Article Text

Statistics from Altmetric.com
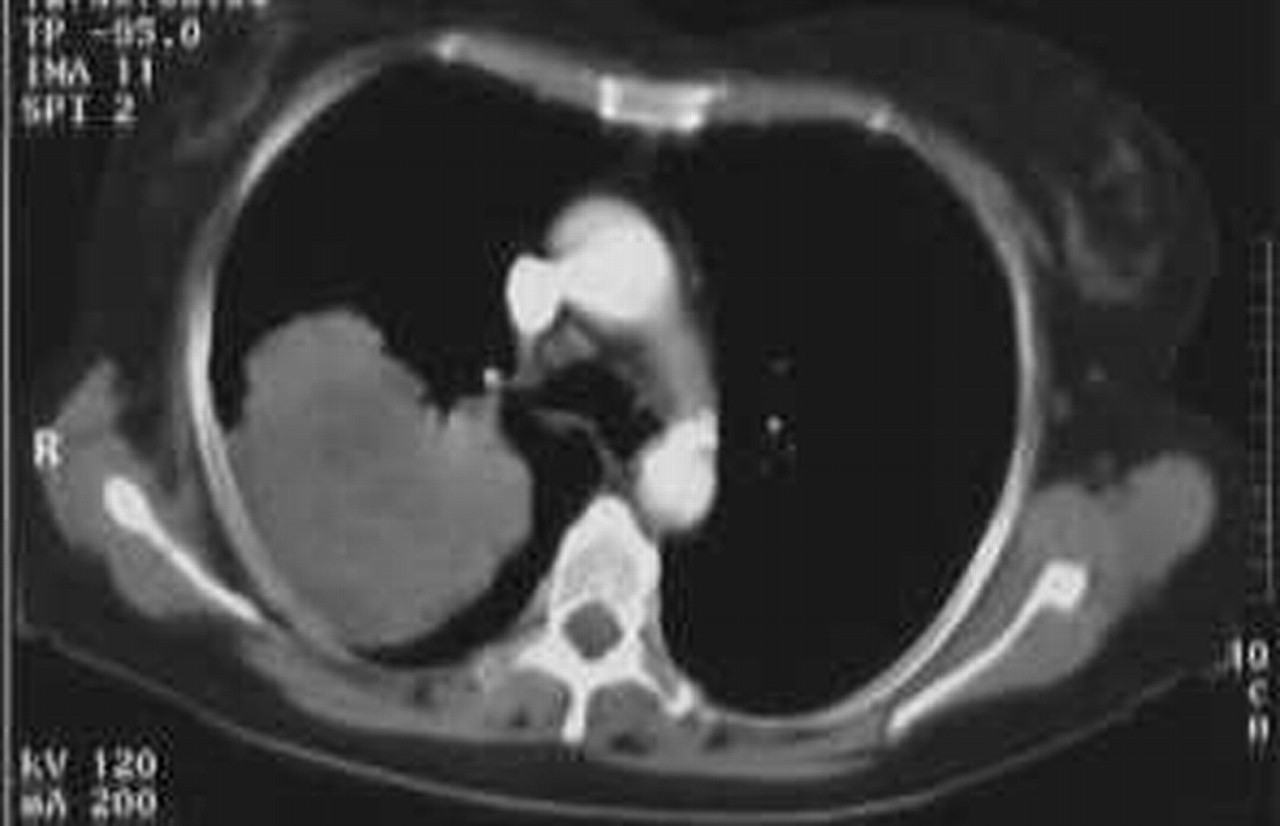
A 61 year old woman was investigated for a 12 month history of progressive thickening of the skin of her palms and soles. She had also complained of diarrhoea, exertional breathlessness and cough, and weight loss. There was no relevant past medical history or family history, but she had a 45 pack year history of cigarette smoking. Physical examination revealed diffuse hyperkeratosis of the palms and soles (fig 1), digital clubbing, and right sided chest signs. Her chest radiograph and thoracic CT scan (fig 2) showed a mass in the right upper lobe. This was confirmed by percutaneous biopsy to be a primary adenocarcinoma of the lung. Additional imaging excluded metastatic disease and detailed gastrointestinal investigations were all normal or negative.
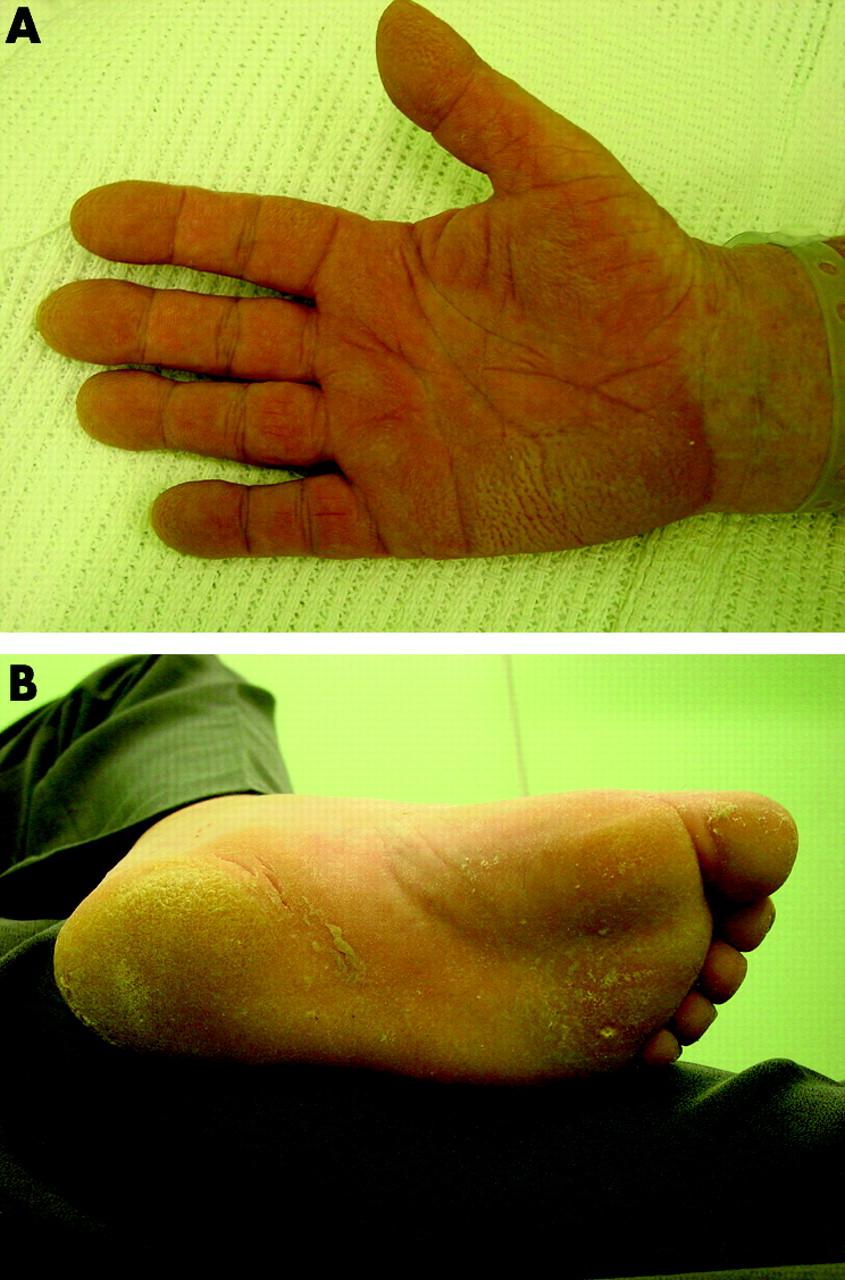
Diffuse keratoderma of (A) the right palm and (B) the left sole.
{kind=link}
{kind=link}
Section of contrast enhanced thoracic CT scan showing a large lobulated mass in the right upper lobe extending towards the right hilum.
The keratoderma was managed initially with 10% salicylic acid in Vaseline with some response. As the tumour was inoperable on the grounds of lung function, the patient received systemic chemotherapy. This resulted in a reduction in size of the primary tumour associated with a marked improvement in the cutaneous appearance.
Acquired non-familial palmoplantar keratoderma—sometimes referred to as “tripe palms”—is strongly associated with underlying neoplasia.1,2 At least 90% of cases occur in patients with an internal malignancy, most commonly of the gastrointestinal tract or lung. Pulmonary tumours are usually non-small cell, with squamous carcinomas described most frequently.
Learning points
-
Acquired non-familial palmoplantar keratoderma is an unusual paraneoplastic phenomenon.
-
At least 90% of cases are associated with an underlying neoplasm.
-
Cutaneous disease may precede the diagnosis of malignancy by many months.
Footnotes
-
Competing interests: none declared.