Article Text

Abstract
Background: Recent studies have repeatedly shown weak correlations among lung function parameters, atopy, exhaled nitric oxide level (Feno), and airway inflammatory markers, suggesting that they are non-overlapping characteristics of asthma in adults. A study was undertaken to determine, using factor analysis, whether the above features represent separate dimensions of childhood asthma.
Methods: Clinically stable asthmatic patients aged 7–18 years underwent spirometric testing, methacholine bronchial challenge, blood sampling for atopy markers and chemokine levels (macrophage derived chemokine (MDC), thymus and activation regulated chemokine (TARC), and eotaxin), Feno, and chemokines (MDC and eotaxin) and leukotriene B4 measurements in exhaled breath condensate (EBC).
Results: The mean (SD) forced expiratory volume in 1 second (FEV1) and Feno of 92 patients were 92.1 (15.9)% predicted and 87.3 (65.7) ppb, respectively. 59% of patients received inhaled corticosteroids. Factor analysis selected four different factors, explaining 55.5% of total variance. The Kaiser-Meyer-Olkin measure of sampling adequacy was 0.587. Plasma total and specific IgE levels, peripheral blood eosinophil percentage, and Feno loaded on factor 1; plasma TARC and MDC concentrations on factor 2; MDC, eotaxin and leukotriene B4 concentrations in EBC on factor 3; and plasma eotaxin concentration together with clinical indices including body mass index and disease severity score loaded on factor 4. Post hoc factor analyses revealed similar results when outliers were excluded.
Conclusions: The results suggest that atopy related indices and airway inflammation are separate dimensions in the assessment of childhood asthma, and inflammatory markers in peripheral blood and EBC are non-overlapping factors of asthma.
- BHR, bronchial hyperresponsiveness
- BMI, body mass index
- EBC, exhaled breath condensate
- FEno, exhaled nitric oxide
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- MDC, macrophage derived chemokine
- NO, nitric oxide
- TARC, thymus and activation regulated chemokine
- airway inflammation
- asthma
- exhaled breath condensate
- factor analysis
- lung function
- children
Statistics from Altmetric.com
- BHR, bronchial hyperresponsiveness
- BMI, body mass index
- EBC, exhaled breath condensate
- FEno, exhaled nitric oxide
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- MDC, macrophage derived chemokine
- NO, nitric oxide
- TARC, thymus and activation regulated chemokine
Asthma is characterised by reversible airway obstruction, bronchial hyperresponsiveness (BHR), and atopy.1 A number of clinical and spirometric parameters are used to evaluate the severity of the disease and to assess the response to treatment in chronic stable asthma.2 Traditionally, clinical symptomatology and disease scores as well as physiological measures of airway function (spirometry, peak expiratory flow rate, bronchial provocation) have been the primary means of assessing asthmatic patients. There has been increasing interest in monitoring airway inflammation in asthma. The cellular inflammatory response of the bronchial mucosa in asthma is characterised by eosinophil infiltration. Sputum eosinophilia is also shown to reflect disease severity of asthma.3–5 We recently reported that type 2 T helper lymphocyte (Th2) specific chemokines were associated with eosinophilia in peripheral blood and were increased in acute and chronic stable asthma.6–8 These patients also had increased nitric oxide (NO) and inflammatory mediators in exhaled breath.9–11 In many studies, however, there were poor interrelations between these outcome measures.5,10–13 For instance, the concentrations of Th2 specific chemokines (thymus and activation regulated chemokine (TARC), macrophage derived chemokine (MDC) and eotaxin) in exhaled breath condensate (EBC) did not show good correlations with those measured in peripheral blood in asthmatic children.10 The clinical, atopic, and inflammatory variables might therefore provide complementary data for monitoring the disease.
Factor analysis is commonly used to reduce a large number of disease parameters to a relatively small number of independent “factors”. As each factor groups associated parameters, the results help to provide insight into the pathogenesis of complex diseases. Being essentially free of a predetermined hypothesis on any interrelated parameters, this statistical technique can be viewed as a hypothesis generating tool. Factor analysis has been applied previously in studies of asthma in adults,14–17 and the results showed that clinical characteristics, spirometric parameters, BHR, and sputum inflammatory markers are non-overlapping dimensions. Assessment of disease control and severity in adults with asthma should therefore include measurements of all these parameters. Relevant data on factor analysis in childhood asthma are limited.18,19 Furthermore, most of the previous studies did not include atopic factors (such as plasma total and specific IgE levels) and emerging biomarkers of airway inflammation (such as NO and other mediators in exhaled air). The aim of this study was to specify objectively the heterogeneity of childhood asthma by categorising a number of functional, atopic, and inflammatory features of chronic stable asthma into separate complementary domains without a priori assumption. Such statistical evidence would further support the utility of routine measurement of all these dimensions.
METHODS
Study population
Patients aged 7–18 years with clinically stable asthma, diagnosed according to American Thoracic Society guideline,1 were recruited from the paediatric outpatient clinic of a university teaching hospital in Hong Kong. None were cigarette smokers. The patients had been free from symptoms of infection for 2 weeks before the study. Their anti-asthma treatments were also stabilised for at least 3 months. Asthma severity in these subjects was assessed by the disease severity score (DSS),20 a composite score that included daytime, night time and exercise induced symptoms, frequency of asthmatic exacerbation, and the use of anti-asthma medications, as well as by the Global Initiative for Asthma (GINA) criteria.2 Body weight and height were measured with the subject lightly clothed and barefooted using an electronic weighing scale (Model 708, Seca, Germany) and Harpenden stadiometer.
The parents of the subjects gave written informed consent and the Clinical Research Ethics Committee of our university approved the study.
Pulmonary function testing
All patients underwent spirometric assessment (Compact II, Vitalograph, Buckingham, UK) to measure their forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) which were compared with the local reference values.21 BHR was tested by inhalation of methacholine according to the protocol reported by Yan et al.22 PD20 (the provocative dose of methacholine that resulted in a 20% fall in FEV1) was noted from the log dose-response curve.
Exhaled NO measurement
The fractional exhaled NO concentration (Feno) was measured at an expiratory flow rate of 50 ml/s using a chemiluminescence analyser (NOA280i, Sievers Instruments, Boulder, CO, USA) according to ERS/ATS standard.23 Repeated exhalations were performed without nose clip until three NO plateau values agreed at the 10% level. The mean Feno value was then recorded.
Measurement of atopy and plasma inflammatory markers
Eosinophils in EDTA anticoagulated venous blood were counted using a Coulter STKS counter (Beckman-Coulter, Miami, FL, USA). The plasma total IgE concentration was measured by microparticle immunoassay (IMx analyser, Abbott Laboratories, Abbott Park, IL, USA), and specific IgE to Dermatophagoides pteronyssinus (the most prevalent local aeroallergen)8 was measured by fluorescent enzyme immunoassay (AutoCAP analyser, Pharmacia Diagnostics AB, Uppsala, Sweden). Patients with D pteronyssinus specific IgE (levels ⩾0.35 kU/l) were considered atopic. Plasma concentrations of TARC, MDC, and eotaxin were measured in duplicates by sandwich enzyme immunoassays (MDC and TARC: R & D Systems, Minneapolis, MN, USA; eotaxin: Biosource International, Camarillo, CA, USA). The detection limits of these chemokines were 7, 62.5 and 2.2 pg/ml, respectively.
Measurement of chemokines and LTB4 in breath condensate
Following mouth rinse, the subjects breathed tidally into the disposable RTube (Respiratory Research, Charlottesville, VA, USA) for 10 minutes.10,11 EBC thus obtained was immediately stored at −70°C until being assayed for MDC and eotaxin in one batch using the commercial kits described above. The concentration of leukotriene B4 (LTB4) was also measured by acetylcholinesterase competitive enzyme immunoassay (Cayman Chemical, Ann Arbor, MI, USA). The detection limit of this assay for LTB4 was 4 pg/ml.
Statistical analysis
The results were expressed as proportions, mean and standard deviation (SD), or median and interquartile range (IQR). Variables with non-Guassian distribution were logarithmically transformed before analysis. Exploratory factor analysis included the following 12 variables: clinical (body mass index (BMI), DSS); atopic (total and D pteronyssinus specific IgE, peripheral blood eosinophils), and inflammatory markers in peripheral blood (TARC, MDC and eotaxin) and EBC (Feno, MDC, eotaxin, LTB4). Because only 68 patients could successfully perform lung function measurements (FEV1, FVC, FEV1/FVC and PD20; table 1), these spirometric parameters were not included in the factor analysis in order to maintain an acceptable ratio between sample size and number of variables included.24 Bartlett’s test of sphericity was used to test for the possibility to perform factor analysis. The Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy was also evaluated. A high KMO (maximum 1.0; minimum acceptable 0.5) indicates that data are likely to factor well since correlations between pairs of variables can be explained by the other variables (low partial correlation coefficients).
Characteristics of study patients
Correlation coefficients were analysed by principal component analysis and subsequent rotation according to the standard varimax criterion.24,25 In this type of analysis the correlation between parameters is attributed to their common dependence on independent entities called “factors”. The coefficients that link parameters to factors are called “factor loadings”; the number of factors is chosen to be as small as possible but large enough to account for most of the variation within the data. It was decided a priori that the number of factors in the varimax rotation would be based on the number of eigenvalues ⩾1.0 in the principal component analysis.26 To assess the robustness of our findings we repeated the factor analysis after excluding outliers from the data set (defined as data outside the range of mean ±3SD) to determine the stability of the factor structures. Because no procedure is known for estimating standard errors of factor loadings, this study did not evaluate any statistical significance. Instead, we adopted one common and conventional rule of thumb to consider “factor loadings” of 0.45 or larger to be “high”.24
All analyses were performed with the Statistical Package of Social Sciences for Windows version 10.1 (SPSS Inc, Chicago, IL, USA).
RESULTS
Subjects
Ninety two consecutive asthmatic children were approached and all consented to participate. Table 1 summarises their clinical and laboratory characteristics. Forty five (49%) were receiving inhaled corticosteroid (ICS) treatment and nine were receiving treatment with a combination of ICS and inhaled long acting β agonist. Eighty eight patients (96%) were atopic. BHR was present in 26 (68%) steroid naive and 21 (70%) ICS treated patients, respectively (p = 0.889).
Asthma severity and study parameters
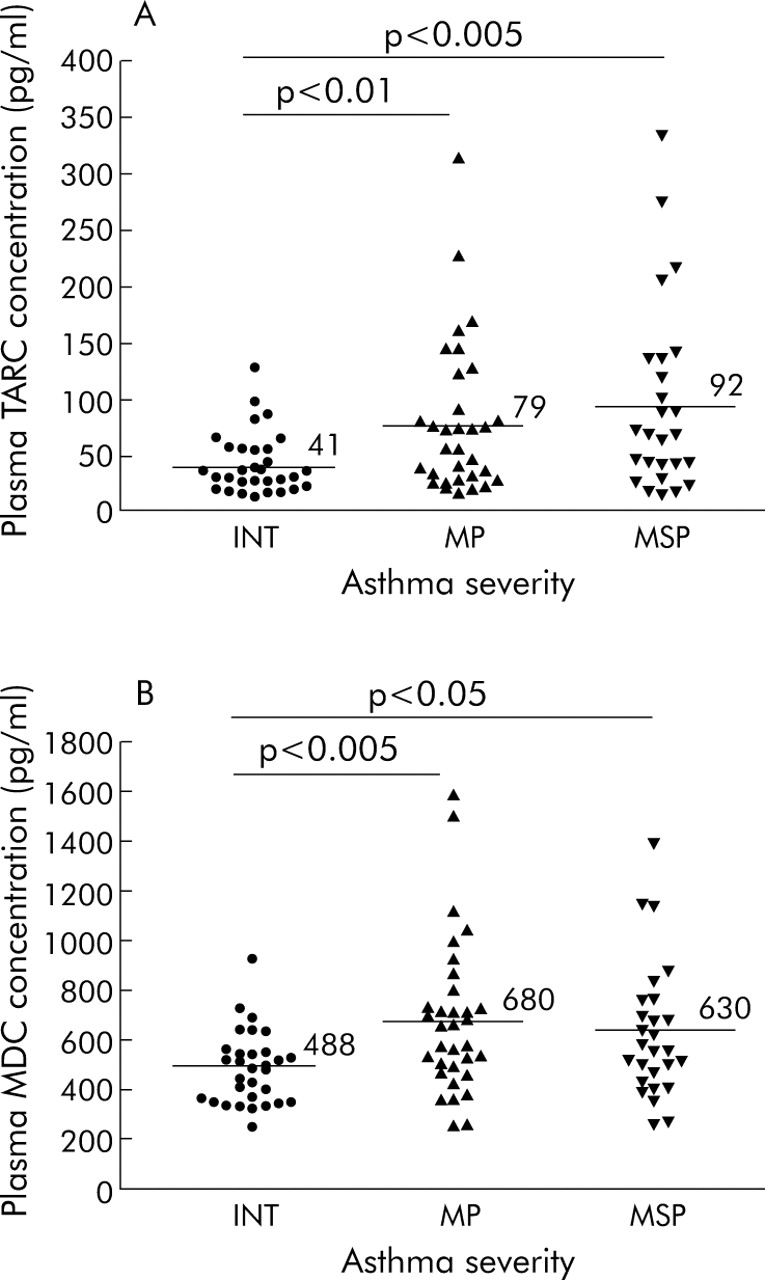
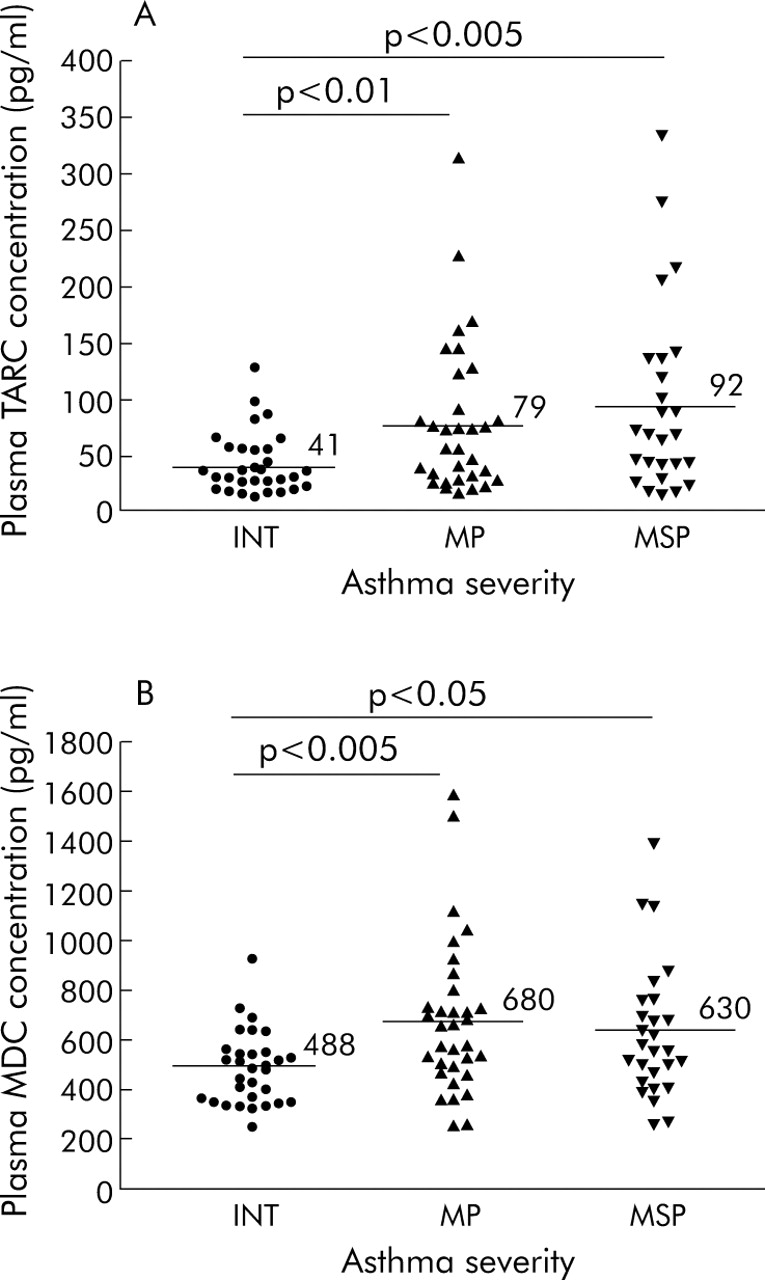
According to the GINA criteria, 31 patients (34%) suffered from intermittent asthma, 34 (37%) from mild persistent asthma, 12 (13%) from moderate persistent asthma, and 15 (16%) from severe persistent asthma. Plasma TARC and MDC concentrations were significantly higher in patients with persistent asthma than in those with intermittent disease (p = 0.006 and p = 0.009, respectively, ANOVA; fig 1). Other measured clinical, atopic, spirometric, or inflammatory parameters did not differ among the various GINA groups (results not shown).
{kind=link}
Distribution of plasma concentrations of (A) thymus and activation regulated chemokine (TARC) and (B) macrophage derived chemokine (MDC) in asthmatic patients with intermittent (INT), mild persistent (MP), and moderate to severe persistent (MSP) disease. Horizontal bars indicate the mean values for the respective groups.
Factor analysis
Bartlett’s test of sphericity indicated a correlation between the presently used variables because the correlation matrix was statistically different from an identity matrix (χ2 = 135.8, degree of freedom = 66, p<0.0001). The KMO measure of sampling adequacy was 0.587. Factor analysis yielded four separate factors that could explain 55.5% of the total variance in the data set when the “eigenvalue = 1” criterion was used. The addition of one more factor only resulted in an increase in the total explained variance to 63.8%. Thus, factor analysis with four components was presented (table 2). When factor analysis was repeated after excluding outliers >3SD, the KMO measure of sampling adequacy was 0.580. A total of five factors were identified (table 3). The robustness of the original factor structure was confirmed by the fact that all parameters except those in the original factor 4 (DSS, BMI, and plasma eotaxin concentration) were clustered into the same factors when outliers were excluded. Plasma eotaxin interestingly “returned” to the same factor as plasma TARC and MDC concentrations, and DSS and BMI were separated into two independent factors.
Varimax rotated factor loading matrix for all 92 asthmatic patients*
Distribution of parameters into different factors after exclusion of outliers
DISCUSSION
This study focused on the factor analysis of asthma related parameters in 92 children and adolescents with chronic stable asthma. Most of these patients had normal or mildly obstructed airways (mean FEV1 92%) but with significant airway inflammation (mean Feno 87.3 ppb). Factor analysis reduced 12 parameters into mostly four different factors with satisfactory sampling adequacy. Plasma total and D pteronyssinus specific IgE levels, peripheral blood eosinophil percentage, and Feno loaded on factor 1, plasma Th2 specific chemokines (TARC and MDC) loaded on factor 2, MDC, eotaxin and LTB4 levels in EBC loaded on factor 3, and DSS, BMI, and plasma eotaxin level loaded on factor 4. Post hoc factor analyses revealed similar clustering of the parameters when outliers were excluded.
This is the first study using factor analyses to show that the inflammatory markers (MDC and eotaxin) being measured in both peripheral blood and EBC are assigned to separate factors. Although the results from this limited study should not be generalisable to other biomarkers, our findings support the possibility that inflammatory mediators may be differentially regulated in these compartments in childhood asthma.
The factor analysis clearly demonstrated weak correlations between clinical, atopic and inflammatory parameters in childhood asthma. These differences can probably be explained by the fact that the health status of asthma has a number of distinct components. If the poor correlations are due mainly to measurement error of a single concept, the asthma parameters will not be separated into such clinically sensitive dimensions. BMI, plasma IgE levels, and airway inflammatory markers were consistently segregated into different components. In addition, although it was specified a priori that the number of factors in the varimax rotation would be based on the number of eigenvalues ⩾1.0 in the principal component analysis, exploratory rotations with both three and five factors were also conducted. The distributions on these alternative numbers of factors did not significantly alter the total variance explained. Lastly, all “factor loadings” were larger than 0.45 (table 2) and our final model explained more than 50% of the total variance.24 These results suggest a good assignment of the variables into the four factors.
Factor analysis reduces a large number of related or even seemingly unrelated parameters into a relatively small number of “factors”. As this method does not require a predetermined hypothesis on any interrelated parameters, this statistical technique is invaluable for determining possible ways to categorise the many dimensions of complex diseases such as asthma. However,, this approach does not offer any mechanistic link between variables that cluster in the same factor. In addition, the clustering of variables obtained may apparently be unexplained from the clinical point of view. We should therefore be very careful in deciding on the optimal number of factors (with the help of Scree plot, eigenvalues, etc) while making the best biological sense of the results.24–26
Factor analysis has not been widely applied in studying asthma related parameters in children. Among Chinese children, Qian and colleagues conducted factor analysis to examine the associations between respiratory health outcomes and household risk factors.18 They found that the five factors of heating coal smoke, socioeconomic status, ventilation, environmental tobacco smoke, and parental asthma were independently associated with asthma. In another study on asthmatic children, principal components and factor analysis suggested two independent factors—atopy related indices and loci on chromosome 5q31–33 that encoded the cytokine gene cluster.19 The present study provides further data to this expanding field by suggesting different non-overlapping clinical, atopic, and inflammatory factors in childhood asthma.
Clinical measures of asthma were shown to have poor correlations with subjective quality of life indicators,17 and the occurrence of asthma symptoms was also independent of subjects’ BMI and measures of airway function.27 These observations open up a new dimension for clinical trials; any new asthma treatment should aim to reduce asthma specific mortality and morbidity and improve patient well being, daily activities, and emotional stability.28 In asthma the conventional clinical outcomes address the first concern and quality of life assessment addresses the latter. Thus, subjective patient status has to be measured and interpreted independently. To complicate the issue, the present study suggests that airway inflammatory markers in peripheral blood and EBC are different dimensions in the assessment of childhood asthma. It will be interesting and important to know the ways in which different asthma interventions bring about improvements in clinical, immunological, and quality of life outcomes in these patients.
This study included BMI in the factor analysis because of a number of recent publications on an epidemiological association between asthma and obesity.27,29–31 This relation seemed to be present, irrespective of atopy and eosinophil counts.27,31 In the Childhood Asthma Management Program, BMI was independently associated with FEV1, FVC, and FEV1/FVC but not with asthma symptoms or atopy.27 Our recent study also could not find any association between BMI and spirometric variables, percentage of peripheral blood eosinophils, Feno, or LTB4 levels in EBC.11 Whereas the mechanical properties of the respiratory system associated with obesity may account for this linkage, obese patients were found to have increased levels of leptin and pro-inflammatory cytokines.32 These pathways may be independent of Th2 specific chemokines, so our factor analyses failed to reveal any correlation between BMI and inflammatory markers in peripheral blood or EBC.
Although 12 asthma related parameters are grouped into four factors in this study, this does not mean that childhood asthma is determined only by four factors. There may be other factors that are not captured by these 12 items. For example, quality of life has been found to be an important component of asthma17 but this was not measured in our patients. Although it is too invasive to use bronchial biopsy samples to monitor asthma, the presence of inflammatory markers (such as eosinophils and chemical mediators) in induced sputum has not been evaluated. The inflammatory markers included in this study may also be associated with other as yet unidentified factors. Additional studies should be performed to examine the mechanisms that link the four components of childhood asthma identified in this study.
In conclusion, this study suggests that asthma related parameters including atopic factors and airway inflammatory markers are non-overlapping dimensions in the assessment of chronic stable asthma in children. Specifically, inflammatory markers in peripheral blood and EBC should be considered as separate dimensions. The results support the usefulness of routine measurement of these dimensions in monitoring childhood asthma.
Acknowledgments
The authors thank I H S Chan for measuring total and allergen specific IgE and C Y Li, E Yung, C S S Au, and E K H Liu for measuring Feno and inflammatory markers in peripheral blood and EBC.
REFERENCES
Footnotes
-
Published Online First 29 July 2005
-
This research project is funded by Hong Kong Research Grant Council Earmarked Grant (CUHK 4165/02M) and Direct Grant for Research of The Chinese University of Hong Kong.
-
Competing interests: none of the authors of this article has any competing interest.