Article Text

Abstract
Background: Idiopathic pulmonary fibrosis (IPF) profoundly affects the quality of patients’ lives. A systematic review was performed to evaluate critically the published literature and to examine what is known about health-related quality of life (HRQL) in patients with IPF.
Methods: The MEDLINE, EMBASE, Health and Psychosocial Instruments, and Cochrane Library databases were searched to 1 April 2004. Abstracts and bibliographies of published articles were scanned and contact was made with investigators. Included studies analysed HRQL (or quality of life) in at least 10 patients with IPF. Two reviewers independently selected studies, evaluated their quality according to predetermined criteria, and abstracted data on study design, patients’ demographic and clinical characteristics, and quality of life outcome measures.
Results: Seven studies met the inclusion criteria. The studies enrolled 512 patients with IPF and used three different instruments to measure HRQL. All studies had important limitations in methodological quality; none measured longitudinal changes in HRQL over time. Patients reported substantially impaired HRQL, especially in domains that measured physical health and level of independence. Patients with IPF appear to have similar impairments in HRQL to those with chronic obstructive pulmonary disease. Measures of dyspnoea were moderately correlated with scores from domains that measured physical health (R2 = 0.03–0.66) and energy/fatigue/pep (R2 = 0.19–0.55), but measures of pulmonary function and gas exchange did not correlate as strongly with these and other domains.
Conclusion: Studies of HRQL in patients with IPF suggest that, in addition to the obvious effect on physical health, general health, energy level, respiratory symptoms, and level of independence are also impaired. Variability in HRQL among patients is not fully explained by measures of dyspnoea or pulmonary function, suggesting that HRQL measures provide unique information. More research is needed to identify or design appropriate measurement instruments for patients with IPF and to examine changes in HRQL over time or in response to specific treatments.
- FVC, forced vital capacity
- HQOL, health-related quality of life
- IPF, idiopathic pulmonary fibrosis
- Pao2, arterial oxygen tension
- QOL, quality of life
- SF-36, Medical Outcomes Study Short Form-36
- SGRQ, St George’s Respiratory Questionnaire
- TLC, total lung capacity
- Tlco, carbon monoxide transfer factor
- UIP, usual interstitial pneumonia
- WHOQOL-100, WHO Quality of Life 100 Item Instrument
- pulmonary fibrosis
- interstitial lung disease
- quality of life
Statistics from Altmetric.com
- FVC, forced vital capacity
- HQOL, health-related quality of life
- IPF, idiopathic pulmonary fibrosis
- Pao2, arterial oxygen tension
- QOL, quality of life
- SF-36, Medical Outcomes Study Short Form-36
- SGRQ, St George’s Respiratory Questionnaire
- TLC, total lung capacity
- Tlco, carbon monoxide transfer factor
- UIP, usual interstitial pneumonia
- WHOQOL-100, WHO Quality of Life 100 Item Instrument
Idiopathic pulmonary fibrosis (IPF) is a deadly interstitial lung disease. It is the most common of the idiopathic interstitial pneumonias with a prevalence ranging from 7–20 cases per 100 000 people in the general population to perhaps as many as 175 cases per 100 000 people aged 75 years or older.1 Progressive breathlessness is the hallmark symptom and the disease commonly results in respiratory failure and death.2,3 Conventional pharmacotherapy for IPF has not been shown convincingly to improve morbidity, physiological or radiological markers of disease severity, or survival.4
Like patients with other fatal diseases, patients with IPF greatly value the quality of their lives, perhaps even more than their length of survival. Despite the substantial negative impact of IPF on most aspects of patients’ lives, research focused on quality of life in IPF has been limited. We define quality of life (QOL) as an individual’s perception of contentment or satisfaction with life in areas he or she considers important, and we define health-related quality of life (HRQL) as an individual’s perception of the impact of health (in all its many facets) on his or her quality of life.
Our objective in this systematic review was to identify and critically evaluate published studies that examined HRQL in patients with IPF. We aimed to summarise what these studies have revealed about this important outcome measure, in the hope of developing a clearer understanding of how this disease affects patients’ lives. While we recognise the important distinction between the terms QOL and HRQL, we use the term HRQL in this paper (except when referring specifically to the WHOQOL-100, a generic QOL instrument, and the studies that use it), because we are most interested in examining the impact of IPF and its treatment on quality of life.
METHODS
Study identification
Systematic methods were used to identify potentially relevant studies, assess study eligibility for inclusion, and evaluate study quality.5,6 We attempted to find all published studies examining HRQL (or QOL) in patients with IPF. One investigator, with the help of a professional medical reference librarian, searched MEDLINE, EMBASE, the Cochrane Library, and the Health and Psychosocial Instruments (HAPI) databases to April 2004. To capture additional articles we manually reviewed relevant conference proceedings, meeting abstracts, and reference lists from identified studies and pertinent review articles. Studies published in any language were potentially eligible. Abstracts were considered for inclusion only when investigators provided complete information about study methods and results.
Three search strategies were developed: one for MEDLINE and EMBASE, one for HAPI, and one for the Cochrane Library database (see Appendix A available online only at http://www.thoraxjnl.com/supplemental). We included lung transplantation as one key heading in an attempt to capture pre-transplant assessments of HRQL in patients with IPF.
Two investigators (either JJS/WGK or JJS/SSJ) independently assessed English language studies for inclusion and evaluated study methodological quality according to predefined criteria. Any disagreements were resolved by discussion. One investigator performed these tasks for non-English language studies. Two investigators (JJS and SSJ) abstracted data from studies that met inclusion criteria.
Study eligibility
We included studies that measured HRQL in at least 10 patients with IPF. Studies that enrolled patients with diagnoses other than IPF were eligible for inclusion only if the HRQL data from the IPF patients were analysed separately from non-IPF patients and the results of those analyses were reported.
Study quality
We adapted the reporting guidelines of Staquet et al7 and the methods of Efficace et al8,9 to evaluate six aspects of methodological quality: (1) IPF case definition and cohort assembly; (2) clinical characteristics of the IPF subjects; (3) HRQL instrument selection; (4) HRQL end points and instrument administration; (5) methods of statistical analysis; and (6) completeness of reporting HRQL results. The complete study quality assessment instrument is presented in Appendix B (available online at http://www.thoraxjnl.com/supplemental).
Data abstraction
We abstracted data about demographic characteristics, mode of diagnosis, physiological and radiological measures of disease severity, and co-morbid conditions. We also collected data pertaining to the role of the measurement instruments in each study, how missing HRQL data were handled, the specific HRQL results observed, and the study specific psychometric properties of each instrument.
Statistical analysis
Median values and ranges for summary statistics are reported based on information provided by each of the primary study authors. We did not attempt to pool data across studies because the number of studies was small and there was substantial heterogeneity in patient characteristics and choice of measurement instruments. An overall kappa (κ) coefficient was calculated to assess inter-rater agreement on study inclusion, and κ coefficients were calculated for each individual study to assess agreement on study quality ratings. Correlation coefficients were squared for pairwise relationships between certain clinical variables and HRQL/QOL scores, thus generating R2 values or coefficients of determination for those relationships.10 The resulting value (R2) is interpreted as the proportion of variability in one variable (such as HRQL score) that is explained by the other variable (such as forced vital capacity), regardless of the direction (positive or negative) of the correlation.11
RESULTS
We reviewed 2442 citations of peer reviewed articles and excluded 2432 after carefully reviewing their titles and abstracts. The full reports of the remaining 10 articles were examined for inclusion in the review; of these, six met our criteria for inclusion (table 1). Two studies that enrolled substantial numbers of patients with diseases other than IPF and did not provide separate data for IPF patients were excluded,12,13 together with two studies that enrolled fewer than 10 patients with IPF.14,15 We determined that one of three potentially relevant abstracts was eligible after the investigators provided complete details about study methods and results.16 We excluded an abstract of a study that enrolled several patients with usual interstitial pneumonia (UIP) patterns of lung injury because the number of patients with IPF as the cause of the UIP pattern was not specified.17 Another abstract that otherwise met eligibility criteria was excluded because the investigators did not provide complete details about study methods and results.18 For the interested reader, the results of this study are summarised in Appendix C (available online at http://www.thoraxjnl.com/supplemental).
Studies that assess HRQL or QOL in patients with IPF included in this review
Study description
Two studies measured QOL by administering the World Health Organization’s Quality of Life 100-item instrument (WHOQOL-100),19,20 three studies measured HRQL by administering the Medical Outcomes Study Short Form 36-item instrument (SF-36),21–23 and two studies measured respiratory disease-specific HRQL by administering the St George’s Respiratory Questionnaire (SGRQ).16,19,24 Further details of these instruments are shown in Appendix D (available online at http://www.thoraxjnl.com/supplemental).
Five of the studies were cross sectional in design. DeVries and colleagues19 performed a semi-qualitative study of 10 patients with moderately severe IPF. Although a formal qualitative analysis was not performed, the investigators reported findings from three focus groups. Participants in this study also completed the SGRQ and the WHOQOL-100 and discussed the merits and limitations of these instruments in the context of the focus groups. Martinez et al21 used the SF-36 to compare HRQL in 34 patients with moderately severe IPF with 34 age and sex matched control subjects. Twenty seven of the IPF patients in this study had their diagnoses confirmed by open lung biopsy and all 34 were taking daily prednisone (dose range 10–60 mg). In another study, DeVries and colleagues20 used the WHOQOL-100 to compare QOL scores from 41 patients with biopsy proven IPF with 41 age and sex matched controls. The mean carbon monoxide transfer factor (Tlco) in the IPF group was 45.3% of the normal predicted value and 14 IPF patients were using supplemental oxygen. In another cross sectional study, Martinez and colleagues assessed HRQL in 30 patients with moderately severe IPF using the SF-36.22 The mean forced vital capacity in their cohort was 61.9% of the normal predicted value and the mean arterial oxygen tension (Pao2) while breathing room air was 8.7 kPa (65 mm Hg). Twenty five of these patients had biopsy proven IPF. Nishiyama and colleagues16 evaluated HRQL in 41 consecutive patients (21 biopsy proven) with mild to moderate IPF. The mean total lung capacity (TLC) of their cohort was 78% of the normal predicted value and their mean room air Pao2 was 11.1 kPa (83 mm Hg). These investigators excluded patients from the study if they were using supplemental oxygen. Four of the cross sectional studies examined correlations between scores from the measurement instruments and various concurrently collected clinical parameters (such as dyspnoea and measures of pulmonary function). Only one of the studies was designed specifically to validate the measurement instrument in this patient population.21
Two other studies were controlled clinical trials. Douglas and colleagues23 performed a randomised prospective study at a single large tertiary referral centre. They randomly assigned 26 IPF patients (one biopsy proven) to receive either prednisone or colchicine. There was no difference between the two groups in the composite primary end point (death, significant deterioration in pulmonary function, intolerance or adverse event due to the study drug requiring cessation of treatment, addition of a second drug for the treatment of IPF, and study drop out for any reason) or in HRQL scores from the SF-36. Raghu et al24 reported the results of an international, multicentre, randomised, double blind trial of interferon γ-1b that enrolled 330 patients with IPF. Compared with placebo, interferon γ-1b did not significantly affect progression-free survival, measures of pulmonary function, gas exchange, or HRQL as measured with the SGRQ.
Characteristics of study participants
The studies included a total of 512 subjects with IPF (median 34, range 10–330). The range of mean subject ages was 58–68 years. Overall, 64% of IPF subjects were male (range 37–85%).
In six studies that provided information about the mode of diagnosis, IPF was confirmed by surgical lung biopsy in 3.8–100% of subjects. Overall, 68% (range 0–100%) of IPF subjects (N = 350) were taking oral corticosteroids. For the five studies with available data, 0–36% of IPF subjects were using supplemental oxygen (table 2).
Characteristics of included studies and their participants with IPF
Study quality
The seven studies met a mean (SD) of 46 (10)% of the predetermined quality criteria. The greatest percentage of quality criteria met by any one study was 61%. The median κ coefficient for inter-rater reliability was 0.85, indicating very good agreement between investigators on their ratings of study quality. Studies rarely met the arbitrary cut off value of at least 65% of the criteria in each of the six predefined quality domains (fig 1). Ten individual quality items were not met by any study (see Appendix E available online at http://www.thoraxjnl.com/supplemental).
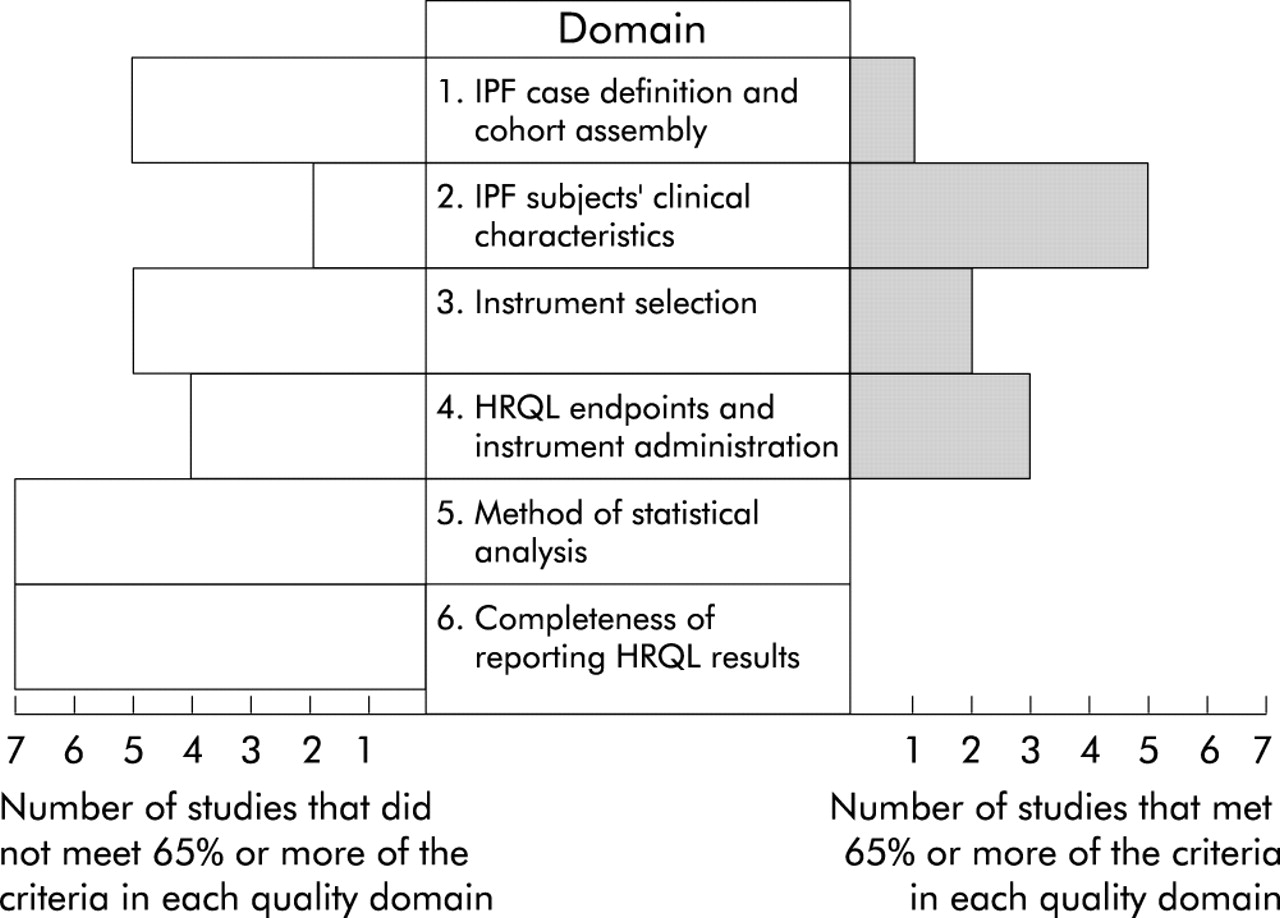
Number of studies meeting or not meeting at least 65% of the items in each of six quality domains.
Study data
Domains impacted
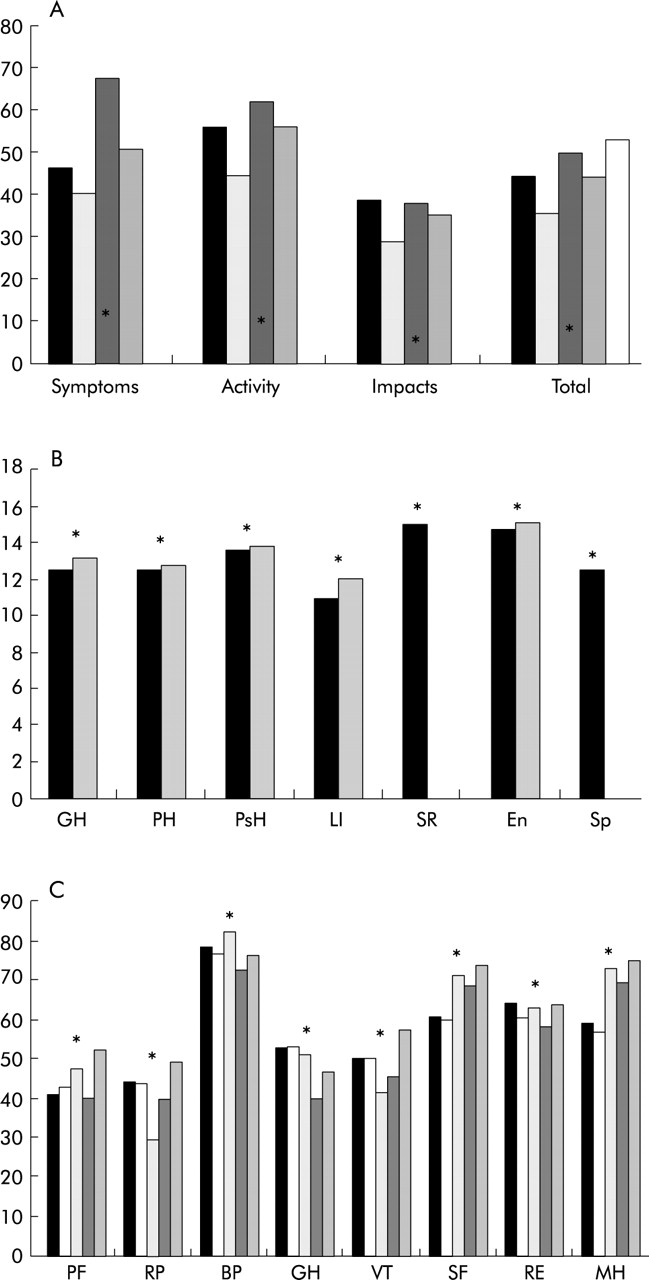
IPF patients demonstrated impaired HRQL in many life domains but physical health was most negatively impacted. Other domains that were rated consistently lower by IPF patients relative to either healthy controls or large samples of the general population included those that assessed respiratory symptoms, energy levels, and degrees of independence. For example, in one study HRQL was most impaired in the Activity domain, as measured by the SGRQ, a respiratory disease specific measure on which higher scores correspond to more impaired HRQL.19 Scores for IPF patients in this domain, which measures the physical activities that either cause or are limited by breathlessness, were markedly higher (mean (SD) 56.0 (20.2)) than scores from a general healthy adult control population (mean (SD) 11 (13)) from another study.25 In comparison to these IPF patients, subjects with milder IPF from another study16 had less severely impaired HRQL in all domains of the SGRQ; however, their scores from the Activity domain were highest and their scores from the Impacts domain were lowest. In general, SGRQ scores from patients with moderately severe IPF appear to be similar to SGRQ scores from comparably aged patients with moderately severe chronic obstructive pulmonary disease (COPD; fig 2A).25,26
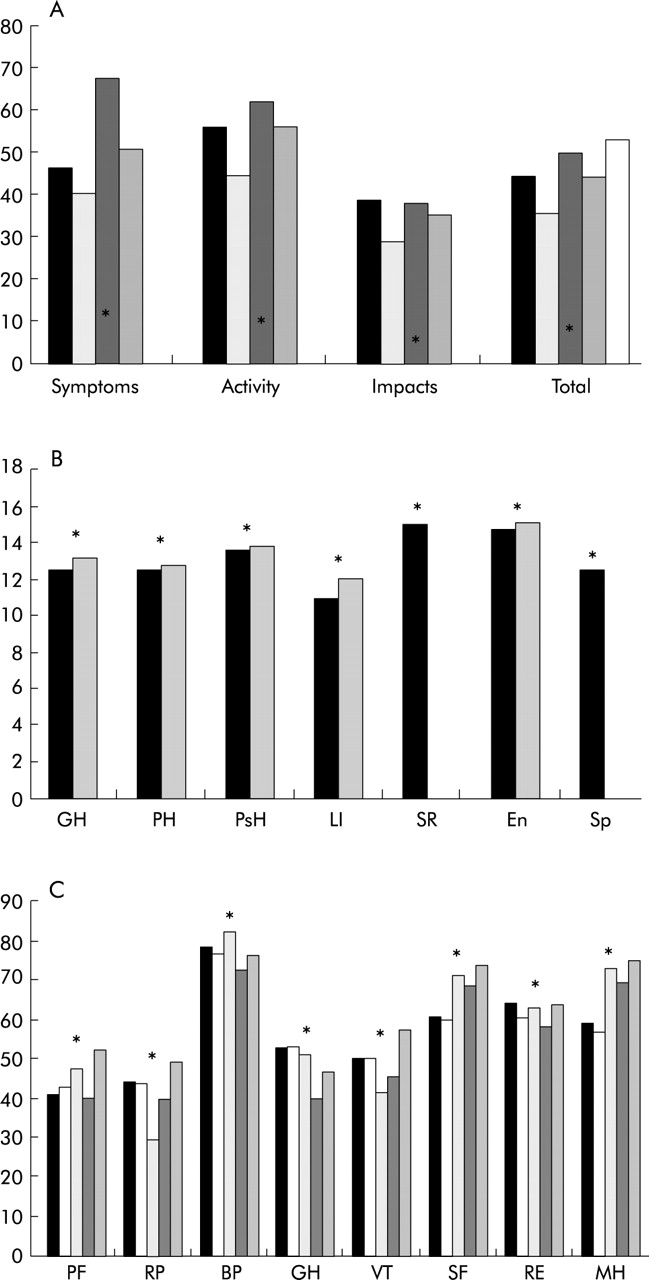
Mean SGRQ (A), WHOQOL-100 (B), and SF-36 (C) scores for IPF patients compared with referent values for patients with COPD (A and C), healthy adults (A and B), and the US adult general population (C). (A) SGRQ: black bars = mean scores for IPF patients (De Vries et al19); light grey bars = mean scores for IPF patients (Nishiyama et al16); dark grey bars = mean scores for COPD patients (ISOLDE study25); mid grey bars = final mean scores for COPD patients who took ipratropium (Dutch/Belgian Tiotropium study26); white bar = mean score for COPD patients (National Emphysema Treatment Trial, NETT30). Domain scores from the NETT trial are unpublished. *Mean scores for healthy controls in ISOLDE study.25 (B) WHOQOL-100: black bars = mean scores for IPF patients (De Vries et al19); grey bars = mean scores for IPF patients (De Vries et al20). *Mean scores from a multinational cohort of healthy adults from 15 WHO field centres that participated in WHOQOL-100 development studies.27 (C) SF-36: black bars = mean scores for IPF patients (Martinez et al22); white bars = mean scores for IPF patients (Martinez et al21); light grey bars = mean scores for IPF patients (Douglas et al23); dark grey bars = mean scores for COPD patients (ISOLDE study25); mid grey bars = final mean scores for COPD patients who took ipratropium (Dutch/Belgian Tiotropium study26). *Mean scores from US adult general population.
In another study20 IPF patients had lower scores (indicating worse QOL) than age and sex matched healthy controls on the WHOQOL-100 General Health (13.1 (3.0) v 16.5 (2.1); p<0.005), Physical Health (12.7 (2.3) v 15.9 (2.2); p<0.005), and Level of Independence (12.0 (2.9) v 17.2 (2.0); p<0.005) domains. Likewise, scores in these domains were lower for IPF patients than for a large multinational population of healthy adults (fig 2B).27
Similarly, IPF patients rated their HRQL lower than healthy controls on every domain of the SF-36 except Bodily Pain. However, the two domain scores consistently found to be most divergent from healthy controls were the Physical Functioning (PF) score which examines the limitations in physical activity imposed by health, and the Role-Physical (RP) score which examines the extent to which physical health interferes with work or other daily activities. For example, the mean PF score for the IPF patients in one study was 42.8 (4.4), the lowest of the eight SF-36 domain scores from that study, and the PF score in the control group was 43 points higher.18 In the same study the RP score for the IPF patients was 44.1 (8.11) compared with 90.4 (4.4) for the control group. In general, on the SF-36, patients with IPF rate their HRQL similar to COPD patients with comparable disease severity. Both of these disease populations rate their HRQL lower than the US adult general population in nearly every aspect (fig 2C).
HRQL and QOL scores: correlations with clinical parameters
Four studies examined the associations between HRQL (or QOL) instrument scores and results of pulmonary function tests (including arterial blood gas tensions), non-invasive measures of oxygenation, and breathlessness as measured by several dyspnoea indexes (see Appendix F available online at http://www.thoraxjnl.com/supplemental).
In general, HRQL scores correlated with pulmonary function tests in the expected directions, but many of the correlations were not statistically significant. Most correlation coefficients had absolute values of <0.4. Dyspnoea consistently correlated better with HRQL and QOL than any other disease symptom or clinical severity measure.12,20–22 The strongest correlations were between dyspnoea and domains assessing aspects of physical health (for example, the SF-36 Physical Functioning domain).
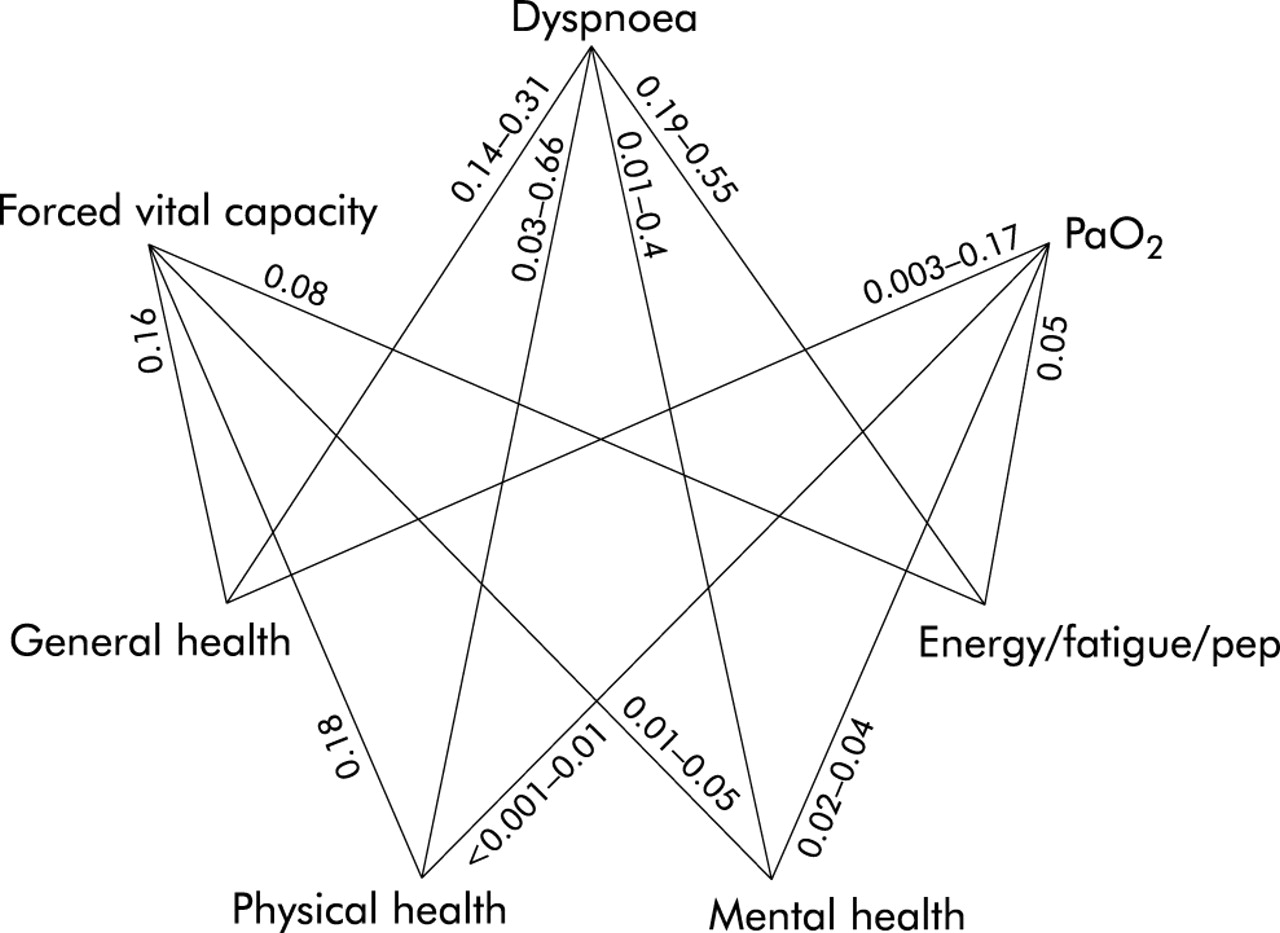
Across studies, the strongest associations were between dyspnoea and physical health (R2 = 0.03–0.66). Relative to the other pairwise associations, dyspnoea was also strongly associated with domains that assess energy, fatigue, or pep (R2 = 0.19–0.55). The association between dyspnoea and emotional health was much weaker, and the associations between either pulmonary function or oxygenation and HRQL were, in general, weaker still (fig 3).
{kind=link}
{kind=link}
{kind=link}
Coefficients of determination (R2) for associations between four domains of HRQL and three clinical parameters. The coefficient of determination represents the proportion of variability in HRQL domains explained by the given clinical parameter. Values represent the lone R2 or range of R2 values for each pairwise relationship from the studies included in this review. For General Health we included R2 values involving the SF-36 General Health domain and the WHOQOL-100 Overall Quality of Life and General Health domain; for Physical Health we included R2 values involving the SF-36 Physical Health domain, the SGRQ Activity domain, and the WHOQOL-100 Physical Health domain; for Mental Health we included R2 values involving the SF-36 Role Emotional domain, the Mental Health domain, and the WHOQOL-100 Psychological Health domain; for Energy/Fatigue/Pep we included R2 values involving the SF-36 Vitality domain and the WHOQOL-100 facet Energy and Fatigue from the Physical Health domain. Concept adapted from Curtis et al.10
HRQL and investigational drugs
Two trials that enrolled a total of 356 IPF patients met the inclusion criteria. In both of these trials the study drugs (colchicine or interferon γ-1b) did not improve HRQL.
DISCUSSION
This systematic review included seven studies that evaluated HRQL (QOL) in IPF patients. In these studies, patients with IPF were found to have impaired HRQL in nearly every life domain, but domains related to physical functioning, symptoms, and level of independence were affected most. In general—to the extent that obstructive lung disease specific instruments are capable of accurately measuring HRQL in patients with IPF, and to the extent that generic instruments are capable of accurately measuring HRQL in patients with severe diseases such as IPF or COPD—patients in comparable stages of IPF and COPD appear to have similar impairments in HRQL. Some scores from the three measurement instruments used in the studies included in this review correlated significantly and in the expected directions with selected measures of IPF severity—both physiological measures and self-report measures that involve patient perception (such as dyspnoea).
The strongest correlations were seen between dyspnoea and HRQL domains that tap overall health or aspects of physical health. The correlations between these same domains and measures of pulmonary function (FVC, Tlco) or oxygenation (Pao2) were much weaker. In fact, many of the correlations reported in these studies, including many of those that achieved statistical significance, might be considered weak in other arenas. However, the impetus for assessing HRQL is the clinical observation that patients with objectively equal physiological parameters can have very different quality of life. A very strong correlation between such parameters and HRQL scores would suggest that there is no need to measure HRQL; knowing the patients’ physiological status would suffice.
The strong associations between dyspnoea and HRQL domains that assess either overall or physical health are not surprising because a measure of an individual’s perception of something—that is, a self-report measure like his assessment of his own physical health—may tend to be more highly correlated with other perception based measures such as reported dyspnoea or with closely associated reliable functional measures such as exercise capacity (as evaluated, for example, by the 6 minute walk test) than with non-perception based measures.
The modest correlations in these studies are also not entirely unexpected because HRQL measures are not perfectly reliable. Such less than perfect reliability can impose an upper bound on the correlations with other measures, however reliable these other measures themselves may be. A labile physiological measurement at a particular point in time and a perception based measure (which generally takes into account a person’s typical circumstance over a longer time period) appear likely not to be very highly correlated by conventional standards, even if the physiological process being measured had a marked role over time in determining the perception based measure. However, assuming that non-perception based measures such as pulmonary function and oxygenation are not particularly labile measures in stable IPF patients, and that HRQL (or QOL) instruments have adequate reliability, the modest correlations observed in these studies suggest that measuring HRQL provides unique information about IPF patients that is not captured by measures of pulmonary function, gas exchange, or dyspnoea.
With regard to study quality, the scores on quality dimensions related to the adequacy of reporting of baseline demographic and clinical characteristics were higher than the scores related to HRQL instrument selection, HRQL data analysis, and HRQL results reporting. Some studies measured HRQL but did not report scores, and investigators frequently did not report their rationale for choosing the instruments used in their studies. This, of course, does not pertain to instrument validation studies since their primary goal is to support the inference that there is a sound rationale for using that instrument for a given purpose in a certain population. For all other studies, however, and particularly for drug trials, a sound rationale for choosing a certain instrument should be described. Data to support the instrument selection for a particular study should be presented, or it should be clear that the study will itself yield data capable of either providing or supplementing such support.
Very little is known about the reliability and validity of existing measurement instruments in patients with IPF. McHorney and Tarlov28 have summarised instrument measurement standards and usefulness criteria to help investigators choose appropriate instruments for their studies. Besides being brief and easily administered, a measurement instrument should have: (1) minimal floor and ceiling effects (that is, a low proportion of respondents in the target population who have scores at either the lowest possible or highest possible value); (2) acceptable internal consistency reliability and known standard errors of measurement; (3) adequate test-retest reliability and a reliable change index; and (4) validity and sensitivity to clinical change for both the population and purpose for which it is to be used. This last criterion is particularly important for studies in which HRQL is measured over time (as sometimes occurs in clinical trials), but no study has specifically addressed instrument longitudinal validity or sensitivity to change in patients with IPF.
As with any review article, the possibility of publication bias exists. However, one strength of our study—the comprehensive literature search performed with the assistance of a professional medical librarian—ensured that we captured relevant published articles. While our inclusion criteria were relatively lenient, we identified only seven eligible studies. We also identified one abstract in which investigators measured HRQL in patients with IPF, but we chose not to include in the review this incomplete report that has not undergone peer review.18 Other published studies of HRQL that enrolled patients with a variety of diffuse lung diseases including IPF did not meet our entry criteria.12–15
The paucity of data related to quality of life in IPF leaves several gaps in our understanding and provides opportunities for future research. For example, it will be important to examine the psychometric properties of existing instruments in this population and to define the most appropriate instrument to use in particular studies. Because they are developed for use in specific patient populations, disease specific instruments contain items of particular relevance and are very likely to be more sensitive to changes in HRQL over time than other instruments.29 Instruments that are sensitive to change are needed to evaluate the impact of investigational pharmacological and non-pharmacological interventions. Currently, there is no disease specific instrument to measure HRQL in patients with IPF, but one that is properly developed and rigorously tested would be expected to be more relevant and therefore more sensitive than existing generic or respiratory disease specific HRQL instruments for studies of patients with IPF.
As with any instrument, the validity of a disease specific instrument for measuring HRQL over time and its sensitivity to change can only be assessed through a longitudinal study. A longitudinal study in patients with IPF would also improve our understanding of the disease by allowing us to assess HRQL in relation to disease progression. Such a study might also enable us to determine whether and how IPF patients adapt to this disabling disease.
In conclusion, we identified seven studies that examined HRQL or QOL in patients with IPF. The studies had several limitations, including inadequately explaining the rationale for measurement instrument selection and incomplete HRQL data analysis and reporting of results. Patients with IPF have impaired HRQL in many life domains, but domains that reflect aspects of physical health are most negatively impacted. More research is needed to learn about how this disease affects patients, whether and how IPF patients adapt to their disease over time, and whether existing measurement instruments are reliable and valid for assessing HRQL over time in this patient population.
Acknowledgments
The authors thank Desmond Sjauwfoekloy for reviewing non-English language studies; Lori Nelson for helping to develop the quality criteria for included studies; Abby King for her thoughtful review of a previous version of this manuscript; and Christopher Stave for his guidance and assistance with the literature searches.
REFERENCES
Supplementary materials
The appendices are available as a downloadable PDF (printer friendly file).
If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement:
- [view PDF] - Appendices A-F.
Footnotes
-
Dr Swigris received support from an NIH training grant (T32 HL07948-01A1). Dr Gould received an Advanced Research Career Development Award from the VA Health Services Research and Development Service. The views expressed in this article are those of the authors and not necessarily the views of the Department of Veterans Affairs.