Article Text

Abstract
Background: A study was undertaken to explore the pathway to diagnosis among a group of patients recently diagnosed with lung cancer.
Methods: A directed interview study triangulating patients’ accounts with hospital and GP records was performed with 22 men and women recently diagnosed with lung cancer at two cancer centres in the south and north of England. The main outcome measures were the symptoms leading up to a diagnosis of lung cancer and patient and GP responses before diagnosis.
Results: Patients recalled having new symptoms for many months, typically over the year before their diagnosis, irrespective of their disease stage once diagnosed. Chest symptoms (cough, breathing changes, and pain in the chest) were common, as were systemic symptoms (fatigue/lethargy, weight loss and eating changes). Although symptoms were reported as being marked changes in health, these were not in the main (with the exception of haemoptysis) interpreted as serious by patients at the time and not acted on. Once the trigger for action occurred (the event that took patients to their GP or elsewhere in the healthcare system), events were relatively speedy and were faster for patients who presented via their GP than via other routes. Patients’ beliefs about health changes that may indicate lung cancer appeared to have played a part in delay in diagnosis.
Conclusion: Further investigation of the factors influencing the timing of diagnosis in lung cancer is warranted since it appears that patients did not readily attend GP surgeries with symptoms. Insight into patients’ perspectives on their experience before diagnosis may help medical carers to recognise patients with lung cancer more easily so that they can refer them for diagnosis and treatment. Encouragement to present early with signs of lung cancer should be considered alongside other efforts to speed up diagnosis and treatment.
- lung cancer
- diagnosis
- patients’ recollections
Statistics from Altmetric.com
Lung cancer remains the most common cause of death from cancer in the UK with over 33 000 deaths a year.1 No clear consensus exists over the potential for earlier diagnosis, yet UK survival rates are poor relative to some other European countries which suggests that there may be scope for improvement.2
Delay in diagnosis of cancer is recognised as an important factor in the overall outcome of treatment.3 Major efforts have been made in the UK to speed the process of referral for patients with suspected cancer by promoting early recognition of symptoms in primary care, early referral for diagnostic tests, and reducing waiting times for investigations.4 Little is known about the pathway to diagnosis for patients with cancer, and this is especially the case in lung cancer where the generally held view is that the disease is silent until it is far advanced and therefore late diagnosis is believed to be inevitable. There is evidence to suggest that avoidable delays in diagnosis occur, and these are attributable to both doctor and patient behaviour. Studies have focused on doctor delay in initiating investigations and system/hospital failures leading to treatment delay.5,6,7,8,9,10,11,12 Studies to date have relied on patient records as the source of information and therefore have not investigated the important period of time before visiting a doctor with symptoms. A recent editorial in this journal has called for continued effort to reduce delays in the diagnosis and treatment of patients with lung cancer.13
While most patients with lung cancer are identified in primary care, little information is available about how GPs respond to patients attending their surgeries with symptoms that might indicate lung cancer. There is also little to guide GPs as to how they might differentiate patients who may have lung cancer from those presenting with non-specific symptoms associated with a minor illness.14 Although symptoms of lung cancer at diagnosis are well known,15 the interrelationship between symptoms and different types and stages of lung cancer is not, nor is there information about how these arise or how patients respond to them before diagnosis.
METHODS
In this exploratory study we used directed interviews with patients recently diagnosed with lung cancer to map their pre-diagnosis symptom history and the events leading up to diagnosis. The purpose was to gather information from a group of patients with lung cancer to develop a detailed picture of the pathway to diagnosis. We wished to test the hypothesis that the symptom history and route to diagnosis of patients with operable disease differs from that of patients with inoperable disease. The intention was also to develop and test a method of collecting information from patients that could later be used in a large case-control study to establish the predictive value of symptoms recalled by patients with lung cancer by comparing these with symptoms recalled by patients with other conditions. We recognised from the outset that using patient recall as a method for gathering information on symptom history has limitations since patients with the benefit of hindsight may attribute different significance to symptoms once they know they have a cancer diagnosis. However, the approach has been used successfully to develop new insights into pre-diagnosis events in ovarian cancer as background work leading to the completion of a prospective case control study.16,17 We compared patients’ accounts with hospital and primary care records using a triangulation approach18 which combines data from interviews with data from the other sources to check patients’ recall.
Participants
A quota sample (to ensure that not less than one third of the patients had operable and therefore potentially curable disease) of 23 patients recently diagnosed with lung cancer but who had not yet started treatment were recruited from outpatient clinics in two hospitals in the South and North of England (table 1). Recruitment was audited in the main recruiting centre. All but four of the eligible patients were approached over a 3 month period (it was not possible to approach three patients for practical reasons and the fourth patient was deemed too ill). Seventeen of the 23 patients (74%) agreed to participate and 16 were interviewed (70% of patients). Eight patients were recruited from the second centre over a similar time frame. Seven patients were awaiting surgery and the remainder had inoperable disease. One patient was subsequently found to have renal cancer and was excluded from the analysis. Ethical approval was granted at each study site and all participants gave written informed consent.
Patient characteristics (n = 22)
Twenty of the patients were interviewed between 3 days and 4 weeks after diagnosis; the remaining two were interviewed between 2 and 3 months after diagnosis. Patients participating in this study share similar characteristics to the UK lung cancer population. There were slightly more women among the participants (UK male/female lung cancer incidence is 3:2). Social class distribution is broadly that reported by the Office for National Statistics.19
Interviews
Directed interviews with patients used a time line entitled “What happened to me?” to assist patients to recall key events20 dating back from being informed of their diagnosis to the first “persistent change in health status” preceding diagnosis. The first part of the interview was semi-structured using the time line as a prompt. The date, week or month when a symptom or health change was recalled and actions taken as a result by the patient were recorded as well as a description of the health change or symptom. Patients were asked to recall life events occurring at the same time such as holidays or significant family events to aid recall. Key events such as visits to a GP and other actions taken to manage health changes or symptoms were also recorded. The second part of the interview was structured and identical for all patients and was used to collect detailed information about each health change or symptom recalled. Information from patients was recorded by the interviewer onto the time line and on the interview schedule. Interviews were also tape recorded to allow more detailed qualitative analysis of descriptions of symptoms and events.
Analysis of data
Interview data were analysed to collate patients’ descriptions of the nature and number of symptoms they recalled before diagnosis. Frequency counts were made of symptoms reported during interviews and were analysed descriptively. Data were used to develop “event charts”20–22 of the pathway to diagnosis for patients; key events were:
-
first persistent symptom or change in health status recalled by the patient in the months or years preceding diagnosis (the patient may or may not have associated the symptom with lung cancer);
-
symptom or event that triggered the chain of events leading to diagnosis;
-
date when the events that led to diagnosis was initiated such as a visit to the GP;
-
date of diagnosis as recorded in the patients’ medical records.
Events recalled by patients during interviews were verified where possible using the various data sources. It was possible to pinpoint when the symptoms or health changes that ultimately led to the diagnosis of lung cancer started. Close to diagnosis (within 6 months) this could be identified to a particular week. Over 6 months and up to 24 months before diagnosis this could be identified as a particular month—for example, “in the January before I was diagnosed”. More than 2 years before diagnosis patients’ recollections were deemed insufficiently detailed to identify the timing of events and therefore were not examined. To assess the accuracy of patients’ recall, levels of agreement between patients’ accounts of key events were compared with hospital and GP records. Agreement was moderate to high (table 2) except for the number of visits to the GP before referral to a hospital specialist where one patient reported having made one visit when nine visits were recorded in the GP records. Four interview schedules were randomly selected and subject to independent verification by a second researcher by completing a second interview schedule from listening to the tape recorded interviews. Percentage agreement between these ranged from 78% to 90%; there was also close agreement on recording of symptoms and times of key events (symptoms: Cohen’s kappa coefficient 0.67–0.73, key events: Pearson’s correlation coefficient 0.72–0.8).
Accuracy of recall: patients’ accounts compared with hospital and GP records
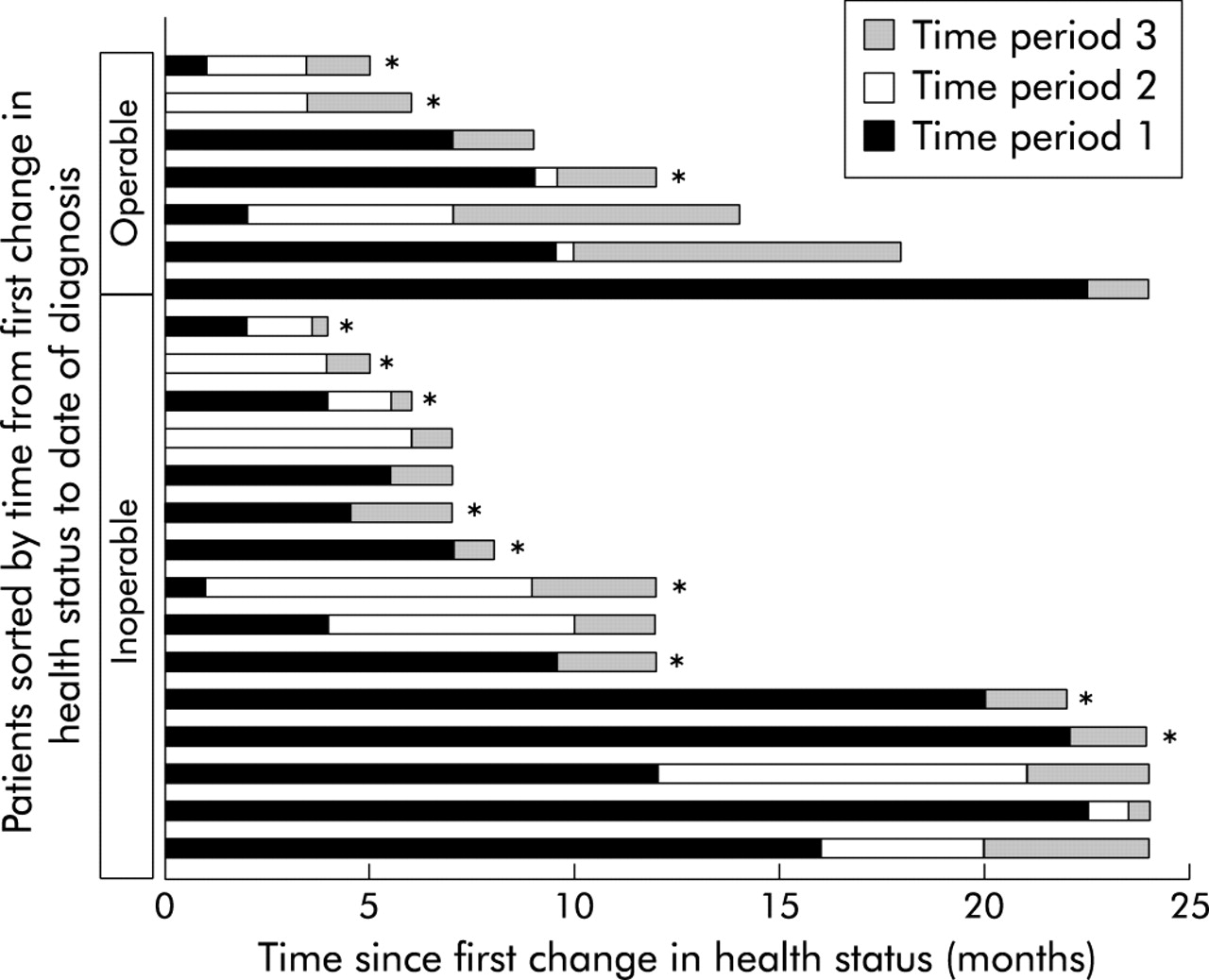
Events were plotted for each patient using interval (months before diagnosis) event charts aligned to the date of diagnosis,21 where the onset of the first recalled change in health status, the onset of the symptom that prompted the patient to visit their GP or other service, the date of contact with GP or other service, the date of diagnosis, and operability at diagnosis are presented (fig 1). Using event charts, raw data were displayed and scrutinised for all patients. The time scales between events were then summarised as median and range—for example, the time from patients’ first change in health status to diagnosis, and trigger for diagnostic investigations to diagnosis. Differences observed using event charts were then tested using the Mann-Whitney U non-parametric statistical test (table 3). Using this approach, new insights into the pathway to diagnosis in lung cancer were revealed from data derived from a small group of patients.
Symptoms recorded

{kind=link}
Interval event chart depicting the pathways to diagnosis for 22 patients with operable and inoperable lung cancer. Time period 1: time from first recalled change in health status to onset of symptom that prompted patients to visit their GP or other service and triggered events leading to their diagnosis. Time period 2: time from onset of symptom to visit to GP or other service. Time period 3: time from visit to GP or other service to date of diagnosis. Note that in some patients the onset of symptom occurred in the same month as the patient’s first recalled change in health status so no distinct time period 1 is shown. Similarly, for some patients the visit to the GP or other service occurred in the same month as the onset of symptom so there is no distinct time period 2 shown. *Diagnosed via GP rather than via another route (e.g. A&E).
Interviews were transcribed verbatim. Patients’ descriptions of symptoms and how they responded to and acted on these were then analysed thematically drawing together the language used to describe how these were experienced and acted on with the contextual information on the patient’s pathway to diagnosis. Analysis was conducted by three researchers. Researcher 1 developed the thematic framework of key findings following interviewing patients and reviewing the interview schedules; researcher 2 analysed the full transcripts and developed the interpretive analysis; and researcher 3 independently analysed the transcripts to confirm and further develop the thematic and coding structure. The findings from the separate analyses were then agreed between the three researchers.
RESULTS
A total of 30 different symptoms were experienced by patients before diagnosis. These appeared to be similar for patients who were awaiting surgery and for those with inoperable disease (table 3). Chest symptoms such as cough and breathing changes were the most common (15/22 patients) and chest or rib pain were experienced by over half the patients (12/22). Fatigue, lethargy or weakness was experienced by 14 patients and weight loss, considered to be a symptom of advanced disease, by over half the patients including four of the seven patients with operable disease. Other symptoms such as joint pain and sensory and skin changes were also reported. All the symptoms were reported as new in the months leading up to diagnosis. All patients had experienced at least one symptom before diagnosis, including one patient who was diagnosed with operable disease following a routine CT scan as part of follow up for renal cancer.
Examples of patients’ descriptions of symptoms are shown in box 1. Interviews reveal that patients often did not act in relation to changes in their health even though these were marked. Patients frequently sought to manage the problem themselves until it became too difficult and they did not (with the exception of haemoptysis) interpret changes in their health as serious or as symptoms of lung cancer. Patients experienced an accumulation of symptoms over time and these also increased in severity (table 4). Patients recalled a single symptom as leading them to consult their GP—for example, a cough that could just be “lived with no longer” even though several other symptoms may have been experienced concurrently. The pattern of symptoms and events over the months leading up to diagnosis appeared remarkably similar for patients with inoperable disease and for patients awaiting surgery for lung cancer.
Number of symptoms at key events
Box 1 Examples of patients’ descriptions of symptoms experienced before diagnosis
Cough
“I had a cough that you couldn’t resist, so you would cough in the middle of speaking. And I thought this was one of those coughs you were getting which might go away. So I didn’t do anything about it for months.”
(Patient no 5: cough was first change in health status recalled, started 6 months before diagnosis; first visited GP with cough and weight loss 6 weeks before eventual diagnosis of inoperable non-small cell lung cancer)
Shortness of breath/breathing changes
“… if I’d done my shopping, like Catch-22, I’d bring it in then I was sort of out of breath … before I put my shopping away, I’ll have a cigarette break … So I was stopping more, but the more I stopped the more I smoked. So it was a vicious circle.”
(Patient no 21: shortness of breath and chest pains were the first changes in health status recalled, started 12 months before diagnosis. First visited GP with change in bowel habit 10 weeks before diagnosis of inoperable non-small cell lung cancer)
Chest pain
“It was my stepson’s wedding anniversary… I could feel what I thought was wind, you know at the centre of my chest, and it started getting, you know, a little bit painful … then it moved a little bit to the side … two, three months passed and I thought ‘that’s a hell of a lot of pain for wind’ you know. Then it was round my back and the pain was getting severe, really severe. And eventually I went to the doctor.”
(Patient no 17: chest pain was the first change in health status recalled, started 7 months before diagnosis. First visited GP with chest pain 4 weeks before diagnosis of inoperable non-small cell lung cancer)
Tiredness
“I noticed that when I was playing golf … I was finding it difficult to finish a round in good shape, and it became evident I couldn’t play golf two days running … I think there were probably signs of it a year before … because I could come home after a round of golf, particularly if it was a long round, say 4 hours, I could come almost straight in, sit down and go to sleep.”
(Patient no 11: tiredness was the first change in health status recalled, started 18 months before diagnosis. First visited GP with tiredness 7 months before diagnosis of operable non-small cell lung cancer)
Weight loss
“I suppose the biggest worry I had was weight loss really, as opposed to lethargy – because it suddenly dropped 10 pounds without any obvious reason.”
(Patient no 11: tiredness was the first change in health status and the reason for visiting GP 7 months before diagnosis with operable non-small cell lung cancer)
Haemoptysis
“I had what I thought was a cold and I spat up some blood one morning…, which then I said ‘right I’ll see the doctor’.”
(Patient no 1: first change in health status recalled was shortness of breath which started more than 2 years before diagnosis. First visited GP immediately after experiencing haemoptysis 2 months before diagnosis with inoperable lung cancer, histology unknown)
To identify sources of delay in diagnosis the pattern of symptoms recalled by patients was examined along side key events such as the timing of their visits to the GP and the date of diagnosis. Symptoms were recalled as having started between 4 months and more than 2 years before diagnosis (median 12 months), suggesting that delay was a factor in patients’ pathway to diagnosis (table 5). To identify sources of delay a distinction was made between symptoms recalled by patients and the symptom or event that was identified as the thing that made patients act. A median of 7 months elapsed between first recalled change in health status and the onset of the symptom that prompted the patient to act. The symptom that acted as the trigger for events leading up to diagnosis was recalled as having occurred between 2 weeks and 8 months (median 2 months) before diagnosis. The close proximity of the trigger—that is, when patients acted on the symptom by visiting their GP, for example—and diagnosis suggests that the process of referral for diagnostic investigations was, for most, rapid. Although patients perceived the response to their symptoms was speedy, half (11/22) of the patients recalled having symptoms for over a year before this, again suggesting considerable delay by patients.
Time between key events and date of diagnosis for 22 patients with operable and non-operable lung cancer
Twelve of the patients presented via their GP. For the remaining 10 the pathway to diagnosis was via other services and, for the latter, the total length of the pathway was longer (median 7.5 months vv 16 months; p = 0.04, Mann-Whitney U test). Three patients were diagnosed as an inpatient, one was diagnosed following attendance at an accident and emergency department, three were initially referred to an elderly care facility, and three were referred to another specialist (one cardiology, one urology, one gastroenterology). It is difficult to judge from the data whether the symptoms of the patients diagnosed via other services differed from those who presented via there GP, although this may have been the case.
For most of the patients, there was little or no contact with the GP over the period of time between the first change in health status and the trigger for diagnosis. A median of 3 (range 0–6) visits to the GP occurred before a referral was made to a hospital consultant. For the 10 patients where information was available on all visits to the GP surgery in the 2 years preceding diagnosis, six had made very infrequent visits (one patient had not seen a doctor for 30 years). The remaining four patients made regular visits to their GP because of a chronic health problem such as hypertension.
Interview transcripts reveal that patients did not appear to associate changes in their health with the possibility that they might be ill. Illness was only considered as a possibility by patients when it was forced upon them because of the severity of their symptoms. Despite the fact that all but one of the patients were current or former smokers, it appeared that symptoms such as breathing changes, cough, chest pain, weight loss, or profound fatigue were not associated with the possibility that these might be symptoms of lung cancer. Symptoms were instead attributed to everyday causes such as “getting older” or the problem was not considered serious enough to warrant medical attention. Haemoptysis was a symptom that prompted a more immediate response and was acted on immediately by three patients who experienced coughing up frank blood. However, there is no suggestion that these individuals thought that they had cancer—for example, one patient believed he had TB. Ten of the participants (45%) had given up smoking in the 12 months before diagnosis. Evidence from the interview transcripts suggests that this was a response to ill health—in the context of the symptoms patients were experiencing there was a point when they could no longer tolerate smoking. There is evidence in patients’ accounts of a lack of expectation of the right to be treated actively or promptly—for example, one patient said: “You hear people talk about smokers – ‘you don’t get the same treatment or whatever’. It’s true that’s what people say. I suppose that was one of the reasons that I expected my doctor might say to me ‘well you are a smoker—look after yourself’.” A consequence of anti-smoking campaigns may be that people who smoke feel undeserving of medical care and this may have played a part in the apparent reluctance in seeking help for the symptoms that patients experienced.
DISCUSSION
This study has limitations due to the small number of patients participating and we recognise that patient recall is problematic as a source of data on symptoms. If it had been feasible, a prospective study would have been preferable. The symptoms recalled by patients also need to be tested with other groups of patients to determine if they are related to lung cancer or can reflect other changes or experiences of ill health.
Our findings, although preliminary because of the limitations of the study, suggest that the widely held view that lung cancer is silent until far advanced may be inaccurate. Patients in this study recalled having symptoms for many months before their diagnosis, regardless of their disease stage once diagnosed. Not all patients had chest symptoms. Other systemic symptoms such as lethargy, weakness, fatigue, weight loss, and change in eating habits were also experienced, even in those with operable disease. Patients’ descriptions of their symptoms before diagnosis differ from those listed in guidance for GPs on suspected cancer.4 Importantly, with the exception of haemoptysis, symptoms reported as marked changes in health were not generally interpreted as serious by patients at the time and no action was taken. Using event charts, it was possible to distinguish between patient delay and GP delay over the pathway to diagnosis. Once the trigger for action occurred—that is, the event that took patients to their GP or elsewhere in the healthcare system—events were, with the exception of three patients, relatively speedy and this was faster for patients who presented via their GP than via other routes. This finding may indicate that GPs have responded to recent guidance4 over early referral for patients with symptoms that might indicate cancer. Although previous studies have indicated that delays may occur due to GP and system failure, this is the first study to highlight patient delay as an important factor that has received little attention to date.6,7
It is recognised that lung cancer has been under researched.23 One reason is the difficulty of conducting research with people who have such a poor life expectancy and who may be very ill. Our study has revealed some new insights into the months preceding diagnosis that may be useful in examining the question of whether earlier diagnosis may be achieved and warrants further detailed investigation. It indicates that even small scale work may be of value in addressing challenging health problems.
It would seem that developing greater understanding of how people respond to changes in their health, especially when these are a prelude to a disease that holds very negative connotations—as in the case of lung cancer—could be used to inform the development of strategies to promote earlier diagnosis. The pathways to diagnosis that we have identified point to the need for different approaches to public health, whereby people at risk (smokers and former smokers) are encouraged to be more conscious of their health and to the possibility that they may develop lung cancer. The apparent acceptance of their symptoms by people with lung cancer suggests that there may be a role for public education about the key symptoms. If successful, this might lead to earlier presentation, faster diagnosis, and better outcomes.
REFERENCES
Footnotes
-
This work was undertaken by researchers from the University of Southampton who received funding from the Department of Health. The views expressed in the publication are those of the authors and not necessarily those of the Department of Health.
-
Competing interests: none
-
The study guarantor is Professor Jessica Corner.
-
All authors are independent from the Department of Health Policy Research programme who commissioned this study.