Article Text

Abstract
Background: Pulmonary complications are a major cause of morbidity and mortality in sickle cell disease (SCD). The relationship of asthma with SCD and acute chest syndrome (ACS) remains uncertain. A study was undertaken to test the hypotheses that asthma and bronchial hyperreactivity (BHR) are more common in children with SCD than in ethnic matched controls and that SCD children with atopic asthma are more likely to have recurrent episodes of ACS.
Methods: A modified International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire was administered and skin prick tests undertaken in 80 children with SCD and 80 ethnic matched controls aged 5–10 years. BHR was assessed by measurement of forced expiratory volume in 1 second before and after a bronchodilator (albuterol 200 μg) or an exercise challenge.
Results: Asthma (48% v 22%, p = 0.002) and BHR (p = 0.02) but not atopy were more common in children with SCD than in controls. Atopy (66.6% v 29%, p = 0.007) and asthma (80% v 40%, p = 0.005), particularly atopic asthma (53% v 12%, p<0.001), were more common in children with SCD who had suffered recurrent episodes of ACS than in those who had suffered a single or no episode.
Conclusions: Asthma and BHR are more common in children with SCD than in ethnic matched controls, and atopic asthma appears to be associated with recurrent ACS. Early and effective anti-asthma therapy might reduce the pulmonary morbidity associated with SCD.
- ACS, acute chest syndrome
- BHR, bronchial hyperreactivity
- FEV1, forced expiratory volume in 1 second
- SCD, sickle cell disease
- asthma
- children
- sickle cell disease
- acute chest syndrome
- ethnicity
Statistics from Altmetric.com
- ACS, acute chest syndrome
- BHR, bronchial hyperreactivity
- FEV1, forced expiratory volume in 1 second
- SCD, sickle cell disease
Children with homozygous SS sickle cell disease (SCD) frequently suffer acute chest syndrome (ACS).1,2 The increased leucocyte count,3 raised secretory phospholipase A2 levels,4 and the release of toxic metabolites of nitric oxide5 are evidence of the inflammatory nature of ACS. The acute episodic inflammation, the inadequate protection in the sickle lung from oxidant injury,6–9 and the underlying chronic subclinical inflammation10 suffered by all patients with SCD may predispose to the development of recurrent wheezing, as is seen following airway inflammation due to gastro-oesophageal reflux11,12 or cystic fibrosis.13
Children with recurrent wheeze are frequently diagnosed as suffering from asthma; thus we hypothesise that the prevalence of asthma would be greater in children with SCD than in controls. Results from epidemiological studies, however, have not substantiated such a hypothesis, reporting either a lower14 or similar prevalence15–18 to that found in controls, but this may be due to the design of the studies. One method to assess the occurrence of asthma is to administer a well validated questionnaire such as the International Study of Asthma and Allergies in Childhood. It is also important to assess bronchial hyperreactivity (BHR) as patients with asthma may be asymptomatic. It is possible that, if an excess of asthma or BHR was found in children with SCD, this may not be a consequence of lung inflammation but rather that premorbid asthma is more common in SCD children.
Atopy is the strongest identifiable risk factor for asthma with an increased risk of 10–20 fold.19,20 We therefore further hypothesise that SCD children with asthma, particularly atopic asthma, would be more likely to suffer recurrent episodes of acute chest syndrome (ACS). During asthma attacks the bronchoconstriction and ventilation-perfusion mismatch results in localised areas of hypoxia and acidosis. These conditions induce a shift in the oxygen dissociation curve to the right, promoting increased sickling which may predispose to ACS. Allergy skin prick testing objectively highlights the presence of atopy. Thus, by undertaking skin prick testing in SCD children and controls, in addition to the investigations described above, it is possible to determine whether atopic asthma is more common in children with SCD and predisposed to recurrent ACS episodes.
By administering a modified ISSAC questionnaire, undertaking exercise/bronchodilator challenges and skin prick testing, this study aimed to test the hypotheses that (1) asthma and BHR are more common in children with SCD than in ethnic matched controls and (2) SCD children with atopic asthma are more likely to have recurrent ACS episodes.
METHODS
Study population
One hundred and sixty six children with homozygous SS disease (SCD) aged between 5–10 years attending the Sickle Cell Clinic at the University of the West Indies, Jamaica were identified from the clinic database. One child from each of four sibling pairs was excluded and another because of being a ward of the court, leaving 161 identified children. The names were randomly ordered by computer software (Stata 8) and these children were approached for recruitment in the prescribed order. Sixteen children were found to be ineligible as they had emigrated (n = 3) or moved to the country (n = 13); nine were untraceable by telephone or visit; three had suffered severe sickle complications and were unable to complete the protocol; nine could not participate due to family crises (n = 2) and social unrest in their neighbourhoods (n = 7); and the parents of seven children had no interest in participating. Eighty three children were successfully recruited. Three were subsequently excluded because of unavailability of a control child (n = 2) and the inability to complete pulmonary function testing (n = 1). The eligible children who were not recruited did not differ from the included sample in sex distribution (49.2% of those not recruited were girls compared with 50.0% of those recruited, p = 0.93) or in age (mean (SD) 6.9 (1.2) years not recruited v 7.1 (1.1) years recruited, p = 0.22).
Each of the 80 children with SCD included in the study was matched to within 1 year of age with an unrelated non-SCD child resident within their immediate community. The study was approved by the ethics committee of the University Hospital of the West Indies and informed written parental consent was obtained.
Protocol
Questionnaire
All children were seen in the paediatric lung function laboratory. Parents were asked to complete a questionnaire based on the International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire. The ISAAC question asking whether the subject had ever had asthma was modified so that parents were asked if their child had ever been diagnosed with a “touch of asthma”, as this is the term frequently used in Jamaica to describe patients with mild to moderate asthma. The ISAAC questions concerning wheeze ever and wheeze in the past 12 months were each modified to include whether the child had had a dry cough lasting at least 7 days which was not associated with the start of a viral upper respiratory tract infection. Additional questions were included to document whether bronchodilators or inhaled corticosteroids had ever been prescribed or were currently being administered.
The validity of the modified questionnaire was examined in a population of 100 consecutive children attending hospital paediatric clinics (asthma clinics excluded) in Kingston, Jamaica. Parents were asked to complete the questionnaire before seeing the clinic doctor. The clinic doctor meanwhile extracted relevant data from the child’s medical records. The results of the parent completed questionnaire were compared with the data obtained from the medical records. Parents and doctors were unaware of each others’ responses.
Pulmonary function tests
The children were weighed and their heights measured. Spirometric tests (Morgan TLC Test Mk 11, Morgan Scientific, Haverhill, MA, USA) were performed in a sitting position and forced expiratory volume in 1 second (FEV1) was measured before and after a challenge. A maximum of eight attempts were undertaken to obtain the best three curves with FEV1 values within 5% of each other in keeping with the European Respiratory Standards.21 Subjects with a baseline FEV1 less than 75% of that predicted for height were re-measured 15 minutes after administration of a bronchodilator (albuterol 200 μg) challenge delivered via metered dose inhaler with an Ace Spacer. BHR was diagnosed if there was an increase of at least 12% in FEV1 after the bronchodilator challenge.22 Those with a baseline FEV1 of more than 75% predicted undertook an exercise test after which they were re-measured. Heart rate and oxygen saturation were monitored immediately before, throughout, and for 30 minutes after the exercise test. The subject was asked to stand on a treadmill (True S.O.F.T. treadmill, True Fitness Technology Inc, O’Fallon, MO, USA). The speed was increased to approximately 2 mph and the inclination increased to 15° within 1 minute. The speed was adjusted to keep the subject’s heart rate within 10 beats/minute of (and not exceeding) the target heart rate ((220 − age) × 0.80) and to keep the oxygen saturation ⩾95% in the controls and within 5% of the baseline of the SCD children. If desaturation or a tachycardia occurred, the speed was decreased to achieve the desired parameters. If the subject did not keep up when the pace was increased or complained of tiredness or shortness of breath despite acceptable parameters, the speed was decreased. The exercise test lasted at least 6 minutes. Acceptable tests were those in which the heart rate remained within the desired range for more than 3 minutes. The spirometric tests were repeated 1, 5, 10, 15, and 20 minutes after exercise. BHR was diagnosed if there was a decrease of at least 10% in FEV1 after the exercise challenge.22 The temperature in the laboratory was maintained between 22°C and 25°C during testing.
Skin prick testing
Skin testing was performed on the forearm with 25 sterile gauge needles using histamine (positive control), diluent (negative control), Dermatophagoides farinae, D pteronyssinus, cockroach (German and American), mould mix, Bermuda grass, cat hair and dog hair (Hollister-Stier Laboratories, Spokane, USA). After 15 minutes the forearm was inspected by two individuals (NL and JK-M) who independently measured and recorded the size of the wheals. A reaction was deemed positive if it was at least 3 mm×3 mm (largest diameter and diameter perpendicular to it). If there was any wheal with the negative control, a test wheal had to be at least 3 mm larger than the negative control in both diameters to be deemed positive. Those with at least a single positive reaction were diagnosed as atopic.
Record review
The Sickle Cell Unit records of the children with SCD were reviewed to determine whether they had had an ACS episode. An ACS episode was diagnosed if the child had suffered an acute onset of abnormal respiratory signs and/or symptoms in association with a new infiltrate on the chest radiograph.23 Children were classified as “ACS ever” if they had had a single ACS episode and “recurrent ACS” if they had had at least two ACS episodes.
Analysis of data
From the parent completed questionnaire, children were defined as having “asthma ever” if they had a doctor’s diagnosis of asthma on the questionnaire and “current asthma” if they had a history of wheeze or prolonged dry cough within the last 12 months. Children were diagnosed as atopic if they had a positive response to at least one aeroallergen, “ACS ever” if they had at least one episode, and “recurrent ACS” if they had at least two episodes of ACS. “Asthma ever” and “current asthma” were further subcategorised into atopic or non-atopic (atopic if the individual had a positive response to at least one aeroallergen by allergy skin testing and non-atopic if there had been no response). The responses to the questionnaire were compared with the doctors’ diagnoses using the kappa statistic measure of agreement, a kappa value of 1 denoting perfect agreement and a kappa value of 0 denoting poor agreement. The sensitivity and specificity of the questionnaire compared with the doctors’ diagnoses in the hospital and clinic settings were calculated using the chart diagnosis as the gold standard.
Differences were assessed for statistical significance using conditional logistic regression or the χ2 test as appropriate, and effect sizes reported as odds ratio and 95% confidence intervals (CI). Analysis was performed using SPSS 10.0 for Windows (SPSS Inc, Chicago, USA).
Sample size
Assuming a prevalence of asthma of 20%,24,25 recruitment of 80 children into each group gave 80% power at the 5% level to detect a twofold difference in the prevalence of asthma between children with SCD and controls.
RESULTS
In the validation population 44% and 39% of the children had “asthma ever” or “current asthma”, respectively, according to the parent completed questionnaire. The medical records highlighted that 41% of the children had “asthma ever” or “current asthma”. Substantial agreement was found between the results of the questionnaire and data from the medical records with a kappa statistic for “asthma ever” of 0.816. The sensitivity and specificity of the questionnaire for “asthma ever” were 93% and 90%, respectively.
Children with SCD in the study population were of similar age to the controls (median 7.77 years (range 5.24–9.73) v 7.78 (5.14–10.45)) with a similar proportion of boys in the two groups (46% v 49%, p = 0.791). “Asthma ever” and “current asthma”, both atopic and non-atopic, were more common in children with SCD than in controls (table 1). Treatment for “current asthma” was infrequent in both the children with SCD and controls (table 1): 16 children were taking a bronchodilator and six were taking inhaled steroids. There was no significant difference in the use of treatment between the two groups (p = 0.12).
Occurrence of asthma, bronchial hyperreactivity (BHR), atopy, and bronchodilator treatment in children with SCD and controls
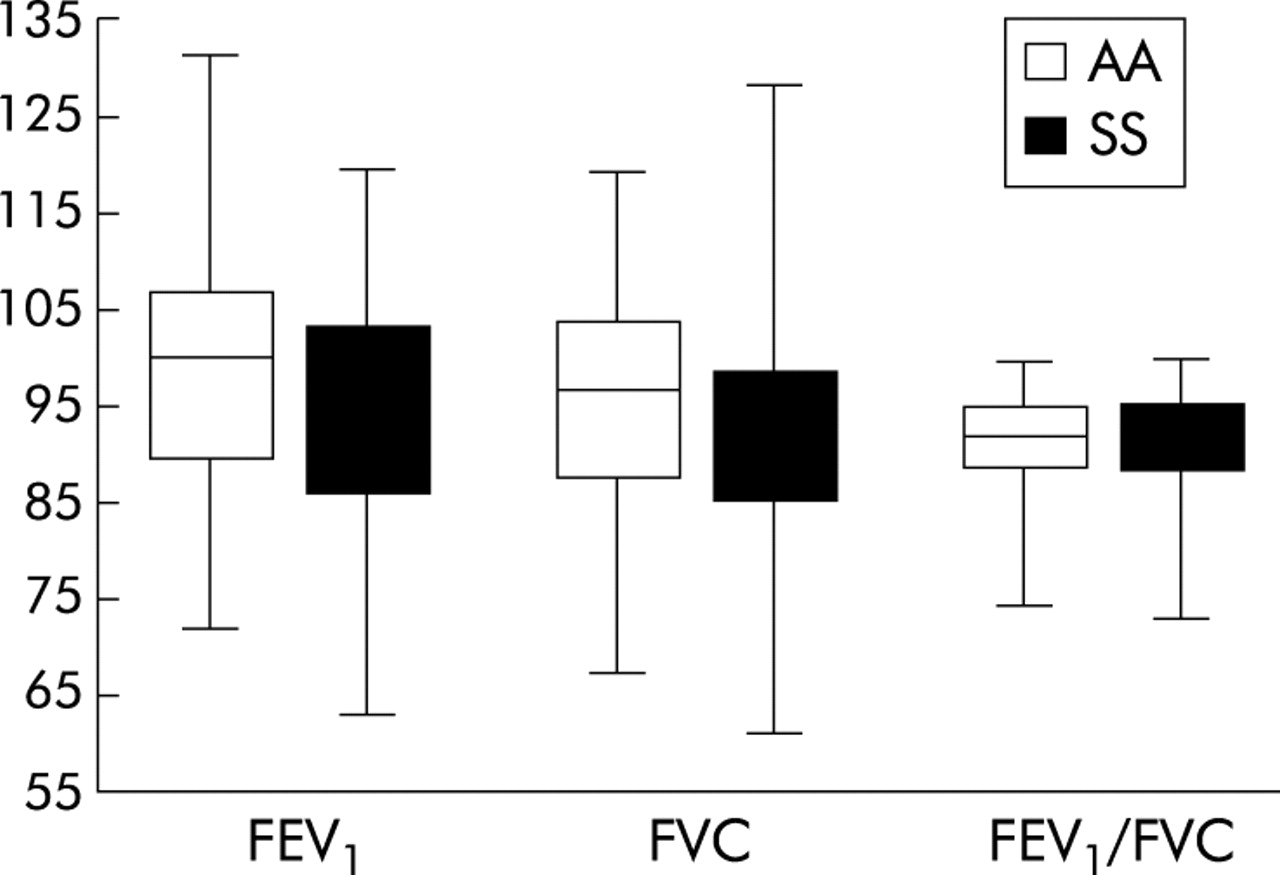
Baseline pulmonary function was similar in children with SCD and controls (fig 1). Six children (five with SCD) had a baseline FEV1 of <75%; two of the six children (both with SCD) had BHR. Exercise tests were satisfactorily completed in 43 control children and 38 children with SCD. Not keeping up when the pace was increased (SCD n = 6; controls n = 25), apparent desaturation (SCD n = 15; controls n = 5) and complaints of tiredness (SCD n = 13; controls: n = 4) were the most common reasons for failure to complete the exercise test. Prolonged cough, limp, and equipment problems each affected one child with SCD (n = 3), while equipment problems and hyperactivity each led to the failure of one control child to complete the exercise test (n = 2). Twenty six children were diagnosed as having BHR from the results of the exercise test (SCD n = 17; controls: n = 9). BHR diagnosed by exercise or bronchodilator testing was more common in children with SCD than in controls (SCD n = 19 (44%); controls n = 9 (20%), p = 0.02). Forty one children with SCD had 66 episodes of ACS (26 had a single episode); the maximum number of ACS episodes suffered by a child was six. Recurrent ACS episodes were associated with “current asthma” (particularly atopic “current asthma”), “asthma ever” (particularly atopic “asthma ever”) and atopy (table 2).
Asthma, bronchial hyperreactivity (BHR) and atopy by recurrent ACS status

{kind=link}
Baseline pulmonary function in children with sickle cell disease (SS) and controls.
DISCUSSION
We have shown that asthma and BHR are more common in children with SCD than in ethnically matched controls of a similar age, and that atopic asthma is associated with recurrent ACS in children with SCD. The difference in the prevalence of asthma was not due to a low prevalence in the controls which, at 22.5%, was similar to the 28.1% reported in Jamaican school children aged 6–11 years.29 The higher prevalence of asthma in children with SCD was not found in earlier studies. Those studies, however, assessed the prevalence of SCD in patients recruited from asthma clinics14,17,18 and their sample sizes were small, ranging from 36 to 155. The prevalence of SCD is one in 167, so studies with a small sample size would have been able to detect only a very strong relationship between asthma and SCD. Furthermore, the asthmatic children were recruited from hospital based asthma clinics, potentially biasing recruitment in favour of those with severe asthma,14,17,18 and the definitions of asthma used varied.15,17 The design of a study in which the prevalence of asthma in SCD patients was found to be similar to that of a control group was also flawed, as comparison was made with a predominantly white ethnic reference population15 and the prevalence of asthma has been shown to vary with ethnic origin.26
These data on asthma in children with SCD are the first to be produced using an easily administered questionnaire based on one that has been well validated and internationally accepted. The questionnaire was modified to include a question as to whether the child had “a touch of asthma”, this being a commonly used term in Jamaica. In addition, to shorten the questionnaire while still allowing the inclusion of cough variant asthma, wheeze and prolonged cough over the previous 12 months (current asthma) were combined in one question. We do not feel these modifications adversely affected the validity of the questionnaire as the comparison of the responses to the questionnaire to diagnoses documented in the medical records of the children seen in paediatric outpatient clinics showed good agreement. In addition, the sensitivity and specificity of the questionnaire for “asthma ever” (93% and 90%, respectively) were similar to those reported by Jenkins et al27 (85% and 81%, respectively) in a comparison of the ISAAC questionnaire with a physician assessment of current asthma status. The high prevalence of asthma in the validation population, however, is notable. The questionnaire was validated in the general paediatric clinic of the largest public paediatric hospital in Jamaica. In that setting only patients with severe asthma were referred to a specialist clinic and mild to moderate cases were followed in the general paediatric outpatient clinic. It is therefore possible that the prevalence of asthma in the general outpatient clinic would be higher than in the general population. We cannot, however, exclude the possibility that asthma was overdiagnosed using the questionnaire, but we suggest that this was unlikely as there was good agreement between the prevalence of asthma in control children determined by the questionnaire and previously published data.
One limitation of this study was that the controls were recruited to participate in “an asthma study” whereas the children with SCD were chosen randomly from the clinic database. If our method of recruitment of the controls had introduced a selection bias, we would have been more likely to recruit controls with asthma as parents who were concerned that their child had asthma would be more willing to participate. The higher prevalence in the children with SCD is therefore all the more striking.
We have shown that BHR was more common in children with SCD than in controls (table 1). This disagrees with the findings of a previous study28 in which no significant differences in changes in lung function to bronchodilator were noted between SCD children and controls. In that study,28 however, no bronchial provocation challenge was undertaken. In contrast, in two uncontrolled studies a higher rate of BHR was found in children with SCD than in our study.29,30 Koumbourlis et al29 reported that 54% of children with SCD had a positive response to bronchodilator while Leong et al30 found that 73% had a positive response to either bronchodilator or cold air challenge. Unfortunately, not all of our children were able to complete the exercise challenge so it is possible that we may have underdiagnosed BHR. However, similar proportions of children completed an exercise test in both groups and significantly more of the children with SCD had BHR than their ethnic matched controls.
Atopic and non-atopic asthma (particularly current asthma) and BHR were more common in children with SCD than in the controls, suggesting that the hypothesis of an association between asthma and SCD is valid. However, no significant difference was found in the prevalence of atopy in children with SCD and controls. It might therefore be suggested that we were misdiagnosing asthma and what we were documenting was reactive airways disease due to the underlying pathophysiology of SCD, as is seen with cystic fibrosis and gastro-oesphageal reflux. There was, however, a significant difference in the prevalence of atopy in SCD children who had recurrent ACS compared with other SCD children. It is therefore tempting to speculate that SCD children with atopic asthma may be predisposed to recurrent ACS; this may be due to an underlying Th2 profile as increased plasma levels of interleukin 4 are more common in patients with SCD than controls.31 There are, however, no data regarding Th2 status and ACS episodes; this merits investigation.
In conclusion, we have shown that asthma and BHR are more common in children with SCD than in ethnic matched controls, and that atopic asthma is associated with recurrent ACS episodes. We speculate that early and effective anti-asthma treatment might reduce the pulmonary morbidity associated with SCD.
REFERENCES
Footnotes
-
Dr Knight-Madden was funded by a Medical Research Council (United Kingdom) research fellowship.
Linked Articles
- airwaves