Article Text

Abstract
Background: Combined treatment with inhaled corticosteroids and long acting β2 agonists is approved for the treatment of chronic obstructive pulmonary disease (COPD), but little is known about the onset of effect of the combination.
Methods: Data were used from 1465 patients with COPD entered into a large 1 year double blind trial with daily measurements of peak expiratory flow (PEF) and symptom scores.
Results: PEF was significantly higher after 1 day in patients treated with salmeterol 50 μg twice daily or the salmeterol/fluticasone propionate combination 50/500 μg twice daily than placebo. In patients treated with fluticasone propionate 500 μg twice daily alone, PEF differed from placebo after 2 days. The differences after 2 weeks compared with placebo were 16 l/min (95% confidence interval (CI) 11 to 21), 11 l/min (95% CI 6 to 16), and 27 l/min (95% CI 22 to 33) for salmeterol, fluticasone propionate, and the salmeterol/fluticasone propionate combination, respectively. For all treatments the effect on PEF after 2 weeks was comparable to that seen at the end of the study. The difference between the salmeterol/fluticasone propionate combination and placebo after 2 weeks as a percentage of baseline was similar for PEF and clinic forced expiratory volume in 1 second (FEV1). Differences in breathlessness scores were statistically significant after 1 day for the group treated with salmeterol alone and after 2 days for the combination group. The 2 week change in FEV1 was only partly indicative of a long term response in individual patients.
Conclusions: The effects of salmeterol and fluticasone propionate, alone or in combination, on PEF and breathlessness are seen within days and most of the obtainable effect on these parameters is reached within 2 weeks.
- chronic obstructive pulmonary disease
- inhaled corticosteroids
- long acting beta agonists
- breathlessness
- lung function
Statistics from Altmetric.com
- chronic obstructive pulmonary disease
- inhaled corticosteroids
- long acting beta agonists
- breathlessness
- lung function
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines for chronic obstructive pulmonary disease (COPD) recommend treatment with both inhaled corticosteroids and long acting bronchodilators for patients with moderate to very severe COPD with a history of exacerbations.1 These recommendations are based on an increasing number of large controlled trials lasting 6–36 months. The effects of inhaled corticosteroids are mainly due to a decrease in the number of exacerbations and a slowing down in the decline in health status;2–4 to date, little attention has been focused on whether an initial improvement in lung function provides symptomatic benefit, in particular a decrease in breathlessness. Long acting bronchodilators lead to an increase in lung function and fewer symptoms, as shown in several studies.5–9 In spite of the increasing evidence of efficacy of these treatments, little is known about how quickly their effects become evident. Drug action is conventionally thought to have a relatively rapid onset of effect in patients with bronchial asthma, but little is known about what happens in COPD and whether addition of an inhaled corticosteroid has any effect. In the recently published TRISTAN trial there seemed to be a rapid onset of effects of treatment with salmeterol and fluticasone propionate as well as the combination of these drugs.10 Similar fast effects were seen for formoterol and budesonide.11
We hypothesised that a large study like the TRISTAN trial would have sufficient statistical power to detect the time of onset of an effect of the individual drugs on lung function and possibly on breathlessness. To study this, we used diary card information on both daily peak expiratory flow (PEF) measurements and symptom assessments obtained during the immediate post-randomisation phase of the TRISTAN trial.
METHODS
The methods of the TRISTAN trial have been published previously.10 Briefly, it was designed to compare the efficacy of a salmeterol/fluticasone propionate combination (50/500 μg twice daily) with salmeterol alone (50 μg twice daily), fluticasone propionate alone (500 μg twice daily) and placebo, and to compare safety of all treatment groups. Inclusion criteria were COPD (ERS definition), age 40–79 years, >10 pack-years, pre-bronchodilator forced expiratory volume in 1 second (FEV1) 25–70% predicted, FEV1/forced vital capacity (FVC) <70%, poor short term reversibility (<10% predicted FEV1 30 minutes after inhaling 400 μg salbutamol), and chronic bronchitis with exacerbations in the last 3 years.
Patients with a current diagnosis of asthma, eczema, allergic rhinitis, use of systemic steroids, antibiotics, or change in COPD medication during the last 4 weeks were excluded. Patients could continue medications like short acting bronchodilators, acetylcysteine, and sodium cromoglycate provided the treatment was kept unchanged during the study; oral corticosteroids and/or antibiotics could be given in short courses for exacerbation treatment. Oral short acting β2 agonists, other inhaled corticosteroids, other long acting β2 agonists, and combination bronchodilators (Combivent, Berodual, Duovent) were not allowed.
The analysis was designed to identify the point at which a treatment effect was first observed in the three treatment arms of the study. Each morning patients recorded in their daily record cards the highest of three PEF values measured with a mini-Wright peak flow meter before taking any medication. They also recorded use of relief albuterol, symptom scores, and number of night-time awakenings in the previous 24 hours. Breathlessness was scored as 0 (none) to 4 (breathless at rest). We limited the period of analysis to the first 14 days after starting study medication. Clinic FEV1 was measured at randomisation, after 2 weeks, and at seven further visits for the remaining 50 weeks.
Statistical methods
The analysis of PEF on days 1–14 was performed using repeated measures analysis of covariance (ANCOVA) which controlled for multiple testing. Smoking status, age, sex, baseline lung function, and country were included in the model as covariates, day was specified as a categorical variable, and a treatment × day interaction term allowed the effect of treatment to differ at each day. Breathlessness scores on each of days 1–14 were analysed using a proportional odds model for ordered categorical data. In this model an odds ratio (OR) for a given treatment describes the likelihood of patients on this treatment experiencing a one step improvement in breathlessness compared with patients on placebo. An OR of 1.5 for a given treatment would mean that the odds of a patient experiencing a one point improvement is 50% higher on this treatment compared than what the patient would experience on placebo. Both models included the covariates of smoking status, age, sex, and baseline symptom score. Clinic FEV1 was analysed using repeated measures ANCOVA. Correlations between change in PEF and FEV1 were analysed using Spearman correlation coefficients. Drop outs in the first 2 weeks were excluded from analyses. All confidence intervals (CI) cover 95%.
RESULTS
The TRISTAN trial was conducted at 196 centres in 25 countries and recruited 1974 patients of whom 1465 received treatment. Demographic data, baseline characteristics, and compliance did not differ between treatments whereas withdrawals were significantly less frequent in all three active treatment arms than in the placebo group. Table 1 shows the baseline characteristics for the four treatment arms for the variables of interest in the present analyses.
Baseline characteristics of the study population
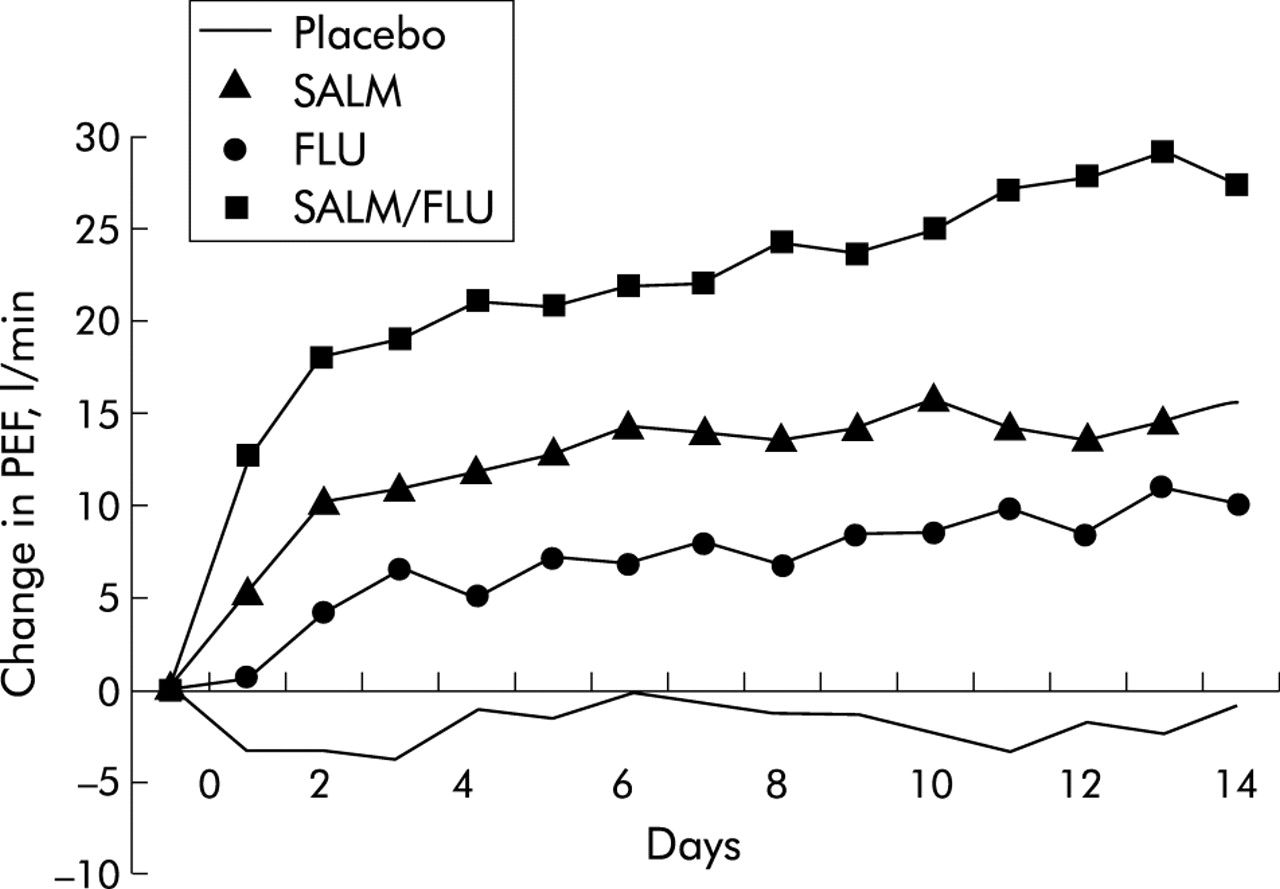
A total of 75 patients (3.9%) dropped out of the study in the first 2 weeks. Figure 1 shows changes in PEF from baseline in the first 2 week period. It can be seen that the PEF differed between the days (p<0.001) and also between the treatments (p<0.001). Moreover, the difference between the treatments was not constant over the 14 days (days × treatment interaction p = 0.002). For salmeterol and the salmeterol/fluticasone propionate combination, PEF was significantly higher than placebo after 1 day (p<0.001 for both), for fluticasone propionate this was the case after 2 days (p<0.001). After 2 weeks the difference between placebo and salmeterol, fluticasone propionate, and the salmeterol/fluticasone propionate combination was 16 l/min (95% CI 11 to 21, p<0.001), 11 l/min (95% CI 6 to 16, p<0.001), and 27 l/min (95% CI 22 to 33, p<0.001), respectively. The change in the combination treatment group was significantly better than all other treatment groups after 1 day: difference between this group and salmeterol group was 7 l/min (95% CI 3 to 12, p<0.001); for the fluticasone propionate group the difference was 12 l/min (95% CI 8 to 16, p<0.001). As shown in fig 1, the PEF had not quite reached a plateau in the three treatment groups after 2 weeks. Over the entire 52 weeks of treatment the difference between placebo and salmeterol, fluticasone propionate, and the salmeterol/fluticasone propionate combination was 15 l/min (95% CI 10 to 20), 13 l/min (95% CI 8 to 19), and 32 l/min (95% CI 26 to 37), respectively.

{kind=link}
Changes in mean peak expiratory flow (PEF) in the four treatment arms in the first 2 weeks after randomisation.
The effect of treatment on breathlessness was measurable slightly later, as shown in table 2 where effects after 1, 2, and 14 days are shown. After 2 weeks the change in the combination treatment group was significantly better than all other treatment groups; OR for improvement compared with the salmeterol group was 1.4 (95% CI 1.0 to 1.9, p = 0.035) and compared with the fluticasone propionate group the OR was 1.7 (95% CI 1.3 to 2.3, p<0.001). Comparable effects were found for cough and night awakenings but not for the phlegm scores (data not shown).
Effects of treatments on breathlessness
Within the first 2 weeks clinic FEV1 also improved significantly. The improvement compared with placebo was 61 ml (95% CI 28 to 94, p<0.001), 41 ml (95% CI 8 to 74, p = 0.016), and 147 ml (95% CI 113 to 181, p<0.001) for the salmeterol, fluticasone propionate, and salmeterol/fluticasone propionate combination, respectively. Compared with the effect of treatment at week 52, the initial improvement represented 113%, 79%, and 94%, respectively, of the overall effect. Due to the large number of measurements, the change in FEV1 at 14 days was significantly correlated with the change in PEF at 14 days (p<0.0001), but with a small r value (r = 0.23).
After 2 weeks the mean FEV1 had increased in all four groups; the increase was 16 ml in the placebo group, 76 ml in the salmeterol group, 55 ml in the fluticasone propionate group, and 163 ml in the salmeterol/fluticasone propionate combination group. Table 3 shows median, 25th and 75th percentiles for the increase in FEV1 in each of the four treatment groups after 2 and 52 weeks. In order to see if the change at week 2 predicted long term change, we looked at patients in the highest quartile in each of the treatment groups after 2 weeks; for this analysis only those who completed 52 weeks of treatment were included. Table 3 shows the change in FEV1 after 2 and 52 weeks expressed as median, 25th and 75th percentiles. For the salmeterol/fluticasone propionate combination group the 75th percentile was 280 ml, a substantial increase. After 52 weeks 55% of those initially in this highest quartile remained in the upper quartile and 74% were in the upper two quartiles—that is, they had an increase in FEV1 at 52 weeks of 80 ml or more. The comparable percentages remaining in the highest quartile and upper half did not differ markedly for the other groups although their actual change in FEV1 was, of course, smaller than in the combination treatment group. Conversely, in the salmeterol/fluticasone propionate combination group only 8% of those initially in the highest quartile ended up in the lowest quartile after 52 weeks and 10% moved from the lowest quartile to the highest within a year.
Change in FEV1 (in ml) after 2 and 52 weeks in each of the four treatment groups expressed as median, 25th and 75th percentiles
DISCUSSION
There is increasing recognition that studies of 1 year or more are needed to evaluate properly the effect of treatment in COPD,3,10,11 but little is known about how quickly treatment works in COPD and whether combining treatments influences the speed of onset of action. In this study we report a rapid onset of action of treatment with salmeterol and a salmeterol/fluticasone propionate combination and, to some extent, with fluticasone propionate alone. The effects of treatment on PEF were apparent within a few days and comparable to the final effects of treatment. Scores for breathlessness also improved quickly and treatment effects were apparent within 2 days in this disease hitherto considered unresponsive.
An effect of salmeterol on lung function in COPD has previously been shown to be apparent within 2 hours of the first dose,12 and the time to onset of the bronchodilator effects in COPD does not differ substantially from that seen in asthma. The changes in PEF we report at 24 hours are identical to those seen in a smaller population of similar severity.13 It is, however, surprising that the effects of fluticasone propionate either alone or when combined with salmeterol become apparent within 1–2 days of treatment. A recent study comparing the effect of formoterol alone or in combination with budesonide within 60 minutes of inhalation14 found a more rapid bronchodilatation from formoterol when given together with budesonide. Because of the short time span, the authors ascribed this to non-genomic effects. It is unclear if this very early effect which was not sensed by the patients relates to our findings. Changes in PEF were mirrored by changes in FEV1 seen after 2 weeks at the first measurement made after randomisation;10 this was seen in all three treatment arms. This initial increase in FEV1 after 2 weeks was similar to the initial change seen in EUROSCOP,15 the estimated change in the statistical modelling used in ISOLDE,2 and in the recent study by Szafranski et al.11 However, no initial effect was seen in the Copenhagen City Lung Study16 or the Lung Health Study,4 so differences in severity of COPD are unlikely to be the sole explanation.
The FEV1 is the standard measure of airway function in COPD1 and most treatments in COPD have been evaluated using FEV1 as the effect parameter. PEF may have more limitations but has a predictive power comparable to that of FEV1 in COPD.17 In this study we have shown statistically significant changes in PEF which at first sight appear to be small. However, the changes seen in these analyses are not small. The proportional changes from baseline were comparable to those seen in FEV1. Changes of 15–30 l/min are not different from changes seen when comparing inhaled corticosteroids with placebo in mild stable asthma; in a recent Cochrane review the mean increase in chronic asthma for fluticasone propionate compared with placebo was 29–49 l/min depending on dose.18 In this study, however, we were able to study changes in FEV1 after 2 weeks as well. We looked at these changes and tried to determine whether the initial change could predict changes after 1 year. Although not all initial responders had a sustained benefit, there was a strong tendency for the initial response to be related to sustained improvement. Given the variation in the measurement of FEV1, a weak association was to be expected. It seems unlikely that the initial response using any lung function measure or biomarker is able to fully identify long term benefits and the notion of a single dichotomy “responder/non-responder” is not biologically plausible. Initial response is only one of the parameters the patient and clinician can use to establish if long term treatment is desirable. This is similar to the situation for many treatments in chronic diseases.
Lung function, however closely linked to our understanding of the natural history of COPD, is a surrogate marker. The core symptom of COPD is breathlessness and our measurements of breathlessness were obtained using a simple diary card score. This methodology has not been validated in terms of the significance of differences in score, but is a valid method of identifying the time points at which changes in breathlessness occurred and for making comparisons between treatments in terms of the point at which differences occurred. In a previous study, changes in lung function in COPD patients after salmeterol were paralleled by reductions in the intensity of dyspnoea occurring within 120 minutes of the first dose.12 The most likely mechanism was an increase in inspiratory capacity and the most favourable response was seen in patients who had a reduction in FEV1 comparable to that in our study population. The bronchodilator induced lung deflation obtained with salmeterol also increases exercise endurance.19
In conclusion, these analyses have shown that combination treatment with an inhaled corticosteroid and a long acting β agonist can provide benefits within days. That mean improvement is sustained over the subsequent year.
REFERENCES
Footnotes
-
↵† Deceased.
-
Funding for this study (protocol number SFC3024) was provided by GlaxoSmithKline.
-
Presented at the 2003 American Thoracic Society Annual Congress in Seattle, USA.
-
Salmeterol/fluticasone propionate combination™, Advair™, and Diskus™ are trade names belonging to the GlaxoSmithKline group of companies.