Article Text

Statistics from Altmetric.com
Thoracic outlet syndrome (TOS), which is caused by osseous and soft tissue abnormalities and presents as tingling, paraesthesia, and weakness of the extremity, is a controversial subject. Surgical treatment for TOS is seen as the last resort and involves resection of the first rib and scalenotomy and leads to an overall improvement of 70% over a period of 5 years.1 The most common postoperative complications are pneumothorax, injury to the subclavian artery and vein, or brachial plexus and long thoracic nerve.2 Second rib fracture as a complication after surgery for TOS has not previously been described.
A 54 year old woman had been symptomatic with bilateral constant numbness, tingling, paraesthesia, and weakness exacerbated by sports and exercises for well over 10 years. Numerous attempts at conservative treatment had failed. She also had bilateral omarthrosis which had been treated by previous acromioclavicular joint resection and subacromial decompression. Nevertheless, the symptoms persisted and increased in both ulnar innervated segments of the arm. The hyperabduction test (Wright) was positive on both sides. In conjunction with her other symptoms, a diagnosis of bilateral neurovascular TOS was established and the patient underwent transaxillary first rib resection on the right side. Any injury to the second rib during surgery could be ruled out. Her recovery was uneventful and both pain and numbness were greatly improved.
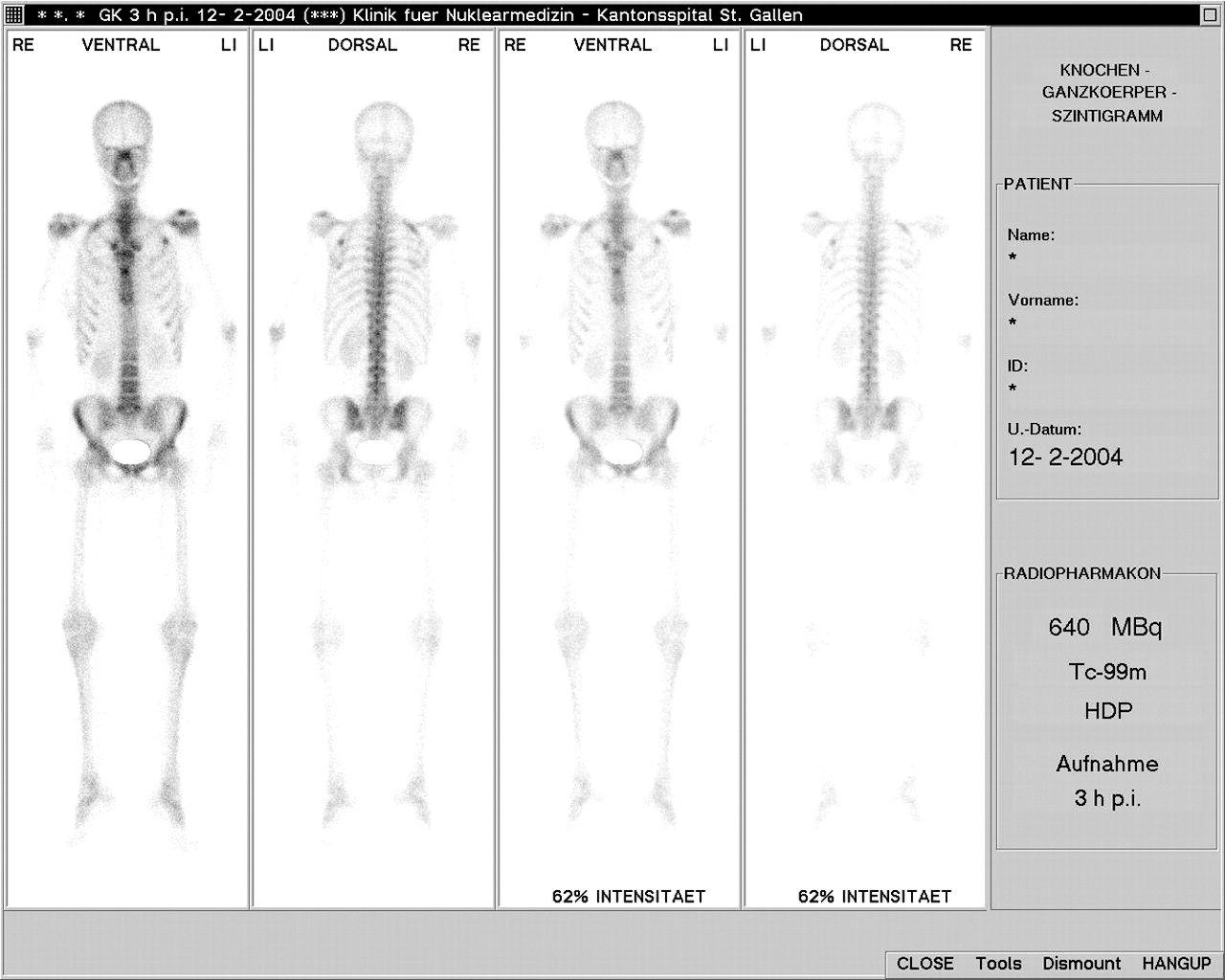
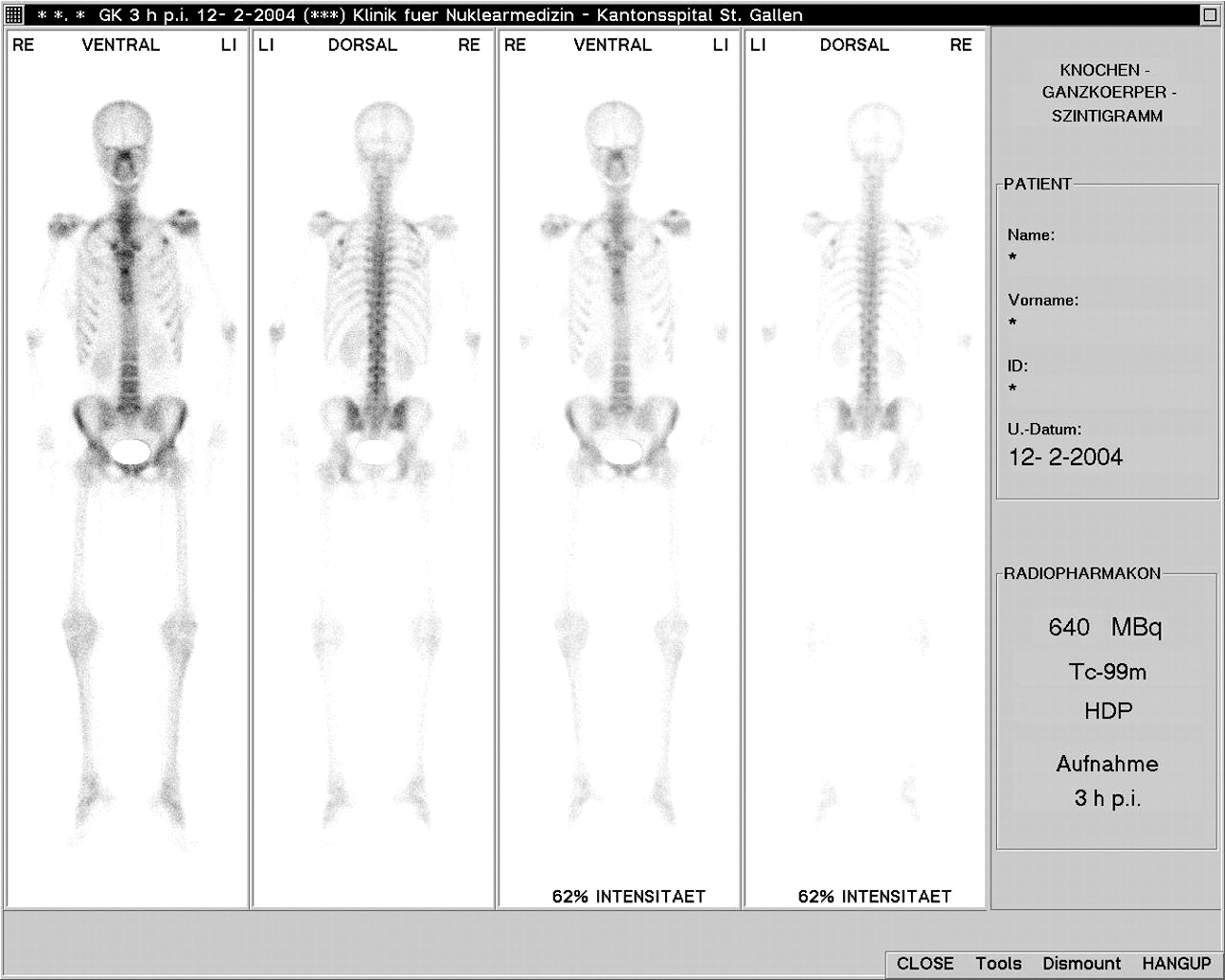
Two months later transaxillary first rib resection was performed on the left side. Again the symptoms improved. Three weeks after this operation the patient felt a sudden crack and tenderness in her left shoulder girdle with no previous minor or major trauma. Radiographs showed an anterolateral left second rib fracture. Two months later the patient developed sudden tenderness in her right shoulder, again with no previous trauma, and a posterolateral second rib fracture was diagnosed by radiography. An osteodensitometric study showed only a slightly deficient calcium intake of estimated 1150 mg instead of 1500 mg per day. T-scores were within the normal range and no diagnosis of osteoporosis could be established. A technetium-99m bone scan and a SPECT showed increased pathological activity in both second ribs consistent with the fractures, but no other abnormalities (fig 1). The patient was treated conservatively and recovered very well; she has had no further problems.
{kind=link}
Technetium-99m bone scan of patient.
Fractures of the first rib are very rare and bilateral fractures are even more uncommon.3–9 Bilateral fracture of the second rib has not been described previously. After first rib resection the second rib becomes the most cranial rib and thus takes the place of the former first rib. Second rib fracture after first rib resection can therefore be compared with first rib fractures in patients who have not undergone first rib resection. Several theories on the aetiology of first rib fractures exist.6,7 Traumatic fractures usually involve not only the first rib but also the clavicle or scapula. Considerable force is required to fracture the first rib since it is protected very well by soft tissue and the clavicle and scapula. Non-traumatic fractures occur without adequate trauma and are regarded as stress fractures and usually can be found in the weakest portion of the rib.3–8 Fractures present with upper chest pain and tenderness.3 Some authors have doubted the existence of this type of fracture and classify it as a congenital anomaly.10
Most authors explain the stress fracture by the anatomy of the first rib.3–8 The rib is broad and flat and weakened by the groove where the subclavian artery crosses it. The scalene muscles produce a bending force in the rib causing it to fracture. This theory has been questioned since it would mean that all fractures would occur at the same location.3 After first rib resection for TOS the second rib takes the place of the first rib and faces the same stress as the former first rib. The second rib is thinner and not as wide as the first rib, leaving it even more vulnerable to stress. This can explain the relatively short time between first rib resection and fracture of the second rib on the left side in our patient. This left the rib with insufficient time to adapt to the increased force after first rib resection. The clavicle may exert pressure on the second rib, particularly when carrying heavy loads. Our patient denied vigorous exercise before the fracture. The fracture of the right second rib may be explained by increased stress due to impaired movement of the left shoulder. Furthermore, scar remodelling around the rib may have impaired motion leaving the rib prone to fracture. The two fractures occurred in different parts of the rib. We conclude that there is no point of least resistance in the second rib. Also, no muscle insertion on the rib is responsible for the fracture. A pathological fracture resulting from bone metastases was ruled out and there was no osteoporosis which would have made the bones more prone to trauma. We classify the fractures as spontaneous non-traumatic fractures in an otherwise healthy patient.
Spontaneous non-traumatic fractures of the first and second ribs remain a controversial topic. The fractures presented with pain and tenderness. Upper chest pain is the only symptom in such patients, and a second rib fracture should be considered in patients who develop chest pain after first rib resection.