Article Text

Abstract
Background: Individuals with severely impaired lung function have an increased risk of lung cancer. Whether milder reductions in forced expiratory volume in 1 second (FEV1) also increase the risk of lung cancer is controversial. Moreover, there is little consensus on whether men and women have similar risks for lung cancer for similar decreases in FEV1.
Methods: A search was conducted of PubMed and EMBASE from January 1966 to January 2005 and studies that examined the relationship between FEV1 and lung cancer were identified. The search was limited to studies that were population based, employed a prospective design, were large in size (⩾5000 participants), and adjusted for cigarette smoking status.
Results: Twenty eight abstracts were identified, six of which did not report FEV1 and eight did not adjust for smoking. Included in this report are four studies that reported FEV1 in quintiles. The risk of lung cancer increased with decreasing FEV1. Compared with the highest quintile of FEV1 (>100% of predicted), the lowest quintile of FEV1 (<∼70% of predicted) was associated with a 2.23 fold (95% confidence interval (CI) 1.73 to 2.86) increase in the risk for lung cancer in men and a 3.97 fold increase in women (95% CI 1.93 to 8.25). Even relatively small decrements in FEV1 (∼90% of predicted) increased the risk for lung cancer by 30% in men (95% CI 1.05 to 1.62) and 2.64 fold in women (95% CI 1.30 to 5.31).
Conclusion: Reduced FEV1 is strongly associated with lung cancer. Even a relatively modest reduction in FEV1 is a significant predictor of lung cancer, especially among women.
- meta-analysis
- lung function
- lung cancer
- sex
Statistics from Altmetric.com
Lung cancer is a major public health problem worldwide. In 2000, 328 million people died from lung cancer globally.1 In Europe, 266 000 men and 64 000 women died from lung cancer in 1995.2 In the US there were over 170 000 new cases of lung cancer and more than 160 000 deaths related to lung cancer in 2004.3 This makes lung cancer the leading cause of cancer deaths in both men and women. Indeed, in the US, lung cancer causes more deaths than the next three most common cancers combined (colon cancer, n = 48 100; breast cancer, n = 40 000; and prostate cancer, n = 30 200).3
The leading cause of lung cancer is cigarette smoking. Other risk factors include exposures to certain occupational hazards, combustion generated carcinogens, and ambient radiation.4,5 Some have argued that reduced lung function is another important risk factor for lung cancer.6–8 However, several epidemiological questions regarding this relationship remain unanswered. Firstly, since individuals with reduced lung function frequently have a significant smoking history, it is not certain whether the relationship between lung function and lung cancer is real or is simply confounded by the effects of smoking. Secondly, it is not known whether the relationship between impaired lung function and lung cancer is dose dependent or threshold dependent. Thirdly, even if there is a significant relationship between these two parameters, it is not known whether sex modifies this relationship. To address these questions we conducted a systematic review and meta-analysis of population based studies of the relationship between lung function and lung cancer risk.
METHODS
Search for relevant studies
Using PubMed (1966–2004) and EMBASE databases, we conducted a comprehensive literature search to identify relevant studies published before January 2005 that examined the relationship between forced expiratory volume in 1 second (FEV1) and lung cancer. We used a disease specific search term (lung neoplasm*) combined with lung function specific search terms (FEV, FEV1, forced expiratory volume, lung function) in all our searches. The electronic searches were supplemented by scanning the reference lists from retrieved articles to identify additional studies that may have been missed during the initial search. We also contacted the primary authors of the study for clarification of data where necessary.
Study selection and data abstraction
The primary outcome of this systematic review was to compare the relative risk of lung cancer among subjects who had impaired lung function, as measured by FEV1, against those who had “normal” lung function at baseline assessment. To mitigate publication bias, we limited our search to studies that (1) were population based and did not select participants on the basis of disease; (2) employed a prospective design; (3) were large in size (at least 5000 participants at baseline); (4) used standardised methods for measuring FEV1; (5) adjusted for important confounders including age, sex, race, height, and smoking status; and (6) divided the cohort into quintiles. The latter criterion allowed us to determine the shape of the relationship between FEV1 and lung cancer.
From each relevant article two investigators (SW, WQG) abstracted the following information: first author, publication year, population sampled, sample size, lung cancer incidence or mortality, follow up time, age, sex, smoking history, FEV1, and other factors (table 1). Any questions or discrepancies regarding these data were resolved through iteration and consensus.
Baseline characteristics of included studies
Statistical methods
Quintile 5 was defined as the group with the best FEV1 and quintile 1 as the group with the worst FEV1. For the primary end point we included all incident cases of lung cancer or deaths from lung cancer, whichever were reported in the original study. There were no studies in which both of these variables were reported. A weighted mean difference technique was used to pool the original data together. The weighted mean difference was derived using an inverse variance weighted method.9 For each outcome the heterogeneity of the results across the studies was tested using a Cochran Q test. If significant heterogeneity was observed (p<0.10), a random effects model—which assigns a weight to each study based on individual study variance as well as between study variance—was used to pool the results together. In the absence of significant heterogeneity a fixed effects model was used.9 Data analysis was conducted for men and women separately and combined. All analyses were conducted using Review Manager Version 4.2 (Revman; Cochrane Collaboration, Oxford, UK).
RESULTS
The study selection process is summarised in fig 1. The electronic literature search yielded 333 citations from PubMed and 16 from EMBASE. The abstracts of these articles were reviewed for suitability. The reasons for exclusion are summarised in fig 1. In all, we identified four studies which met the inclusion and exclusion criteria and were used in the analyses.10–13 In three of these studies10,11,13 we abstracted the salient data from published reports and in the fourth12 we used the public use data files from the National Center for Health Statistics.14 The relevant baseline data from each of the selected studies are summarised in table 1 and the FEV1 data for each quintile group are summarised in table 2. In total, the analysis included 204 990 participants of whom 6185 had or died from lung cancer. The average age of the participants ranged from 42 to 47 years at baseline across the original studies. The follow up time was 9–18 years (table 1).
Lung function levels (% predicted) in quintile groups for each study

Study selection process. FEV1, forced expiratory volume in 1 second.
After adjustments for important covariates such as age, cigarette smoking, and body mass index, participants in quintile 5 (the group with the best FEV1) had the lowest risk of lung cancer while those in quintile 1 (the group with the worst FEV1) had the highest risk of lung cancer (table 3). Surprisingly, even those in quintiles 3 and 4, who had relatively well preserved lung function (mean FEV1 ∼80–100% of predicted), also had an increased risk of lung cancer. The relationship was particularly notable in women where those in quintiles 3 and 4 had risks of lung cancer that were 3.5 and 2.6 fold higher, respectively, than those in quintile 5.
Relative risk (with 95% confidence interval) of lung cancer for men and women in different quintiles of lung function
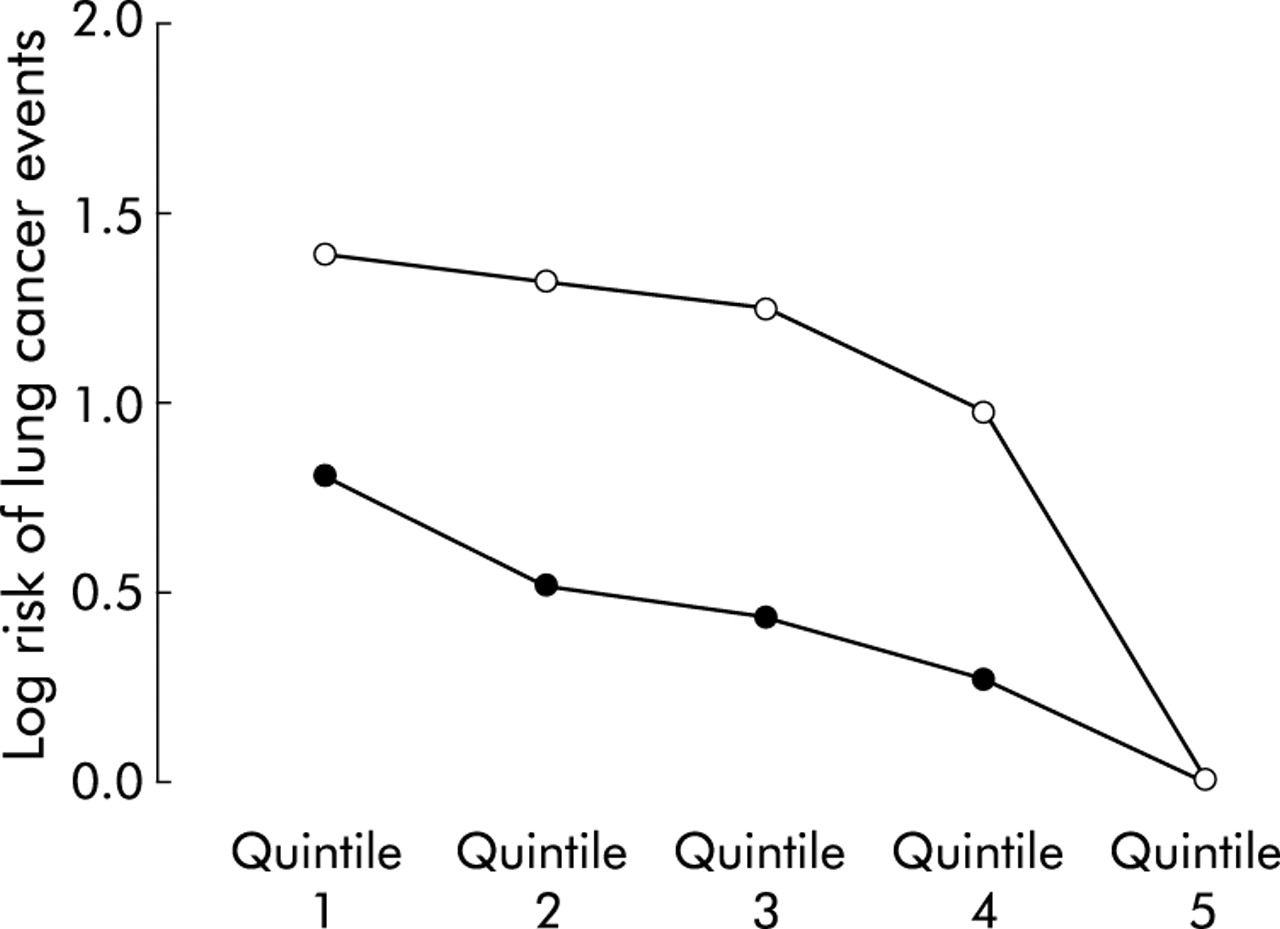
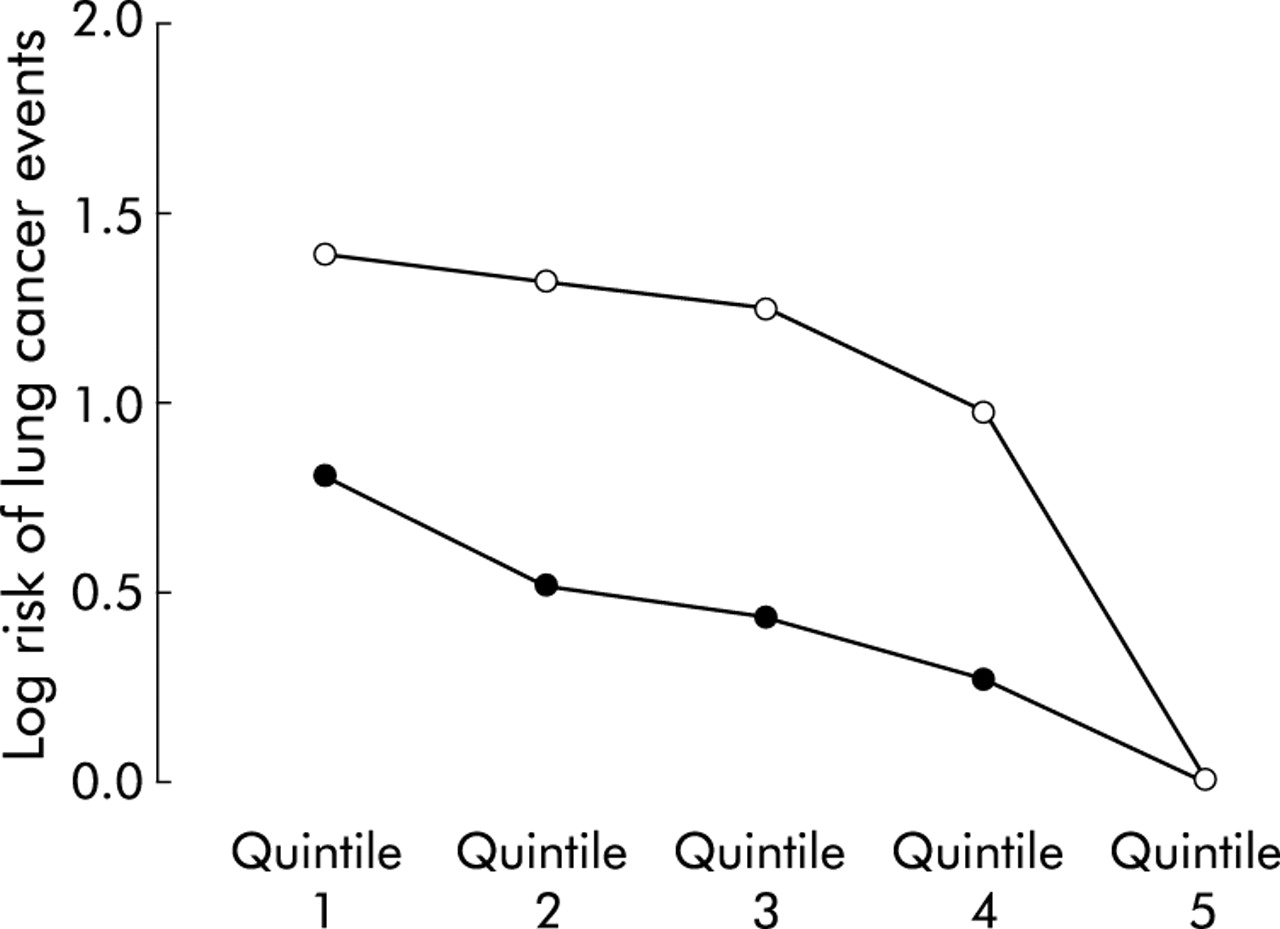
The relationship between FEV1 quintiles and the incidence of lung cancer in both men and women is summarised in table 3 and illustrated in fig 2. The slope of the relationship was significantly steeper in women than in men (p<0.001). Moreover, for every quintile, the relative risk of lung cancer was higher in women than in men. These data suggest that the effects of reduced FEV1 are amplified in women.
{kind=link}
{kind=link}
Risk of lung cancer in men and women on a natural logarithmic scale. Open circles are data for women and solid circles are data for men; p<0.001 for the comparison of slopes between men and women.
In table 4 we have summarised the remaining large epidemiological studies that evaluated the relationship between FEV1 and the risk of lung cancer. Similar to the results of the present meta-analysis, all of these studies showed that reduced FEV1 was a significant risk factor for lung cancer.7,8,15–20 These results could not be used in the meta-analysis, however, because of the marked heterogeneity in the way in which the data were collected and reported across the studies.
Published studies on the association between impaired lung function (FEV1) and the risk of lung cancer morbidity or mortality
DISCUSSION
This systematic review of population based studies which have examined the relationship between lung function and lung cancer has produced several interesting observations. Firstly, independent of cigarette smoking history, reduced FEV1 increases the risk for lung cancer in the general population. Secondly, the relationship is severity dependent such that individuals with the worst lung function have the highest risk whereas those with preserved lung function have the lowest risk. Thirdly, the relationship is alinear; relatively small differences in FEV1 which are commonly considered within the normal range (for example, from 90% of predicted to 100% of predicted) increase the risk of lung cancer by 30–60%. Fourthly, the risk appears to be amplified in women.
The finding that reduced FEV1 at baseline is significantly associated with an increased risk of lung cancer is consistent with several previous reports.7,8,15–21 Although baseline health status, degree of abnormality in lung function, and length of follow up varied considerably between the various cohorts, the associations were remarkably similar.
There are several possible explanations for a relationship between lung function and lung cancer. Firstly, the outcomes may share a causal pathway. One possible shared pathway is lung and airway inflammation which are known to correlate with the decline in lung function among smokers.22,23 Inflammation is thought to be an important mechanism responsible for the proteolytic lung destruction and small airway remodelling and narrowing which reduce lung function in smokers and in chronic obstructive pulmonary disease (COPD),22 and is also implicated in the decline in lung function in asthma24 and pulmonary fibrosis.25 Hence, reduced FEV1 may be part of the process related to lung and airway inflammation. Airway inflammation may also have a major role in the pathogenesis of lung cancer.26 Cigarette smoke and other noxious irritants incite a vigorous inflammatory reaction in the airways leading to the recruitment and activation of pro-inflammatory cells such as leucocytes which, in turn, propagate the inflammatory cascade through the release of various cytokines and reactive oxidative species.27 These latter molecules can cause oxidative damage and promote DNA mutagenesis in the surrounding lung cells.28 If the rate of cell division exceeds the rate at which reactive oxidative species related DNA damage can be repaired, DNA mutagenesis may occur and the risk for cancer increases.28 Reactive oxidative species may also directly activate various oncogenes in the surrounding cells and tissues (for example, jun and fos) which may further increase the risk of lung cancer.29 Consistent with this inflammatory hypothesis for lung cancer, the incidence of lung cancer is increased in inflammatory lung conditions such as idiopathic pulmonary fibrosis,30 asbestosis, and sarcoidosis.31 A corollary of the “shared pathogenesis” hypothesis is that the genes which impart risk for COPD and lung cancer may be common. For instance, individuals who have polymorphisms in genes which influence the oxidant/antioxidant balance in favour of reactive oxidative species may be susceptible to both.
A second possible explanation for the relationship is that the lung dysfunction secondarily enhances the risk of cancer. Individuals who have reduced FEV1 may have an impaired ability to clear inhaled carcinogens from their airways. This could lead to increased contact time between carcinogens and airway epithelial cells. However, this seems unlikely because individuals in quintiles 3 and 4 had “normal” FEV1 levels and yet had an increased risk of lung cancer.
In the present study the relationship between FEV1 and lung cancer was modified by sex. Whether women are more susceptible to lung cancer than men is controversial. Several epidemiological studies have reported data indicating increased susceptibility for lung cancer in women compared with men.32,33 However, other studies have shown the reverse, with men being more susceptible to lung cancer than women,34 while other studies have demonstrated equal susceptibility.35,36 Notwithstanding these data, there is little doubt that there are important biological and histological differences in lung cancer between women and men. For instance, in women, adenocarcinoma is by far the leading histological subtype of lung cancer whereas, in men, squamous and adenocarcinomas are equally prevalent.37 Interestingly, the contribution of cigarette smoking to the risk is less apparent for adenocarcinomas than for all other histological subtypes.38 Although lung cancer is rare in lifetime non-smokers, if it develops in these individuals it is usually an adenocarcinoma.39 Moreover, smoking cessation rapidly reduces the risk for squamous cell carcinoma while the risk for adenocarcinomas decreases much more slowly.40 In general, women have a higher frequency of GC→TA mutations41 and transversions42 in the p53 gene in resected lung tumour specimens than men, even though the level of exposure to carcinogens from cigarette smoking may be lower in women.41 Furthermore, higher levels of smoking related hydrophobic DNA adducts have been reported in the lung cancers and adjacent tissues in women.43,44 Female smokers also exhibit significantly higher expression levels of lung CYP1A1 than men.45 Increased CYP1A1 expression is important in determining individual susceptibility to lung cancer and may be a critical factor for influencing differences between sexes in levels of aromatic/hydrophobic DNA adducts in the lung.45,46 A lower DNA repair capacity in women than in men may also contribute to the variation in susceptibility between women and men.47
There are several limitations to this study. Cigarette smoking is a risk factor for lung function11,12 and lung cancer37 and could confound the relationships observed between FEV1 and lung cancer. However, all of the original studies included in the meta-analysis carefully controlled for the effects of cigarette smoking, making it unlikely that our results could be explained away by smoking. Nevertheless, we cannot fully discount the possibility of residual confounding by smoking. Secondly, we did not have data on the specific histological subtypes of cancer so the relationship between FEV1 and specific histological subtypes of lung cancer remains largely unknown, although the results of a previous study suggest that adenocarcinomas are more likely to develop in those who have small decreases in FEV1 and squamous cell carcinomas are more likely in those with severe impairment of lung function.48 Thirdly, publication bias is a concern. To mitigate this bias we chose only large population based studies. Since small positive studies are more likely to get published than small negative studies, by not including results from small studies the relative risk estimates of reduced FEV1 of the current meta-analysis may be lower than those previously published.7,17 Fourthly, most of the original studies were conducted in relatively young individuals, so the findings of the present meta-analysis may not be generalisable to the older population who develop lung cancer.
Lung cancer is the most lethal cancer in the world. The only reasonable chance for cure is to uncover the disease at a localised stage. However, patients are rarely symptomatic at early stages of disease when curative resection would be possible. Most patients present at advanced stages of the disease, so screening and early diagnosis of lung cancer are therefore imperative in reducing case fatality rates. The present study demonstrates a strong inverse relationship between FEV1 and lung cancer which applies to all levels of FEV1. The risk increases even with a relatively modest reduction in FEV1, especially among women. We found that women were approximately twice as likely to develop lung cancer as men for the same marginal decrements in FEV1. The potential clinical implication is that, in smokers and former smokers, FEV1 may provide criteria beyond age and smoking intensity to identify smokers at high risk for lung cancer; this discriminatory power of lung function testing may be important in selecting smokers for enrollment in chemoprevention and early detection trials. Furthermore, since lung cancer can occur in individuals with only small decreases in FEV1 (especially in women), the traditional boundaries of “normal” FEV1 may need to be modified for screening purposes.
REFERENCES
Supplementary materials
The correct figure for the worldwide mortality from lung cancer in 2000 is 0.85 million, not 328 million as originally stated in the article.
Footnotes
-
DDS is supported by a Canada Research Chair (Respiration) and a Michael Smith/St Paul’s Hospital Foundation Professorship in COPD.
Linked Articles
- Airwaves
- Correction