Article Text

Abstract
Background: Thoracic gas compression (TGC) exerts a negative effect on forced expiratory flow. Lung resistance, effort during a forced expiratory manoeuvre, and absolute lung volume influence TGC. Lung volume reduction surgery (LVRS) reduces lung resistance and absolute lung volume. LVRS may therefore reduce TGC, and such a reduction might explain in part the improvement in forced expiratory flow with the surgery. A study was conducted to determine the effect of LVRS on TGC and the extent to which reduced TGC contributed to an improvement in forced expiratory volume in 1 second (FEV1) following LVRS.
Methods: The effect of LVRS on TGC was studied using prospectively collected lung mechanics data from 27 subjects with severe emphysema. Several parameters including FEV1, expiratory and inspiratory lung resistance (Rle and Rli), and lung volumes were measured at baseline and 6 months after surgery. Effort during the forced manoeuvre was measured using transpulmonary pressure. A novel method was used to estimate FEV1 corrected for the effect of TGC.
Results: At baseline the FEV1 corrected for gas compression (NFEV1) was significantly higher than FEV1 (p<0.0001). FEV1 increased significantly from baseline (p<0.005) while NFEV1 did not change following surgery (p>0.15). TGC decreased significantly with LVRS (p<0.05). Rle and maximum transpulmonary pressure (TPpeak) during the forced manoeuvre significantly predicted the reduction in TGC following the surgery (Rle: p<0.01; TPpeak: p<0.0001; adjusted R2 = 0.68). The improvement in FEV1 was associated with the reduction in TGC after surgery (p<0.0001, adjusted R2 = 0.58).
Conclusions: LVRS decreased TGC by improving expiratory flow limitation. In turn, the reduction in TGC decreased its negative effect on expiratory flow and therefore explained, in part, the improvement in FEV1 with LVRS in this cohort.
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- LVRS, lung volume reduction surgery
- NFEV1, FEV1 obtained using no compression method
- absolute DFEV1, NFEV1 − FEV1
- percentage DFEV1, absolute DFEV1/FEV1
- PEF, peak expiratory flow
- Pel, elastic recoil pressure at TLC/TLC
- Rle, expiratory lung resistance
- Rli, inspiratory lung resistance
- RV, residual volume
- TGC, thoracic gas compression
- TLC, total lung capacity
- TPpeak, peak transpulmonary pressure during a forced expiratory manoeuvre
- lung volume reduction surgery
- thoracic gas compression
- chronic obstructive pulmonary disease
- lung mechanics
Statistics from Altmetric.com
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- LVRS, lung volume reduction surgery
- NFEV1, FEV1 obtained using no compression method
- absolute DFEV1, NFEV1 − FEV1
- percentage DFEV1, absolute DFEV1/FEV1
- PEF, peak expiratory flow
- Pel, elastic recoil pressure at TLC/TLC
- Rle, expiratory lung resistance
- Rli, inspiratory lung resistance
- RV, residual volume
- TGC, thoracic gas compression
- TLC, total lung capacity
- TPpeak, peak transpulmonary pressure during a forced expiratory manoeuvre
- lung volume reduction surgery
- thoracic gas compression
- chronic obstructive pulmonary disease
- lung mechanics
Chronic obstructive pulmonary disease (COPD) is a progressive and debilitating disease. Expiratory flow limitation is the hallmark of COPD. Lung elastic recoil pressure, frictional pressure loss upstream of the choke point, and the relationship between cross sectional area and transmural pressure of the airways at the choke point determine the maximal expiratory flow.1 Absolute lung volume influences the lung elastic recoil pressure.2 Reduced lung elastic recoil pressure, increased lung resistance, and mismatch between size of the lung and the chest cavity are proposed mechanisms of airflow limitations in emphysema.1,2
During a forced expiratory manoeuvre, thoracic volume diminishes due to both exhaled air and compressed air. At high and mid lung volumes, as flow increases to equal that of wave speed, flow limitation will occur regardless of the driving pressure gradient.3–5 It is at this point that thoracic gas compression (TGC) may occur even in areas of the lung with access to open airways. Furthermore, dynamic narrowing of airways during a forced manoeuvre in subjects with flow limitation may create areas of trapped gas in the lung and may result in gas compression.5 The TGC is greatest in subjects with a large lung volume, strong expiratory muscles, and expiratory flow limitation.6 Jaeger and Otis,7 in a study of normal subjects, showed that TGC increased with increasing airway resistance, increasing expiratory effort, and increasing lung volume. Large lung volume and expiratory flow limitation are hallmarks of COPD. Thus, subjects with COPD can generate large TGC during forced expiratory manoeuvres. By reducing the absolute lung volume, the TGC reduces the retractive forces that keep the airways open and hence both forced expiratory flow and forced expired volume in 1 second (FEV1) diminish. Because of the TGC, the highest values for FEV1 are associated with forced vital capacity (FVC) manoeuvres performed with submaximal effort.6
Lung volume reduction surgery (LVRS) has shown promise in improving lung function, exercise capacity, and quality of life in patients with severe emphysema. Several studies have reported significant improvements in FEV1 with LVRS, but always with wide individual variability.8,9,10,11 Studies of LVRS have proposed an improvement in lung elastic recoil pressure, a reduction in lung resistance, and a reduction in hyperinflation (RV/TLC) as mechanisms of expiratory flow improvement.9,10,12 LVRS reduces lung resistance and lung volume and increases lung elastic recoil pressure;9,12 it should therefore reduce the TGC and its negative effect on expiratory flow and FEV1. In this study we report the effect of LVRS on TGC and explore the effect of TGC reduction on the improvement in FEV1.
METHODS
Twenty seven subjects with severe emphysema were enrolled in a randomised controlled trial of bilateral LVRS through median sternotomy at the Michael E DeBakey VA Medical Center. The subjects underwent lung function measurements at baseline and at 6 months follow up. All subjects were clinically stable at the time of the study, and all had ceased smoking for at least 3 months before the beginning of the study. The study protocol was approved by the Institutional Review Board and each subject gave written consent.
Physical measurements
Standard spirometric measurements were obtained before the study. Lung mechanics were measured with the subjects seated in an air conditioned volume displacement plethysmograph. The characteristics of this type of plethysmograph are described elsewhere.13 Flow at the mouth level was measured by a no. 3 Fleisch pneumotachograph connected to an MP 45 Validyne (Northridge, CA, USA) pressure transducer (±2 cm H2O). Transpulmonary pressure was measured by a 10 cm long thin latex balloon positioned in the lower third of the oesophagus (38–45 cm from the nostril) and connected to a pressure transducer (352 cm H2O; Statham 131). The flow, transpulmonary pressure, and volume displacement transducers were connected to Validyne CD19A high gain carrier demodulator amplifiers and the signals were digitally collected with a personal computer (133 MHz Pentium Dell) using a National Instruments 12 bit data acquisition board (Lab-PC+).14 The data collection system is described in detail elsewhere.15 Signals were collected at a rate of 100 Hz. During each session we obtained at least three reproducible forced expiratory manoeuvres. For the forced manoeuvres, each subject was instructed to inspire to total lung capacity (TLC) then, with maximal effort, to expire to residual volume (RV). Quality control measures as outlined by the American Thoracic Society were used to select appropriate manoeuvres.16 Each subject was instructed to expire forcefully for at least 6 seconds. In addition, expiratory and inspiratory lung resistances were measured during quiet breathing using the model reported previously.17 This model examines the whole breath with the addition of a term (R′e) to account for the increasing resistance during expiration in subjects with dynamic hyperinflation. The R′e term measures an interaction between volume and resistance during expiration.17 TLC and RV were measured in all subjects at baseline and after intervention. We used the coefficient of retraction—the ratio of static recoil pressure at TLC to absolute lung volume at TLC—as an indicator of elastic recoil.18 Reference values for lung function parameters published by Black and Hyatt were used.19,20 The software was written and developed in MATLAB (Natick, MA, USA) to compute the estimated parameters for the described methods.21
After data collection the computational program in the MATLAB environment was used to calculate the FEV1 corrected for the effect of TGC. The specification of the method (No Compression Method or NCM) is described elsewhere.22 The software was developed based on the following assumptions. A plot of the expiratory flow signal versus the box volume signal in an x–y graph is generated. This plot represents the forced expiratory flow-volume loop with units of litre/second (l/s) on the y axis and litres (l) on the x axis. Subsequently, the software inverts the expiratory flow signal between TLC and RV, plots the box volume signal (l) on the x axis and the inverted expiratory flow signal (s/l) on the y axis, and generates a graph. This new graph contains a very steep negative slope at the beginning of the manoeuvre that reverses to a positive shallow slope during the effort independent portion (below 80% of TLC) of the FVC manoeuvre. Integration of the area under this curve produces a measure with a unit of seconds (computed time). The computed time (a time based on volume and flow) is the mouth transit time for increments of box volume. Likewise, mouth transit time is smaller at the start of the forced manoeuvre (at TLC) than at the end of the manoeuvre (at RV). As an individual becomes more obstructed near the end of a forced manoeuvre, the likelihood of the gas compression is higher. By summing each computed time point, the software reconstructs a time line that represents volume changes based on expiratory mouth flow and body plethysmograph volume.
After generating the computed time, the software calculates the subject’s FEV1 corrected for TGC (NFEV1). The software uses the computed time and the backward extrapolation technique to determine the start time for the NFEV1 calculation.23 To estimate the magnitude of TGC, we used the equation DFEV1 = (NFEV1 − FEV1)/FEV1, where NFEV1 and FEV1 are absolute values of forced expiratory volume in 1 second (litres) as measured by the standard method and the NCM (see above).
Statistical analysis
STATA version 7 (College Station, TX, USA) was used for statistical data analysis. Demographic and baseline lung function data were analysed by descriptive statistics and presented as means and standard deviation. The paired Student’s t test was used to evaluate the effect of LVRS on different lung function parameters (table 1). The relationships between the TGC and other parameters of lung function were evaluated by stepwise multiple regression analysis. A p value of <0.05 was considered an acceptable level of significance. To identify predictors of FEV1 improvement with LVRS a stepwise multiple regression analysis was used (p value entrance and removal criteria of 0.2 and 0.4, respectively). The results of the analysis are reported as p values, β coefficients, and adjusted R2.
Lung mechanics in 27 subjects before and 6 months after LVRS
The subjects were also grouped according to their FEV1 response into responders (improvement in FEV1 of 200 ml and 12% from baseline) and non-responders. An unpaired Student’s t test was used to compare the baseline lung function parameters between the two groups (table 2). Logistic regression analysis was used to identify the predictors of response.
Baseline lung mechanics in 27 subjects undergoing LVRS according to their FEV1 response to the surgery
RESULTS
The baseline and post LVRS pulmonary function data of the 27 study subjects are shown in table 1. All the subjects were male with a mean (SD) age of 63 (7) years, and all suffered from severe emphysema. At baseline the subjects had severe expiratory flow limitation as indicated by high Rle, low FEV1, and low PEF. In addition, they suffered from significant hyperinflation as indicated by high TLC, RV, and RV/TLC ratio. They also produced very high intrathoracic pressure during the forced manoeuvres as shown by high peak transpulmonary pressure (TPpeak). The profile of the patients in our study is similar to published data from other LVRS trials.8,9,12
NFEV1 was significantly higher than FEV1 at baseline (p<0.0001) and the mean (SD) DFEV1 was 74 (52)% at baseline. In multiple regression analysis, baseline DFEV1 was significantly predicted by baseline TPpeak (p<0.0001, β coefficient = 0.006), RV/TLC ratio (p<0.02, β coefficient = 2.545) and Rle (p = 0.07, β coefficient = 0.007; R2 = 0.83). Lung mechanics data before and 6 months after LVRS in one patient with COPD are shown in fig 1. In this patient FEV1 increased by 25% from baseline after LVRS whereas NFEV1 did not change, so the DFEV1 was reduced. The subject’s effort was not appreciably different as shown by similar TPpeak measurements at baseline and follow up.

Effect of LVRS on thoracic gas compression (TGC) in a representative patient with COPD. Solid black line shows FEV1 and dotted line shows NFEV1 (A) at baseline and (B) 6 months after surgery. DFEV1 fell from 75% to 40% with LVRS. These data show that LVRS has a considerable effect on TGC.
DFEV1 decreased significantly after LVRS (p<0.05). In stepwise multiple regression analysis, changes in TPpeak and Rle significantly predicted the change in DFEV1 (TPpeak: p = 0.0001, β coefficient 0.005; Rle: p = 0.01, β coefficient −0.023; R2 = 0.68). Other parameters including change in TLC, RV, and RV/TLC were not significantly predictive of the change in DFEV1 with the surgery.
LVRS in this cohort resulted in a significant improvement in FEV1 and elastic recoil pressure and a significant reduction in Rli, Rle, TLC, RV, and RV/TLC (table 1). In linear regression analysis the improvement in FEV1 with LVRS was significantly correlated with the reduction in Rle (p<0.02, R2 = 0.17, β coefficient −0.015 (95% CI −0.028 to −0.003)), Rli (p<0.002, R2 = 0.35, β coefficient −0.103 (95% CI −0.159 to −0.048)), DFEV1 (p<0.0001, R2 = 0.58, β coefficient 0.557 (95% CI 0.368 to 0.746)), RV/TLC (p<0.03, R2 = 0.14, β coefficient −1.569 (95% −2.965 to −0.17)), and TPpeak (p<0.05, R2 = 0.28, β coefficient 0.003 (95% CI 0.001 to 0.005)). In stepwise multiple regression analysis the improvement in FEV1 was predicted by the change in DFEV1 (p<0.0001, β coefficient 0.451 (95% CI 0.237 to 0.665)) and Rli (p = 0.07, β coefficient −0.046 (95% CI −0.096 to −0.004) with adjusted R2 = 0.62.
Table 2 shows the baseline lung mechanics data for the FEV1 responders and non-responders after LVRS. DFEV1 at baseline differed significantly between the two groups (p = 0.01). In linear regression analysis using FEV1 as a continuous variable, baseline DFEV1 was predictive of the improvement in FEV1 with LVRS (p<0.0001, R2 = 0.4, β coefficient 0.523 (95% CI 0.271 to 0.776)). The TPpeak was different in the two groups but this difference did not reach statistical significance. Data showing an association between baseline DFEV1 and FEV1 improvement from baseline with LVRS are shown in fig 2. The baseline TGC strongly predicted FEV1 improvement with LVRS.
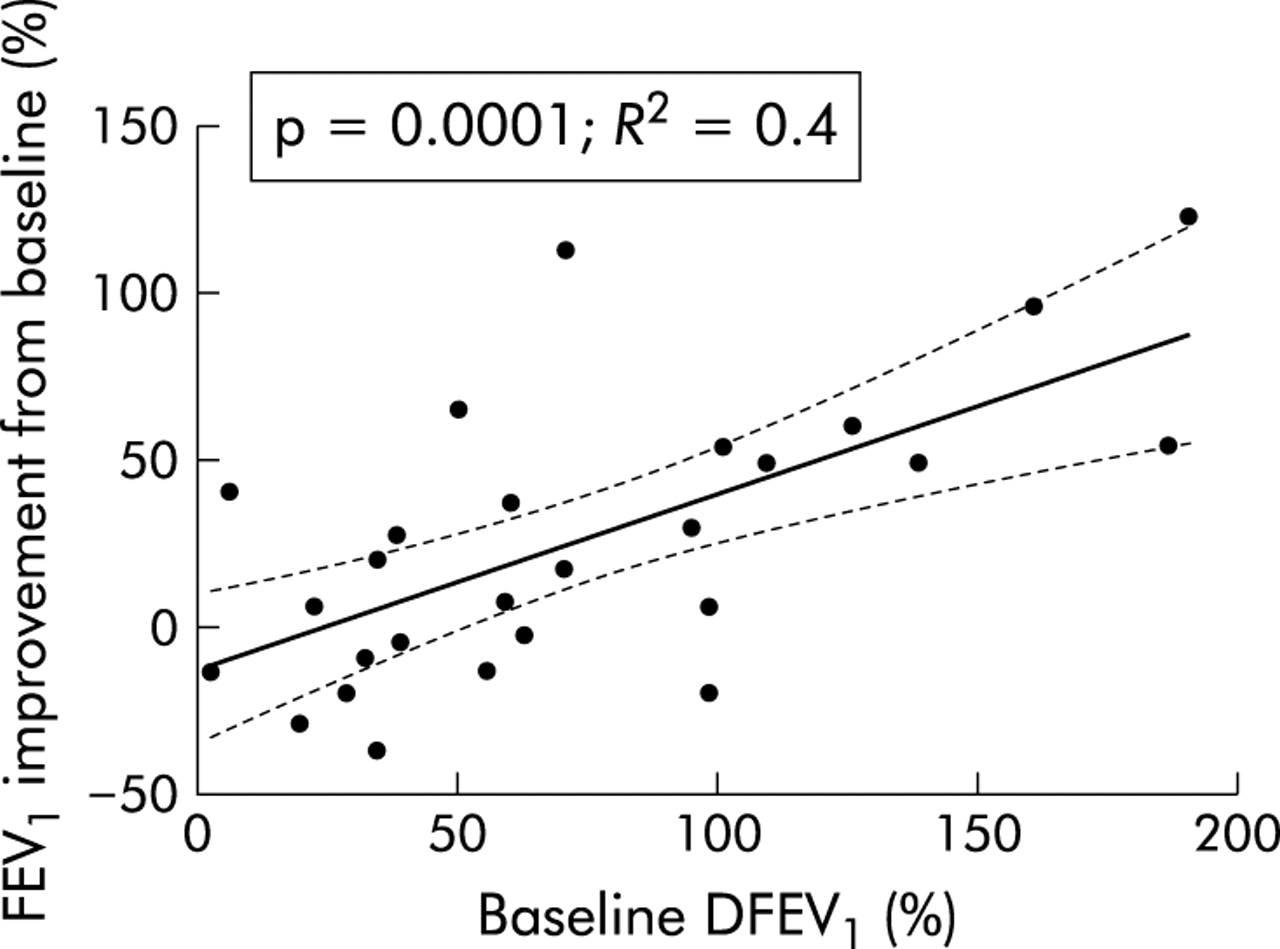
Improvement in FEV1 with LVRS correlates with baseline TGC. There is a strong association between baseline DFEV1 and improvement in FEV1. A large TGC at baseline linearly predicted a greater improvement in FEV1 with surgery. Linear regression line and 95% confidence interval lines are also shown.
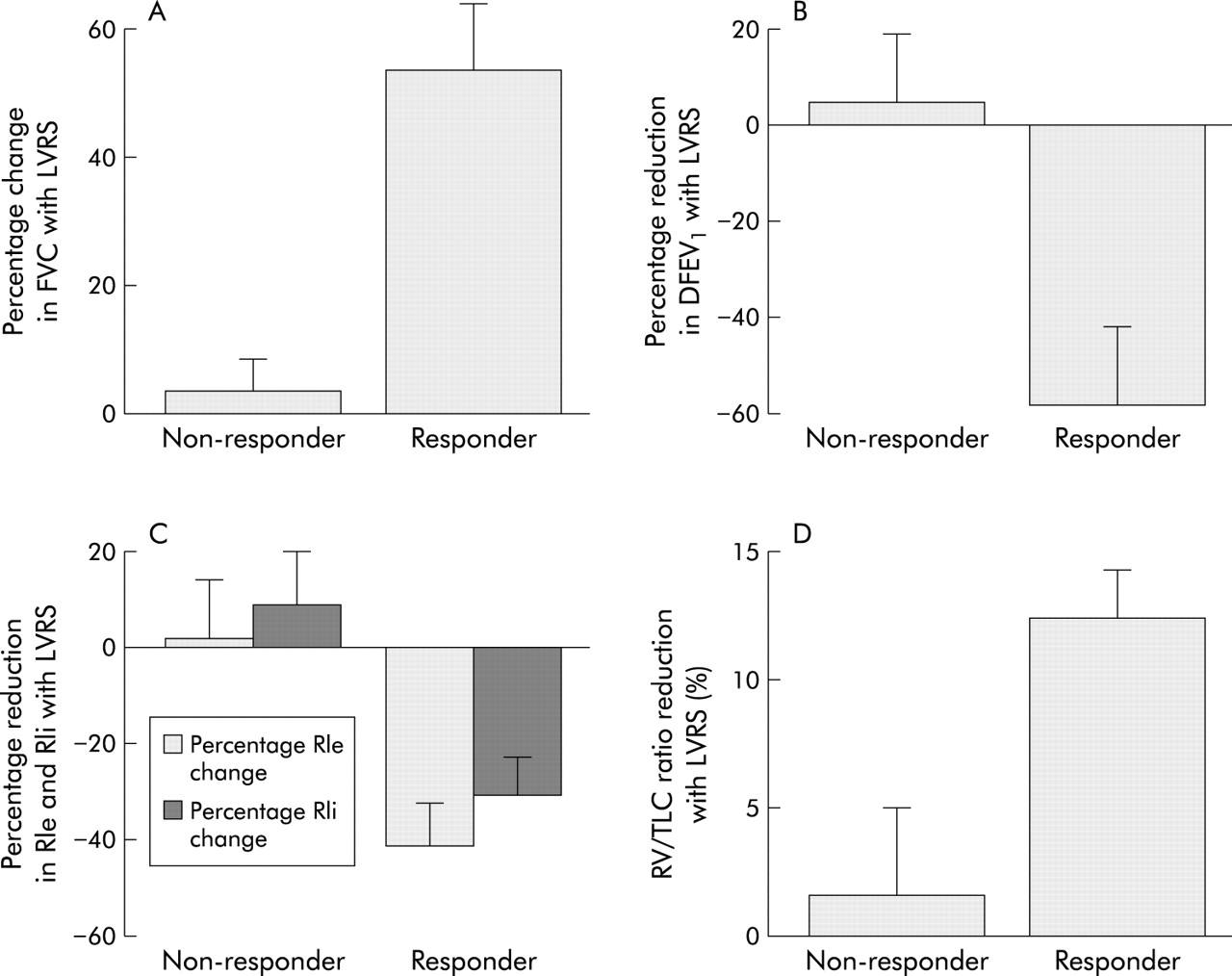
A comparison of the change in lung function parameters with LVRS between FEV1 responders and non-responders is shown in fig 3. The improvement in FVC with LVRS was significantly higher in FEV1 responders (fig 3A) and TGC was reduced more with LVRS in FEV1 responders (fig 3B). A similar pattern was seen for expiratory and inspiratory resistances (fig 3C) and RV/TLC ratio (fig 3D).

{kind=link}
{kind=link}
{kind=link}
Changes in lung function in LVRS responders and non-responders. Compared with non-responders, responders showed (A) a significantly greater improvement in FVC; (B) a significantly diminished TGC; (C) reduced expiratory and inspiratory lung resistances; and (D) a greater reduction in the RV/TLC ratio.
DISCUSSION
In this cohort of subjects with severe airflow limitation due to emphysema, TGC was large. TGC is appreciably higher in subjects with COPD than in normal subjects.22 Lung resistance, the subjects’ effort, and lung volume significantly predicted the magnitude of TGC. LVRS reduced TGC mainly as a result of improvement in lung resistance. The most striking result of our study is that a reduction in TGC was predictive of an improvement in FEV1 with LVRS. Furthermore, baseline TGC significantly predicted FEV1 improvement with the surgery. The lung function characteristics of our patients were similar to those enrolled in other LVRS studies including the National Emphysema Treatment Trial.8
Previous studies have shown that TGC is influenced by expiratory flow limitation, lung volume, and subject’s effort.6,7 Our subjects had a large lung volume and increased lung resistance, and generated a significant degree of positive intrathoracic pressure during forced expiratory manoeuvres. In our study the expiratory lung resistance and the effort significantly predicted the magnitude of TGC.
Several studies have reported an improvement in expiratory flow and FEV1 and a reduction in hyperinflation with LVRS.8,10,11 The improvements in FEV1 and lung resistance observed in our study were similar to those reported by others.8,10,11 Furthermore, although both TLC and RV were reduced, RV decreased more than TLC. This resulted in a reduction in hyperinflation and increased FVC with the surgery (table 1). The intrathoracic pressure generated during the forced manoeuvres did not appreciably change with LVRS. In contrast, TGC diminished with improvement in expiratory flow and reduction in hyperinflation. However, according to regression analysis, only reduced lung resistance with LVRS significantly predicted the reduction in TGC. Lung volumes remained high after LVRS, and this may explain the lack of effect of lung volume change on TGC in our study.
Our data support the role of TGC reduction in FEV1 improvement with LVRS. Absolute lung volume is a major determinant of maximal expiratory flow, especially in lung volumes below 75% of TLC.24 TGC exerts a negative effect on forced expiratory flow by reducing the lung volume and thus diminishing the retractive forces applied by the lung parenchyma on the small airways. For example, submaximal effort during forced expiratory manoeuvres in subjects with expiratory flow limitation result in higher FEV1.6 This effect is due to lower TGC. Our analysis showed that half of the improvement in FEV1 with LVRS can be explained by the reduction in TGC.
In our study the baseline TGC predicted the improvement in FEV1 with LVRS. The baseline TGC, as reflected by DFEV1, was higher in responders than in non-responders. One of the most striking results of our study is that the baseline TGC alone can predict 40% of the improvement in FEV1 with LVRS. TGC is influenced by a number of factors. A large absolute lung volume and RV/TLC ratio are associated with higher TGC. Furthermore, increased airway resistance and a large expiratory effort are required to produce a significant TGC. Although not statistically different, the maximum intrathoracic pressure generated in the responders appeared to be higher than in the non-responders. This may indicate that patients with higher TGC have more preserved expiratory muscle function. Ramírez-Sarmiento and others showed that deterioration in expiratory muscle strength and endurance were associated with parallel impairments in other respiratory muscle groups.25,26 The ability to generate a higher transpulmonary pressure during a forced manoeuvre may therefore indirectly affect the function of the respiratory muscles. Furthermore, the mismatch between the size of the lungs and the chest in patients with emphysema is an important factor in causing flow limitation.12 The magnitude of gas compression therefore reflects the patient characteristics which may influence the response to LVRS.
In summary, in our cohort of patients with severe COPD, LVRS reduced TGC and this reduction partially explained the improvement in FEV1. Our data suggest that baseline TGC might predict the FEV1 response to LVRS, but further studies are needed to confirm this finding.
Acknowledgments
The authors thank Ms Pamela Smithwick for her effort in conducting this study.
REFERENCES
Footnotes
-
This work is supported by the office of Research & Development of the Department of Veterans Affairs and VA Medical Research Service Merit Award for LVRS (SGW) and by NIH HL-072839 (AMB).
-
None of the authors of this manuscript has any conflict of interest.