Article Text

Abstract
Background: Nitric oxide in exhaled air (FENO) is a marker of eosinophilic airway inflammation. A study was undertaken to determine whether FENO predicts asthma relapse in asymptomatic asthmatic children in whom inhaled corticosteroids are discontinued.
Methods: Forty children (21 boys) of mean age 12.2 years on a median dose of 400 μg budesonide or equivalent (range 100–400) were included. FENO was measured before and 2, 4, 12, and 24 weeks after withdrawal of steroids. A relapse was defined as more than one exacerbation per month, or need for β agonist treatment on 4 days per week for at least 2 weeks, or diurnal peak flow variability of >20%. FENO measurements were performed online with an expiratory flow of 50 ml/s.
Results: Nine patients relapsed. Two and 4 weeks after withdrawal of steroids geometric mean FENO in children who were about to relapse was higher than in those who did not relapse: 35.3 ppb v 15.7 ppb at 2 weeks (ratio 2.3; 95% CI 1.2 to 4.1; p = 0.01) and 40.8 ppb v 15.9 ppb at 4 weeks (ratio 2.6; 95% CI 1.3 to 5.1). An FENO value of 49 ppb at 4 weeks after discontinuation of steroids had the best combination of sensitivity (71%) and specificity (93%) for asthma relapse.
Conclusion: FENO 2 and 4 weeks after discontinuation of steroids in asymptomatic asthmatic children may be an objective predictor of asthma relapse.
- FENO, fractional nitric oxide concentration in exhaled air
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- ICS, inhaled corticosteroid
- PEF, peak expiratory flow
- asthma
- exhaled nitric oxide
- children
Statistics from Altmetric.com
- FENO, fractional nitric oxide concentration in exhaled air
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- ICS, inhaled corticosteroid
- PEF, peak expiratory flow
Remission of asthma is common in children.1,2 It is difficult to determine the time point at which to reduce or stop inhaled corticosteroids (ICS). ICS are currently adapted on clinical grounds with dose reduction based on patient history, sometimes influenced by parental or doctor’s fears of side effects. However, there are few if any objective means to guide parents or children. According to current practice, ICS are discontinued in asthmatic children who are symptom-free for at least 6 months on a low dose of inhaled steroids. Follow up is discontinued soon after withdrawal of ICS. However, some of these children will have a relapse, and there is currently no objective parameter to predict the probability of asthma relapse following steroid withdrawal. Measurement of the fractional nitric oxide concentration in exhaled air (FENO) has been proposed as a marker of eosinophilic airway inflammation.3,4 FENO levels can be obtained easily and repeatedly with minimal discomfort to the patient, and measurement techniques have been well standardised.4,5 Treatment with ICS reduces FENO by a direct effect on transcription of inducible NO synthase and by reducing airway inflammation.6–8 Even low doses of ICS may decrease FENO to normal levels.6,9–13 If FENO could give additional information on the risk of asthma relapse, this could potentially modify current treatment strategies. Only a few studies have addressed the use of FENO as a predictor of loss of asthma control related to changes in the ICS dose in adults, and the results are unequivocal.11,14,15 The aim of this study was to evaluate whether or not FENO predicts the probability of asthma relapse in children in whom ICS are discontinued because of clinical remission.
METHODS
Forty children aged 6–18 years with asthma according to ATS criteria were enrolled at the moment when discontinuation of ICS was considered because of lack of symptoms for more than 6 months at a stable dose of ICS (100–400 μg/day budesonide or equivalent). Children on leukotriene receptor antagonists were excluded. Atopy was defined as RAST class 2 or higher for at least one airborne allergen. Written informed consent was obtained and the study was approved by the medical ethical committee of the Erasmus Medical Centre.
Study design
This prospective study lasted 26 weeks. During a run-in period of 2 weeks (from t = −2 to t = 0) and 2 weeks before every visit, children recorded cough, wheezing, and dyspnoea twice daily on a 4 point scale (0–3) on a diary card as used in previous studies.16 The maximum possible cumulative symptom score was 252. Medication use and peak expiratory flow (PEF) were recorded twice daily. Children used a peak flow meter at home (Glaxo Wellcome, Zeist, The Netherlands) and recorded the personal best value of three attempts in the morning and evening. Diurnal PEF variability was defined as the difference between evening and morning values, divided by the mean of both measurements. At the start of the run-in period, the inhalation technique was checked and adherence to ICS treatment was strongly encouraged. Baseline FENO was measured at t = −2 and t = 0 weeks. Forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV1) before and after bronchodilation were measured at t = −2, 12 and 24 weeks. At t = 0 weeks, treatment with ICS was discontinued in patients with low symptom scores (below 14), mean PEF variability within 20%, and not needing rescue medication. FENO was monitored 2, 4, 12, and 24 weeks after withdrawal of ICS. The study design is shown in table 1.
Study design
In cases in whom an upper respiratory tract infection occurred, follow up visits were postponed for 2 weeks. Patients were asked to contact the investigator if an exacerbation occurred, which was defined as asthma symptoms not responding to the bronchodilator. Subsequently, children were seen and treated by their own paediatric pulmonologist, not the investigator. A relapse was defined as more than one exacerbation per month and/or exacerbations requiring oral or inhaled steroid use and/or need for rescue bronchodilators on 4 or more days per week for at least two consecutive weeks and/or mean diurnal PEF variability of >20% according to the guidelines of the Dutch Paediatric Respiratory Group.17 The primary end point was relapse. At the point at which relapse occurred, children dropped out of the study.
FENO measurements
FENO was measured online with an expiratory flow of 50 ml/s according to ATS and ERS guidelines.4,5 NO was continuously sampled with a sampling flow of 175 ml/min and analysed by a chemiluminescence analyser (Sievers 280 NOA, Boulder, CO, USA). The analyser was calibrated weekly using 0 and 115 ppb NO certified gases (BOC, Herenthout, Belgium).
Lung function testing
Flow-volume curves were obtained with a dry rolling seal spirometer (Jaeger, Würzburg, Germany) according to ATS guidelines. After maximal inspiration, three reproducible loops with a maximum variability in FVC of 10% were obtained. FVC and FEV1 are expressed as percentage predicted.18
Statistical analysis
FENO values were logarithmically transformed before statistical analyses and the results expressed as geometric means. FENO at t = 0 weeks was used as baseline. For each interval between two measurements we assessed whether FENO at the beginning of the interval was predictive for the occurrence of relapse during the interval. Subsequently, the information from these four analyses were combined using conditional logistic regression which relates the probability of relapse in each period to FENO at the start of this period.19 Multivariate analysis was repeated using either FENO or the ratio of FENO to baseline FENO. FENO at baseline and at the various time points was compared in patients with and without clinical relapse using Mann-Whitney U tests. ROC curves for FENO 2 and 4 weeks after discontinuation of ICS were constructed. The correlation between FENO and clinical and lung function parameters was assessed using Spearman’s correlation coefficient.
RESULTS
Of the 40 children included in the study, one dropped out because of a high symptom score during the run-in period and two were lost to follow up. The remaining 37 patients (21 boys) had a mean age of 12.2 years (range 7.3–16.9). Data on the study population are shown in table 2. Twenty nine were atopic; these children did not differ from non-atopic children in age, height and weight, nor in pulmonary function tests or baseline FENO. None of the children used long acting β2 agonists or leukotriene antagonists.
Baseline anthropometric and lung function data of study population (n = 37 children, 21 boys)
Baseline geometric mean FENO at t = 0 was 11.2 ppb (95% CI 8.5 to 15.3). This did not differ significantly from FENO at t = −2, the start of the run-in period (p = 0.67). Intra-individual variability between values at t = −2 and t = 0 weeks was considerable (intraclass correlation coefficient 0.52).
FENO and relapse of asthma
Nine patients (24%), one of whom was non-atopic, had a clinical relapse after a median of 36 days (range 14–141). Of these nine patients, five had two exacerbations within 1 month or a single exacerbation requiring oral or inhaled steroids and four used their bronchodilator as rescue therapy for ⩾4 days a week during at least two consecutive weeks. Six children relapsed between 4 and 12 weeks after withdrawal of ICS; in the periods 0–2 weeks, 2–4 weeks, and 12–24 weeks, one patient relapsed in each period (fig 1). Children who experienced an asthma relapse did not differ in baseline demographic or pulmonary function data (table 2). There was no difference in initial steroid dose of children who did or did not relapse (Mann-Whitney U test, p = 0.28), nor was there a significant difference in baseline geometric mean FENO between the two groups of patients (14.8 ppb v 10.5 ppb, respectively; ratio 1.4; 95% CI 0.7 to 2.8, p = 0.32). Two weeks after withdrawal of ICS the geometric mean FENO in children who relapsed thereafter (n = 8) was significantly higher than in those who did not relapse (35.3 ppb v 15.7 ppb; ratio 2.3; 95% CI 1.2 to 4.1, p = 0.01). The same was true for FENO after 4 weeks without steroids for the seven children who relapsed after 4 weeks (40.8 ppb and 15.9 ppb; ratio 2.6; 95% CI 1.3 to 5.1, p = 0.009; fig 1).
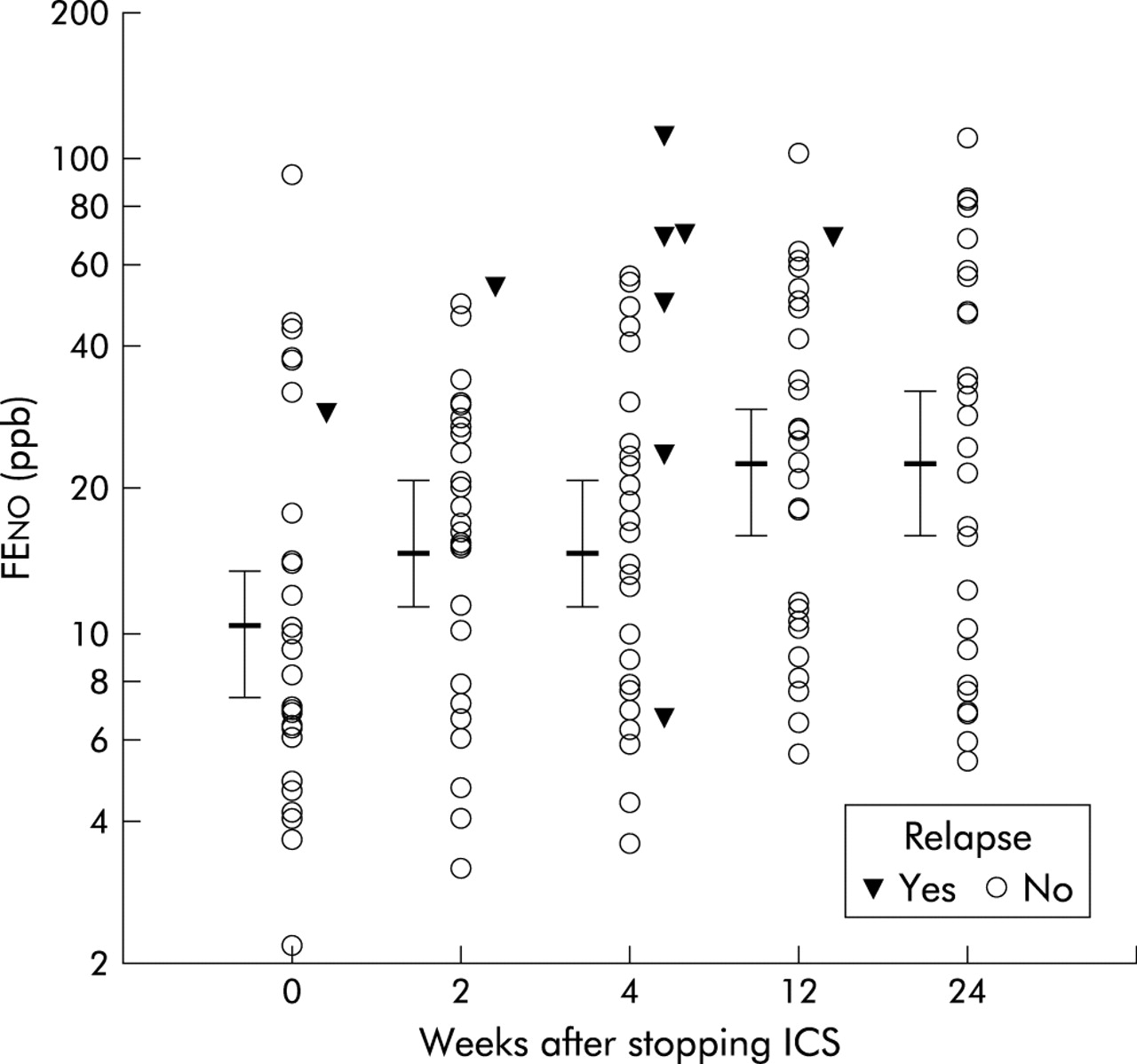
FENO values in patients with and without an asthma relapse. For each period (0–2, 2–4, 4–12, and 12–24 weeks) patients were classified according to whether they relapsed or not in the period indicated. FENO values were obtained at the start of each period. For patients without a relapse geometric mean FENO and 95% confidence intervals are given. The x axis depicts number of weeks after withdrawal of ICS. One patient relapsed in the first period (0–2 weeks), one between 2 and 4 weeks, six between 4 and 12 weeks, and one after 12 weeks.
FENO at 4 weeks after withdrawal of ICS predicted relapse in the forthcoming period (4–12 weeks after withdrawal, p = 0.025). Multivariate logistic regression combining results of all periods showed that FENO was a better predictor of asthma relapse (p = 0.001) than the FENO ratio (actual FENO divided by baseline FENO) (p = 0.04). For each doubling of FENO the relapse rate increased by a factor 3.0 (95% CI 1.5 to 7.1). The results were similar when only atopic patients were analysed.
Two patients were included who later admitted to having used more than 400 μg budesonide regularly before enrolment. One of them relapsed. If both children were excluded, multivariate logistic regression still showed that FENO predicted asthma relapse in the remainder (p = 0.003).
ROC curves indicated that a FENO value of 49 ppb 4 weeks after stopping steroids had the best combination of sensitivity and specificity for predicting relapse (sensitivity: 71% (95% CI 29 to 96) and specificity 93% (95% CI 76 to 99); fig 2). The positive and negative predictive values of FENO of 49 ppb were 71% and 93%, respectively.

ROC curve for FENO 4 weeks after discontinuation of inhaled corticosteroids. The optimal combination of sensitivity and specificity for identifying children with relapse was for FENO 49 ppb (71% and 93%, respectively).
The course of FENO in all individuals who experienced a relapse is shown in fig 3. In patients who did not relapse there was a general trend for FENO to rise with time from a geometric mean of 10.2 ppb at the start of the study to 22.2 ppb after 26 weeks of follow up (fig 1). FENO showed an overall tracking pattern in those who did not relapse.

{kind=link}
{kind=link}
{kind=link}
Course of FENO values in nine patients who relapsed. The only non-atopic patient who experienced a relapse is marked with an asterisk.
Correlations between FENO, clinical symptoms, and pulmonary function tests
The results of pulmonary function tests, atopic state, PEF variability, cumulative symptom score and use of rescue medication during the run-in period did not differ between children with or without a relapse. Cumulative symptom scores, spirometric data, PEF values, and PEF variability did not correlate with geometric mean FENO at any time point.
Other parameters and relapse of asthma
Symptom scores, peak flow, diurnal variability in peak flow, or other lung function tests performed during the run-in period did not predict asthma relapse.
DISCUSSION
We found that FENO at 2 and 4 weeks after discontinuing ICS predicted asthma relapse in asthmatic children who were taken off ICS because of clinical remission. Initial FENO levels measured while patients were still on ICS were not predictive of relapse. An FENO of 49 ppb or higher 4 weeks after discontinuation of ICS had the best combination of sensitivity (71%) and specificity (93%).
Few other studies have assessed FENO longitudinally after discontinuation or reduction of ICS, and none of these included children. Our results are in agreement with the study by Jones et al11 in which adult asthmatics treated with a mean daily ICS dose of up to 1600 μg were forced off steroids and followed for loss of asthma control. In this study, in contrast to ours, discontinuing steroids was not clinically indicated, and loss of control occurred earlier, after a median of 17 days. Their FENO values were much lower, probably due to the higher flow rate of 250 ml/s used to obtain exhaled air samples. Lim et al14 performed a similar study in adults and their preliminary report states that NO in mixed nasal/oral exhaled air did not predict asthma relapse. However, mixed expired air is contaminated by high nasal levels of NO which makes interpretation impossible. Moreover, they defined relapse as a recurrence of asthma symptoms requiring either β2 agonists or ICS. This might well explain any discrepancy between their findings and ours.
Jatakanon et al20 studied several non-invasive markers of airway inflammation in asthma exacerbations induced by forced reduction of ICS doses from more than 800 μg to 200 μg budesonide in adults. FENO at baseline did not predict loss of asthma control. However, there was a rapid increase in FENO before exacerbations 2–4 weeks after decreasing inhaled steroids. Only 15 patients were included in the study, and this small number could easily lead to non-significant findings. Furthermore, ICS were not completely withdrawn, which reduces the possibility of finding a difference between the groups.
The increases in FENO over time in children who relapsed were consistent and larger than within-subject baseline fluctuations. However, the intra-individual variability in FENO measurements at the beginning and end of our 2 week run-in period was quite high. Few data are available on long term within-subject reproducibility of FENO in asthmatic children. Earlier reports have focused on short term reproducibility, which is excellent. Kharitonov et al21 found intraclass correlation coefficients better than 0.90 in adults and children with and without asthma, with 95% limits of agreement of about 4 ppb when children were tested repeatedly within 4 days. Jones et al reported a within-subject coefficient of variation of FENO measured with a 1 week interval of 10.5%.11 The variability in our study may be due to the long interval of 2 weeks between FENO assessments. We also reasoned that inclusion in the study as such might affect FENO because of better compliance with ICS during the run-in. This seems unlikely as increased compliance would lead to a reduction in FENO whereas we found no significant difference between FENO at t = −2 and t = 0, with a trend towards higher levels at t = 0. In addition, ambient NO levels can be a source of variability. However, we found no relation between ambient NO and FENO, so we think ambient NO levels do not explain the variability in FENO.
We included both atopic and non-atopic asthmatic subjects, reflecting the asthma population in daily practice. The numbers are too small for a subgroup analysis; only one non-atopic child relapsed. The patients who did not relapse without medication showed a wide range of FENO values (fig 1). In these children no correlation was found between FENO and symptom scores. As our follow up was 6 months, we cannot exclude that some of the children might relapse later. The possible clinical relevance of an increased FENO in asymptomatic children therefore remains unclear.
What are the implications of these results for clinical practice? Our findings in this relatively small group of asthmatic children strongly suggest that FENO measurements at 2 and 4 weeks after cessation of steroids are helpful for identifying children in whom relapse of asthma is more likely to occur and who might benefit from a close follow up. However, patient numbers in this study are small and more children who did not relapse had raised FENO levels than those who did relapse. Larger studies are needed to confirm the role of FENO in decision making on ICS in asthmatic children and to calculate more accurately the sensitivity and specificity of different cut-off levels of FENO.
In conclusion, this is the first study in children showing that FENO is an early predicting marker of relapse in asthma after cessation of ICS. Larger studies are now warranted to substantiate this finding to further define the role of FENO in this aspect of asthma management.
REFERENCES
Footnotes
-
MWP was supported by a research grant from the Dutch Asthma Foundation and WH was supported by an unrestricted grant from Glaxo Smith Kline, The Netherlands.