (n = 4), non-acute asthma (n = 14), anticholinergics alone were studied (n = 6), hospitalised patients (n = 8), use of atropine (n = 5), chronic asthma (n = 18), and use of intravenous route (n = 1). A total of 32 randomised controlled trials (16 including children and adolescents12–27 and 16 including adults28–43) were therefore selected for further analysis (tables 1 and 2). Five studies were supported by Boehringer Ingelheim.17,18,35–37 Data for 3611 subjects (1564 children and adolescents, 2047 adults) were available for meta-analysis. There was a total agreement between the two independent reviewers on inclusion of studies and Jadad study quality grading. The anticholinergic agent used was ipratropium bromide in 29 studies,12–32,34–38,40,42,43 oxitropium bromide in two studies,39,41 and glycopyrrolate in one study.33 Trials were grouped according to the intensity of the anticholinergic treatment: those testing the addition of a single dose of an anticholinergic agent to β2 agonist inhalations were named single dose protocols, and those testing more than one dose were grouped as multiple dose protocols. Thirteen studies (five in children12,13,16,18,21 and eight in adults28,29,31,32,33,36,38,43) tested a single dose protocol and the remaining 19 trials used more than one dose of anticholinergic. Of these, 18 studies tested multiple doses in a predetermined fixed regimen (multiple dose fixed protocol) and one study tested the addition of anticholinergics to every β2 agonist inhalation, leaving the number of inhalations determined by the patient’s needs (multiple dose flexible protocol).20 One trial tested the first two protocols.18 Asthma severity was defined at baseline by spirometric testing (forced expiratory volume in 1 second (FEV1) or peak expiratory flow (PEF) 70–50% of predicted = moderate exacerbation, and FEV1 or PEF <50% of predicted = severe exacerbation) or different clinical scores. Most enrolled patients with acute asthma had moderate to severe exacerbations, but several studies reported data stratified on asthma severity.22–24,37,41,42 The most frequently reported outcomes were hospital admission (20 studies) and spirometry (26 studies); respiratory resistance measured by forced oscillation was used in one trial.21 One study did not provide spirometric data or admission rates.13 Clinical scores were used in only a few studies and the reporting of adverse effects was variable.
Characteristics of trials in children included in the review
Characteristics of trials in adults included in the review
Hospital admissions
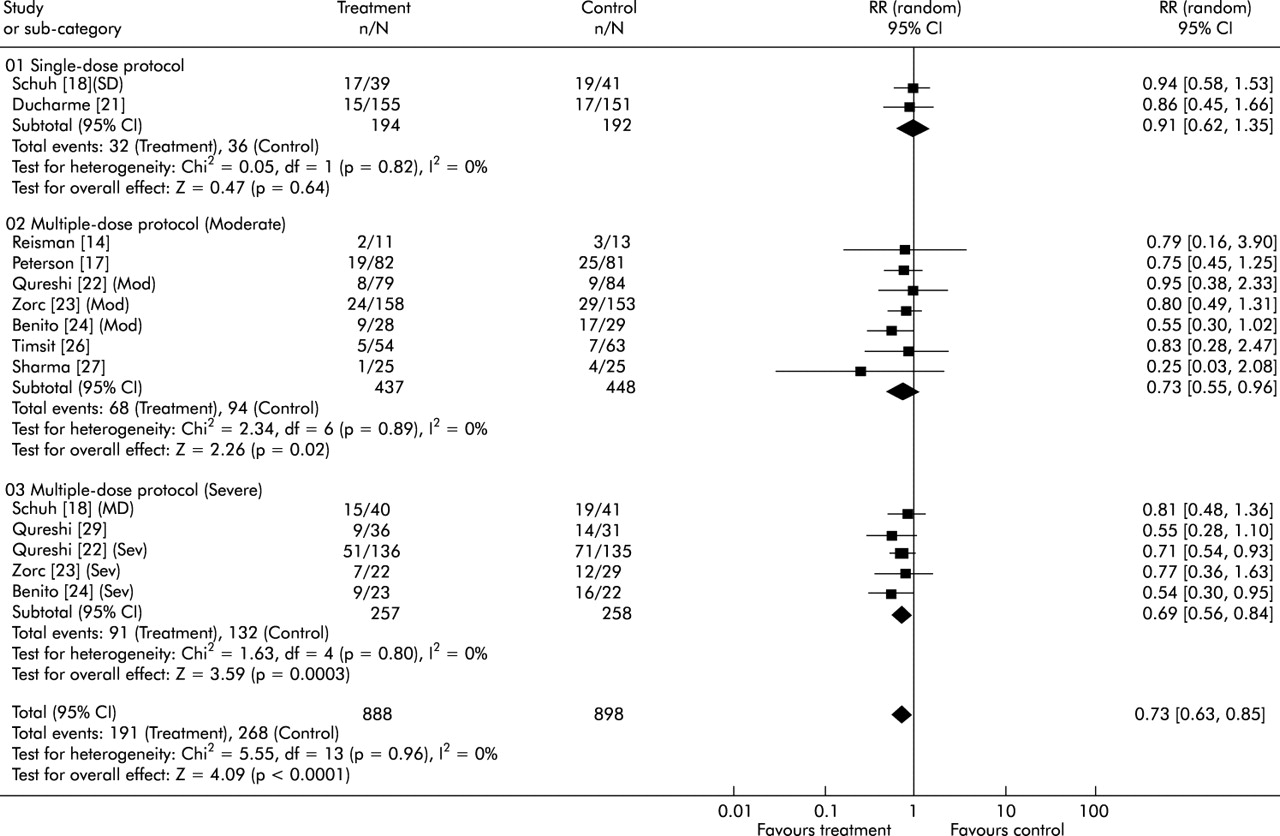
Ten studies accumulating 1786 children and adolescents reported hospital admissions.14,17–19,21–24,26,27 One study tested two protocols (single and multiple fixed dose)18 and three trials reported data stratified by asthma severity (moderate and severe patients).22–24 At the end of treatment patients who received inhaled β2 agonists and anticholinergics had a significantly lower admission rate (fig 1). The NNT was 13 (95% CI 9 to 28), indicating that 13 children needed to be treated with β2 agonists and anticholinergics to prevent one admission. There was no evidence of systematic bias identified by the measure of funnel plot asymmetry. Also, no significant heterogeneity was demonstrated, which accepts the null hypothesis of similar treatment effects. Stratification on the basis of baseline severity (moderate v severe) and the intensity of the anticholinergic protocol (single v multiple fixed dose protocol) suggested a trend towards a reduced risk of admission in children with the most severe asthma attack and treated with multiple doses of anticholinergics. The NNT to prevent one admission among severe patients was 7 (95% CI 4 to 16). The hospital admission rate did not change when we excluded studies without explicit admission criteria (RR = 0.73; 95% CI 0.62 to 0.85, I2 = 0%). The use of systemic CCS did not modify this outcome (RR = 0.69; 95% CI 0.58 to 0.81).

Pooled relative risk for hospital admission (with 95% confidence interval) of eligible studies in children comparing the addition of anticholinergic agents to β2 agonists (treatment) with β2 agonists alone (control). Trials stratified according to intensity of anticholinergic treatment (single or multiple fixed dose protocols) and asthma severity (moderate or severe patients).
Nine trials totalling 1556 adults with acute asthma reported hospital admissions.33–38,40–42 One trial reported data stratified on asthma severity (moderate and severe patients).42 There was a significant reduction in the hospital admission rate favouring anticholinergic use (fig 2). The NNT was 14 (95% CI 9 to 30). There was no evidence of systematic bias identified by the measure of funnel plot asymmetry. Again, no significant heterogeneity was demonstrated. Stratification on the basis of baseline severity (moderate v severe) and the intensity of the anticholinergic protocol (single v multiple fixed dose) suggested a trend towards a reduced risk of admission in adults with the most severe asthma attack and treated with multiple doses of anticholinergics (fig 2). Intensity of anticholinergic treatment greatly influenced the reduction in hospital admission; a greater reduction was seen in trials using three or more doses of anticholinergic agents (RR = 0.53; 95% CI 0.36 to 0.76, p = 0.0006; NNT = 6; 95% CI 4 to 13). These results did not change when only studies with explicit admission criteria were pooled (RR = 0.58; 95% CI 0.38 to 0.87, I2 = 28%) or when systemic CCS were used (RR = 0.74; 95% CI 0.48 to 1.14).
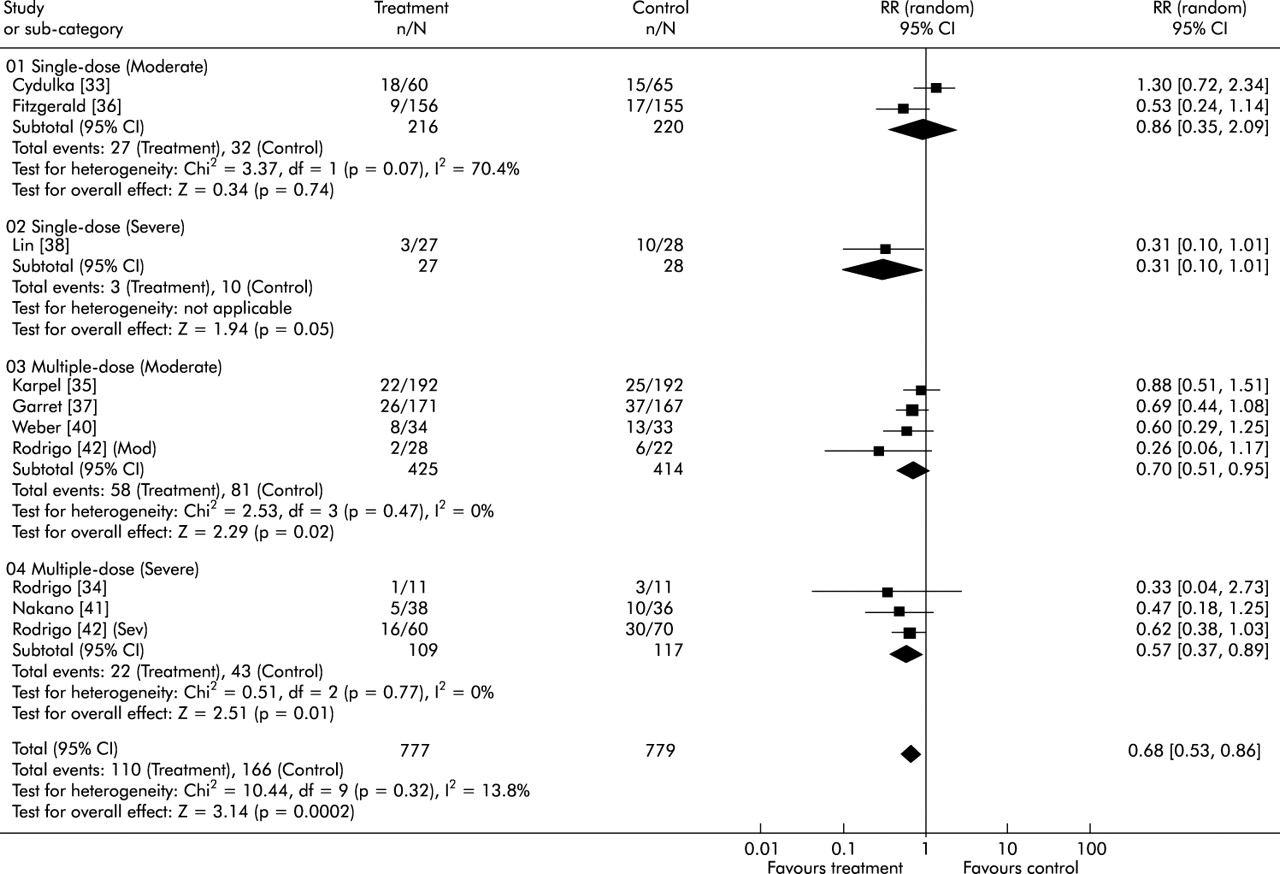
Pooled relative risk for hospital admission (with 95% confidence interval) of eligible studies in adults comparing the addition of anticholinergic agents to β2 agonists (treatment) with β2 agonists alone (control). Trials stratified according to intensity of anticholinergic treatment (single or multiple fixed dose protocols) and asthma severity (moderate or severe patients).
Spirometric testing
Nine studies examined the response to treatment in children and adolescents with acute asthma using spirometry.12,14–16,18,19,22,25,27 Five trials reported the percentage change in FEV1,12,14–16,25 three reported the percentage change in PEFR,19,22,27 one reported the change in percentage predicted FEV1,18 and one study reported the percentage change in respiratory resistance.21 One trial tested two protocols18 (single and multiple fixed dose) and one study presented data stratified by severity of obstruction (moderate and severe).22 Data were recorded 60–120 minutes after the last combined treatment. When all the studies were pooled a significant improvement in spirometric parameters favoured the combination treatment (SMD = −0.54; 95% CI −0.28 to −0.81, p = 0.0001). However, there was significant heterogeneity (χ2 = 23.41, df = 10, I2 = 57.3%, p = 0.009). When we pooled the seven studies that reported FEV1 data (change in percentage predict or percentage change)12,14–16,18,25,27 stratified by the intensity of anticholinergic treatment (one or two doses v more than two doses), homogeneity was achieved (fig 3). The use of more than two doses of anticholinergics showed more benefit than lower doses. There was no evidence of systematic bias. Patients treated with one or two doses of anticholinergic agents had a mean difference of change in FEV1 of 12.4% (95% CI 5.4 to 19.4) compared with those who did not receive anticholinergics, while those who received more than two doses had a mean difference of 16.3% (95% CI 8.2 to 24.5).

Pooled standardised mean difference (with 95% confidence interval) in forced expiratory volume in the first second (change in percentage predicted or percentage change) of children studies comparing the addition of anticholinergic agents to β2 agonists (treatment) with β2 agonists alone (control). Trials stratified according to the intensity of anticholinergic treatment (one or two doses v more than two doses).
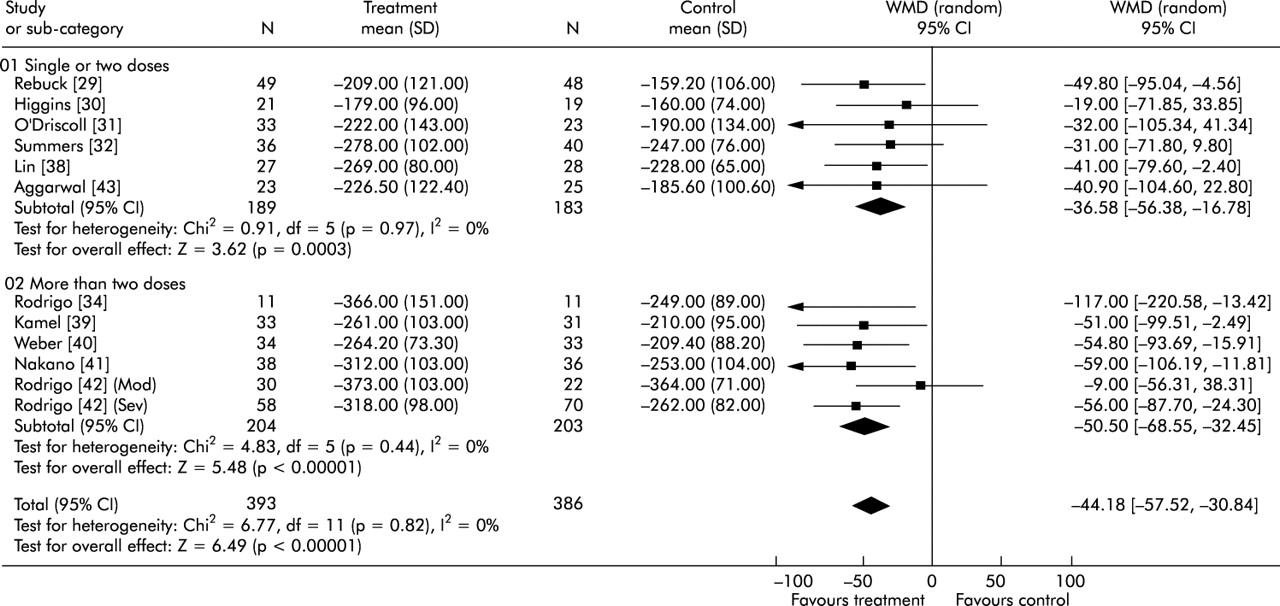
Spirometric data were reported by 16 studies in adult subjects.28–43 Two trials showed data stratified by severity of obstruction (moderate and severity).41,42 Eight trials reported FEV1 (l),28,29,34–37,39,42 11 reported PEFR (l/min),29–32,34,38–43 and one reported FEV1 (% predicted).33 Combined treatment produced a significantly greater increase in spirometric parameters than β2 agonists alone (SMD = −0.36; 95% CI −0.23 to −0.49, p = 0.00001). There was a significant heterogeneity between trials (χ2 = 25.5, df = 15, I2 = 41.3%, p = 0.04). Homogeneity was achieved when studies that reported PEFR (l/min) were stratified by intensity of anticholinergic treatment (fig 4).29–32,34,38–43 Again, the use of more than two doses of anticholinergics produced a greater benefit than one or two doses and there was no evidence of systematic bias. As previously observed for PEFR, patients treated with more than two doses of anticholinergics had a significant difference in FEV1 of 0.44 l (95% CI 0.25 to 0.63) while those treated with one or two doses had a difference of only 0.15 l (95% CI 0.05 to 0.24).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pooled weighted mean difference (with 95% confidence interval) in peak expiratory flow (l/min) of studies in adults comparing the addition of anticholinergics to β2 agonists (treatment) with β2 agonists alone (control). Trials were stratified by intensity of anticholinergic treatment (one or two doses v more than two doses).
Other outcomes
Three paediatric studies21,22,24 reported a significant reduction in the clinical score after combined treatment (SMD = −0.29; 95% CI −0.51 to −0.07, p = 0.01). No significant heterogeneity was demonstrated (χ2 = 1.33, df = 3, p = 0.72, I2 = 0%). There was no apparent increase in the occurrence of side effects among subjects treated with either single or multiple dose protocols. Thus, there was no significant difference between groups in the five studies in children that reported the presence of tremor (RR = 1.15; 95% CI 0.79 to 1.69, p = 0.46).13,14,17,18,27 An identical pattern was seen in three adult studies that reported the same variable (RR = 1.28; 95% CI 0.92–1.78, p = 0.14).31,35,42 Six adult trials that evaluated the effect of treatment on heart rate did not find a difference between groups (WMD = −2.07; 95% CI −4.35 to 0.21, p = 0.07).28,29,31,34,35,42 There was insufficient information to pool outcomes such as oxygen saturation due to the insufficient number of trials reporting this outcome. Analysis of the only trial which tested the administration of multiple inhalations of combined treatment until a satisfactory clinical response was achieved (multiple dose flexible protocol) showed a significant decrease in the clinical score at 30–45 minutes between patients treated with salbutamol and ipratropium and those treated with salbutamol alone.20
DISCUSSION
This systematic review constitutes an effort to incorporate the best evidence available up to April 2005 on the role of inhaled anticholinergic agents added to β2 agonists in children, adolescents, and adults with acute asthma in the ED setting. New data were found which we added to previous review.3,5 Thus, 10 new randomised trials (four in children24–27 and six in adults33,34,39,41–43) with a total of 809 patients have been added, representing an increase of 22% on the previous sample. Unlike the previous reviews, this study has enabled analysis of the effect of cumulative doses, particularly in adult studies. Several important conclusions can be made. Overall, our analysis confirmed that early administration of inhaled anticholinergic agents with β2 agonists lead to a reduction in admission rates of both children and adults of 30%. Baseline severity and the intensity of the anticholinergic protocol clearly influenced the magnitude of the benefit. Thus, anticholinergic agents are particularly beneficial in patients with moderate to severe obstruction (FEV1 <70% of predicted) treated with multiple dose fixed protocols consisting of three or more doses of an anticholinergic. These patients had a reduction in the hospital admission rate of 30–45% and only 6–14 subjects need to be treated to prevent one hospital admission. This is a very relevant finding since hospital admissions count for the largest part of direct health costs for asthma in most countries, and children or adults with more severe asthma attacks are more prone to be admitted to hospital. However, this review did not identify any beneficial effects of anticholinergic agents in patients with mild acute asthma. The fact that the use of systemic CCS has not shown a significant effect is in agreement with the evidence that they require 6–12 hours to modify outcomes such as hospital admission or spirometric parameters.44,45 The short duration of the study period in all trials made it unlikely that these drugs would have a significant contribution.
Significant differences favouring the combination treatment were observed on spirometric data in both children and adults. Again, there was a dose-response relationship, with a greater benefit being achieved in patients treated with more than two doses of anticholinergic agents in combination with a β2 agonist. In adults, treatment with more than two doses produced clinically significant improvements in both FEV1 (0.44 l) and PEFR (50.5 l/min).46
In our meta-analysis we also looked at secondary outcomes and side effects but these were difficult to analyse because there was insufficient information to be pooled. A few of the studies in children reported a significant reduction in different clinical scores after combined treatment. There was no apparent increase in the occurrence of side effects such as tremor or heart rate among subjects treated with single or multiple dose protocols.
Strengths and limitations of the study
This study met most of the methodological criteria suggested for scientific reviews.47 Similar to all systematic reviews, this meta-analysis is limited by the quality and quantity of existing research and how data are reported. A comprehensive search of the published literature for potentially relevant studies was conducted using a systematic strategy to avoid bias. All of the 32 trials were randomised, and 26 were double blind. Exclusion of trials with lower methodological quality did not affect the conclusions. Assessment of the consistency of effects across studies is an essential part of the review to determine the generalisability of the findings; low values of heterogeneity (<15%) were obtained in all group and subgroup comparisons. The generalisability of study results to different countries should also be considered, particularly with regard to the hospital admission criteria. The decision to admit patients is based on many factors including past asthma and current exacerbation histories and spirometric test results, as well as clinical factors. Important variations in admission criteria could therefore influence the results. However, the results did not change when we analysed only studies with explicit criteria for admission to hospital.
REFERENCES
Footnotes
-
Published Online First 17 June 2005
-
GJR has received fees for speaking from Boehringer Ingelheim.
Linked Articles
- Correction
- Correction